


Abstract
Background Transforaminal lumbar interbody fusion (TLIF) and posterolateral fusion (PLF) without an interbody device are two common approaches for single-level, open posterior fusion. Presently, it is unknown whether one of these operations leads to better outcomes. We sought to compare reoperation, complication, and readmission rates between TLIF and PLF for patients undergoing elective single-level, open, posterior lumbar fusion.
Methods A single-center, retrospective cohort study utilizing prospectively collected data was performed. Inclusion criteria were patients undergoing elective single-level, open, posterior lumbar decompression and fusion between October 2010 and April 2021 with at least 1-year follow-up. The two comparison groups were TLIF vs PLF alone without interbody. The primary outcome was need for reoperation at most recent follow-up. Secondary outcomes included 90-day complication and readmission rates. Univariate and multivariable logistic regression analyses were performed.
Results A total of 850 patients were included, 591 (69.5%) of whom underwent TLIF and 259 (30.5%) of whom underwent PLF. Median follow-up was 6.1 years (interquartile range 3.7–8.9). No significant difference was found in overall reoperation rates (12.4% vs 13.9%, P = 0.534). When stratified by <5-year follow-up (n = 231 TLIF, n = 85 PLF; 37.2%) and ≥5-year follow-up (n = 360 TLIF, n = 174 PLF; 62.8%), no significant differences were seen in either cohort (<5 years: n = 24 TLIF vs n = 9 PLF, P = 0.959; 5+ years: n = 49 TLIF vs n = 27 PLF, P = 0.555). On multivariable logistic regression analysis, the presence of interbody fusion was not associated with reoperation (OR 2.26, 95% CI 0.66–7.74, P = 0.194).
Clinical Relevance For patients undergoing elective single-level, open, posterior lumbar fusion without isthmic spondylolisthesis, no differences were seen in reoperation rates at long-term follow-up. Similar 90-day complication and readmission rates were seen. These results suggest that in degenerative lumbar spine disease without isthmic spondylolisthesis, TLIF and PLF achieved similar outcomes.
Level of Evidence 3.
Introduction
Lumbar degenerative disease resulting in low back pain and/or lower extremity radiculopathy is a potentially debilitating condition with increasing prevalence due to an aging population.1,2 Lumbar decompression and fusion surgery is well established as a treatment for degenerative spine pathology, including disc degeneration, spondylosis, and spondylolisthesis.3 Over time, increasing rates of lumbar spine surgery and improved outcomes have been observed, attributable to advances in surgical technique, such as the introduction of interbody fusion approaches.2,4
Two of the most common lumbar fusion techniques are transforaminal lumbar interbody fusion (TLIF) and posterolateral fusion (PLF) alone without interbody fusion.5,6 Historically, PLF was considered the gold standard; however, extensive decompression can reduce available surface area for bony fusion, presenting a potential limitation to success.7,8 The introduction of interbody techniques as a strategy to increase surface area for grafting has resulted in TLIF surpassing PLF as the most commonly implemented technique for the surgical treatment of lumbar spondylolisthesis. The percentage of degenerative spondylolisthesis patients treated with TLIF increased from 13.6% in 1999 to 32% in 2011.9,10 The latter was partly due to improved fusion rates observed following TLIF compared with PLF, reaching 90% in some studies.11,12 The addition of an interbody spacer provides biomechanical anterior column support, offers the advantage of load sharing, provides indirect decompression, and strengthens the posterior pedicle screw and rod construct.7,13,14
In patients with degenerative single-level lumbar spinal stenosis and degenerative spondylolisthesis, several prospective and retrospective cohort studies have compared various interbody fusion techniques with PLF and shown no statistically significant difference in functional outcomes or postoperative complication rates.2,15–17 However, while studies comparing TLIF and PLF exist, the literature may benefit from studies with larger sample sizes, narrower inclusion criteria, and longer follow-up intervals.17,18 In a cohort of patients undergoing elective, single-level, open, posterior lumbar decompression and fusion, we sought to compare reoperation rates between TLIF and PLF, with secondary outcomes comparing 90-day complication and readmission rates.
Methods
Study Design
A retrospective cohort study was undertaken, utilizing our institution’s prospective spine outcomes registry of all patients undergoing elective spine surgery since October 2010. Institutional review board (IRB) approval was appropriately obtained for the study (IRB no. 211290). A signed consent for participation was obtained from all patients a priori.
Patient Population
Demographics, past medical history, radiographic and operative variables, and postoperative outcome variables were extracted from the registry. Inclusion criteria were all adult patients aged 18 years or older undergoing elective, single-level, open, posterior lumbar fusion with or without interbody fusion between 10 October 2020 and 4 April 2021. Exclusion criteria included patients with isthmic spondylolisthesis, as interbody placement was indicated for the majority of these patients.19 Furthermore, patients undergoing minimally invasive surgeries and those with anterior and lateral spinal fusions were excluded.
Independent Variables
The primary exposure variable of interest was the presence of interbody fusion. The cohort was dichotomized into two groups: TLIF and PLF alone without interbody fusion, relying solely on a PLF across the transverse processes and remaining facet joints. The presence of interbody fusion was determined from operative notes. For our purposes, TLIF included both a transforaminal approach, as well as a more classic posterior lumbar interbody fusion (PLIF) approach.
Additional independent variables included demographic information (ie, age, gender, race, etc), past medical history (ie, comorbidities, smoking status, preoperative ambulation status, preoperative diagnosis, etc), radiographic variables (ie, disc height, flexion-extension measurements, presence of spondylolisthesis, etc.), and perioperative variables, including estimated blood loss (EBL) and operative time. Follow-up interval was determined by review of the electronic medical record (EMR) and recorded as time from index operation to present (1 January 2022).
Outcomes
The primary outcome of interest was long-term reoperation rates, defined as the need for subsequent operation following the initial operation. Patients were dichotomized into less than 5 years and more than 5-year follow-up based on the date of index surgery and the need for reoperation at the time of EMR chart review. Secondary outcomes included 90-day complication rate and readmission. Complications included wound-related issues such as surgical site infection (SSI) and hematoma formation, as well as non-wound-related complications such as urinary tract infection, neurological deficit, pneumonia, and deep vein thrombosis. Readmission rate and indication were noted in the 90-day postoperative period.
Statistical Analysis
Descriptive statistics were performed for all demographic, past medical history, preoperative, and postoperative variables. Continuous variables were presented as mean and standard deviation (SD), while categorical variables were presented as frequencies. Subsequently, between-group analysis was performed comparing TLIF and PLF patients using Student t tests for continuous variables and χ 2 test for categorical variables. To assess the relationship between presence of interbody fusion and outcome variables, univariate and multivariable logistic regression analyses were performed, comparing TLIF with PLF. Covariates in the multivariable logistic regression were defined a priori based on prior literature and included age, body mass index (BMI), disc height, presence of movement on flexion-extension, amount of movement on flexion-extension, and spondylolisthesis grade. Statistical significance was defined a priori at P < 0.05. All analyses were performed using SPSS 22 (IBM, Armonk, NY, USA).
Results
Demographics and Medical History
The final cohort included 850 patients undergoing single-level, open, posterior lumbar fusion, 591 (69.5%) of whom underwent TLIF and 259 (30.5%) of whom underwent PLF. Most patients were White (n = 753, 88.6%), and more than half were women (n = 473, 55.6%). Based on retrospective EMR review, median follow-up time for the total cohort was 6.1 years (interquartile range [IQR] 3.7–8.9). Compared with PLF patients, TLIF patients were younger at time of surgery (59.0 ± 11.3 vs 63.3 ± 12.6 years; P < 0.001) and had a higher BMI (31.3 ± 6.6 vs 30.2 ± 12.6; P = 0.019). Furthermore, TLIF patients were more likely to be covered by private insurance than their PLF counterparts (50.3% vs 39.0%; P = 0.001). No statistically significant differences were observed in number of comorbidities, past medical history, symptom duration, or preoperative diagnosis between the two groups. Demographic and medical history variables are presented in Table 1.
Demographic characteristics of patients who underwent TLIF vs PLF.
Radiographic, Perioperative, and Postoperative Variables
Radiographic, perioperative, and postoperative variables in patients undergoing single-level, open, posterior lumbar fusion are summarized in Table 2. No differences were observed between TLIF and PLF patients in preoperative disc height (8.8 ± 3.2 vs 8.8 ± 2.9 mm; P = 0.785), presence of movement on flexion-extension (n = 68, 11.5% vs n = 27, 10.4%; P = 0.555), and mean millimeters of movement on flexion-extension measurement (3.0 ± 2.6 vs 2.7 ± 1.5 mm; P = 0.620). Furthermore, no statistically significant difference in the presence (n = 413, 69.9% vs n = 185, 71.4%; P = 0.341) or grade of spondylolisthesis was observed between the TLIF and PLF cohorts.
Radiographic, perioperative, and postoperative variables of patients undergoing TLIF vs PLF.
Perioperatively, no statistically significant difference was observed in EBL (415.6 ± 300.8 vs 381.7 ± 299.6 cc; P = 0.190) or operative time (207.4 ± 58.7 vs 203.6 ± 55.7 minutes; P = 0.441) between TLIF and PLF. At discharge, compared with PLF patients (n = 209, 80.7%), more TLIF patients were discharged home (n = 510, 86.3%; P = 0.026) than to inpatient rehabilitation facilities or skilled nursing facilities. No statistically significant difference was observed in length of stay between TLIF and PLF patients (2.8 ± 2.3 vs 3.0 ± 1.4 days; P = 0.110).
Primary Outcome: Reoperation
All primary and secondary outcome variables are summarized in Table 3. Median follow-up time for the TLIF cohort was 5.7 years (IQR 3.8–8.8) compared with 7.0 years (IQR 3.4–8.9) for the PLF cohort. For the primary outcome of reoperation at last follow-up, 231 TLIF patients (39.1%) had less than 5 years of follow-up, while 360 (60.9%) patients had more than 5 years follow-up. There were 85 (32.8%) PLF patients with less than 5 years of follow-up compared with 174 (67.2%) patients with more than 5 years of follow-up. No statistically significant difference was observed in overall reoperation rates between the TLIF (n = 73, 12.4%) and PLF (n = 36, 13.9%) cohorts (P = 0.534) (Figure A). When divided into reoperation for patients with less than 5 years of follow-up (n = 24, 10.4% vs n = 9, 10.5%; P = 0.959) and more than 5 years of follow-up (n = 49, 13.6% vs n = 27, 15.5%; P = 0.555), no statistically significant differences were observed between patients undergoing TLIF and PLF, respectively, in either group.
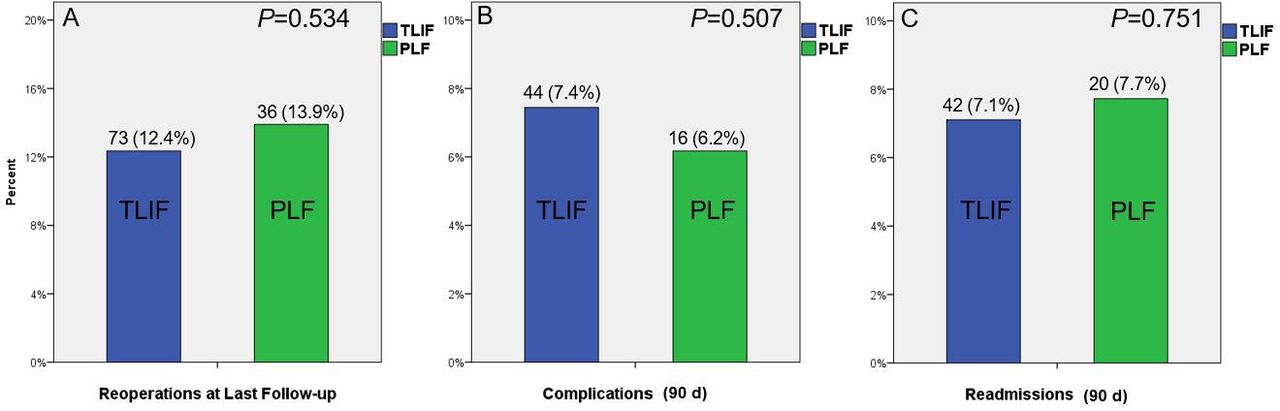
Comparison of primary and secondary outcomes between transforaminal lumbar interbody fusion (TLIF) and posterolateral fusion (PLF) cohorts with regard to reoperation rates (A), 90-d complication rate (B), and 90-d readmission rate (C).
Outcome variables of patients undergoing TLIF vs PLF.
Univariate (OR 1.14, 95% CI 0.74–1.75, P = 0.535) and multivariate (OR 2.26, 95% CI 0.66–7.74, P = 0.194) regression analysis controlling for the aforementioned covariates revealed no significant association between the presence of interbody fusion and overall reoperation rate (Table 4).
Univariate and multivariate logistic regression of complications, readmission, and reoperation and presence of interbody fusion.
Secondary Outcomes: 90-Day Complications and Readmission
For the secondary outcome of complications within 90 days, no statistically significant difference was observed in the TLIF cohort compared with the PLF cohort (n = 44, 7.4% vs n = 16, 6.2%; P = 0.507) (Figure B). Postoperative hematoma was documented for 1 patient in both the TLIF (0.2%) and PLF (0.4%) cohorts. Five (0.8%) TLIF patients experienced a neurological deficit compared with 1 PLF patient (0.4%). Fourteen TLIF patients (2.4%) experienced SSI compared with 4 PLF patients (1.5%).
On univariate logistic regression analysis, TLIF was not significantly associated with 90-day complications as compared with PLF (OR 1.22, 95% CI 0.67–2.20; P = 0.507). A multivariable logistic regression model adjusting for age, BMI, disc height, presence of movement on flexion-extension, amount of movement on flexion-extension, and spondylolisthesis grade revealed no significant association between presence of interbody fusion and 90-day complications (OR 1.39, 95% CI 0.19–9.88; P = 0.742). Univariate and multivariable regression analysis are presented in Table 4.
For the secondary outcome of readmission, no statistically significant difference was observed in 90-day readmission rates between TLIF and PLF (7.1% vs 7.7%, P = 0.751) (Figure C). On univariate logistic regression, the presence of interbody fusion was not associated with 90-day readmission rates (OR 0.91, 95% CI 0.52–1.59; P = 0.751). Similarly, multivariate analysis remained nonsignificant when controlling for the aforementioned covariates for 90-day readmission rates (OR 1.03, 95% CI 0.13–7.72; P = 0.976).
Discussion
In the current study, we compared TLIF and PLF in a cohort of patients undergoing single-level, open, posterior lumbar spinal fusion. No significant differences were seen in long-term reoperation rates at the most recent follow-up between the two operative techniques. Furthermore, no difference was observed between TLIF and PLF in 90-day complication or readmission rates. Importantly, several potential confounders were controlled for, including the presence of spondylolisthesis, spondylolisthesis grade, disc height, and flexion-extension measurements. These results support that in patients undergoing single-level, open, posterior lumbar fusion, TLIF and PLF have similar long-term reoperation rates and short-term complications and readmissions.
Compared with patients undergoing TLIF, patients undergoing PLF for elective single-level, open posterior lumbar fusion did not experience higher reoperation rates. The current findings are consistent with other studies comparing the two operative techniques. A previous study by Park et al20 reviewed patients undergoing single-level fusion surgeries in the Korean Health Insurance Review and Assessment Service database, finding no differences in repeat decompression and fusion rates between patients undergoing TLIF (n = 381/12,086, 3.15%) and PLF (n = 268/8520, 3.15%). Moreover, our findings are supported by a meta-analysis from Zhang et al21 comparing TLIF and PLF in degenerative lumbar spondylosis; the authors found no significant differences in reoperation between the two approaches in either randomized controlled trials (relative risk [RR]: 0.83, 95% CI 0.18–3.75, P = 0.809) or observational studies (RR 0.21, 95% CI 0.03–1.77, P = 0.151).
In a study comparing two-level PLF augmented with single vs two-level TLIF, the authors found no significant differences in reoperation rates between TLIF at a single level vs both levels (13.1% vs 10.3%, P = 0.440).22 The authors suggested that additional TLIF did not contribute to increased need for revision surgery. Additionally, while a previous study of 89 patients undergoing an isolated L4-L5 decompression and fusion compared TLIF (N = 58) with PLF (N = 31) and found a higher rate of reoperation in TLIF patients (n = 16, 28% vs n = 2, 6%, P = 0.02). However, this particular study featured a small sample size of 89 patients.7 Our larger analysis of patients undergoing single-level, open, posterior lumbar surgery found no significant differences in reoperation rates for patients with less than 5 years and those with more than 5 years of follow-up, suggesting comparable short-term and long-term outcomes between the two approaches.
Our study has the advantage of being a homogenous sample, restricting the operation to only a single-level fusion, whereas several prior studies include heterogenous samples of multilevel fusions. As such, the similar reoperation rates may be due to only examining patients with single-level fusions, as multilevel TLIFs have been shown to be more prone to reoperation due to development of adjacent segment disease, mechanical complications, and pseudarthrosis compared with single-level TLIFs.22 These complications may arise from increased relative motion and increased intradiscal pressures at levels adjacent to the TLIF, which are mitigated in single-level fusion.23,24
Our study found no statistically significant differences between TLIF and PLF in 90-day complication and readmission rates in patients undergoing elective single-level, open posterior lumbar fusion. This is generally supported by the broader literature comparing the two fusion techniques. A study of single-level lumbar surgery by Plantz et al25 compared short-term outcome measures and complications between single-level PLF alone (n = 8905), single-level posterior interbody fusion (PLIF/TLIF) (n = 5954), and combined single-level PLF and PLIF/TLIF (n = 9369) and found that a combined approach was associated with higher EBL relative to either operative approach alone (8.2% vs 7.1% vs 4.8%, P < 0.001); however, no significant differences were observed in other surgical complications, such as surgical site infection (1.2% vs 1.4% vs 1.5%, P = 0.313) and wound dehiscence (0.3% vs 0.2% vs 0.2%, P = 0.206).
A systematic review and meta-analysis by Levin et al26 quantitatively examined 5 studies comparing TLIF and PLF, and found that TLIF was superior in achieving radiographic fusion (OR 0.33, 95% CI 0.13–0.82) but equivocal in postoperative infection rates (OR 1.09, 95% CI 0.25–4.75) and blood loss (mean difference: −58.87, 95% CI −178.81 to 61.07). While there has been conjecture into the protective effect of TLIF in reducing rates of early screw loosening, the evidence on this front is limited.27 Furthermore, in line with the results of the aforementioned meta-analysis and previous literature, our study found no differences between the two operative approaches in 90-day readmission rates or perioperative variables such as EBL or operative time,9 suggesting that the two approaches are comparable in patients undergoing single-level lumbar fusion.
Limitations
The current study is not without limitations. First, the use of registry data introduced the possibility of confounding stemming from incorrect or absent coding. Furthermore, our data were extracted from a single institution with a limited number of spine surgeons, and the decision to perform TLIF vs PLF alone was based solely on surgeon preference, introducing potential selection bias and affecting the generalizability of our results. Further inquiry with a larger multicentered study containing more patients and surgeons is indicated to validate the findings of our study. In addition, follow-up was determined based on EMR review, rather than actively calling patients to ensure they didn’t have another spine surgery elsewhere. Although our center is the single tertiary medical center in the area, it is possible that some of our patients sought spine care elsewhere that may have been missed in the retrospective EMR review. Moreover, we were not able to control for potentially important variables such as use of bone morphogenic protein and other biologics, and the amount of decompression, variables not collected in our registry. In theory, a larger decompression may predispose patients to pseudarthrosis and thus the need for reoperation when compared with a more limited decompression. Additionally, postoperative radiographic measurements were also not reported in our study. Including radiographic assessments during follow-up visits may add additional insight into postoperative outcomes between the two groups and is an appropriate future direction. Efforts are ongoing in our research group to evaluate the importance of segmental lordosis in degenerative lumbar fusion surgery. Finally, although our study controlled for multiple covariates hypothesized to relate to overall outcomes, such as disc height and flexion-extension movement, including presence of spondylolisthesis, it did not consider the specific pathology and indication for operation, such as spinal stenosis or adjacent segment disease.9
Conclusion
In a cohort of patients undergoing single-level, open, posterior lumbar fusion, TLIF and PLF exhibited similar rates of long-term reoperation, in addition to similar 90-day complication and readmission rates. Taken together, TLIF and PLF appear to have comparable long-term reoperation and short-term complication rates.
Acknowledgments
We would like to acknowledge the late Clint Devin for providing the study idea at its inception.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Amir M. Abtahi received institutional research support from Stryker Spine. Byron F. Stephens has received consulting fees from DePuy-Synthes and research support from Stryker Spine. Scott L. Zuckerman reports being an unaffiliated neurotrauma consultant for the National Football League. The remaining authors have nothing to report.
Institutional Review Board Approval Institutional Review Board (IRB) approval was appropriately obtained for the study (IRB #211290).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.