


ABSTRACT
Background: Regional and segmental changes of the lumbar spine have previously been described as patients transition from standing to sitting; however, alignment changes in the cervical and thoracic spine have yet to be investigated. So, the aim of this study was to assess cervical and thoracic regional and segmental changes in patients with thoracolumbar deformity versus a nondeformed thoracolumbar spine population.
Methods: This study was a retrospective cohort study of a single center's database of full-body stereoradiographic imaging and clinical data. Patients were ≥ 18 years old with nondeformed spines (nondegenerative, nondeformity spinal pathologies) or thoracolumbar deformity (ASD: PI-LL > 10°). Patients were propensity-score matched for age and maximum hip osteoarthritis grade and were stratified by Scoliosis Research Society (SRS)–Schwab classification by PI-LL, SVA, and PT. Patients with lumbar transitional anatomy or fusions were excluded. Outcome measures included changes between standing and sitting in global alignment parameters: sagittal vertical axis (SVA), pelvic incidence minus lumbar lordosis (PI-LL), pelivc tilt (PT), thoracic kyphosis, cervical alignment, cervical SVA, C2-C7 lordosis (CL), T1 slop minus CL (TS-CL), and segmental alignment from C2 to T12. Another analysis was performed using patients with cervical and thoracic segmental measurements.
Results: A total of 338 patients were included (202 nondeformity, 136 ASD). After propensity-score matching, 162 patients were included (81 nondeformity, 81 ASD). When categorized by SRS-Schwab classification, all nondeformity patients were nonpathologically grouped for PI-LL, SVA, and PT, whereas ASD patients had mix of moderately and markedly deformed modifiers. There were significant differences in pelvic and global spinal alignment changes from standing to sitting between nondeformity and ASD patients, particularly for SVA (nondeformed: 49.5 mm versus ASD: 27.4 mm; P < .001) and PI-LL (20.12° versus 13.01°, P < .001). With application of the Schwab classification system upon the cohort, PI-LL (P = .040) and SVA (P = .007) for severely classified deformity patients had significantly less positional alignment change. In an additional analysis of patients with segmental measurements from C2 to T12, nondeformity patients showed significant mobility of T2-T3 (−0.99° to −0.54°, P = .023), T6-T7 (−3.39° to −2.89°, P = .032), T7-T8 (−2.68° to −2.23°, P = .048), and T10-T11 (0.31° to 0.097°, P = .006) segments from standing to sitting. ASD patients showed mobility of the C6-C7 (1.76° to 3.45°, P < .001) and T11-T12 (0.98° to 0.54°, P = 0.014) from standing to sitting. The degree of mobility between nondeformity and ASD patients was significantly different in C6-C7 (−0.18° versus 1.69°, P = .003), T2-T3 (0.45° versus −0.27°, P = .034), and T10-T11 (0.45° versus −0.30°, P = .001) segments. With application of the Schwab modifier system upon the cohort, mobility was significant in the C6-C7 (nondeformed: 0.18° versus moderately deformed: 2.12° versus markedly deformed: 0.92°, P = .039), T2-T3 (0.45° versus −0.08° versus −0.63°, P = .020), T6-T7 (0.48° versus 0.36° versus −1.85°, P = .007), and T10-T11 (0.45° versus −0.21° versus −0.23°, P = .009) segments.
Conclusions: Nondeformity patients and ASD patients have significant differences in mobility of global spinopelvic parameters as well as segmental regions in the cervical and thoracic spine between sitting and standing. This study aids in our understanding of flexibility and compensatory mechanisms in deformity patients, as well as the possible impact on unfused segments when considering deformity corrective surgery.
INTRODUCTION
Adult spinal deformity (ASD) includes a spectrum of deviations in spinal alignment arising from a multitude of etiologies.1 The range of spinal diseases presenting in adulthood serve as a source of substantial back pain and disability.2 The escalating population age has led to a striking rise in ASD prevalence rates.3,4
Treatment for ASD ranges from nonoperative therapies to operative correction of deformity.5 The decision for a patient to undergo a corrective operation stems from the severity of spinal malalignment and correlated disability.6,7
Accurate classification of ASD requires a thorough radiographic evaluation of both the spine and pelvis. Concurrent appraisal of the cervical, thoracic, and lumbar spine, as well as the femoral heads and pelvis, is also necessary. Regional, global, and pelvic alignment contribute to the overall evaluation of the spine.8 The combination of deformity and the compensation to maintain a free-standing posture define the alignment, resulting in the classification of ASD severity from an alignment standpoint. Pain and disability levels correlate to severity categorization from a clinical point of view.9,10
The Scoliosis Research Society (SRS)–Schwab classification system describes the radiographic parameters to group ASD based upon severity, specifically pelvic incidence minus lumbar lordosis (PI-LL), sagittal vertical axis (SVA), and pelvic tilt (PT).11 Many studies have demonstrated that radiographic alignment and sagittal balance significantly correlate with health-related quality of life (HRQOL).9,12–14 After the decision to undergo corrective surgery, while taking into account the patient's pain and disability, analysis of the alignment is mandatory to have optimal and sustainable results. Different radiographic signs define the surgical objectives, but alignment is not considered as an indication for surgery.15
As the sitting position has become the most common posture in today's workplace, identification of differences in regional and segmental changes when transitioning from standing to sitting is important in understanding ASD. Recent studies have shown that the lumbar lordosis angle is decreased by 50% and PT increases by 25% in the sitting position in nondeformity patients; however, changes in other regions of the spine have not been examined.16 With the change in position, the overall mobility can be investigated in groups of patients labeled with ASD. The change in posture compared between ASD patients and those with nonpathologic and nondeformity spines can contribute to the overall understanding of spinal balance and the development of degenerative changes in the spine.17 The goal of this analysis was to assess cervical and thoracic regional and segmental changes in patients with thoracolumbar deformity versus a normative thoracolumbar spine population.
MATERIALS AND METHODS
Data Source
This was a retrospective cohort study of nonconsecutive patients visiting a single academic center for spine-concerning complaints from November 2013 to May 2017. Institutional Review Board approval was obtained prior to study initiation.
Data Collection
Demographic data collected included age, body mass index (BMI), and gender. Each patient underwent biplanar full-body stereographic imaging.
Biplanar Radiographic System and Measurements
Radiographs were captured according to the standardized protocol for imaging with patients in a weight-bearing, free-standing position, arms flexed at 45° with fingers on the clavicles to avoid superimposition with the spine, as well as patients sitting comfortably on a stool, adjusted for the height of the patient, such that the knee and hip were flexed at a 90° angle. Both positions have been shown to maintain the individual's center of gravity.18 The EOS system (EOS Imaging, Paris, France) consists of two x-ray sources for simultaneous acquirement of antero-posterior and lateral images.19 As the two images are acquisitioned, the entire system itself is vertically translated. Images were computed with validated software (Surgimap, Nemaris Inc., New York, New York) at a single center. Sagittal spinopelvic parameters measured for the present analysis included SVA (horizontal distance between plumb line extended from C7 vertebral body and posterosuperior S1 vertebral corner), PI (angle between vertical and line from the center of the bicoxofemoral axis to the midpoint of S1 endplate), LL (angle between upper endplate of L1 the upper endplate of S1), as well as the mismatch between PI and LL (PI-LL), PP (angle between vertical and line from the center of the bicoxofemoral axis to the midpoint of S1 endplate), and thoracic kyphosis (angle between upper endplate of T1 and upper endplate of L1). Cervical alignment parameters measured included: cervical SVA (cSVA: angle between the C2 plumb line and the posterior superior end plate of C7), C2-C7 lordosis (CL: angle between the inferior end plate of C2 and the inferior end plate of C7), and the T1 slope minus CL (TS-CL: angle between the superior endplate of T1 and the horizontal). The segmental changes were recorded from C2 to T12 between standing and sitting radiographs.
Study Inclusion Criteria
Patients included in the present analysis were adults (≥18 years) with nondeformed spines (nondegenerative, nondeformity spinal pathologies) or those with a diagnosis of ASD utilizing SRS-Schwab radiographic criteria (SVA > 4 cm, PI-LL > 10°, or PT > 20°), with available biplanar full-body stereoradiographic imaging (EOS Imaging). Patients with lumbar transitional anatomy or fusions were excluded from the analysis.
SRS-Schwab System
The SRS-Schwab classification of ASD was developed to provide the clinician with a pragmatic approach to categorize radiographic elements of spinal deformity in the adult. The sagittal modifiers of this system include PI-LL, global alignment (SVA), and PT. Radiographic presentation of each of the modifiers signifies the severity of deformity of the adult. The entire propensity-score–matched cohort was then reclassified as follows: nonpathologic or 0 included PI-LL < 10°, SVA < 4cm, and PT < 20°. Moderate spinal deformity or + included 10° < PI-LL < 20°, 4 cm < SVA < 9.5 cm, and 20° < PT < 30° and marked deformity (++) included PI-LL > 20°, SVA > 9.5 cm, and PT > 30°.
Statistical Analyses
Patients were stratified into one of two groups: nondeformity or ASD. To control for differences in age, BMI, and maximum hip osteoarthritis grade (as classified by the radiographic evaluation study by Terjesen and Gunderson20), the two groups were propensity-score matched. This attenuates differences between groups in measured independent variables.11 Means and standardized deviations for continuous variables, as well as frequencies and percentages for categorical variables, assessed overall cohort characteristics such as gender, age, and BMI. Paired Student t tests for continuous variables were used to assess the differences in pelvic, global, and cervical spinal radiographic alignment changes from standing to sitting, as well as for segmental changes in alignment from C2 to T12 within groups. Paired t tests were utilized for the analysis of mobility for both global and segmental changes between groups. A separate analysis was then performed based on SRS-Schwab classification groups. Repeated-measure analysis of variance (ANOVA) tests assessed differences between Schwab modifiers. All statistical analysis was performed using SPSS version 23.0 (IBM, Armonk, New York) and a P value of less than .05 was considered statistically significant.
Age-Adjusted Ideals
An additional separate analysis was performed by stratifying the patients by age, consistent with groupings used previously by Lafage and colleagues in the development of age-adjusted spinopelvic alignment normative values.21 As derived from previously published formulas, age-specific alignment ideals were established for PT, PI-LL, and SVA:


We considered the patient at the age-adjusted alignment ideal if the patient was within a ± 10 -year threshold.21 Included patients, after propensity-score matching (PSM), were stratified by percentile (under: < 25th; normative: 25th to 75th; over: > 75th) for standing, sitting, and difference across nondeformity and ASD groups. Chi-squared and ANOVA tests assessed differences in rates of ideal PT, PI-LL, and SVA alignment as appropriate.
RESULTS
Overall Cohort Characteristics
A total of 338 patients were included in this study, 202 with a nondeformed spine and 136 patients meeting ASD criteria. The average age was 57.61 (SD ± 16.61) years old; 62% of patients were female, and the average BMI was 27.3 (SD ± 6.06).
After PSM, 162 patients were included: 81 nondeformity and 81 ASD categorized patients (61 ± 13 years, 54% female, 28.2 ± 6.2 kg/m2). Maximum and right- and left-hip osteoarthritis (OA) grades were not significant between nondeformity and ASD groups (P > .05), with means of 1.99, 1.35, and 1.34, respectively. The maximum anterior-posterior (AP) Cobb angle, or the angle formed between a line drawn parallel to the superior endplate of one vertebra above the fracture and a line drawn parallel to the inferior endplate of the vertebra, was found to be greater in the ASD group compared to the nondeformity group (17.1 versus 10, P < .001) (Table 1).
Demographic and OA grades across patients groups of nondeformity and ASD classified after propensity-score matching by age and maximum OA grade.
Cohort as Described by the SRS-Schwab Modifier
The average PI-LL for patients within the cohort was 6.04°, with the nondeformity group mean at −7.45° (majority nonpathologic); the ASD group mean was 18.36° (72.31% moderate deformity and 27.9% marked). Between groups, mean SVA was −5.07 cm in the nondeformity group (96.8% nonpathologic), and 40.76 cm in the ASD group (45.6% nonpathologic, 39.7% moderate, and 14.7% marked deformity). Between groups, mean PT was 11.83° in the nondeformity group (91% nonpathologic) and 24.87° in the ASD classified group (28.7% nonpathologic, 44.9% moderately deformed, and 26.5% markedly deformed).
Positional Alignment Changes
The overall differences from standing to sitting in the matched cohort included an increase in PT (+ 10.05°), PI-LL (+ 16.54°), C2-T3 (+ 5.48°), and SVA (+ 38.36 mm). From standing to sitting, there were significant differences in sagittal spinopelvic alignment changes between nondeformity and ASD patients. SVA (49.5 mm versus 27.4 mm, P < .001) and the mismatch between PI and LL (20.12° versus 13.01°, P < .001) had greater angular changes for nondeformity patients than for those with ASD. Across global, pelvic, and cervical alignment changes from standing to sitting within the nondeformity and ASD groups, PT, pelvic incidence (S1P1), thoracic kyphosis, TS-CL, C2-C7, cSVA, C2-T3, and C2 sacral slope (C2SS) were not significant (P > .05) (Table 2).
Pelvic and global spinal alignment changes from standing to sitting after propensity-score matching.
Segmental Changes
The subanalysis included investigation of segmental changes from C2 to T12 from standing to sitting. Nondeformity patients showed significant mobility of the T2-T3 (−0.99° to −0.54°, P = .023), T6-T7 (−3.39° to −2.89°, P = .032), T7-T8 (−2.68° to −2.23°, P = .048), and T10-T11 (0.31° to 0.097°, P = .006) from standing to sitting. ASD patients had significant mobility of the C6-C7 (1.76° to 3.45°, P < .001) and T11-T12 (0.98° to 0.54°, P = .014) (Table 3). The degree of mobility between nondeformity and ASD patients were significant in C6-C7 (−0.18° versus 1.69°, P = .003), T2-T3 (0.45° versus −0.27°, P = .034), and T10-T11 (0.45° versus −0.30°, P = .001) segments. The differences appeared to be mostly at the cervicothoracic and thoracolumbar region, while the midthoracic region was more similar between nondeformity and ASD patients (Table 4).
Segmental changes from C2 to T12 from standing to sitting after propensity-score matching.
Mobility (changes from standing to sitting) comparison between nondeformity patients and ASD patients from standing to sitting.
Differences Based on ASD Severity
Based upon the SRS-Schwab classification of ASD, the PI-LL, SVA, and PT values categorize patients' spines into either nonpathologic (41.3%), moderately deformed (40.6%), or markedly deformed (18.1%). Among the three categories within the study's cohort, PI-LL (19.07° versus 15.62° versus 12.22°, P = .040) and SVA (48.49 mm versus 32.69 mm versus 25.92 mm, P = .007) were the only significant differences in pelvic and global alignment from standing to sitting. For the segmental changes from standing to sitting, there was significance in mobility between the three categories of ASD severity for C6-C7 (0.18 versus 2.12 versus 0.92, P = .039), T2-T3 (0.45 versus −0.08 versus −0.63, P = .020), T6-T7 (0.48 versus 0.36 versus −1.85, P = .007), and T10-T11 (0.45 versus −0.21 versus −0.23, P = .009). Again, the cervicothoracic and thoracolumbar regions were significant between the groups, with greater similarity seen amongst the midthoracic segments (Table 5).
Analysis on change from standing to sitting based on severity of ASD (based upon PI-LL, C7-S1 SVA, and PT).
Effect of ASD on Ideal Alignment
Across patient groups of nondeformity and ASD-classified patients, those who matched their age-adjusted alignment did not have significant differences of sitting to standing. The patients who were under the age-adjusted alignment in the thoracolumbar deformity group had greater PI-LL differences, and fewer PT and SVA differences when compared to the nondeformity group (P < .05) (Table 6).
Assessing differences between ASD and nondeformity patients across ideal age-adjusted alignment goals.
Case Example
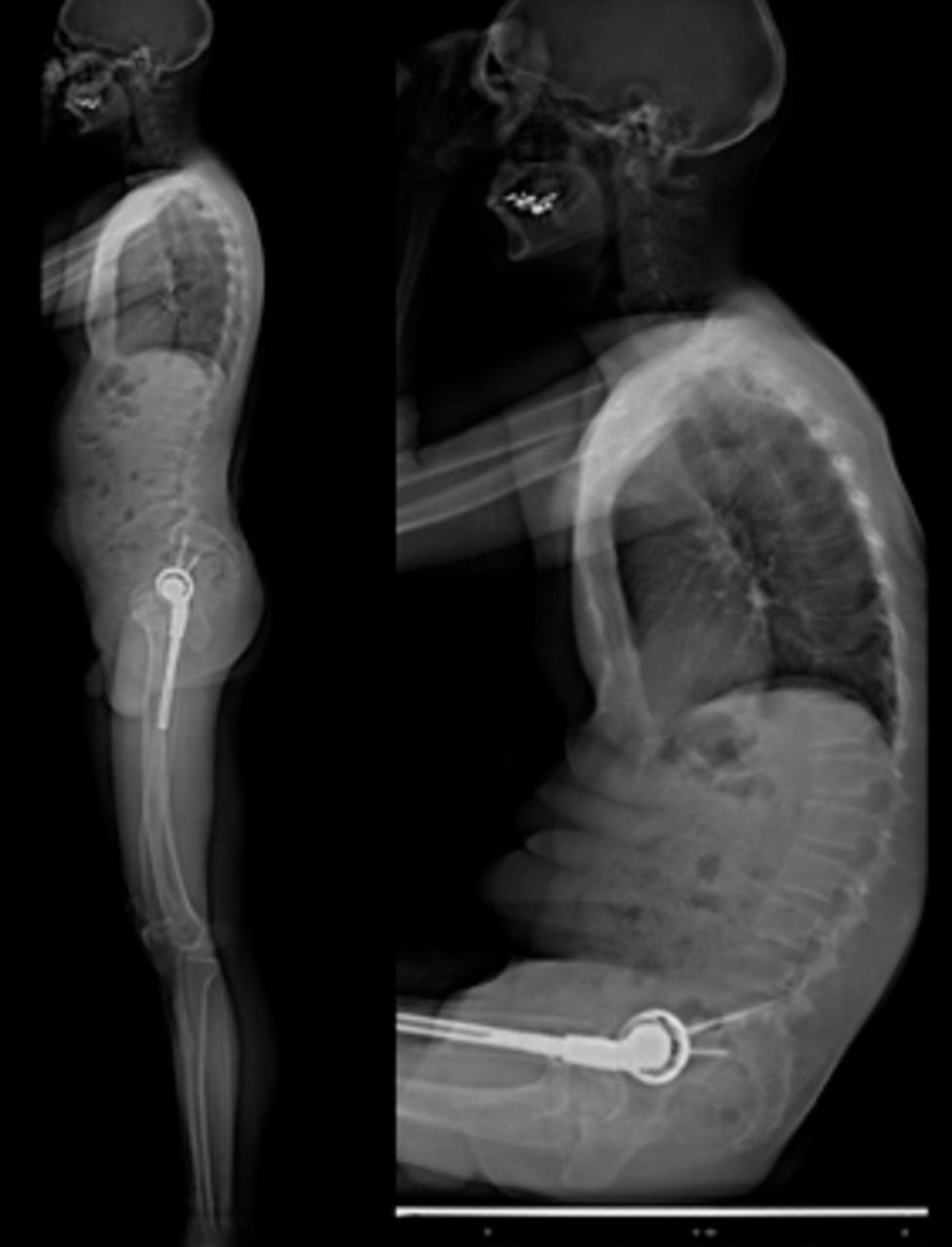
An illustrative case example of a 60-year-old male (45.2 kg/m2) characterized as an ASD patient by the SRS-Schwab modifier classification is presented in Figure 1. Using the SRS-Schwab classification, this patient has a PT grade of +, and PI-LL and SVA grades of ++ at baseline. The patient had positional alignment changes of 14.88° for PT and 3.43° for PI-LL, and an SVA difference of −47.53 mm (Figure 1).

Standing and sitting lateral radiographs of a 60-year-old male characterized as an ASD patient by the SRS-Schwab modifier classification with a pelvic tilt (PT) grade of +, and pelvic incidence minus lumbar lordosis (PI-LL) and sagittal vertical axis (SVA) grades of ++ at baseline. The patient had positional alignment changes from standing to sitting of 14.888 for PT and 3.438 for PI-LL, and an SVA difference of −47.53 mm.
To compare, a case example of a 50-year-old male (20.1 kg/m2) characterized as a nondeformity patient by the SRS-Schwab modifier classification is shown in Figure 2. With this classification, the patient has PT, PI-LL, and SVA grades of 0, or nonpathologic. He had positional alignment changes of 52.76° for PT and 62.43° PI-LL, and an SVA difference of 38.74mm. Between the ASD patient and the nondeformity patient, the segmental differences were 2.60° versus −1.52° for C6-C7, −0.36° versus 1.27° for T2-T3, −0.97° versus 2.30° for T6-T7, and −0.73° versus 1.44° for T10-T11 (Figure 2).

Standing and sitting lateral radiographs of a 50-year-old male (20.1 kg/m2) characterized as a nondeformity patient by the SRS-Schwab modifier classification with pelvic tilt (PT), pelvic incidence minus lumbar lordosis (PI-LL), and sagittal vertical axis (SVA) grade of 0, or nonpathologic at baseline. He had positional alignment changes of 52.76° for PT, 62.43° for PI-LL, and an SVA difference of 38.74 mm.
DISCUSSION
Understanding flexibility of a deformed spine is critical to improving our understanding of the consequences of operative treatment. Prior literature has described a number of compensatory mechanisms associated with the loss of LL in ASD. The pelvis retroverts (as measured by an increase in PT) in effort to hyperextend the hips.22 This is followed by flexion of the knees. Patients may also decrease their thoracic kyphosis—a mechanism called thoracic compensation.23
Nondeformed spines demonstrate substantial changes in alignment with standing to sitting. The pelvis retroverts, lumbar lordosis and thoracic kyphosis decrease, and SVA increases.24 In relation to the nondeformed patients within our present study, deformed patients had less of an increase in SVA, less change in PI-LL mismatch, and less relaxation in lumbar lordosis when analyzing alignment changes from sitting to standing. This was further confirmed by the analysis based on the SRS-Schwab classification of deformity severity – the more severe the deformity, the less the increase in SVA and the less the increase in PI-LL mismatch with positional change of standing to sitting. One explanation for this finding is that ASD patients already have decreased LL and increased SVA in the standing position, thus in order to maintain physiologic balance in the sitting position, they may not need to decrease LL and SVA as much as those with a nondeformed spine. On the other hand, this may represent stiffness in the spine and the inability to relax LL due to arthritic changes; it is unclear if it is a direct or reciprocal effect. Presently, there are no validated measurements to assess overall sitting balance; their development might be useful in further answering this question.
Janjua et al demonstrated that patients who met ASD criteria with baseline thoracic compensation in standing do not significantly increase their thoracic kyphosis with sitting, as opposed to patients without thoracic compensation (nondeformed patients), who do relax their thoracic kyphosis with sitting.25 We demonstrated similar findings in the present study—ASD patients who likely have baseline thoracic compensation in standing demonstrated less ability to segmentally relax thoracic kyphosis.
Interestingly, however, ASD patients segmentally increased their cervical lordosis more than nondeformed patients. Overall, these findings demonstrate that changes with alignment from standing to sitting are focused more in the thoracic spine in nondeformed patients, as demonstrated by decrease in segmental thoracic kyphosis, and more in the cervical spine in ASD patients, as demonstrated by the increase in segmental cervical lordosis. In standing, cervical lordosis has been shown to correlate with HRQOL measures in an ASD population; the influence of these changes in cervical mobility on HRQOL remains to be studied.26
Analyzing the segmental changes from standing to sitting, ASD patients had a greater mobility in C6-C7, while they had significantly less mobility in the T2-T3 and T11-T10 segments. These major differences appear to be mostly at the cervicothoracic and thoracolumbar regions, while the midthoracic region was more similar between nondeformity and ASD patients. This was further verified with the SRS-Schwab classification.
Limitations of this study include a retrospective study design. Second, the relatively small sample size may have limited the power of the study; there may exist additional differences in global and segmental alignment that were not demonstrated in this study. Future investigations may examine an operative cohort to better understand changes in thoracic and cervical alignment after undergoing surgery for ASD.
In conclusion, ASD patients demonstrate diminished mobility in global spinal alignment from standing to sitting as compared to their nondeformed counterparts. Furthermore, ASD patients have diminished segmental relaxation of thoracic kyphosis and increased mobility of segmental cervical lordosis. These findings further our understanding of the relationship of deformity and dynamic alignment, and should be considered when evaluating the impact of deformity correction on unfused segments.
Conclusions
Deformity patients displayed decreased mobility of the spine in the PI-LL and SVA , as well as cervicothoracic and thoracolumbar segment regions compared to patients with nondegenerative and nondeformed spines when moving from standing to sitting. This was also shown across SRS-Schwab classification groups. Future work should investigate these relationships further while taking into account more patient factors.
Footnotes
Disclosures and COI: No funding was received in relation to the creation of this work. Each institution obtained approval from their local Institutional Review Board to enroll patients in the prospective database and informed consent was obtained from each patient. Peter G. Passias, MD, reports personal consulting fees for Spinewave, Zimmer Biomet, and Medicrea outside the submitted work. Virginie Lafage, PhD, reports Depuy Synthes paid lectures, Nuvasive paid lectures, K2M paid lectures, Medtronic paid lectures, and Nemaris board member and shareholder.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2019 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.