


ABSTRACT
Background: The aim of this review is to investigate current uses of fibrinogen as a tool to reduce operative and postoperative blood loss in different surgical fields especially orthopedic spine surgery. This is a systematic review.
Methods: MEDLINE (via Ovid 1946 to June 1, 2020) and Embase (via Ovid 1947 to June 1, 2020) were searched using the keywords “fibrinogen”, “surgery”, and “spine” for relevant studies. The search strategy used text words and relevant indexing to identify articles discussing the use of fibrinogen to control surgical blood loss.
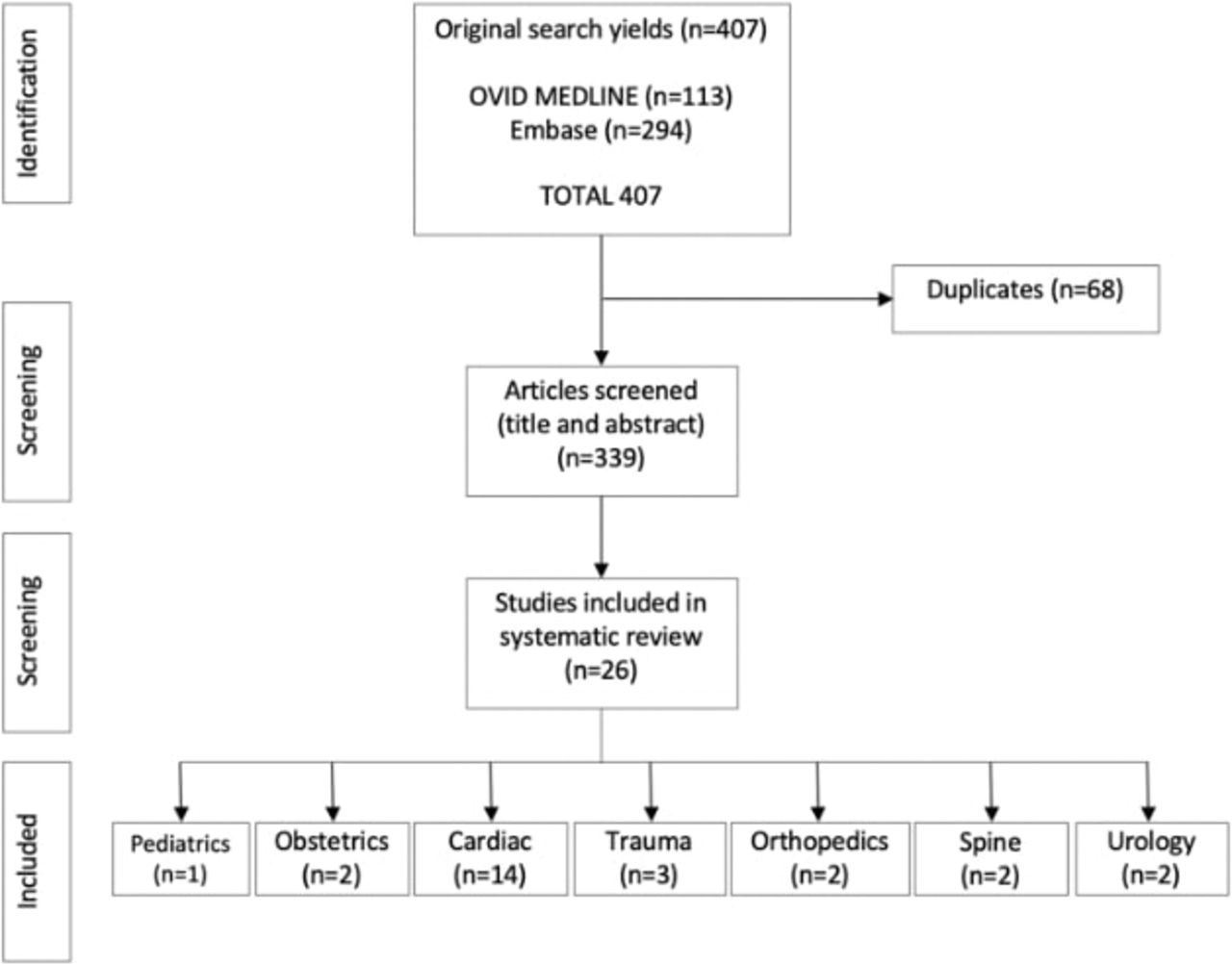
Results: The original literature search yielded 407 articles from which 68 duplications were removed. Three hundred thirty-nine abstracts and titles were screened. Results were separated by surgical specialties.
Conclusions: Multiple studies have looked at the role of fibrinogen for acute bleeding in the operative setting. The current evidence regarding the use of fibrinogen concentrate in spine surgery is promising but limited, even though this is a field with the potential for severe hemorrhage. Further trials are required to understand the utility of fibrinogen concentrate as a first-line therapy in spine surgery and to understand the importance of target fibrinogen levels and subsequent dosing and administration to allow recommendations to be made in this field.
INTRODUCTION
Fibrinogen is an essential protein in the management of bleeding. When hemostatic activation occurs, during the coagulation cascade, thrombin cleaves fibrinogen and hastens fibrin polymerization, which forms a strong network important in clot formation.1 Acute blood loss and volume resuscitation can lead to dilutional coagulopathy and a reduction in fibrinogen levels. In recent literature, fibrinogen is highlighted as a key substrate for managing bleeding in surgical patients.2–6 In this review article, we will study the application of fibrinogen in a variety of surgical settings, with a focus on orthopedic spine surgery.
During major surgery extensive blood loss is frequent. Clot formation is essential in reaching and maintaining hemostasis. Fibrinogen has been found to be the first clotting factor to fall below critical levels during major hemorrhage.7 It is thus evident that fibrinogen levels are invaluable in the hemostasis process and that a deficiency can lead to serious complications during major surgery.
Fibrinogen is a 340 kDa plasma glycoprotein8 with a half-life of 2.7–3.6 days, which is synthesized in the liver.9 It is a substrate of the following enzymes: plasmin, thrombin, and factor XIIIa. During the coagulation cascade, thrombin cleaves the fibrinogen molecule, which gives the soluble fibrin monomer.1 During the initial stage of the clot formation, these monomers create a network that traps red blood cells. This clot is then strengthened by factor XIIIa and the elasticity of the clot and resistance to fibrinolysis is increased.10 Platelet aggregation is also aided by fibrinogen as it acts as a ligand for glycoprotein IIb/IIIa receptors positioned on platelets.11
Fibrinogen levels can fall to critical levels due to numerous variables. Commonly in major hemorrhage and when fibrinogen metabolism exceeds synthesis leading to a reduction in concentration.12 Another way by which hypofibrinogenemia occurs is with hemodilution during volume replacement.13,14 Additionally, colloids can impair polymerization of fibrin.15 This will lead to poor clot quality and will subsequently worsen the hemorrhage. This highlights the reason for optimizing fibrinogen levels preoperatively, perioperatively, and postoperatively.
Normal Fibrinogen Levels
Normal fibrinogen levels are between 150 and 350 mg/dL,16 and studies have shown that hypofibrinogenemia increases the risk of perioperative bleeding in different types of surgery. Previous literature suggests 100 mg/dL as the threshold for administering fibrinogen in patients with congenital fibrinogen deficiency.17
Management strategies for fibrinogen deficiency due to major hemorrhage and dilution effects are still primitive. Studies have shown that a serum fibrinogen level above 200 mg/dL is required for fibrinogen to function optimally.18 It has been found that fibrinogen can in fact increase with age and varies within different age groups.19 This suggests that fibrinogen supplementation must be personalized.
Fibrinogen Preparation and Administration
Fibrinogen is produced from human plasma and converted to lyophilized powder. During this preparation process, the product is pasteurized and viruses inactivated.3 This procedure also removes antibodies and antigens making it a safe product by preventing potential immunological and allergic reactions. The safety of fibrinogen administration is increased by the fact that it does not require blood type screening before use and can be stored at room temperature allowing fast use.3,6
Administration of cryoprecipitate is the most common way to supplement a patient with fibrinogen. This method is used in North America and in the United Kingdom, with other countries using lyophilized fibrinogen concentrates instead.6 Dosing of fibrinogen can be personalized depending on the severity of the bleeding and plasma fibrinogen concentration preoperatively. However, in an acute setting, it has been recommended to use 1–2 g with the opportunity to administer more if needed.6,20 Larger doses, up to 8 g are also safe to administer in severe cases.15 The dose can be calculated as follows:
Fibrinogen concentrate dose (g) = desired increase in plasma fibrinogen level (g L) × plasma volume (L)
Fibrinogen concentration can be measured very swiftly using thromboelastometry (ROTEM device, TEM International, Munich, Germany) or thrombelastography.21 This allows physicians to assess the patient fibrinogen levels during a procedure and thus enable immediate intervention with fibrinogen supplementation if required. The device used to measure the fibrinogen level (ROTEM device) can even establish the concentration of fibrinogen is needed.6
METHODS
A systematic review of the literature was conducted in line with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Figure 1). The search was performed in both MEDLINE (via Ovid 1946 to June 1, 2020) and Embase (via Ovid 1947 to June 1, 2020). Search terms included subject headings specific to the relevant databases. The search strategy included the use of the keywords: “fibrinogen”, “surgery”, “spine”, and “bleeding”. The initial search yielded 407 articles published any time before June 2020; after removal of duplicates, 338 articles were screened by 2 reviewers, BB and PM. After review, 26 were assigned a level of evidence according to Oxford Centre for Evidence-Based Medicine 2009 Guidelines and included in the final article (Table 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) table; search methodology.
Overview of clinical studies detailing fibrinogen concentrate administration.
Inclusion criteria included application of fibrinogen in surgery and data collected included the study methodology, dose of fibrinogen administered, timing of administration, and qualitative effect on bleeding. If other publications were noted during the screening of reference lists, they were also added. Due to the heterogeneity of the data and variability in the experimental study methods, it was not possible to conduct a statistical analysis. For this reason, a comprehensive review of the clinical application of fibrinogen in surgery is presented.
RESULTS
The systematic review conducted resulted in 407 articles. After the removal of duplicates, 339 articles were screened based on their title and abstract. Subsequently, 26 articles were found to be relevant based on the inclusion criteria (Figure 1). Following this, the manuscripts were divided into the following surgical categories: pediatrics (n = 1), obstetrics (n = 2), cardiac (n = 14), trauma (n = 3), orthopedics (n = 2), spine (n = 2), and urology (n = 2).
Pediatric Surgery
Blood loss in major pediatric surgery is associated with high risk for morbidity and mortality. These surgeries frequently require transfusion of allogeneic blood products. There is robust evidence that side effects related to blood transfusions are associated with increased morbidity and mortality especially in children.46 The European Society of Anesthesiology guidelines recommend fibrinogen concentrate as the management of perioperative bleeding in acquired hypofibrinogenemia.47 Fibrinogen concentrates represent a possible technique for increasing hemostatic competence and reducing reliance on allogeneic blood products.
A study performed on pediatric major craniosynostosis surgery showed that transfusion requirements could be reduced significantly by using fibrinogen concentrate.22 There is also a case report of a 7-year-old child who sustained major abdominal and pelvic injuries in which fibrinogen concentrate had a major role in achieving successful management.48 Additionally, a comparative randomized study of 63 pediatric patients underwent cardiac surgery treated with fibrinogen concentrate or cryoprecipitate in which fibrinogen concentrate was shown to be a valuable option for controlling bleeding and avoiding transfusion in pediatric cardiac surgery patients.49 An observational study of children with severe acquired hypofibrinogenemia during chemotherapy for acute lymphoblastic leukemia supplemented by fibrinogen concentrate at an adequate dosage and in selected cases suggested reduction of the risk of transmission of viral infection and better outcome.50
Obstetrics
Postpartum hemorrhage is a major cause of maternal morbidity and mortality worldwide. Physical causes such as uterine atony and placental complications if associated with hemostatic impairment can lead to consumptive and dilutional coagulopathies. This can result in life-threatening bleeding requiring rapid volume resuscitation and allogeneic blood transfusion.
A case series of postpartum hemorrhage showed an additive effect of fibrinogen concentrate associated with conventional treatments for obstetric hemorrhage associated with hyperfibrinogenemia secondary to dilutional and consumptive coagulopathies.24 These findings support that fibrinogen concentrate infusion has a role in controlling obstetric hemorrhage. A randomized clinical trial investigated the use of fibrinogen concentrate in acute postpartum hemorrhage in 249 randomly assigned subjects. They studied the effect of early empirical administration of fibrinogen concentrate on blood transfusion in postpartum hemorrhage and concluded that preemptive administration of fibrinogen concentrate did not reduce red blood cell transfusion in patients with normal fibrinogen levels.23 A retrospective analysis comparing fibrinogen concentrate usage in 36 patients with acquired hyperfibrinogenemia to 64 patients who received cryoprecipitate was conducted. This study supported the use of fibrinogen concentrate and showed superiority in comparison with cryoprecipitate in relation safety and overall benefit.51 Multiple large randomized double-blind placebo controlled trials are ongoing to provide evidence on the efficacy, safety, and feasibility of fibrinogen concentrate during acute bleeding in postpartum hemorrhage.52,53
Cardiac Surgery
Complex cardiovascular surgeries often requires blood transfusion perioperatively and postoperatively. Although blood components are considered safe, it may be associated with serious adverse effects.54,55 Thus, alternative options to reduce blood transfusion are desirable.
A prospective randomized controlled trial of 61 patients was conducted where elective thoracic or thoracoabdominal aortic replacement surgery involving cardiopulmonary bypass (randomized into 2 groups—managed with fibrinogen concentrate or placebo) showed significant reduction of blood products transfusion in the treatment group.34 Another randomized controlled study showed fibrinogen concentrate as targeted first-line hemostatic therapy in aortic surgery significantly provides short-lived increases in plasma fibrinogen and fibrin-based clotting after aortic surgery.56 Shams et al25 have also demonstrated a similar increase in fibrinogen levels and improved clot stability without having an effect on platelet aggregation. In a prospective pilot study including 20 patients who underwent elective coronary artery bypass graft surgery, prophylactic fibrinogen infusion significantly reduced postoperative blood loss and helped maintain hemoglobin levels.6 Other prospective and retrospective studies have also supported the administration of fibrinogen concentrate during cardiovascular surgery and are associated with the reduction in blood transfusion and incidence of postoperative bleeding.5,6,28,57 This reduction in bleeding is more significant in patients with underlying hypofibrinogenemia33 specifically at a fibrinogen level that is less than 100–130 mg/dL.31 Most studies look at intraoperative administration, but as described by Sadeghi et al,36 preoperative administration seems to have a similar effect. Administration of 1 g of fibrinogen seems to be an insufficient amount. As described by Lupu et al,26 this dose does not stop bleeding and does not reduce the need for transfusion. Although fibrinogen administration seems safe, Jahangirifard et al29 observed an increased risk of postoperative acute kidney injury after its administration.
Trauma
Trauma is one of the leading causes of death for individuals up to the age of 45 years worldwide.58 Hemorrhage is responsible for up to 40% of deaths related to trauma and is considered the leading preventable cause in this setting.59 Massive hemorrhage can result in a coagulopathy leading to hypofibrinogenemia, which can subsequently extend to tissue damage. Initial volume resuscitation with fluid causes dilution of coagulation factors.2 In addition, acidosis and hypothermia associated with massive bleeding play a major role in fibrinogenolysis and fibrinogen synthesis inhibition.60 As a result, fibrinogen replacement is important in these circumstances to restore baseline hemostasis.61,62
Several clinical reports have shown the potency of using fibrinogen concentrate along with antifibrinolytic medication to correct trauma-related coagulopathy and restore hemostasis without the need for transfusion of either platelets or fresh frozen plasma.20,38 Various studies composed of large numbers of traumatic patients described the applicability and use of fibrinogen concentrate and/or prothrombin complex concentrate in correcting coagulopathy. They showed reduction in the requirement of blood and platelet transfusion while improving survival rates in comparison with receiving fresh frozen plasma.20,38,63
A retrospective study enrolled 435 patients divided into 2 groups (treated with fibrinogen concentrate in the first 24 hours of arrival to hospital and control group) showed no significant difference in plasma fibrinogen concentration up to 7 days posttrauma.64 On the other hand, a randomized trial of 50 patients demonstrated that the infusion of fibrinogen concentrate within 1 hour of arrival to hospital in the case of trauma in patients at risk of significant hemorrhage is feasible, fast, and improves plasma fibrinogen levels considerably.65
A number of randomized controlled trials taking place internationally in multiple centers such as the RETIC trial, STATA trial, FiiRST, E-FIT1, and PRooF-iTH are currently investigating the use of factor concentrates in traumatic hemorrhage.66 These trials will certainly help in addressing significant shortage in the evidence regarding the use/role of fibrinogen concentrate in severe trauma.
Urology
Radical cystectomy and prostatectomy are urologic procedures with a significant bleeding potential,67,68 and administration of fibrinogen in the perioperative setting is a therapeutic option used in many centres based on limited evidence and contradictory results.
Soleimani et al44 did not see a hemostatic advantage from administering 2 g of fibrinogen to patients undergoing prostate surgery. Fenger-Eriksen et al45 noticed improved hemostasis and decreased bleeding when administering a dose of 45 mg per kg during cystectomy.
Orthopedics
Orthopedic surgeries are often associated with severe hemorrhage due to impaired coagulation system and poor hemostasis intraoperatively. A randomized controlled trial looking at the prophylactic administration of fibrinogen in the perioperative period of a total hip arthroplasty was conducted by Najafi et al39 where 30 patients were either given fibrinogen concentrate or placebo. The 2 groups had similar preoperative fibrinogen, hemoglobin, and platelet levels. The prophylactic administration of fibrinogen concentration was found to be safe and effective in lowering the bleeding perioperatively during total hip arthroplasty surgery.39 A prospective study looking at 66 major orthopedic surgery patients who randomly received volume resuscitation with modified gelatin solution, hydroxyethyl starch, or Ringer lactate showed that fibrinogen concentration supplementation can reverse the effects of intravascular volume therapy and promote hemostasis.4
Spine Surgery
Spine surgery is associated with high rates of hemorrhage intraoperatively and postoperatively.21 This leads to depletion of coagulation factors. Treatment with high volumes of fluid replacement can give rise to dilutional coagulopathy and weakened fibrin formation. A prospective study looking at the prophylactic administration of fibrinogen in posterior spinal fusion surgery was assessed by Pournajafian et al41 where 41 patients were randomly assigned to the intervention of 1-g fibrinogen infusion preoperatively versus placebo. They found the need for blood transfusion was significantly higher in the control group suggesting that the prophylactic infusion of fibrinogen in posterior spinal fusion surgery may decrease intraopertive and postoperative bleeding and blood transfusion requirement.41 Javaherforoosh et al42 observed that 1 g of fibrinogen administered at time of incision to patients undergoing lumbar spine surgery also significantly decreased the need for blood products transfusion. Carling et al43 suggest that measuring the preoperative fibrinogen plasma concentration can identify spinal fusion patients with an increased risk of excessive perioperative bleeding. The limited literature on fibrinogen in spine surgery suggests that 1 g of fibrinogen administered 5 minutes after induction provides a hemostastic benefit and reduces postoperative bleeding. There is nonetheless no consensus on the timing of the administration and the correlation with the plasma fibrinogen levels. Studies in other surgical disciplines have demonstrated similar hemostastic benefits and safety of fibrinogen when administered preoperatively or intraoperatively at doses between 2 and 8 g. It remains unknown whether these findings can be translated to the field of spine surgery.
CONCLUSIONS
Fibrinogen plays a crucial role in the management of acute hemorrhage and remains an area of recent interest. A low level of fibrinogen leads to various complications such as low clot strength and coagulopathies. Fibrinogen administration has been shown to be safer than allogenic blood product administration, and multiple studies in different disciplines have described hemostatic benefits and decreased intraoperative and postoperative blood loss. In addition, the ability to administer it almost immediately makes it an extremely useful therapy to have at your disposal.
The field of orthopedic surgery, more specifically spine surgery, is an area with a high risk of important hemorrhage that requires a great deal more research in regards to fibrinogen therapy. Pournajafian et al41 has shown promising hemostatic benefits of intraoperative fibrinogen administration. Multiple authors have made similar observations across different surgical fields. Administration of 1 g of fibrinogen has been demonstrated to be safe and effective by Pournajafian et al,41 but some authors describe similar findings for doses up to 8 g. Further trials are required to understand the utility of fibrinogen concentrate as a first-line therapy in spine surgery and also to understand the importance of target fibrinogen levels and subsequent dosing and administration to allow recommendations to be made in this field.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
- 1 .↵
- 2 .↵
- 3 .↵
- 4 .↵
- 5 .↵
- 6 .↵
- 7 .↵
- 8 .↵
- 9 .↵
- 10 .↵
- 11 .↵
- 12 .↵
- 13 .↵
- 14 .↵
- 15 .↵
- 16 .↵
- 17 .↵
- 18 .↵
- 19 .↵
- 20 .↵
- 21 .↵
- 22 .↵
- 23 .↵
- 24 .↵
- 25 .↵
- 26 .↵
- 27 .
- 28 .↵
- 29 .↵
- 30 .
- 31 .↵
- 32 .
- 33 .↵
- 34 .↵
- 35 .
- 36 .↵
- 37 .
- 38 .↵
- 39 .↵
- 40 .
- 41 .↵
- 42 .↵
- 43 .↵
- 44 .↵
- 45 .↵
- 46 .↵
- 47 .↵
- 48 .↵
- 49 .↵
- 50 .↵
- 51 .↵
- 52 .↵
- 53 .↵
- 54 .↵
- 55 .↵
- 56 .↵
- 57 .↵
- 58 .↵
- 59 .↵
- 60 .↵
- 61 .↵
- 62 .↵
- 63 .↵
- 64 .↵
- 65 .↵
- 66 .↵
- 67 .↵
- 68 .↵
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.