


Abstract
Background Patients with epilepsy have a higher risk of skeletal injuries, and some of these fractures occur in the spine during a seizure. Seizure-induced spinal fractures (SISF) are unusual injuries that typically occur in the thoracolumbar spine. Because these skeletal injuries are not well described in the literature, this article aims to analyze the characteristics of this uncommon clinical entity.
Methods A PubMed and Scopus search adhering to preferred reporting items for systematic reviews and meta-analyses guidelines was performed to include studies reporting patients with SISF. The data gathered from this review were analyzed to characterize this condition.
Results The search yielded 34 articles with a total of 38 patients with SISF. All studies were case reports (level 5 evidence). Most fractures occurred in the thoracic and lumbar spine, and the most common injuries were type A1 and A4 fractures according to the AO spine classification system. Different characteristics of SISF are described including demographics, clinical findings, imaging, and treatment.
Conclusions SISF should be ruled out in patients who have a recent history of seizures and who report persistent dorsolumbar pain or neurological deficit. SISF usually occurs in the thoracolumbar spine and less frequently in the cervical spine. This review shows that different patterns of neurological deficits, some of them severe, may occur in approximately a quarter of patients with SISF.
Clinical Relevance This study provides awareness of an uncommon spine condition. Physicians should suspect SISF in patients with persistent dorsolumbar pain after a seizure.
- seizure-induced spinal fractures
- spinal fractures related to convulsions
- vertebral compression fractures
- fractures related to seizures
- fractures related to epilepsy
Introduction
Patients with epilepsy are prone to multiple types of bone fractures.1,2 These injuries can occur either directly as a result of the violent force of a seizure or may occur secondary to falling at the time of the episode. A wide variety of fractures and dislocations have been described associated with convulsive events. Seizures mainly induce fractures of the humerus, scapula, hip, and spine. Previous studies showed that the incidence of fractures after seizures was 0.3% ,3 and the incidence of spinal fractures induced by seizures was 0.04%.1
Seizure-induced spinal fractures (SISF) are not well described in the literature; thus, our goal was to describe the characteristics of this uncommon condition.
Methods
Study Selection
A comprehensive literature search of PubMed and Scopus was performed in accordance with preferred reporting items for systematic reviews and meta-analyses guidelines. Also, a search was performed on Google scholar to identify articles not reported in PubMed or Scopus. The search for publications was undertaken using the following keywords: “seizure-induced spine fractures,” “seizure-induced vertebral fractures,” “convulsion spine fracture,” and “spine fracture related to seizure.” The search extended to all available English language articles from 1970 to February 2021. Articles were reviewed by 2 of the study authors (L.A.R. and A.G.M.), who performed title and abstract reviews separately. Titles and abstracts were initially reviewed to identify articles with positive exclusion criteria. For those abstracts that met the inclusion criteria, the full text was retrieved and reviewed by the authors. Furthermore, the references for all search-selected manuscripts were also reviewed for potential cases.
Inclusion and Exclusion Criteria
Cases were included in the final review only if patients had SISF corroborated by radiographic studies and the article showed adequate clinical and radiological information. The following articles were excluded: literature reviews, animal studies, correspondence or letters, articles not available in full text, articles reporting different pathologies to SISF, vertebral fractures not related to seizures, and articles with incomplete clinical information.
Data Extraction
The following data were extracted from eligible cases: (1) age and gender, (2) symptoms, (3) cause of seizures, (4) previous use of antiepileptic drugs, (5) number of seizures previous to fracture, (6) location of spinal fracture, (7) time from fracture to diagnosis, (8) presence of osteoporosis, (9) associated conditions or injuries, (10) treatment, and (11) outcome.
Radiological studies were analyzed to confirm the presence of SISF. Imaging methods included x-ray, computed tomography, and magnetic resonance images. Descriptions of thoracolumbar fractures were made according to the AO spine injury classification system.4
The presence of bone density anomalies was sought in patients who underwent a bone density test, especially dual-energy x-ray absorptiometry (DEXA). Osteopenia was considered when the T score was between −1.0 and −2.5, and osteoporosis was diagnosed when the T score was −2.5 or below.
Results
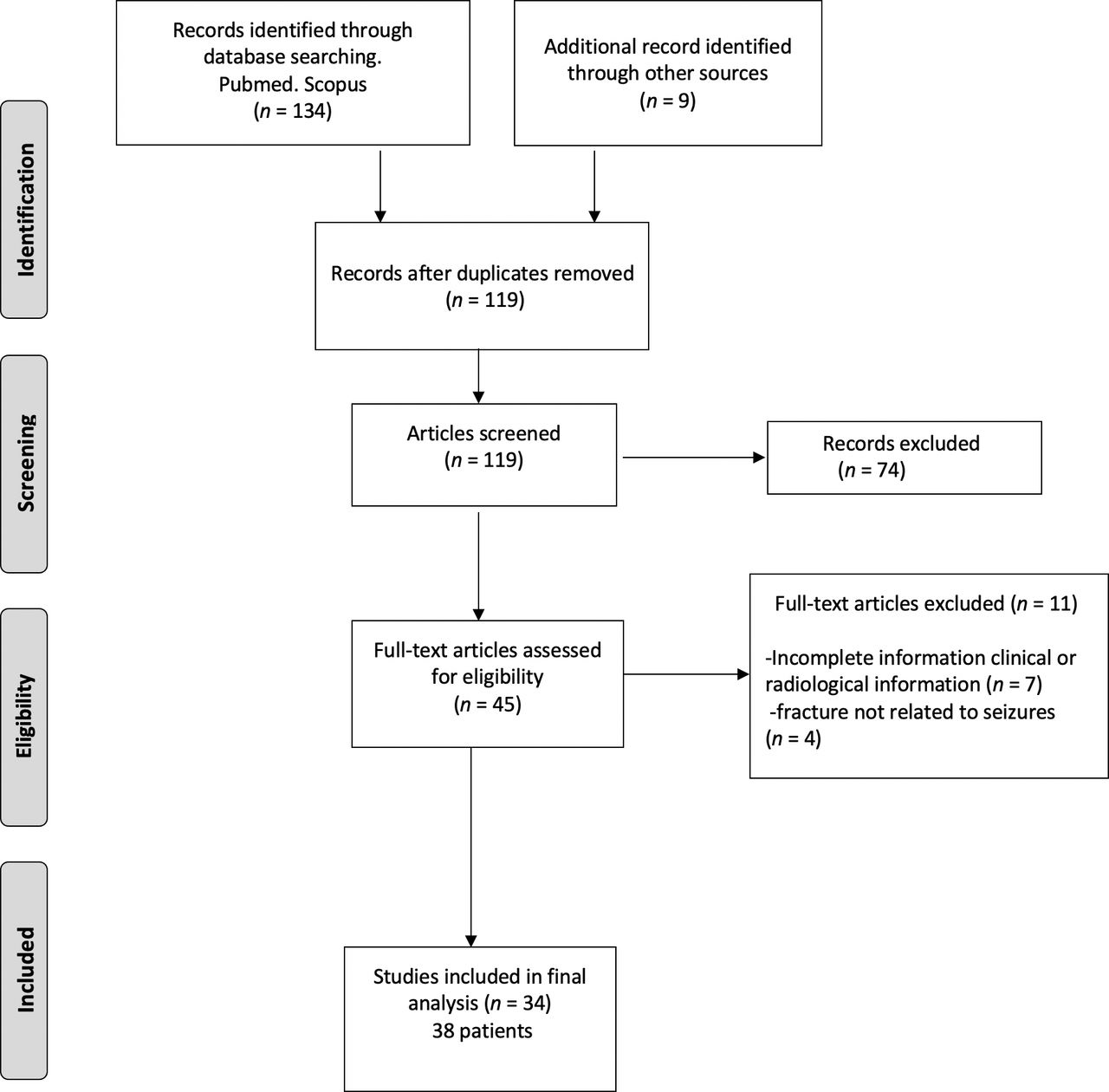
The initial literature search yielded 134 articles. Nine articles reporting cases included for analysis were obtained from Google scholar. After the removal of duplicates, the title and abstract of 119 articles were screened and, based on exclusion criteria, 74 articles were eliminated. After this initial filter, 45 articles were assessed for eligibility, of which 11 were excluded for different reasons. Thus, 34 studies with a total of 38 patients were eligible for analysis (Figure 1). The Table shows the characteristics of these 38 patients with SISFs who were identified from previous publications.1,5–37 All included articles were case reports, and according to the Oxford Center for Evidence-Based Medicine table, they were labeled as level V studies. Not all articles provided information about each item; therefore, a comparative analysis was limited by the nature of the source data. Statistical analysis was not conducted for this review because comparative analyses could not be performed.
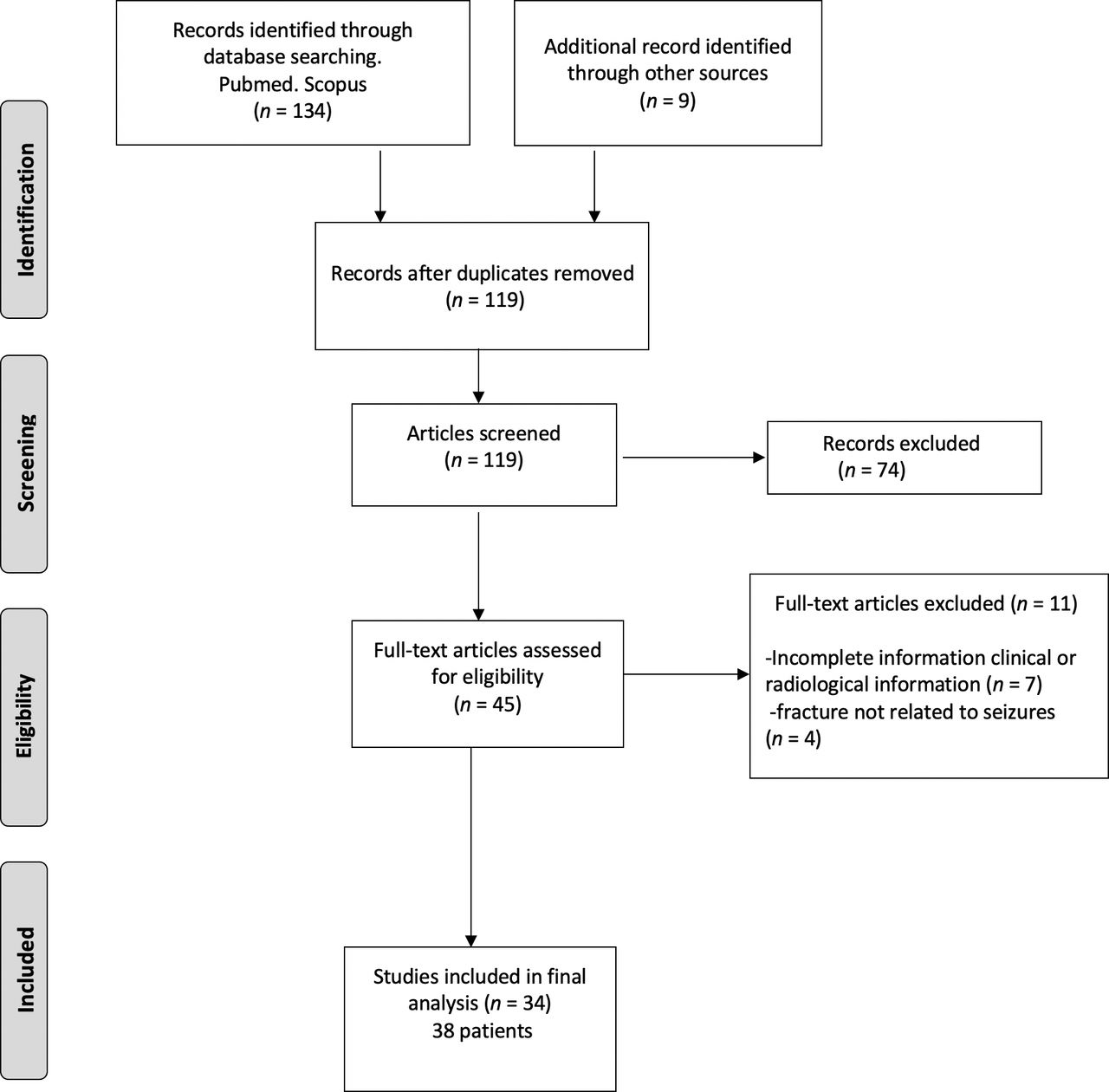
Flow chart of the literature search strategy and article selection for screening and analysis.
Summary of patients with seizure-induced spinal fractures.
Patient Demographics
The youngest patient was 11 years old, and the oldest was 75 years old. The average age was 40 years. Fifty-five percent of cases occurred among individuals in the fourth and fifth decades of life. Seventy-three percent of patients were men.
Clinical Manifestations
The most common symptom observed was local pain depending on the fracture’s location. Local pain was observed in every patient with cervical and thoracolumbar fractures. Twenty-six percent of patients experienced a motor deficit in the lower limbs, and some of them presented with cauda equina syndrome.
Causes of Seizures
The most common cause of seizures in these patients was idiopathic epilepsy; less common causes of seizures were brain tumors, medication overdoses, and others.
Location and Type of Fractures
The most common type of fractures was A1 and A4. SISF may be observed on any level of the thoracolumbar spine, being L1 and L2 the most common sites of injury. In 4 patients, the fracture was located in the cervical spine.
Bone Density Status
DEXA was performed in only 10 patients (26%) in this study. The presence of osteoporosis, osteopenia, and normal results was equally distributed in these cases.
Treatment and Outcome
All patients who manifested with only local pain achieved a good outcome, regardless if they were treated with surgery or conservatively. Treatment was tailored according to the severity of the fracture, wedge-compression fractures were treated conservatively, and burst fractures were usually treated with surgery. All patients with cervical fractures were treated with surgery. Patients with motor deficits showed partial improvement at follow-up.
Discussion
Epileptic seizures are relatively common, affecting approximately 0.2%–0.5% of the general population.21 Bone fractures in epileptic patients may be related to trauma either induced directly by a convulsion or resulting from a fall or other accident resulting from the seizure. In the absence of external trauma, it is reported that the mechanism of vertebral fracture is by the powerful contraction of the paraspinal muscles during a seizure.
This study presents a comprehensive systematic review of patients with SISF. In the following paragraphs, data obtained from this review and other sources are summarized to describe the characteristics observed in patients with SISF.
Demographics
Previous studies showed an incidence of 0.3% of skeletal fractures in cases of tonic-clonic seizures and an incidence of 0.04% of spinal fractures.1 Literature suggests that SISF may be underreported, especially those patients with mild or minimal symptoms.
A previous study reported that a rate of 15% of vertebral compression fractures in epileptic patients with no history of trauma or back pain.2 In this review, it was observed that SISF may occur at any age and for unknown reasons, a 3:1 ratio favoring men was observed. There was a variety of causes of seizures in this study, with idiopathic epilepsy the most common cause, followed by medication overdose, brain tumors, hypoglycemia, and others.
Clinical Presentation
The most common clinical manifestation observed in this review was local pain in the area of the fractured vertebra, which is why radiological studies were indicated in these patients. Continuous local pain at the fractured spinal site was observed in each case in this review. The presence of neurological deficit has been reported in a few cases of SISF. In this review, almost 30% of patients experienced some type of neurological deficit, including sensory deficit, cauda equina syndrome, paraparesis, quadriparesis, paraplegia, and quadriplegia. As expected, patients with more severe fractures were those who presented with neurological manifestations.
Most patients were diagnosed with SISF on the same day of the epileptic event; however, in some patients, the diagnosis of the fracture occurred in a delayed fashion. In some cases, when the seizure was unwitnessed, especially during the night, the presence of continuous and unexplained local pain was the motive to order imaging tests and diagnose these injuries. In this study, SISF occurred after a single convulsive event in 85% of cases, and the fracture was related to multiple seizures in 15% of cases.
Location and Type of SISF
The most common location of SISF reported in the literature is the upper and midthoracic spine.29 During a seizure, the muscles of the neck, abdomen, pelvis, and back contract violently. During contraction of the muscles, these forces are concentrated along the anterior and middle columns of the midthoracic kyphotic curve; thus, these injuries are more frequent in this area.1
In this review, the most common site of SISF was observed in the upper lumbar spine (L1-L3), occurring in 50% of cases. Fractures located in the midthoracic region (T5-T8) were the second most common location and were present in 35% of patients. Fractures located in different areas of the spine were observed in a lower percentage. In 4 patients, the fracture was located in the cervical spine, including 2 injuries at C2 (odontoid type II and hangman fractures).
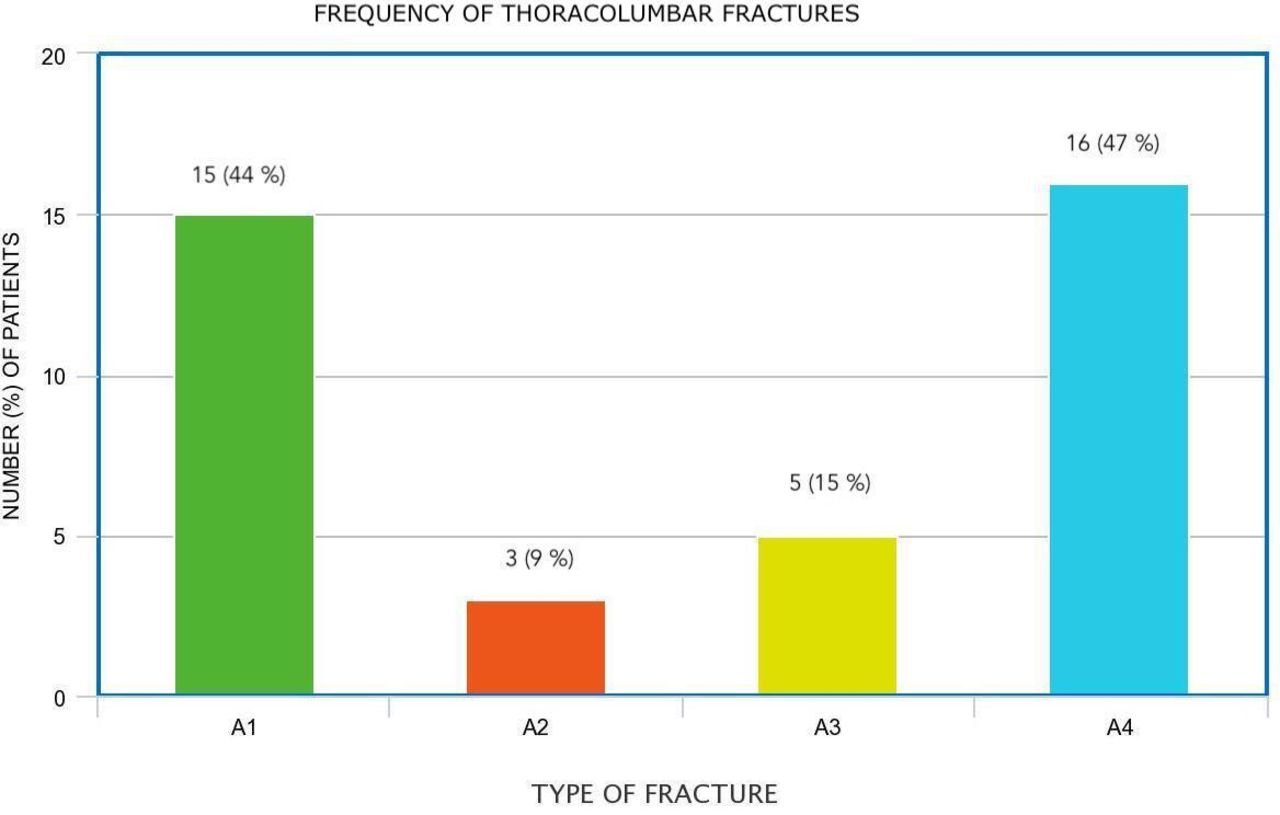
Ninety percent of the fractures observed were located in the thoracolumbar spine. All thoracolumbar SISFs reported in this review were compression fractures. Forty-four percent of cases were wedge-compression fractures (A1) and burst fractures (A4), which were observed in 47% of cases. Less common fractures were split fractures (A2) and incomplete burst fractures (A3). Figure 2 shows the frequency of thoracolumbar fractures observed in this study. Some patients with multiple fractures presented with a different type of fractures at different levels.
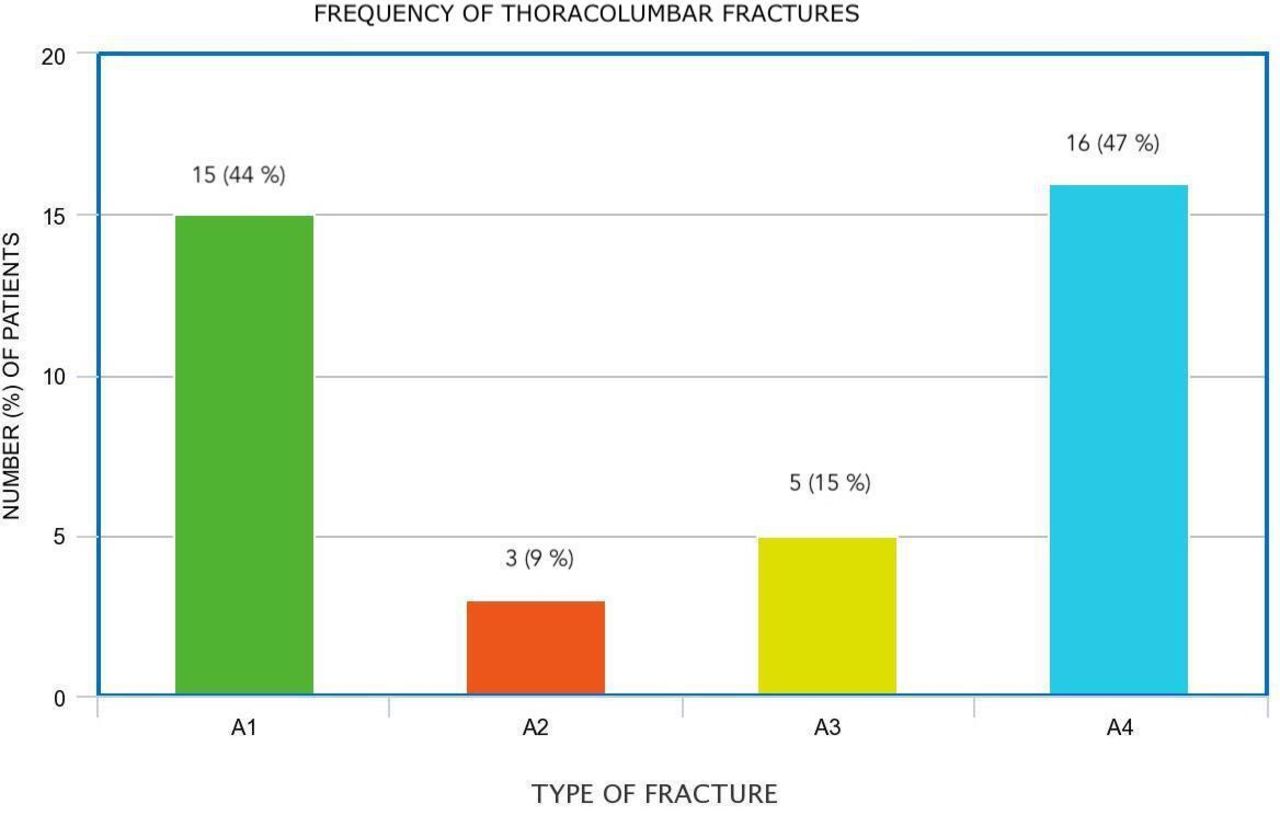
Bar chart showing the frequency of types of thoracolumbar fractures observed in this review. Different fracture patterns were observed in the same patient.
The results observed in this review are somewhat different from what has been reported in the literature, where it is mentioned that fractures in the midthoracic spine are the most common site of SISF. This finding may be the result of the fact that compression fractures occurring in the thoracic spine are usually minor, thus leading to underreporting of these injuries.
Presence of Low Bone Density
People with epilepsy have a 2–6 times greater risk of fractures than the general population, with a particularly higher incidence of fractures of the vertebral bodies and femoral neck.38 In recent years, there has been increasing evidence suggesting that epilepsy and its treatment can have adverse effects on bone mineralization and calcium metabolism.39 Different studies have shown a significant reduction in bone mineral density and an increased fracture risk in patients treated with valproate and enzyme-inducing antiepileptics, such as phenobarbital, carbamazepine, and phenytoin.39–41 Another study reported that although a deficit in bone mineral density is observed in patients with epilepsy, this is too small to explain the increase in fracture risk observed in these patients, and it was concluded that the increased risk of fractures may be linked to seizures.42
In this review, 82% of patients were not taking anticonvulsants when the vertebral fracture occurred. This finding suggests that the use of these medications likely did not have any influence on the occurrence of SISF. DEXA was performed in only 26% of patients in this review, showing a very similar incidence of findings of osteopenia, osteoporosis, and normal results. Of all patients who showed osteoporosis and osteopenia on DEXA, none of them were taking anticonvulsants. DEXA was performed on only 2 patients who were taking anticonvulsants, and this test was normal in both cases.
Although this is a very low number of patients, these results suggest that the decrease of bone mineral density was not secondary to the use of antiepileptics. However, the presence of low bone density observed in some patients in whom DEXA was performed may indicate that pre-existent low bone density caused by different factors may have had a role in the development of SISF.
Associated Injuries and Conditions
The most common musculoskeletal injuries seen after tonic-clonic seizures include thoracolumbar fractures, humeral head fractures and dislocations, manubriosternal joint disruption, and femoral neck, pelvic, acetabular, and scapular fractures.20 The presence of simultaneous skeletal injuries in different areas is seldom reported in the literature. In this review, almost 20% of patients showed fractures in other anatomic areas, including scapular fractures, humerus fractures, and shoulder dislocation. The patient with more associated fractures experienced a sternal fracture, bilateral humerus fractures, and femur fracture.10 Other nontraumatic conditions observed in these cases included brain tumors, depression, type 1 diabetes, rheumatoid arthritis, lupus, and schizophrenia.
Treatment and Outcome
The treatment of SISF was based on the characteristics of each fracture. The treatment of these skeletal injuries was basically the same as that used to treat spinal fractures from other causes. In this review, because most patients were collected from case reports, the treatment strategy was carried out according to the preferences of each surgeon and was generally based on the previously established management of spinal fractures.
Depending on the type of cervical injury, these patients were treated with different techniques, including anterior C2 screw for an odontoid fracture, occipitocervical fusion for a hangman type fracture, and cervical fusion for subaxial injuries.
Most patients with thoracolumbar wedge-compression (A1) fractures were treated conservatively with a brace and medical treatment. Patients with split fractures (A2) were treated either with surgical stabilization or conservative treatment, and surgical treatment included posterior stabilization. Cases of incomplete burst fractures (A3) were treated either with conservative treatment or surgery; surgical stabilization was performed through an anterior approach in these patients. Finally, all patients with burst fractures (A4) underwent different types of surgical stabilization and decompression, being posterior instrumentation and laminectomies the most common surgical procedure.
In general, our findings were very similar to what is reported in the management of fractures from other causes, especially traumatic injuries. The outcome was reported with different periods of follow-up, some of them very short; therefore, it is not possible to report reliable outcomes.
Limitations
Although this study shows relevant information about SISF, it has some limitations. All of these patients were extracted from case reports; therefore, they are subject to reporting and description bias. In addition, only English language articles were included for review and therefore articles published in a different idiom could have been excluded. We also believe that SISF is underreported, especially in cases of fractures causing minor symptoms. Despite these limitations, this review summarizes all the accessible pertinent cases and gives insights into this special disease.
Conclusions
SISF is an uncommon event observed usually in the thoracolumbar spine. Persistent local pain at the fractured area is a constant symptom in these cases. Type A1 and A4 injuries localized in the thoracolumbar area were the most common fractures observed in this study. The results of this study show that the management of these fractures is similar to the treatment of vertebral fractures caused by other pathologies.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.