


Abstract
Background Cervical pedicle screw fixation provides a biomechanically superior fixation in comparison to traditional lateral mass screws. The traditional open technique has limited adoption due to technical challenges and significantly increased wound morbidity. Navigated, percutaneous pedicle screw fixation circumvents the traditional technical challenges and minimizes wound morbidity. We present here a technique description and case report of navigated, percutaneous posterior cervical minimally invasive fixation.
Methods Small lateral skin incisions are made on the neck using intraoperative computed tomography–guided navigation. Navigated cervical pedicle screws were placed using the proficient minimally invasive system (Spine Wave, Shelton, CT).
Results Minimally invasive cervical fixation options have been limited traditionally. Navigated, percutaneous cervical minimally invasive surgery (MIS) fixation provides an effective, safe option for cervical fixation. This technique is described and illustrated in a case example of a patient who suffered a burst fracture and underwent treatment.
Conclusions Navigated, percutaneous posterior cervical MIS fixation provides biomechanically superior fixation while avoiding the morbidity of traditional, open approaches to the posterior cervical spine. Percutaneous cervical pedicle screw techniques will be pivotal in the continued advancement of posterior cervical decompression and fusion techniques.
Clinical Relevance Navigated, percutaneous cervical minimally invasive fixation is an achievable form of cervical fixation with acceptable complication rates and radiographic outcomes.
Level of Evidence 4.
Introduction
Lateral mass screw fixation has been the gold standard for posterior cervical fixation. Cervical pedicle screw fixation has also been described. The open technique for cervical pedicle screw fixation requires a pronounced lateral-to-medial trajectory exacerbating the musculoskeletal morbidity associated with the posterior approach. Furthermore, the close proximity of the neural elements and vertebral artery requires fluoroscopic guidance. Several small series describing minimally invasive cervical fixation techniques have been described, but these typically utilize lateral mass fixation and require specialized retractors as well as fluoroscopy. Navigated, percutaneous posterior cervical minimally invasive surgery (MIS) fixation is a feasible technique that combines the biomechanical superiority of pedicle screw fixation with the muscle sparing benefits of a minimally invasive approach.
Methods
Patient Selection
Indications for percutaneous cervical MIS fixation are currently relatively narrow. This technique has great utility in patients not requiring posterior decompression, such as patients requiring posterior fixation following extensive anterior surgery or select trauma cases. Broadly, this technique is indicated for patients who require rigid fixation of the cervical spine and who either do not require decompression or have undergone an anterior approach that has adequately accomplished decompression.
The following represents appropriate indications for this MIS, navigated technique:
Supplemental fixation
Multilevel (≥3 levels) anterior cervical discectomy and fusion.
Multilevel (≥2 levels) anterior corpectomy patients.
A single-level corpectomy on patients with significant risk factors for pseudarthrosis or instability.
Three column, traumatic cervical spine injuries that require a reduction or decompression anteriorly.
Primary fixation
Unstable traumatic cervical spine injuries without significant stenosis or spinal cord compression.
Complete spinal cord injury patients reduced with cervical traction.
Type II odontoid fractures.
Preoperative Considerations
Preoperatively, patients should undergo computed tomography (CT) of the cervical spine to evaluate the cervical pedicle anatomy. In addition, magnetic resonance images of the cervical spine should be obtained to evaluate for neural compression so that if necessary, the appropriate anterior decompression can be performed. In the instance of trauma involving the foramen transversarium, CT angiogram of the neck should be obtained to evaluate for possible vertebral artery injury. The vertebral artery courses should be evaluated preoperatively to insure no aberrant course.
Patients are placed in a Mayfield frame and positioned prone on a radiolucent Jackson table. The Mayfield frame is rigidly fixed to the Mayfield attachment. As with all navigated procedures, it is essential that the patient is rigidly fixated throughout the procedure to maintain navigation accuracy.
The patient is then prepped and draped in standard sterile fashion. It is important that the neck is prepped and draped as far lateral on the neck as possible due to the unusually lateral entry point. In addition, taping down the shoulders can help open the access to the lateral neck.
A 2-cm midline incision is made over the C7 or T1 spinous process. A small fascial incision is made bilaterally, just large enough to accommodate the spinous process clamp. Care is taken to preserve the interspinous ligaments. The reference frame is attached and secured. The O-arm is brought in for an intraoperative cone beam CT image.
A navigated wand is used to map the skin entry points along the axis of the cervical pedicles. Local anesthetic is infiltrated. Small 1.5-cm stab incisions are made over the entry points. The SureTrak (Medtronic, Minneapolis, MN) mount and array are placed on an electrocautery knife with extended electrode and registered creating a navigated electrocautery knife. The device can then be used to cut through the fascial layers of the neck directly along the trajectory of the pedicle. Once bone is palpated, the fascia along the lateral mass can be released with electrocautery.
The primarily navigated MH80 drill (Medtronic, Minneapolis, MN) is then used to make a pilot hole and advanced into the origin of the pedicle. We have noted that the pedicle origin can be sclerotic and advancing the drill initially through this sclerotic bone allows for better penetration of the tap. A 3.5-mm navigated, power tap is then used to advance through the pilot hole along the length of the pedicle into the vertebral body. In circumstances of pedicles less than 4 mm in diameter, the same lateral-to-medial trajectory is taken, but a shorter screw is inserted and stopped prior to traversing the pedicle. Appropriate size width and length screw are chosen based on the navigation display (commonly 3.8 or 4.2 mm width × 22–28 mm length). Navigated wand is then used to palpate the tract and insure no breach.
A navigation integrated driver is then used to place the screw, which is affixed to a reduction tower. Once placed, the driver is removed and the reduction tower remains in place. Once all the screws have been placed, confirmatory imaging is obtained with either repeat intraoperative O-arm spin or anteroposterior (AP) and lateral scout imaging with O-arm. Percutaneous rods are then placed and finally tightened. Rod length can be confirmed with direct visualization or with additional fluoroscopic imaging.
Incisions are then closed with inverted 2–0 vicryl and 3–0 vicryl in the subcutaneous tissue. Adhesive skin glue is placed on the skin.
Results
Case Example
A 64-year-old man presented following a motor vehicle collision with quadriplegia. Physical examination was consistent with a C5 ASIA B incomplete spinal cord injury. CT of the cervical spine demonstrateed diffuse idiopathic skeletal hyperostosis with a C6-C7 fracture dislocation (Figure 1). The fracture was significantly displaced and translated with kyphotic angulation. A magnetic resonance image of the cervical spine showed a large ventral disc fragment and cord contusion (Figure 2).

Sagittal computed tomographic image of the cervical spine demonstrating C6-C7 fracture dislocation.

Sagittal T2 magnetic resonance image of the cervical spine demonstrating C6-C7 fracture dislocation.
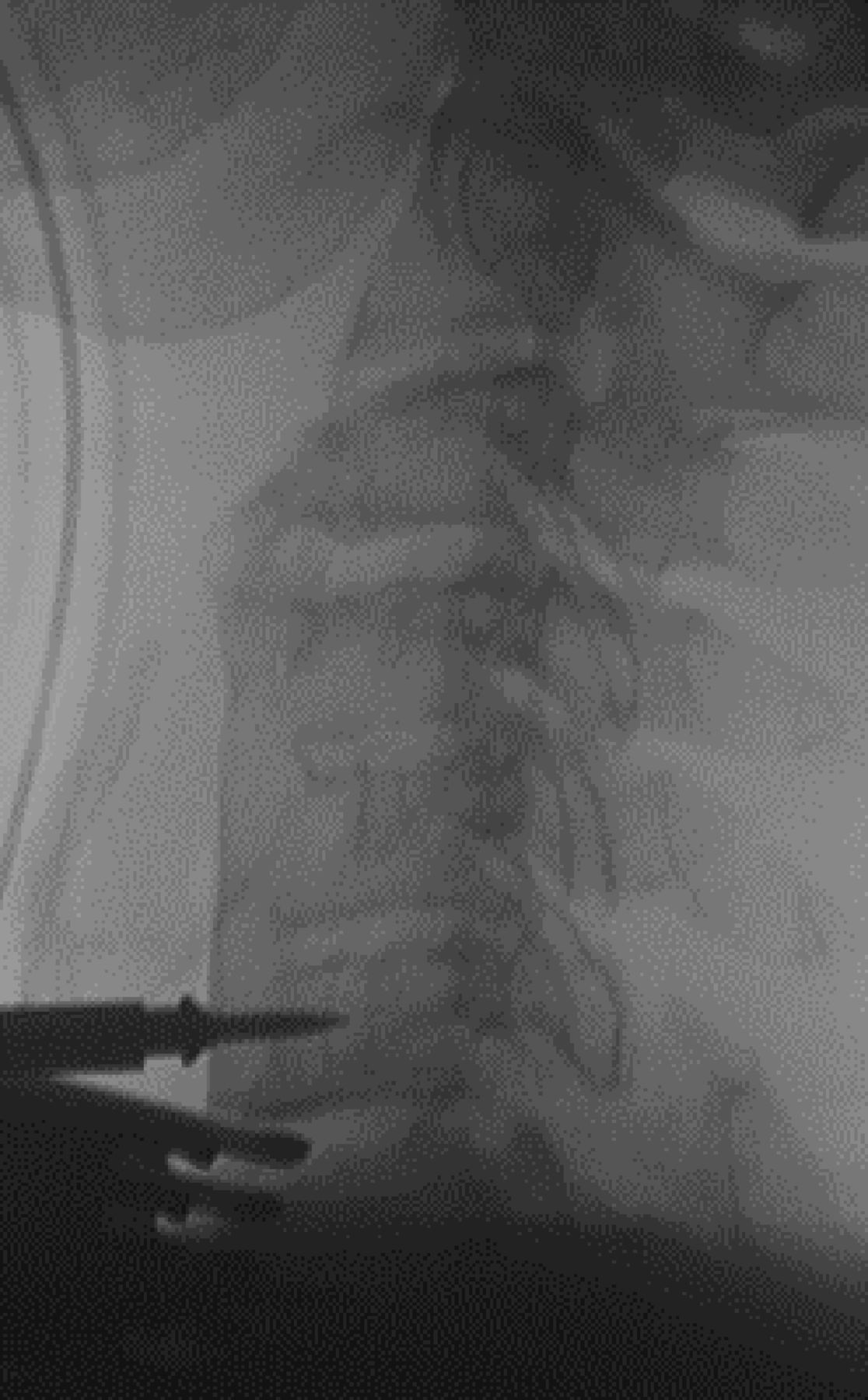
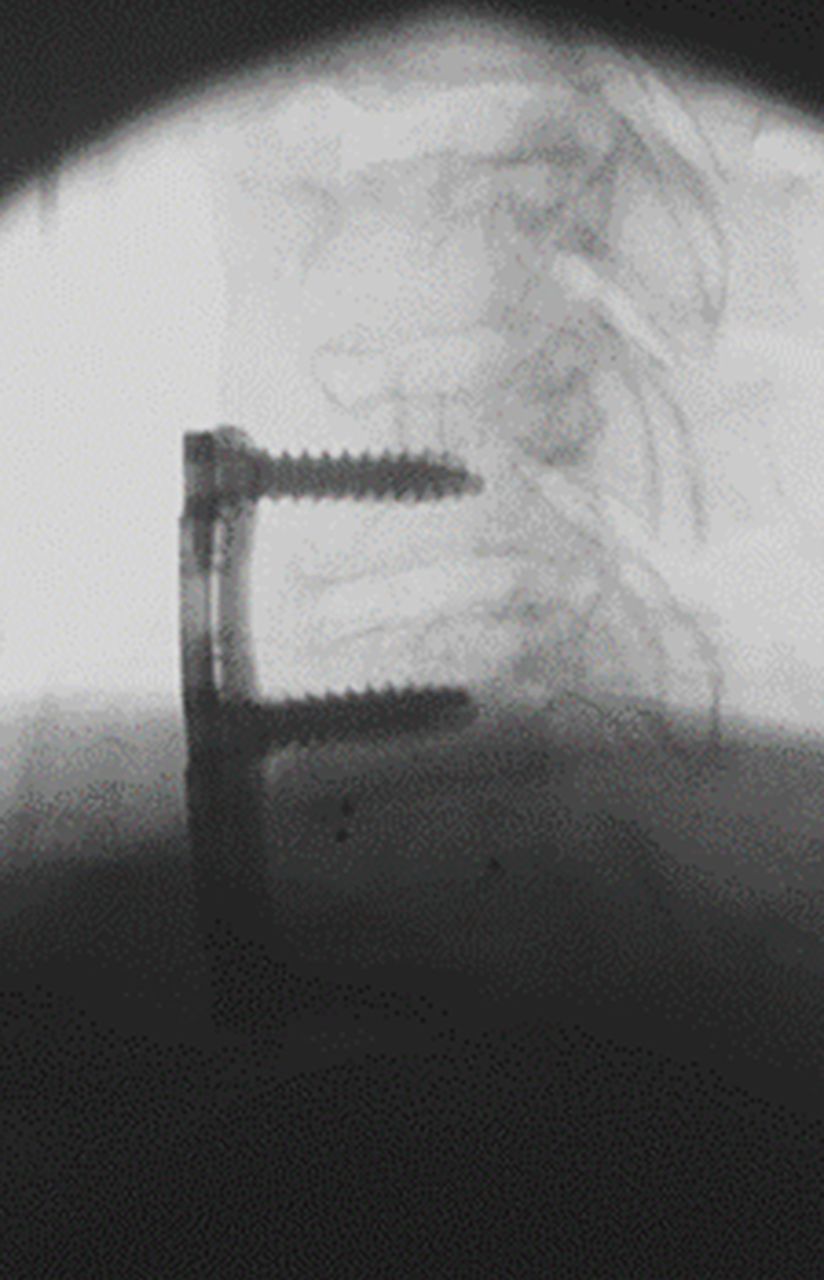
The patient was taken to the operating room emergently for an open reduction and C6-C7 anterior cervical discectomy, decompression, and fusion. Anterior plating was performed from C5 to C7 for additional fixation (Figures 3 and 4).

Intraoperative lateral cervical spine x-ray image demonstrating fracture reduction.

Intraoperative lateral cervical spine x-ray image demonstrating reduction of fracture with anterior plating.
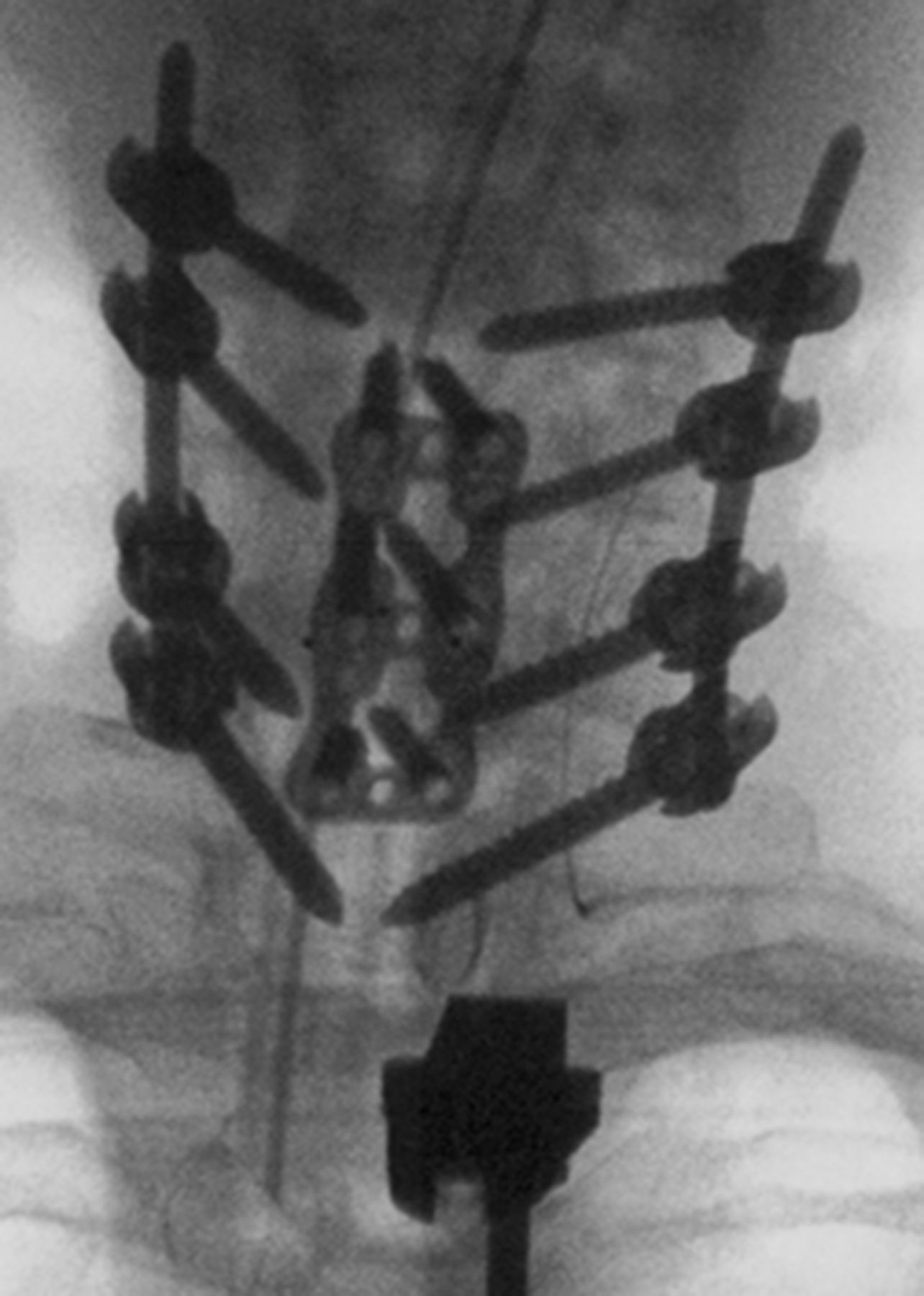
The patient then underwent navigated, percutaneous posterior cervical MIS fixation from C5 to T1. Figure 5 shows intraoperative AP radiograph following posterior fixation. Figures 6 and 7 show postoperative AP and lateral radiographs. Operative time for the posterior portion of the procedure from skin incision to closure was 98 minutes. Implant sizes are shown in the Table.

Intraoperative anteroposterior cervical spine x-ray image demonstrating C5-T1 percutaneous fixation.

Postoperative anteroposterior cervical spine x-ray image.

Postoperative lateral cervical spine x-ray image.
Implant descriptions.
The patient did not require a collar postoperatively. He was discharged to rehabilitation on postoperative day 10. He improved clinically to C5 ASIA C with some return of lower extremity motor strength. Figure 8 demonstrates well-healed skin incisions at 3 months after the operation.

Posterior skin incisions at 3-month follow-up.
Discussion
Pedicle screw instrumentation is the standard of care for the thoracolumbar spine. Despite this, lateral mass screws remain the most common posterior cervical fixation technique. The cervical pedicles have a smaller diameter, have neurovascular structures in close proximity, and have a steep lateral-to-medial angulation. Therefore, the technique is more challenging. In addition, the traditional open technique for cervical pedicle screws typically requires a relatively morbid musculoligamentous dissection.
Subaxial C3-C6 pedicle screw placement has not been widely adopted, partly due to the close proximity of surrounding neurovascular structures. Cadaveric studies demonstrate the vertebral artery to be on average 1.1–1.7 mm lateral to the cervical pedicle1 and the nerve root 1.4–1.7 mm caudal to the pedicle on average.2 Despite these concerns, the literature does not indicate an increased risk of neurovascular injury for open cervical pedicle screw placement compared with lateral mass screws.3–6
Cervical pedicle screws are biomechanically superior to lateral mass screw fixation. Lateral mass fixation is typically performed with screws measuring 3.5 mm in diameter and a length of 12 or 14 mm. Cervical pedicles can typically accommodate screw diameters of 3.8 to 4.5 mm and lengths from 22 to 30 mm. The longer screw size and pedicle purchase as well as triangulated lateral-to-medial trajectory translate into significant biomechanical advantage. Cadaveric studies have shown that the pullout strength of a cervical pedicle screw is 4 times stronger than a lateral mass screw.7 This does not account for the additional biomechanical advantages of preserving the posterior musculoligamentous complex.
Cervical pedicle screw fixation was first described by Abumi et al in 1997.8–11 This technique has been described in various open posterior cervical constructs. However, traditionally, this technique has been limited to C2 and C7 due to the larger size of these pedicles.12 Subaxial C3-C6 cervical pedicle screw placement has typically been used in combination with a traditional open exposure. There are only a few small published series of true percutaneous cervical pedicle screw techniques, and these generally employ fluoroscopy .1–3,13
Our initial experience with navigated true percutaneous fixation in 27 patients demonstrated that it can be performed safely.4 Two screws were revised intraoperatively in this series. One screw was placed caudally in the C2 pars with poor screw purchase. The second screw was encroaching on the C5 transverse foramen. Both screws were revised intraoperatively without any postoperative neurovascular sequelae. Only one patient in this series required reoperation. This was due to symptomatic breach of a C5 screw that was impinging on the C4-C5 foramen. This was removed, and the patient’s symptoms were resolved. There was no vertebral artery or spinal cord or nerve root injury reported in this series.
There are significant advantages to this navigated, percutaneous technique. The use of navigation in robotics in spine surgery is increasing the accuracy of instrumentation placement.5 Percutaneous techniques preserve the posterior musculoligamentous posterior tension band giving additional stability and reducing postoperative wound morbidity and neck pain. The benefits of percutaneous muscle sparing techniques have been well described in the lumbar spine, and similar advantages are gained with minimally invasive cervical spine surgery.6
Robust posterior cervical fixation reduces the need for bracing postoperatively. Rigid cervical bracing can have significant morbidity, particularly in the spinal cord injury population.7,14–16 In the relatively immobile trauma population, there are significant wound healing advantages to this approach. The small, lateral incisions help reduce the direct pressure on the wound edges. The percutaneous muscle splitting approach reduces the wound dead space. In addition, the avoidance of placing the incision over the midline reduces additional wound pressure caused by the spinous processes.
The current application of this posterior cervical MIS technique is limited to a relatively narrow patient population. Robotic and navigation advances will expand the role for this robust fixation method. In addition, minimally invasive methods for decompression and fusion will continue to broaden the indications for minimally invasive posterior fixation.17–20
Conclusion
Navigated, percutaneous posterior cervical MIS fixation is a novel technique that provides significant biomechanical and clinical advantages. In the case example illustrated here, a C6-C7 fracture dislocation in a patient with diffuse idiopathic skeletal hyperostosis is effectively treated with rigid fixation posteriorly using this technique after reduction of the fracture anteriorly.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosures The authors have no personal or institutional financial interest in the drugs, materials, or devices described in this article, except as follows: Domagoj Coric, MD: Spine Wave—consultant, royalties, direct stock ownership; and Medtronic—consultant, royalties.
IRB Approval This study was approved by Atrium Health Institutional Review Board Approval Number: 03-21-22E
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.