


Abstract
Background The gold standard of surgical treatment of adolescent idiopathic scoliosis (AIS) consists of a posterior approach requiring complex 3-dimensional correction with multisegmental pedicle screws and 2 contoured rods. The substantial corrective forces and the ability of the rod to withstand these forces rely on its biomechanical properties. The aim of this study is to compare outcomes of 5.5-mm cobalt-chrome (CoCr) and 6-mm titanium alloy (TiAl) rods in surgical correction in Lenke 1 AIS patients. TiAl has greater elasticity, which may facilitate the correction maneuver, whereas the stiffness of CoCr may result in stronger correction forces. The literature provides no clear indications about which rod may allow better correction and safety.
Methods A total of 64 consecutive patients (30 CoCr vs 34 TiAl) with Lenke 1 AIS <100°, with 2 years minimum follow-up, requiring correction and posterior fusion at our institution were included. The primary outcome measure was coronal and sagittal correction and loss of correction at 2-year follow-up. Secondary outcome measures compared peri- and postoperative complications.
Results The mean coronal correction was higher in the CoCr group: −73.6% ± 7.4 vs −65.5% ± 11 (P = 0.001). Mean T5-T12 kyphosis did not change significantly after surgery. In patients with hypokyphosis (<10°), an improvement in thoracic kyphosis was observed in both groups, but the improvement was significantly higher in the TiAl group (P = 0.038). In patients with hyperkyphosis (>40°), a similar reduction in thoracic kyphosis was observed in both groups. At follow-up, no coronal correction loss occurred. The sagittal correction loss was slight (0.5° ± 1.5 for the CoCr group, 1.5° ± 3 for the TiAl group) but statistically higher in the TiAl group (P = 0.032). There were no mechanical complications. One revision was required for infection in the CoCr group.
Conclusion In this series of Lenke 1 AIS, with the limitations of the study, 5.5-mm CoCr rods have provided better correction in the coronal plane than 6-mm TiAl rods. However, TiAl rods have been found to be associated with higher increase of thoracic kyphosis in hypokyphotic curves, although the clinical relevance of this finding could be questionable.
Clinical Relevance This article provides surgeons with more information regarding rod material options when correcting Lenke 1 AIS.
Level of Evidence 3.
Introduction
The gold standard of surgical treatment of adolescent idiopathic scoliosis (AIS) consists of a posterior approach requiring complex 3-dimensional correction with multisegmental pedicle screws attached to 2 contoured rods. The substantial corrective forces and the ability of the rod to withstand these forces rely on its biomechanical properties. These properties depend on the material, diameter, and shape of the rod. Among the others, 5.5-mm cobalt-chrome (CoCr) and 6-mm titanium alloy (TiAl) rods may be used for AIS surgery. Their mechanical properties differ: TiAl is less stiff and has a greater yield strength, which means that it acts as a more elastic material. This may facilitate the correction maneuver, reducing pull-out risk during approximation of the rod to the screws and reducing the risk of plastic deformation of the rod. On the contrary, CoCr has a much higher Young’s modulus and a lower yield strength, which mean that it is a stiffer and plastic material1; this may result in stronger corrective forces that may be crucial in spinal deformity surgery. Additionally, CoCr rods have a better fatigue performance than TiAl rods.2,3 Regarding rod diameter, an increase in radius alters stiffness to the fourth power of the change in radius. Some studies reported a higher correction rate in both frontal4,5 and sagittal6 plane using CrCo rather than TiAl, with the same diameter. However, there are no studies that demonstrate that an increase in diameter of TiAl rods may allow one to achieve a comparable correction rate to those achieved using thinner CoCr rods while maintaining the advantages of TiAl.
With this background, the aim of our study is to compare the radiological outcomes of 5.5-mm CoCr and 6-mm TiAl rod systems in AIS patients with Lenke 1 curves, with attention paid also to peri- and postoperative complications.
Methods
A total of 64 consecutive patients with Lenke 1 AIS who required correction and posterior fusion with 2 years minimum follow-up at our institution between January 2016 and December 2017 were included in this retrospective comparative study.
All patients underwent surgery performed by the same team of experienced surgeons. During all surgeries, somatosensory- and motor-evoked potentials were monitored. Patients were divided into 2 groups that were homogeneous in age, Lenke curve type and lumbar and sagittal modifiers, scoliosis severity, thoracic kyphosis (TK), implant density, corrective strategy, and use and number of the Ponte osteotomies. No pedicles subtraction osteotomies were performed. Patients with nonidiopathic scoliosis or with Cobb’s angle >100° were excluded. We decided to exclude these patients because the extent of curve correction may depend on too many factors (eg, number and type of osteotomies, age, intraoperative anesthesiologic and neurological conditions, etc) as well as the material of the rod, making it difficult to have 2 homogeneous groups to compare. Only type 1 curves according to Lenke were included. The same corrective strategy was used for all patients, consisting of high-density pedicle screw constructs (>80%), periapical Ponte osteotomies (when necessary to improve flexibility), translation maneuver over differently shaped rods (hypercontoured in concavity and hypocontoured in convexity), and final direct vertebral rotation.7 Upper instrumented vertebra and lower instrumented vertebra were decided based upon each patient’s curve characteristics, considering T1 tilt, clavicle angle, lumbar modifier, and stable vertebra. The desired amount of correction was chosen also considering the lumbar modifier for each curve, to avoid any coronal imbalance. However, this does not result relevant for our results, since the distribution of the sagittal modifiers was not different between the 2 groups (P < 0.05).
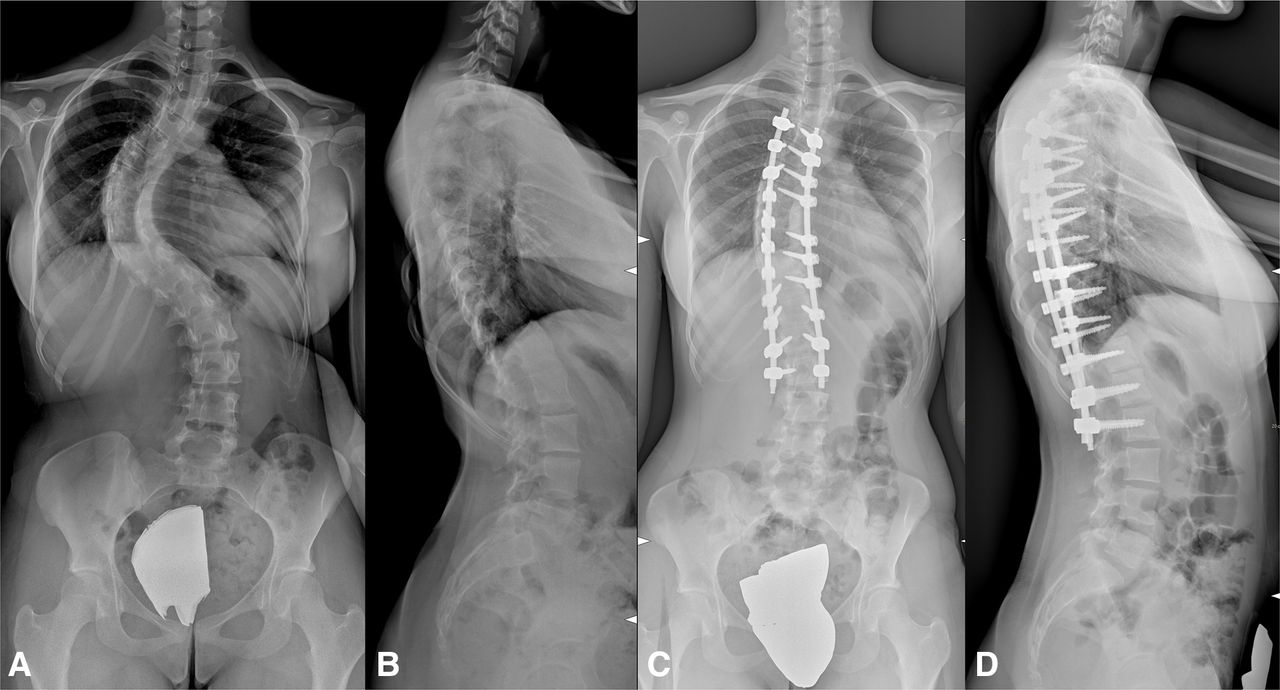
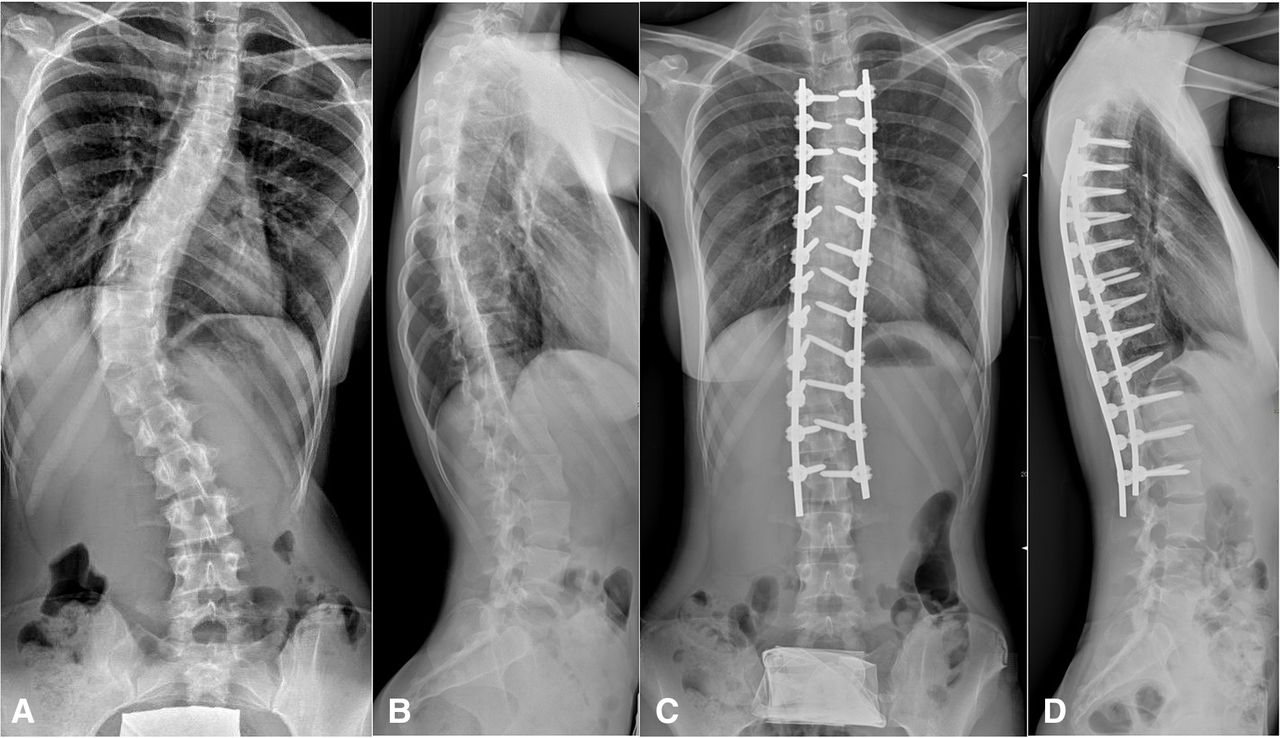
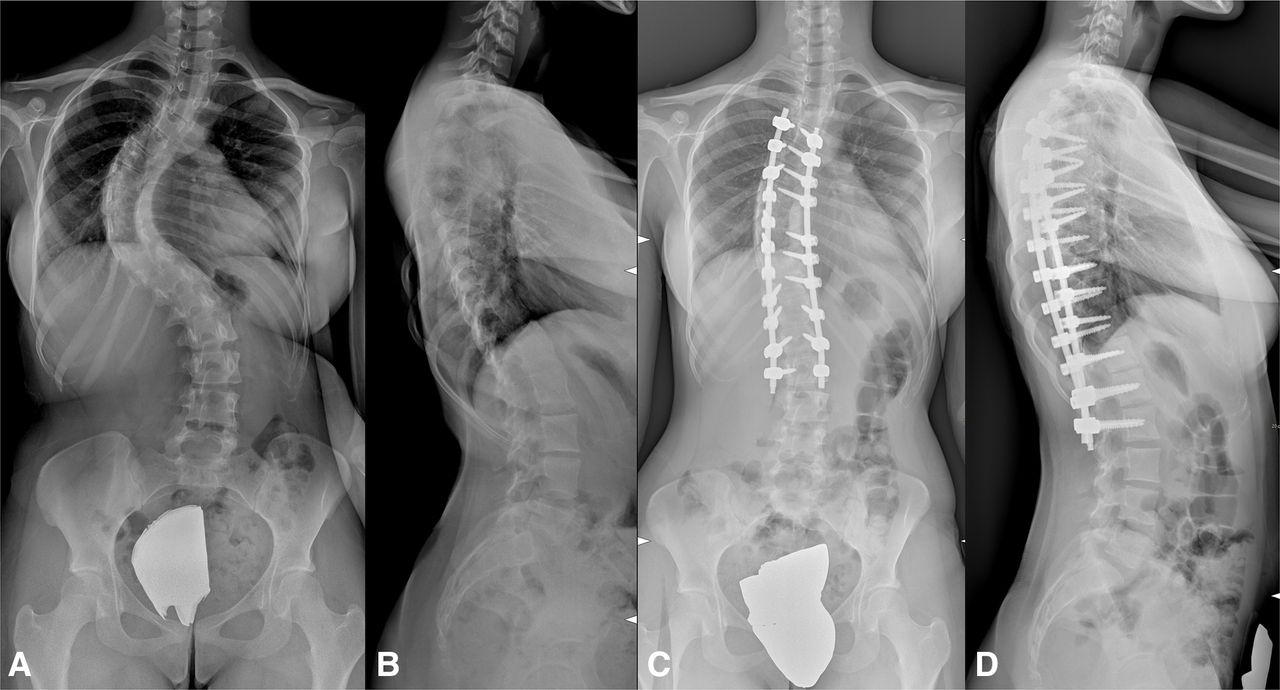
For the first group, 5.5-mm CoCr rods were used to fix correction (CoCr group, n = 30) (Figure 1), and for the second group, 6-mm TiAl rods were used (TiAl group, n = 34) (Figure 2). Treatment (type of rods) was chosen by the lead surgeon of each surgery, according to his preference. However, all the lead surgeons belonged to the same team and adopted the same corrective technique.

A 17-year-old female patient with a Lenke 1AN scoliosis with a main Cobb angle of 70° treated with cobalt-chrome rods: coronal (A, B) and lateral (B, D) view of pre- (A, B) and postoperative (C, D) x-ray images. After correction and posterior fusion from T4 to L3, an optimal 3-dimensional spine profile is achieved.
A 15-year-old patient with a Lenke 1BN scoliosis with a main thoracic curve of 71° treated with titanium alloy rods: coronal (A, C) and lateral (B, D) view of pre- (A, B) and postoperative (C, D) x-ray images. After correction and posterior fusion from T4 to L2, correct coronal and sagittal balance are restored.
For each patient, using pre- and postoperative full-length standing and lateral side-bending radiographs, we measured the coronal Cobb’s angle of each curve, the coronal flexibility, and the TK Cobb’s angle. In addition, for each patient we identified the length of the instrumentation area and the apical, stable, and neutral vertebrae of the curves. One experienced spine surgeon was blinded to group belonging of each patient and evaluated all radiograph in both groups. Hence, all measurements were done with the help of software (Carestream Health Italy, Inc., Genova, Italy) at a magnification of 300%.
The primary outcome measure was the entity of correction of both coronal and sagittal planes and the loss of correction at 2-year follow-up in both groups. Secondary outcome measures included a comparison of peri- and postoperative complications.
Parametric test was used to compare samples in case of normal distribution, equal variance, and appropriate numerousness. The Shapiro-Wilk test was used to verify normal distribution. The Levene’s test was used to analyze homogeneity of the variances. As parametric test, we used the Student’s t test for groups with equal variance, the Welch’s t test otherwise. The unpaired t test was used to compare different groups, and the paired t test was used to assess the consequences of a treatment on the same group. As nonparametric test, we used Mann-Whitney U test for unpaired groups and the Wilcoxon test for paired groups. Continuity correction for nonparametric tests was applied in case of discrete distribution. Odds ratios were used to quantify the strength of the association between the variables analyzed and the complications rate, using the χ2 test with Yates’ correction to establish significance. A P value <0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS version 26.0 (SPSS Inc., Chicago, Illinois).
Results
The mean preoperative Cobb’s angle of the 2 groups was 60.3° ± 15.5 and 65.6° ± 10.7 for the CoCr group and the TiAl group, respectively (P = 0.116) (Table 1).
Clinical and radiographic findings of the patients.
The mean coronal correction was significantly higher in the CoCr group vs the TiAl group: postoperative Cobb angles were 16.1° ± 6.1 vs 22.8° ± 8.3 (P = 0.0005), respectively, with a reduction of −73.6% ± 7.4 vs −65.5% ± 11 (P = 0.001) (Table 1).
In both groups, the general mean T5-T12 kyphosis did not change significantly after surgery (the overall kyphosis was 20.5° ± 13.4 preoperatively and 20.3° ± 6.4 postoperatively, P = 0.914) (Table 1). Following treatment, in both groups, the mean kyphosis significantly decreased until it normalized in the subgroup of hyperkyphotic patients before surgery (P = 0.009 and P = 0.035 for the CoCr group and the TiAl group, respectively) and significantly increased until it normalized in the subgroup of hypokyphotic patients before surgery (P = 0.034 and P < 0.0001 for the CoCr group and the TiAl group, respectively) (Tables 1–2). Analyzing only patients with a lordotic thoracic spine (TK less than 10°), a significant improvement in TK was observed in both groups with a higher sagittal correction observed in the TiAl group (P = 0.038) (Tables 1–2). In patients with a hyperkyphotic thoracic spine (TK less over 40°), a significant reduction in TK was observed in both groups without any differences between the CoCr and the TiAl groups (P = 0.999) (Tables 1–2).
T5-T12 kyphosis corrections according to subgroup (+, N, −) and type of rods used.
Mean follow-up was 2.2 years ± 0.2 (range 2–2.4) for the CoCr group and 2.1 years ± 0.3 (range 2–2.9) for the TiAl group (Table 1). At last follow-up, no coronal correction loss was detected in either groups (P = 0.745 and P = 0.663 for the CoCr group and the TiAl group, respectively) (Table 1). The sagittal correction loss was slight (0.5° ± 1.5 and 1.5° ± 3 for the CoCr group and the TiAl group, respectively) but statistically higher in the titanium bar group (P = 0.032) (Table 1).
There were no mechanical complications. No symptomatic proximal junctional kyphosis (PJK) was found. Postoperative radiographic PJK has not been evaluated for instrumental limitations, caused by poor visualization of proximal thoracic vertebrae in lateral x-ray images projection without the use of EOS technology. No neurological and vascular complications related to screw placement were recorded. Two screws (0.2%, 1 for each group) were removed intraoperatively for somatosensory-evoked potentials and motor-evoked potentials signal alteration. Only 1 complication requiring revision was recorded: an infection in the CoCr group.
Discussion
To the best of our knowledge, there are no studies that compared the correction rate between the 6-mm TiAl and 5.5-mm CoCr rod with homogeneity of groups. Our 2 groups were extremely homogeneous in age, curve pattern, curve magnitude, and TK. Moreover, all the surgeries were performed by the same surgical team, using the same technique, consisting in high-density pedicle screw systems (>80%),8 periapical Ponte osteotomies, translation over asymmetrically molded rods, and direct vertebral rotation. This combination of techniques has proved to be extremely powerful,7,9 allowing optimal 3-dimensional correction of the deformity in both groups. However, CoCr rods provided a significantly greater correction in the coronal plane, with a 73.6% amount of correction compared with 65.5% correction of the TiAl group. This is in line with the hypothesis that a stiffer material provides stronger corrective forces. In fact, Serhan et al,4 in an in vitro biomechanical study, found that CrCo rods provided intraoperative reduction forces that were 42% higher than TiAl rods. Our result is in contrast with the studies by Angelliaume et al,6 Sabah et al,10 and Yang et al.11 These studies showed no significant difference in coronal correction between CoCr and TiAl rods, even though they compared rods of the same diameter, thus keeping a high difference in rod stiffness between their groups. Surprisingly, while our choice to compare 6-mm TiAl and 5.5-mm CoCr was aimed to reduce the difference in rod stiffness and in the consequent theoretical corrective potential, this did not result in comparable coronal correction rates between the 2 groups. We interpret these differences as a result of the deep complexity of this deformity. In fact, many variables must be considered when approaching surgical treatment of scoliosis (selection of patients, corrective maneuver, rod materials, high/low density of screws, etc), and identifying and analyzing all these factors separately may be challenging. In particular, the cited studies6,10,11 had substantial differences in study design, patients stratification, and surgical technique when compared with our study. With the limitations of the retrospective nature of the study, we tried to keep any confounding factors as minimal as possible, comparing 2 groups that were homogeneous except for the rod type.
Regarding the sagittal plane, both groups showed no significant differences in overall TK and lumbar lordosis after the surgical procedure. Interestingly, both TiAl and CoCr rods allowed restoriation of a normal TK in hypokyphotic patients with a negative Lenke sagittal modifier, as well as in hyperkyphotic patients with a positive sagittal modifier. Therefore, this seems to indicate that the restoration of a correct sagittal alignment is mainly the result of the corrective technique adopted, rather than the material used. Previous biomechanical12 and clinical13 studies reported that direct vertebral rotation (DVR) may lead to TK. Our study, in contrast to this view, confirms that DVR does not necessarily lead to a TK flattening. On the contrary, if properly associated with strategies like asymmetric rod contouring and Ponte osteotomies, it allows to restore an optimal thoracic sagittal profile, significantly increasing TK when reduced, significantly reducing it when increased. Other studies7,14–17 supported this view, particularly Demura et al,16 who recorded an increase in T5-T12 TK from 13 to 20° in patients with TK under 20° and a slight decrease from 30 to 24° in patients with TK over 20°. Interestingly, in our patients with hypokyphosis, a significantly higher sagittal correction was seen in the TiAl group. This is in contrast with Liu et al,18 who described a better TK restoration using a stiffer rod. While it is questionable whether such a small difference, although statistically significant, would be clinically relevant, it is also unclear how TiAl allows a better correction of hypokyphosis. Considering the technique adopted, based upon asymmetric rod contouring, translation, and DVR, our hypothesis is as follows: in order to achieve the corrective forces appropriate for the specific curve when TiAl is used, the concave rod could tend to be overshaped to compensate its lower stiffness that, otherwise, would tend to straighten the rod during the translation maneuver. So, when the translation maneuver over the concave rod is completed, the rod partly loses some of its shape. Then, when the translation maneuver on convex side begins, the forces acting on the concave TiAl rod are reduced, and there is an elastic return of the concave rod to its original hyperkyphotic shape. Instead, when CoCr is used, due to its plastic nature, the concave rod during the translation maneuver tends to retain its original shape without any elastic return. A second hypothesis is that the surgeon may be prone to undershape the CoCr rods to avoid any pull-out risk, given the fact that they exert higher forces due to their stiffness.
After a minimum of 2 years of follow-up, no significant correction loss was detected in both groups. However, when comparing loss of correction in the sagittal plane between CoCr and TiAl, TiAl showed a significantly higher loss. Although this radiographic finding may not be clinically relevant, it may be a consequence of the elastic nature of the TiAl rod. In fact, during the first few months, before any bone fusion is achieved, the TiAl rod is forced by the spinal deformity to an elastic pullback, which leads to an increase in TK, as Sabah et al10 stated.
Several studies18–21 reported that the use of CoCr may be a risk factor for PJK. Despite the different properties of the 2 materials, there were no statistically significant differences in symptomatic PJK and mechanical complications. The only complication requiring revision was an infection occurred in the CoCr group, and this poses the question regarding whether the use of CoCr may be an infection risk factor. Literature toward this topic is controversial. While some studies22–24 emphasized a protective role of TiAl rods compared with stainless steel, others25,26 showed no difference in infection rate between the various materials.
Our study is not without limitations. First, it is a retrospective study with a relatively small sample size. Second, patients were not randomized to a group, although the adopted corrective technique was the same. Moreover, some factors that affect the results of these procedures, such as bone-screw and screw-rod interfaces, were not considered. Finally, the mean follow-up period was relatively short. All these limitations increase the risk of bias and do not allow for strong evidence-supported elements to guide the choice between the 2 materials. The rod selection still appears to be based upon surgeon preferences. However, both rods gave satisfactory results. Further research on this topic is needed, preferably a large prospective randomized controlled trial.
Conclusions
In this series of Lenke 1 AIS, with the limitations of the study, 5.5-mm CoCr rods have provided better correction in the coronal plane than 6-mm TiAl rods. However, TiAl rods have been found to be associated with a higher increase of TK in hypokyphotic curves, although the clinical relevance of this finding could be questionable.
Footnotes
Funding No funding was received for this study.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The study was approved by the institutional review board of our hospital.
Data availability statement Data are available on PACS (picture archiving and communication system) of our Institute.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.