


Abstract
Background Thoracic spinal tuberculosis (TB) causes destruction of the spine and compression of the adjacent spinal cord. This study aimed to identify the risk factors for neurological deterioration in patients with thoracic spinal TB to guide decision-making regarding immediate surgery before the onset of weakness.
Methods Demographic, clinical, laboratory, and radiologic (x-ray and magnetic resonance imaging) data of 115 patients with active thoracic spinal TB were retrospectively analyzed. Patients with neurological status categorized as Frankel grades A, B, or C (n = 71) were classified as the neurological deficit group, while those with neurological status categorized as Frankel grades D and E (n = 44) constituted the control group. Univariate and multivariate logistic regression analyses were used to predict the risk factors for neurological deficits.
Results The mean patient age was 57.2 years. The most common lesion location was the distal thoracic region (T9-L1; 62.6%). Paradiscal involvement was the most common form of involvement (73%). In the univariate analysis, the significant risk factors associated with neurological worsening were overweight (body mass index [BMI] >25), C-reactive protein level > 20 mg/L, panvertebral involvement, loss of cerebrospinal fluid posterior to the cord, cord signal changes, and canal compromise. The multivariate analysis revealed that only BMI >25 (adjusted OR = 16.18; 95% CI 1.60–163.64; P = 0.018), cord signal changes (adjusted OR = 7.42; 95% CI 1.85–29.74; P = 0.005), and canal encroachment >50% ( adjusted OR = 51.86; 95% CI 5.53–486.24; P = 0.001) were independent risk factors for predicting the risk of neurological deficits.
Conclusions Overweight (BMI >25), cord signal changes, and canal compromise >50% significantly predicted neurological deficits in patients with thoracic spinal TB. Prompt spinal surgery should be considered before progressive worsening of the neurological condition in patients with all of these risk factors.
Clinical Relevance Predictive factors for neurological deficits in thoracic spinal TB were determined. Overweight, cord signal changes, and canal compromise >50% showed predictive value. These factors can help identify patients who require early surgical intervention.
Level of Evidence 3.
Introduction
Tuberculosis (TB) is among the oldest infectious diseases known to man.1 Globally, an estimated 2 billion people are infected with TB. However, only 5%–15% of patients become symptomatic, and the remaining patients have latent infections.2 The exact incidence of spinal TB is unknown; however, extrapulmonary TB has been reported to occur in 20% of infected individuals.3
Skeletal TB is known to occur in nearly 10% of patients with active pulmonary disease, and the spine is the most common skeletal site of involvement (approximately 50% of patients with skeletal TB).4 Spinal TB is a severe form of musculoskeletal TB that causes pain, vertebral destruction, and neurological deficits. This manifestation is more common in cervical and thoracic disease as a result of the proximity to the spinal cord and is rarer in the lumbar spine. Eventually, the neurological symptoms can progress to myelopathy and paraplegia, or even tetraplegia if the lesions are sufficiently cephalad.5
The management of spinal TB differs for those with and without neurological complications. While anti-TB medication is the mainstay of treatment in both groups, additional surgical treatment provides better results in patients with neurological complications.6 Thus, optimal patient outcomes can be achieved if patients at risk for neurological deterioration are identified and treated promptly. However, the literature has limited information regarding the risk factors predicting neurological deterioration in adult thoracic spinal TB patients.7–10 Therefore, this study aimed to determine the predictive factors for neurological deficits in patients with thoracic spinal TB.
Methods
Study Design and Population
The medical records of 115 consecutive patients with thoracic TB treated at our institute between 2016 and 2021 were retrospectively reviewed. The study protocol was prepared in accordance with the Declaration of Helsinki and ICH Good Clinical Practice Guidelines (Number 086/2019) and reviewed and approved by the institute’s Ethics Committee for Human Research. TB was diagnosed using pathological samples, tissue cultures, and polymerase chain reaction tests. Patients with active TB of the thoracic spine were included in this study. Patients showing late-onset neurological deficits in cases of healed TB were excluded. The collected data included information regarding patient characteristics, clinical features, neurological status categorized by Frankel grade, laboratory results, and radiographic and magnetic resonance imaging (MRI) findings.
Outcome Measurements
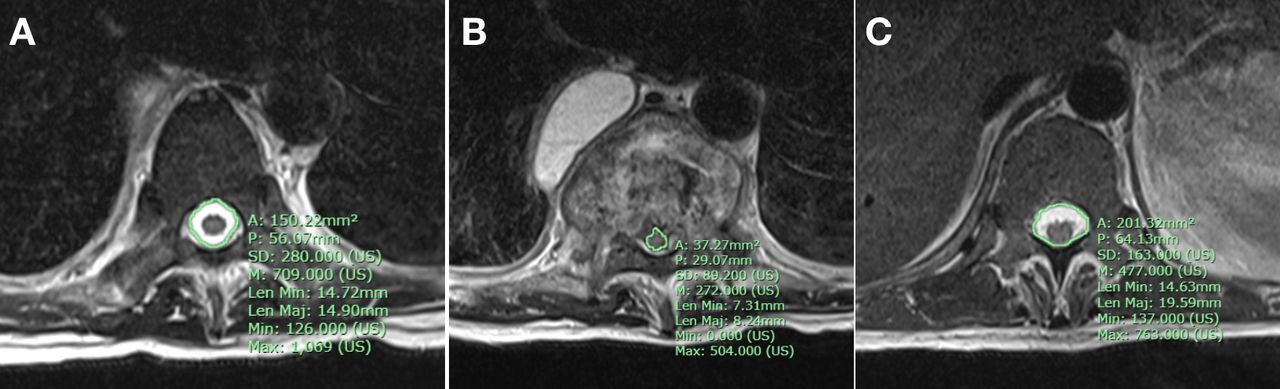
Data for possible risk factors were also collected, including (a) clinical characteristics (ie, age, sex, BMI, body temperature, duration of symptoms, and neurological deficit); (b) laboratory investigations (ie, erythrocyte sedimentation rate [ESR] and C-reactive protein [CRP] level); and (c) radiographic results and MRI findings (ie, Cobb angle, vertebral collapse, endplate destruction, loss of cerebrospinal fluid [CSF] anterior and posterior to the cord, signal cord changes, posterior element involvement, epidural abscess/granulation tissue, canal encroachment, and level of spine involvement). All factors were recorded as present or absent, except for (i) age, which was recorded in years; (ii) ESR, which was recorded as <80 or >80 mm/h; (iii) CRP level, which was recorded as <20 or >20 mg/L; (iv) kyphosis, which was classified as <30o or >30o using the Cobb method11,12 (ie, by evaluating the angle between the upper border of the upper normal vertebra and the lower border of the lower normal vertebra) (Figure 1); (v) anterior vertebral height loss percentage (AVH loss),13 which was recorded as <50% or >50% anterior vertebral body height loss; and (vi) percentage of canal encroachment area (CEA), which was calculated on the axial image at the site of maximum compression using the Surgimap software (the maximum of spinal cord compression area/average canal area × 100). The average canal area was calculated as the average canal area of the vertebrae proximal and distal to the diseased segment14 (Figure 2). The patients were divided into the neurological deficit group (Frankel grades A, B, or C) and the control group (Frankel grades D or E). Surgeries in patients with neurological deficits included posterior decompression, costotransversectomy for anterior spinal cord decompression, and posterior pedicle screw fixation. In patients without neurological deficits, tissue biopsy and abscess drainage were performed using the transpedicular technique.
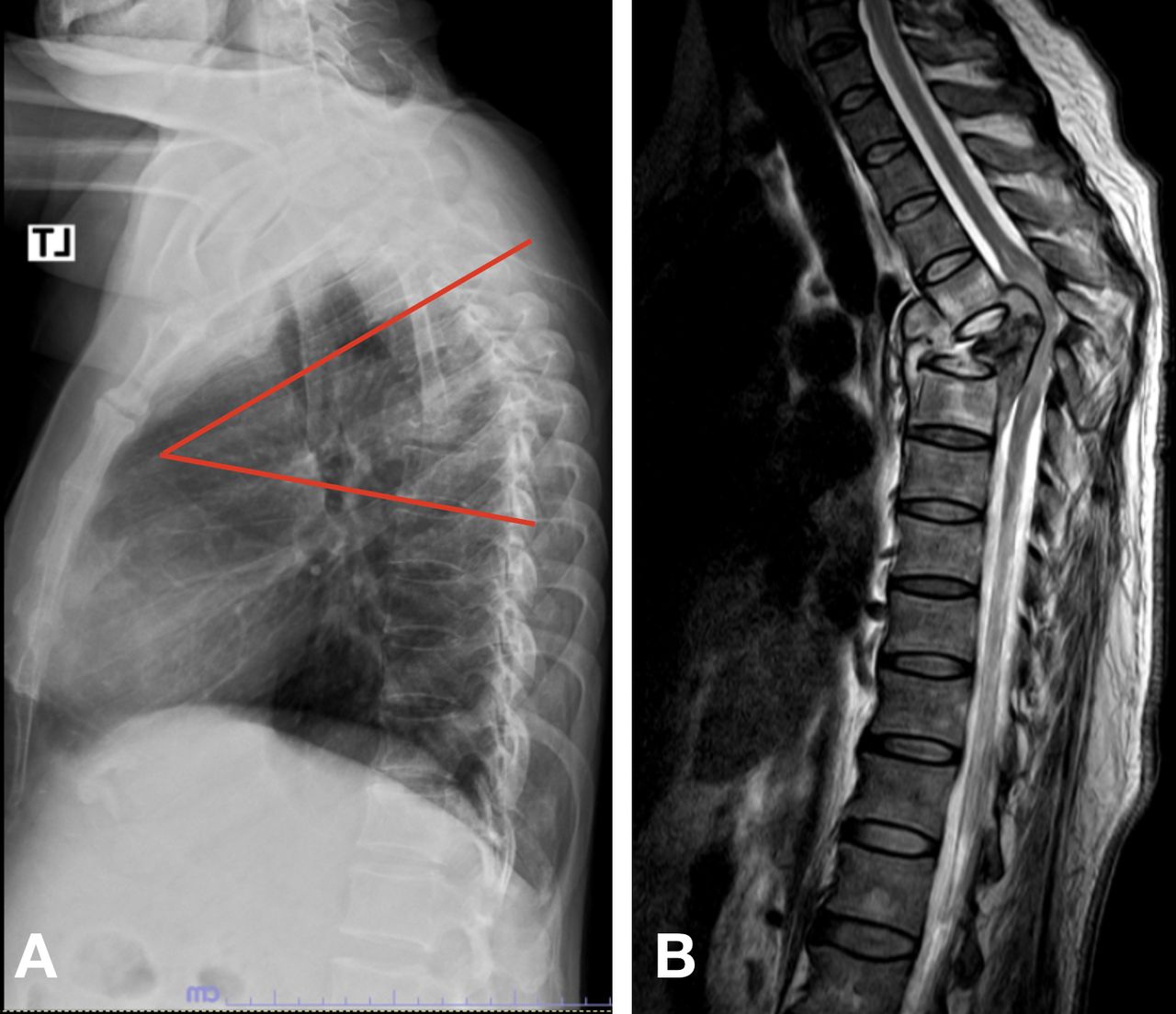
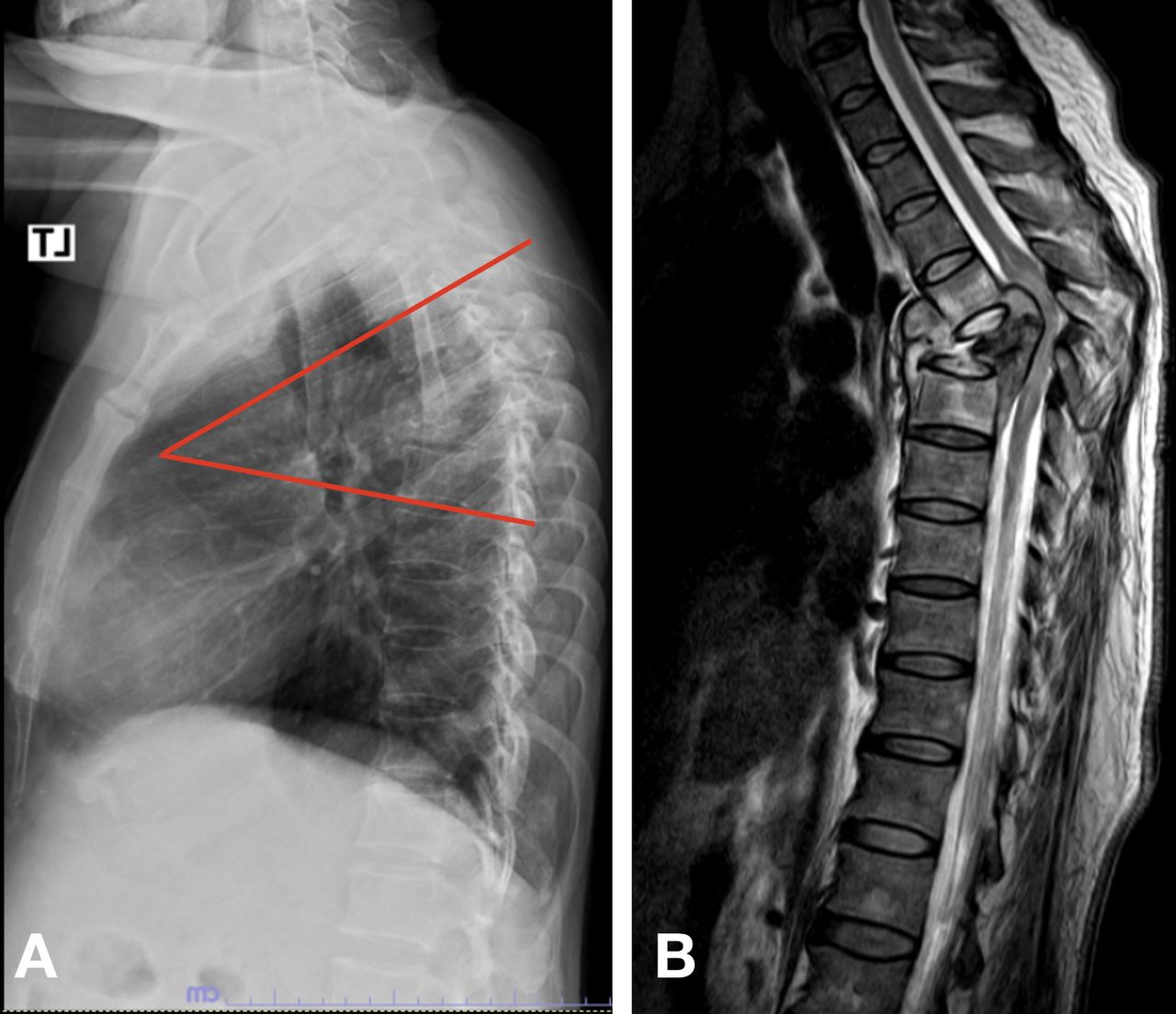
(A) Measurement of kyphosis deformity using the Cobb method (ie, evaluation of the angle between the upper border of the upper normal vertebra and the lower border of the lower normal vertebra). (B) Hyperintense signal cord change (together with anterior and posterior spine destruction) at the area of the kyphotic deformity on the T2-weighted image.
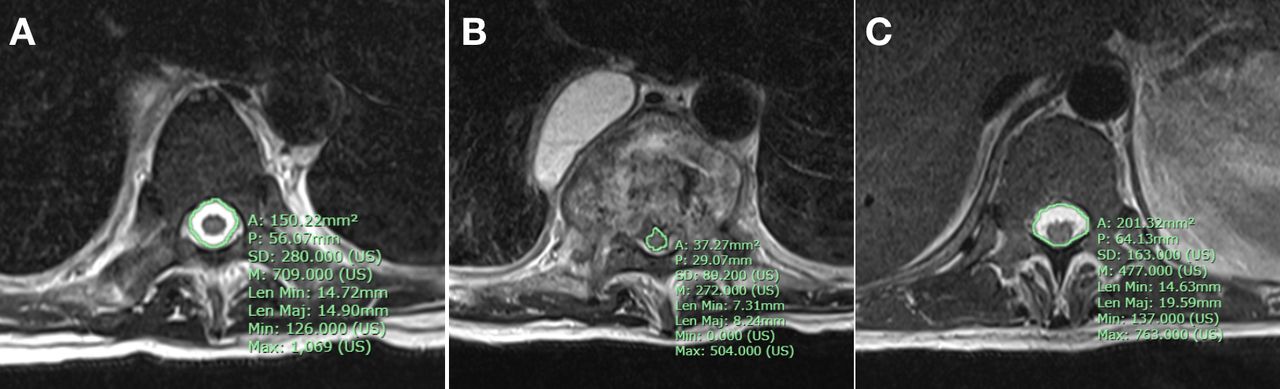
Surgimap magnetic resonance imaging software was used to measure canal encroachment in an axial section. (A) The cross-sectional area of the canal level was above the site of maximum compression. (B) The area occupied by the spinal cord at maximum compression. (C) The cross-sectional area of the canal level was below the site of maximum compression. The average canal area was calculated by obtaining the average canal area of the vertebrae proximal and distal to the diseased segment. The percentage of canal encroachment area (CEA) reflected the maximum compression of the spinal cord area/average canal area ×100.
Statistical Methods
The descriptive statistics included means, SDs, and 95% confidence intervals (CIs). The baseline demographic data were compared between the neurological deficit and control groups. Independent t tests and nonparametric tests were used to compare continuous and categorical data, respectively. Univariate and multivariate logistic regression analyses were used to determine the risk factors for neurological deficits. Variables that indicated an association with neurological deficits in the univariate analysis (ie, P < 0.2) and in the literature15 were included in the multivariate regression analysis. Backward logistic regression was used to construct the model. The overall significance level was set at P < 0.05. All data were analyzed using Stata Statistical Software (version 14; StataCorp LP., College Station, TX, USA).
Results
A total of 115 patients with thoracic spinal TB, including 57 men (mean age, 55.87 ± 16.9 years) and 58 women (mean age, 58.48 ± 15.32 years), were enrolled in our study. The mean age of the patients was 57.19 years (range, 24–85 years). The most common disease location in the thoracic region was the distal thoracic region (T9-L1) (62.6%), followed by the middle thoracic (T5-T8) (27.8%) and proximal thoracic (T1-T4) (8.7%) regions and extensive lesions (0.9%). Paradiscal involvement was the most common type of involvement, observed in 73% of the cases (n = 84), followed by panvertebral (13%, n = 15), central (11.3%, n = 13), and posterior involvement (2.6%, n = 3). Abscesses were the most common compressive pathology (72%, n = 83), followed by vertebral body bulging (12.1%, n = 14) and granulation tissue (11.3%, n = 13). The average number of vertebral bodies involved was 1.73 (range, 1–4). The descriptive data of the patients in the 2 groups are summarized in Table 1. The 2 groups showed a statistically significant difference (P < 0.05) in terms of the location of thoracic involvement, loss of CSF posterior to the cord, presence of cord signal changes, and >50% canal encroachment (Table 1).
Demographic data of the spinal thoracic tuberculosis patients at the initial visit.
BMI >25, onset of clinical back pain for 30–90 days, level of thoracic involvement, CRP level >20 mg/L, panvertebral involvement, loss of CSF posterior to the cord, cord signal change, and canal encroachment >50% were possible risk factors for neurological deficits in the univariate analysis (P < 0.2) in our study (Table 2). Multivariate logistic regression analysis showed that BMI >25 (adjusted OR = 16.18; 95% CI 1.60–163.64; P = 0.018), cord signal change (adjusted OR = 7.42; 95% CI 1.85–29.74; P = 0.005), and canal encroachment >50% (adjusted OR = 51.86; 95% CI 5.53–486.24; P = 0.001) were independent risk factors for neurological deficits (Table 3).
Results of univariate analysis of possible risk factors.
Results of multivariate analysis of possible risk factors.
Discussion
Antituberculous drugs are the mainstay of treatment for spinal TB, and surgery is performed to improve the effects of medical treatment.6,16 However, patients with spinal TB may show neurological deficits, so identification of the clinical and radiologic risk factors that can predict neurological deterioration and guide the addition of surgical decompression to medical treatment is essential.17 In this study, the mean patient age was 57.2 years. The distal thoracic region was the most commonly affected region (62.2%), followed by the middle thoracic region (27.2%) and the proximal thoracic spine (8.7%). Paradiscal involvement was the most common type of presentation (73%), followed by panvertebral (13%) and central (11.3%) presentation. Most cases showed compression by abscesses (72%). Similar findings have been reported in previous studies.6,8,18 In our study, the total rate of surgical decompression was 73.9%. Frankel grades A, B, and C neurological impairments in these individuals resulted in surgical decompression rates of 95.8%, 95%, and 70.3%, respectively. According to the results of our study, BMI >25, cord signal alterations, and canal encroachment >50% are significant risk factors for neurological impairments and should be considered when treating patients with thoracic spinal TB.
A large number of patients present with advanced disease for the first time, and delayed treatment of spinal TB has been reported to lead to the progression of neurological deficits in 23%–76% of the cases.17,19 In our study, 61.7% of the patients presented with neurological deficits categorized as Frankel grades A, B, or C, and the high proportion of such cases is likely due to the fact that our study included complicated cases referred for management at our tertiary care hospital.
Neurological deficits in patients with active thoracic TB can be caused by factors such as age and comorbidities. Mechanical compression is caused by mass effects such as abscesses, granulation tissue, and vertebral bulging. Mechanical instability of the spine caused by structural destruction of the vertebral column and the cord itself can cause infection, inflammatory edema, and intrinsic cord changes, leading to neurological deficits.16 We considered all of these risk factors while evaluating neurological deficits in this study.
In our study, univariate analysis showed that the ORs of canal encroachment >50%, cord signal change, loss of CSF posterior to the cord, panvertebral involvement, BMI >25, CRP level >20th mg/L, duration of onset, and level of thoracic involvement were 18.07, 16.8, 7.55, 4.64, 3.97, 2.19, 0.5, and 0.12, respectively (all P < 0.2). In addition, multivariate logistic regression analysis showed that the adjusted ORs for canal encroachment >50%, cord signal change, and BMI >25 were 51.86 (P = 0.001), 7.42 (P = 0.005), and 16.18 (P = 0.018; Tables 2 and 3), respectively. Thus, these 3 were considered independent risk factors that can be used to predict neurological problems in patients with thoracic spinal TB. In the multivariate analysis, the duration of clinical symptoms had an adjusted OR of 0.09 (P = 0.04), since patients with severe TB usually visited hospitals early.
Among the laboratory investigations, elevated ESR and CRP levels were recommended over leukocytosis, which has proven to be less useful.20,21 While Tan et al22 reported that ESR was a predictive factor for neurological deficits, ESR was not a predictive factor for neurological deficits in our study. Instead, our findings were consistent with those reported by Sudprasert et al,21,23 who observed elevated CRP levels in patients with spinal TB with neurological deficits and used an earlier decline in the CRP level postoperatively to determine neurological recovery. Similar to that study, a high CRP level (>20 mg/L) was the only laboratory indicator of neurological deficits in the univariate analysis in our study. However, it was not found to be an independent risk factor in multivariate analysis.
The radiographic changes associated with TB include a characteristic loss of bone density in the anterior spine and destruction of the vertebral endplate and vertebral body (Figure 3). These changes can also result in kyphotic deformities, which can be evaluated using the Cobb method. While previous studies9,10,24 reported that a kyphotic angle >30° was a predictive factor for neurological deficits, in our study, kyphosis >30° was not a predictive factor for neurological deficits. Since our patients with neurological deficits (Frankel grades A, B, or C) had severe back pain, they could not be positioned upright for radiography. Thus, the kyphotic angle measurements were underestimated in comparison with those obtained using upright radiography.
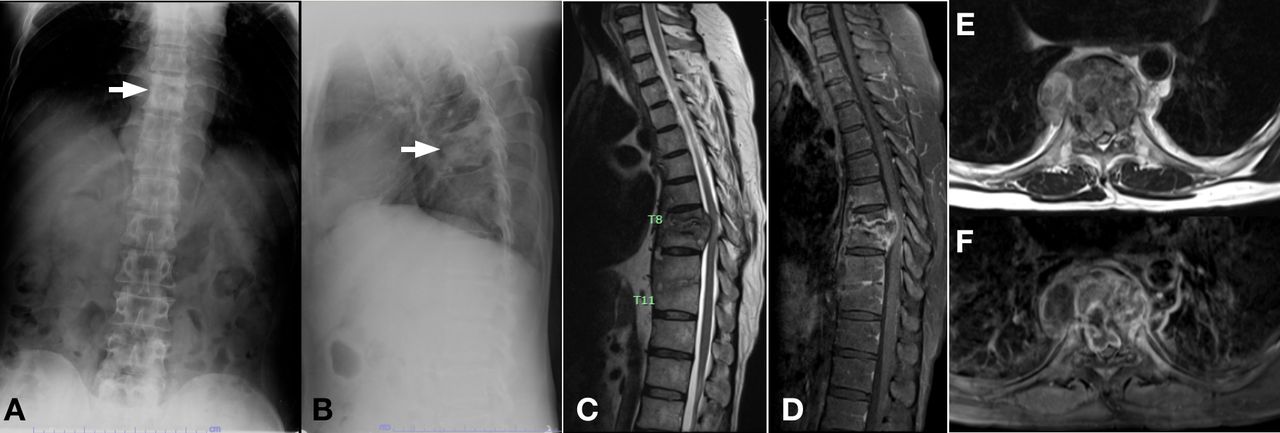
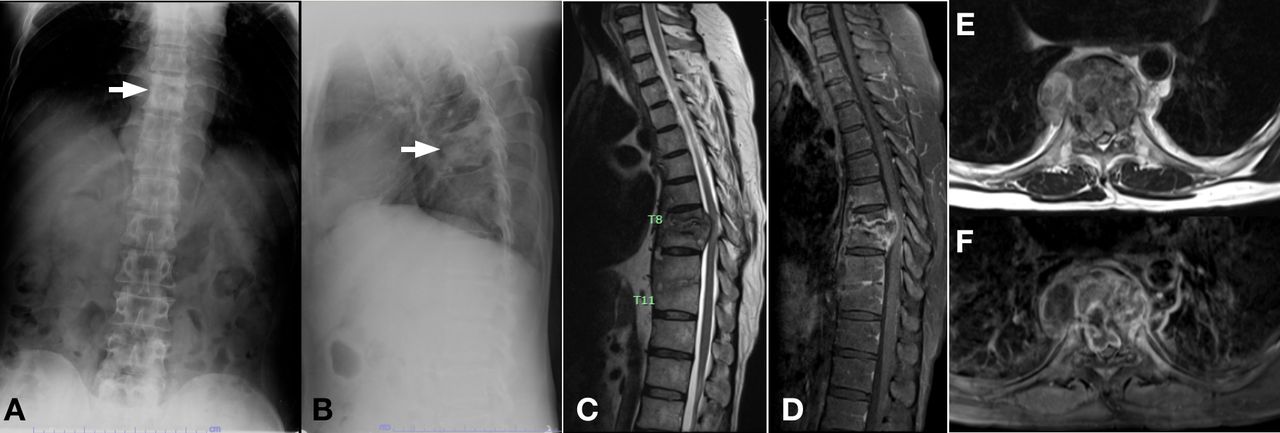
A 46-year-old male patient diagnosed with spinal tuberculosis at the T8–T9 segment and a neurological deficit (Frankel grade B). Radiographs in the anteroposterior view (A) and lateral view (B) show blurred endplates of T8–T9 (arrow) with kyphosis of 20° measured using the Cobb method. Sagittal T2-weighted (T2W; C), sagittal T1-weighted + gadolinium (T1W+Gd; D), axial T2W (E), and axial T1W+Gd (F) magnetic resonance images show paradiscal involvement of the T8–T9 vertebral bodies with endplate destruction and changed marrow signal intensity, prevertebral and epidural collection, which caused loss of anterior and posterior CSF around the cord and cord compression.
MRI currently provides better information regarding neural structures, the central canal, and spinal cord lesions (Figure 3). In patients with spinal TB, the spine appears different on MRI because the vertebral body and endplate are severely damaged, showing signs of osteomyelitis, and the paravertebral or epidural abscess has spread into the epidural space.16 In our study, patients with neurological deficits showed statistically significant differences in the proximal thoracic level, loss of posterior CSF, panvertebral spinal involvement, canal encroachment >50%, and the presence of cord signal change. However, significant independent risk factors for neurological deficits were canal encroachment >50% and cord signal changes. These findings are consistent with those reported by Subhadrabandhu et al,25 who showed that spinal TB at the proximal level and vertebral body loss were more commonly associated with neurological deficits. Similarly, Sae-Jung et al9 reported that disease location, signal cord changes, and epidural abscesses were associated with neurological deficits. Jain et al14 found that 76% of cases showing canal encroachment in patients with active TB had intact neurological findings. This is because the cord is flexible and possesses a physiological reserve for gradual compression. However, a deficit can occur with a lesser degree of encroachment if more than 1 factor is present, as observed in this study. In this regard, we found that BMI >25 was also a risk factor for neurological deficits in thoracic TB patients. This is due to the fact that being overweight seems to be a potential mechanism through an event of mechanical instability. Also, when the spinal cord is mechanically compressed, it is more likely to be damaged by a mechanically unstable event.
The findings of this study indicate that patients with thoracic spinal TB who present with back pain and a normal neurological status should undergo MRI of the spine as soon as possible to identify disease location, vertebral body destruction, cord signal changes, loss of CSF posterior to the cord, and canal compromise, since all of these findings are significantly associated with neurological deficits in the thoracic spinal TB. BMI >25, cord signal changes, and canal encroachment >50% are important predictive factors for neurological deficits, as evidenced in our study, and thus should be evaluated while planning treatment for patients with thoracic spinal TB. Among these 3 factors, canal compromise >50% showed the highest odds for neurological deficits, with the odds of developing neurological deficits being 50 times higher in patients with severe canal encroachment than in those without severe canal encroachment. Moreover, patients with an altered cord signal were 7 times more likely to develop neural deficits than those with a normal cord signal, while the risk estimate for developing neurological deficits was 16 times higher in overweight patients than in those with a normal weight.
This study had several limitations. First, this study had a retrospective design and only included cases from a single hospital. Second, neither our findings nor an analysis of the clinical features of TB in the spine was made. Third, given that this study involves patients who were referred to our tertiary hospital, there might be selection bias.
Conclusion
Thus, the predictive factors for neurological deficits in thoracic spinal TB are overweight (BMI >25), canal compromise of more than 50%, and spinal cord signal changes on MRI. These independent risk factors can help surgeons choose early decompressive surgery to prevent morbidity due to neurological deficits.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval Ethics approval was obtained from the Maharat Nakhon Ratchasima Hospital Institutional Review Board: MNRH IRB No. 086/2019
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.