


Abstract
Background Cervical spondylotic myelopathy (CSM) is the most common degenerative dysfunction of the spinal cord in the cervical spine in patients older than 55 years. The Japanese Orthopedic Association developed a scoring system to quantify clinical impairment of CSM patients, allocate them according to the degree of impairment, and suggest best timing for surgery. The original version evaluates the upper limb motor function through the ability of feeding with chopsticks, which are not intrinsic in western populations. To compare severity and treatment improvement of any diseases, it is preferable to have modified and translated versions of questionnaires and scores closest to the original ones. The authors present a prospective cohort study to validate the 17-point Brazilian Portuguese translated version of the modified Japanese Orthopedic Association (mJOA-BR17) survey.
Methods Patients with CSM (n = 36) were allocated to the disease group, while age- and sex-matched healthy volunteers (n = 34) were recruited for the control group. Comparison of statistical analysis of mJOA-BR17 domains for each group was established. After the translation and adaptation of mJOA-BR17, the validation was made through application to the 2 groups.
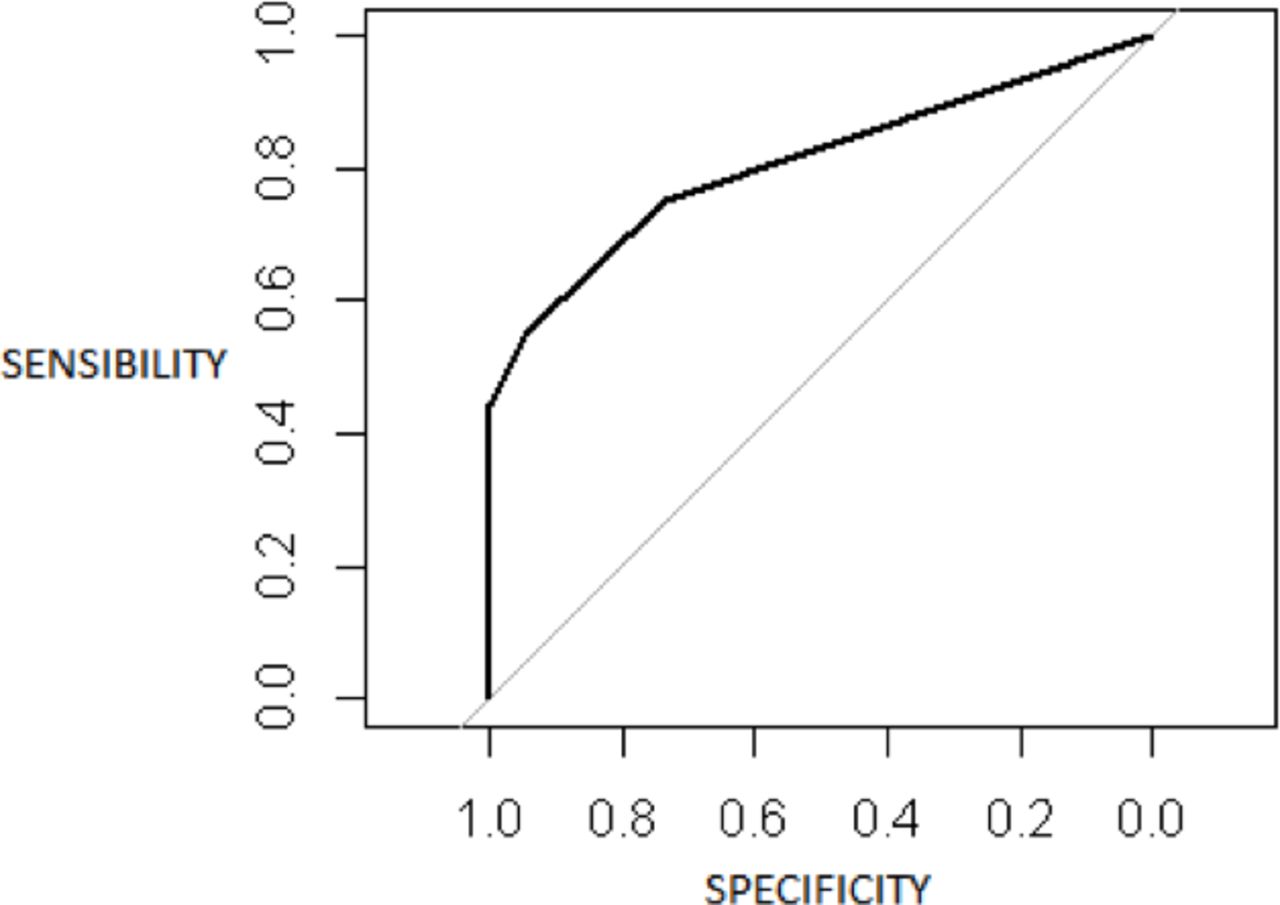
Results There were statistical differences between groups in total mJOA-BR17 score (CSM, 14.14 ± 2.92; control, 16.68 ± 0.59: P < 0.001), lower limbs motor function (CSM, 3.25 ± 1.02; control, 3.91 ± 0.29: P < 0.001), upper limbs sensory function (CSM, 1.17 ± 0.81; control, 1.86 ± 0.36: P < 0.001), lower limbs sensory function (CSM, 1.62 ± 0.64; control, 2.0 ± 0.0: P < 0.001), and bladder function (CSM, 2.69 ± 0.52; control, 2.97 ± 0.17: P = 0.005). The receiver operating characteristic curve was 0.81, indicating usefulness of the mJOA-BR17 score to identify patients with CSM from healthy controls.
Conclusions The mJOA-BR17 demonstrated similarity, applicability, and good understanding in comparison to the English-modified version of 17-point JOA score for CSM, becoming a valuable tool to quantify and differentiate CSM patients from healthy individuals.
Level of Evidence 4
INTRODUCTION
Cervical spondylotic myelopathy (CSM) is the most common degenerative dysfunction of the spinal cord in the cervical spine in patients aged 55 years or older and may have massive clinical impacts. Then, CSM can progress to severe disability and functional impairment. Early diagnosis and accurate clinical evaluation are mandatory to achieve better treatment results.1–4
The Japanese Orthopedic Association (JOA) developed a scoring system to quantify clinical impairment of patients with CSM, allocate them according to the degree of impairment, and thus suggest the best timing for surgery. Moreover, the JOA score for CSM is used worldwide in studies about CSM as a valuable tool for severity and outcome evaluation.1,5–7
The JOA score for CSM has 4 domains that cover most myelopathy symptoms: (1) Motor dysfunction of upper extremity; (2) motor dysfunction of lower extremity; (3) sensory deficit (upper and lower extremities and trunk); and (4) sphincter dysfunction. The total score is obtained by summation of the 4 domains resulting in a maximum of 17 points. The original version also evaluates the upper limb motor function through the ability of feeding with chopsticks, which are widely used in Asian cultures but not intrinsic in western populations. Because of that, some English-modified translated versions were published few years after the original JOA score for CSM.8
Modified JOA (mJOA) versions from Chiles et al9 and Benzel et al10 are usually used to address CSM in western countries (Table 1). However, they have some crucial differences: The version from Chiles et al tried to stay close to the original, and the only major adaptation was the substitution of the ability to use chopsticks for the ability to use a fork and knife, allowing the tool to keep the maximum total score to 17 points, which is the same as the original version. In the version from Benzel et al, the tool evaluates the upper limbs motor function through the capability of buttoning a shirt, which added an extra point to that domain for a maximum total score of 18 points. However, the additional point adds difficulty to pooling outcomes of different studies together and also depends on patients buttoning shirts quite frequently.9,10
mJOA and final mJOA-BR17.
Worldwide, to compare severity and treatment improvement of any diseases, it is preferable to have modified and translated versions of questionnaires and scores closest to the original ones as possible, such as the same domains and total score values. Speaking in CSM, that is not different, and the standardization and universalization of outcome measurements are strictly recommended, allowing centers worldwide to speak the same language even for independent studies.
The objective of the present study ws to perform the translation and cultural validation of the original 17-point modified version of the JOA score for CSM published by Chiles et al9 through a scientific method previously established by Beaton et al.11
MATERIALS AND METHODS
Translation
The method previously described by Beaton et al11 was followed in order to reach the Brazilian Portuguese version of mJOA score.9 Briefly, the method by Beaton et al consists in translation, back translation, and development of final version by 2 English and 2 Portuguese first language translators naive to the objective of this study. This original version is named the 17-point Brazilian Portuguese translated version of the modified Japanese Orthopedic Association score (mJOA-BR17). The cultural adaptation, linguistic adaptation, and validation were also performed as described in the following paragraphs.
Two Brazilian Portuguese native translators, who were also fluent in English independently and were blinded to the study objective, translated the English version of mJOA to Portuguese. These versions were compared and analyzed by 2 other researchers consisting of a spine surgeon and a spine physical therapist and resulted in the first Brazilian Portuguese version of mJOA-BR17.
After the first Portuguese version, a back translation to English was made by 2 translators independently, both of whom used English as their native language and were also fluent in Portuguese and were blinded to the objectives of this study. Again, the versions were compared and analyzed by the other 2 researchers. The next step was a final translation to Portuguese in the exactly the same way as the first translation was made 30 days after the first translation, resulting in the final version of the mJOA-BR17 (Table 1).
Participants
The includsion criteria were the presence of clinical and radiographic diagnosis of cervical myelopathy and cervical canal stenosis, recruited as soon as the diagnostics were made in sequence of admission in the spine surgery department of our institution. Other criteria were age of more than 18 years, any gender, and literate who could read and understand the form.
Patients with cognitive deficits; neurological degenerative diseases; visual, verbal, and motor inability to communicate;, and motor loss due to other causes besides myelopathy were not included in this study to avoid confounding bias.
Healthy volunteers without back problems and without neurological impairment of any nature were included as the control group, which was comparable to studied group in matter of gender and age.
All participants signed the consent form approved by the Institutional Review Board number (CAAE 59169016.7.0000.0071) at Albert Einstein Hospital.
Pretest
At this step, 10 participants were enrolled, 5 patients with CSM and 5 controls, and a pretest with translated questionnaire was made. Participants also had to respond regarding their comprehension about the translated version of mJOA-BR17, giving any other commentaries about the text, and they were prompted to give suggestions to improve it. After that, the final version was ready to be applied.
Finally, the documentation and results of all steps to translate and cultural adaptation of mJOA were sent to the author of the original version in English to guarantee the fidelity of the process and final version.
Questionnaire Application
At the second part of this study, the final translated version of mJOA-BR17 was applied to the participants. It also filled up a form with demographic characteristics with additional information of all participants. All of this information will be described in the results section later in this manuscript.
Because pain is a common symptom in patients with cervical disease, the visual analog scale (VAS) was applied to all patients in order to register whether they had any pain at the moment of the evaluations.
Statistical Analysis
Data analysis included the description of variables through mean, SD, median, interquartile interval (first and third quartiles), and minimum and maximum values.12 The studied groups were compared using the Mann-Whitney U test. Then, to verify the capability of the mJOA-BR17 score to identify affected patients using only 1 domain, the receiver operating characteristic curve was made.13 Statistical analysis was performed using the statistical package R (https://www.r-project.org/) with the significance level of P < 0.05.
RESULTS
This study enrolled 70 participants: 36 patients in the CSM group (mean age 56.90 ± 11.41 years) and 34 healthy volunteers in the control group (mean age 62.45 ± 11.42 years). Table 2 presents the summary of age, total mJOA-BR17 score, and VAS results.
Summary of age, mJOA-BR17 total score, and VAS.
Table 3 presents the domains of mJOA-BR17 results independently.
Results of the mJOA-BR17 domains.
The Mann-Whitney U test abetted to show differences between the CSM group and control group. There were statistically significant differences in VAS (P < 0.001), mJOA-BR17 total score (P < 0.001), lower limbs motor function (P < 0.001), upper limbs sensory function (P < 0.001), lower limbs sensory function (P < 0.001), and bladder function (P = 0.005). The motor function of the upper limbs domain also had a significant difference (P = 0.007). The remaining domain, trunck sensory funtion, did not show statistical significance (P = 0.173; Table 2).
To verify whether the mJOA-BR17 score is capable of distinguishing patients with CSM in comparison to the control volunteers, the receiver operating characteristic curve was calculated and had an area under the curve of 0.81 (Figure).
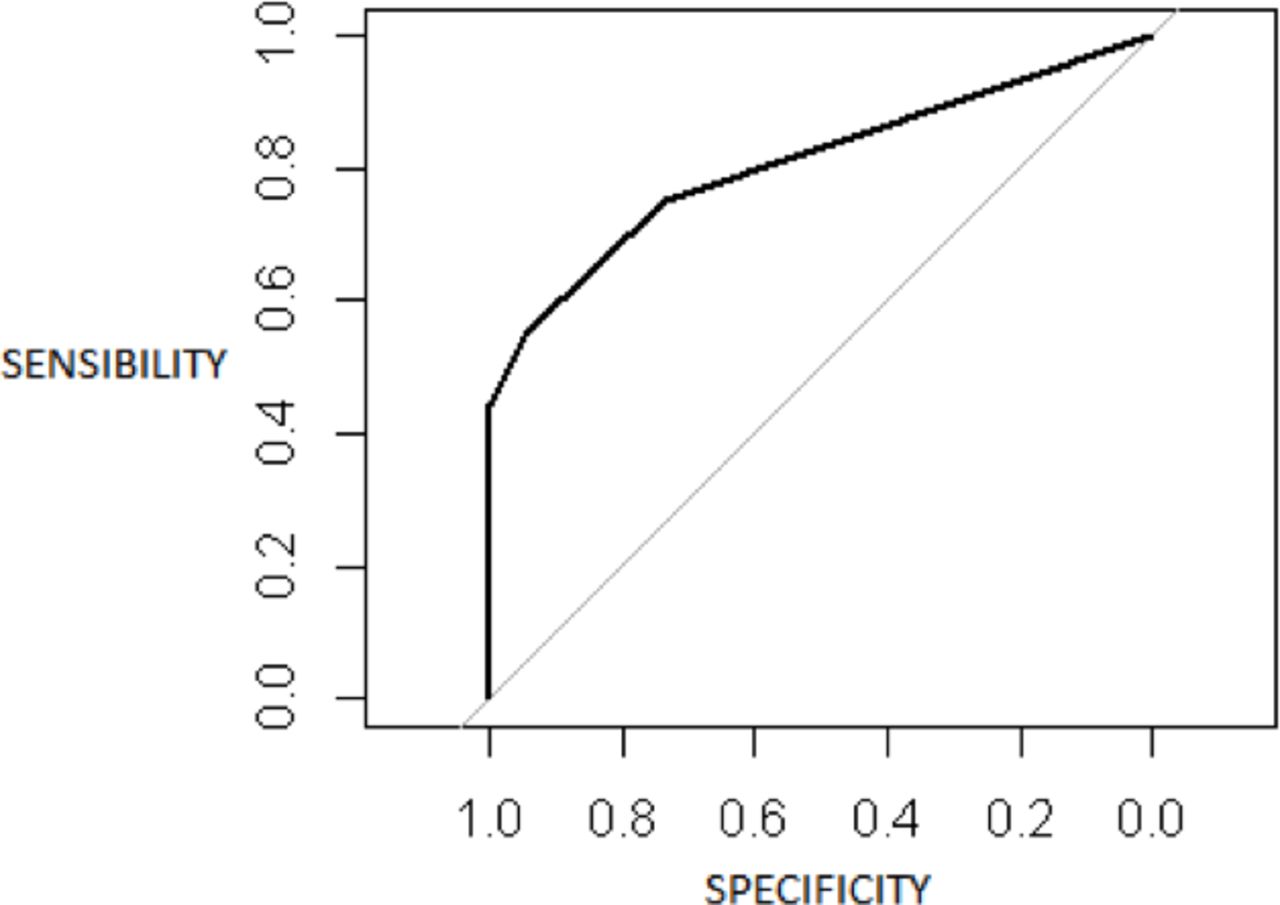
Receiver operating characteristic curve 17-point Brazilian Portuguese translated version of the modified Japanese Orthopedic Association score. Area under the curve is 0.81.
This finding supports the difference between 2 groups, which was already identified through the Mann-Whitney U test.
DISCUSSION
Good research practices must include standardized outcome methods. It is crucial to speak a universal language, which allows researchers to compare and combine results from independent centers in meta-analyses or multicentric studies. Brazilian studies should be comparable to other nations studies and use the same original or equivalent/modified outcome tools.
Numeric instruments, such as questionnaires, scales, or scores, help to simplify data analysis in a clear and objective way. JOA score and its modified versions5,6,9,10,14 are valuable instruments to evaluate limb motricity, sensory function, and sphincter dysfunction. It is preferable that any questionnaire or score use the local language as well as be validated with local culture.
There are some English-modified versions of JOA, originally in Japanese and based on Asian cultures. The most popular versions of the JOA are those by Chiles et al,9 which has a total score of 17 points, is very close to the original JOA,5 and substitutes fork and knife use for chopstick use to evaluate the function of upper limbs , and by Benzel et al,10 which has a total score of 18 points and adds the capability of buttoning a shirt to upper limbs motor function evaluation.
The present study used the Chiles et al modified English version motivated by the fact that this version has exactly the same total score of the original JOA (17 points) and is the closest to the original JOA after comparison by a Japanese orthopedic surgeon also fluent in English language.
Moreover, when evaluated in detail, Chiles et al’s version assesses the sensibility of upper limbs, lower limbs, and trunk independently, as well as the original version. In other words, structurally, Chiles’ mJOA version is divided in 4 domains: (1) motor dysfunction of upper extremity; (2) motor dysfunction of lower extremity; (3) sensory deficit (and this is divided in upper limbs, lower limbs, and trunk, independently); and (4) sphincter dysfunction. Those domains are exactly the same and have the same score count of the original version.
Benzel et al’s mJOA English version, despite being very popular among western spine centers, presents a total score of 18 points with different evaluation questions and lacks lower limbs and trunk sensibility assessment, resulting in a thwarting comparison of individual domains and total scores to the original JOA. Moreover, nowadays, use of button shirts could be different among genders and social-economic statuses and may not be a usual activity anymore—certainly not as trivial as the use of a fork and knife to feed.
Bartels et al14 proposed a standardization based on Benzel’s version; however, the approach of differences between scales did not mention the crucial dissimilarities between Benzel et al’s and the original JOA score that goes beyond total score values. Nevertheless, Benzel et al’s mJOA version still is a valuable tool used in many spine departments, and its importance is not being questioned here. However, worldwide standardization is a key point and is the reason why we chose to use the English-modified version closest to the original JOA. Other than that, a multiple line of evidence regarding CSM has been reported from Asian countries, including Japan. Therefore, using a compatible scoring system is valuable.
At the time the present study began, there were no published manuscripts about Brazilian versions of the mJOA to the author’s knowledge. However, during the process of data collection, 2 articles based on Basel’s version of the mJOA score were brought to public and called mJOA-br.15,16 That makes this study unique and baseline to other modifications since it approaches the mJOA version of 17 total score points proposed by Chiles et al, closest to original Japanese version, referred to here as mJOA-BR17.
Despite the global aging population and incidence of cervical myelopathy ranging between 6 and 76 per million, the inclusion of patients in cervical myelopathy studies usually is not an easy task. Therefore, one limitation of the present study is the number of patients included, which was defined using a convenience sample of patients without a previous sample test.
The original JOA score had its results compared with several other scales, such as Cooper Myelopathy Scale, European Myelopathy Scale, and Short Form-36, and these studies concluded JOA as a valuable and analogous tool, with additional advantages providing categorized details of clinical impairment.9,17,18
Despite the consistent difference observed between studied groups, the present analysis still has a specific limitation regarding a low number of severe CSM cases, which may bring less difference in trunk sensorial evaluation. This probably occurred due to our service being a private health reference in spine treatment and, in that case, having a focus on early diagnosis and treatment. Because of ethics, it is strongly recommended to treat CSM cases as soon as diagnose is made, avoiding, or even minimizing, permanent impairment.
Unlike other mJOA Portuguese versions, the mJOA-BR17 analyzes independently the sensory deficit in the trunk, upper, and lower limbs, which allow a better picture of each participant; however, it was not possible to say whether previous studies had similar trends.16 For that matter, more studies with a greater heterogeneity of patients, including a greater amount of severe stenosis cases, could possibly show strong difference in the sensory deficit trunk session of the mJOA-BR17 scale, as expected.
It is important to notice that, as previously mentioned, mJOA scales translated to different languages other than English have already been studied for specific validation and application in an international level.14 Translated scales to Dutch and Arabic were applied to 25 and 100 patients, respectively, both of which showed both high degrees of interobserver reliability.14,19 Another version in Italian, the mJOA-IT, was applied to an Italian population and was also shown to be reliable as an outcome measure for clinical e-research studies.20
As presented in this manuscript, the 17-point total score JOA is one of the most used tools in worldwide Asian spine centers, and the 18-point total score mJOA is very popular in Western countries; however, it is strongly recommended to authors of future studies to use both Portuguese validated versions, mJOA-BR17 and mJOA-br, in order to have results comparable to foreign studies regardless of the JOA version applied to them.
CONCLUSION
The mJOA-BR17 original version translation, adaptation, and validation based on the 17-point mJOA English version demonstrated similarity, applicability, good understanding, and great potential to universalization of this valuable tool in clinical and outcomes evaluation for patients with cervical myelopathy.
Acknowledgments
Statistical analysis was performed using the statistical package by an institutional statistical consultant. There was no other contribution from anyone who does not meet the criteria for authorship.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.