


Abstract
Background Mechanobiology can help optimize spinal fusion by providing insights into the mechanical environment required for bone healing and fusion. This includes understanding the optimal loading conditions, the mechanical properties of implanted materials, and the effects of mechanical stimuli on the cells involved in bone formation. The present article reviews the evidence for surface technologies and implant modification of spinal cages in enhancing spinal fusion.
Methods Databases used included Embase, MEDLINE, Springer, and Cochrane Library. Relevant articles were identified using specific keywords and search fields. Only systematic reviews, meta-analyses, review articles, and original research articles in English were included. Two researchers independently performed the search and selection process. A flowchart of the search strategy and study selection method is provided in the article.
Results The studies indicate that surface modification can significantly enhance osseointegration and interbody fusion by promoting cellular adhesion, proliferation, differentiation, and mineralization. Various surface modification techniques such as coating, etching, nanotopography, and functionalization achieve this. Similarly, implant material modification can improve implant stability, biocompatibility, and bioactivity, leading to better fusion outcomes. Mechanobiology plays a vital role in this process by influencing the cellular response to mechanical cues and promoting bone formation.
Conclusions The studies reviewed indicate that surface technologies and implant material modification are promising approaches for improving the success of spinal cage fusion. Mechanobiology is critical in this process by influencing the cellular response to mechanical signals and promoting bone growth.
Introduction
Mechanobiology and biomechanics are interrelated fields of study with different foci and approaches that often overlap in their research questions and techniques. These fields examine the mechanical properties and behaviors of biological systems using fundamental physics, engineering, and biology principles and aim to develop new strategies and technologies for improving health and performance.
Biomechanics studies the structural properties and mechanical behaviors of biological systems. In orthopedic biomechanics, our understanding continues to grow regarding behaviors of bone, articular cartilage, and soft tissues across different musculoskeletal regions. Innovative tools and analysis techniques have led to a better understanding of joint kinematics and tissue function during different activities. Mathematical modeling and improved engineering design of orthopedic implants have also progressed significantly. Biomechanical principles have been applied to address clinically relevant problems, improving patient treatments and outcomes through collaboration between bioengineers and orthopedic surgeons.1
Mechanobiology studies how cells sense mechanical stimuli and respond by altering growth, differentiation, and migration behaviors—a core principle known as mechanotransduction. It focuses on complex molecular machinery that regulates mechanical signaling pathways at cellular, tissue, and organ levels.2 A deeper understanding of how mechanical stress regulates cells can contribute to the functional advancement of these technologies.3
Relevance to Spine Surgery
Low back pain is a prevalent ailment that frequently arises as a result of degenerative disc disease. It is a primary contributor to work absenteeism, disability, and diminished quality of life.4 Chronic low back pain is primarily attributed to disc-related pain, followed by facet joint and sacroiliac joint pain.5,6 The worldwide occurrence of low back pain is estimated to be around 60% to 70%, with significant variations observed among individuals and regions. Young and middle-aged adults experience the highest occurrence of low back pain, resulting in prolonged disability, surpassing other ailments.7,8
Spinal fusion surgery alleviates chronic back pain, enhances spinal stability, and prevents further damage.9 The success of this surgery depends on factors such as the spinal condition’s severity, level of pain and disability, and overall health status. Spinal fusion surgery is usually recommended for patients with conditions causing instability10 or chronic pain, including degenerative disc disease,11 spinal stenosis, scoliosis,12 or a spinal fracture that failed conservative management. The surgical goals are reducing pain, improving function, providing stability, correcting deformity, and obtaining fusion. Applying mechanobiology principles and techniques can assist significantly in achieving spinal fusion as it is a complex procedure involving physical forces and chemical processes that promote bone tissue growth and fusion.
Mechanobiology investigates how mechanical forces, such as tension, compression, and stiffness, are sensed and transduced into biochemical signals, which affect cellular behavior, gene expression, and tissue organization.13 The extracellular matrix (ECM) communicates mechanical stimuli to cells through mechanotransduction, which generates different responses depending on the load’s type, magnitude, duration, and location. Knowledge of mechanobiology can assist in creating innovative approaches and technologies for spinal fusion that take advantage of the mechanical environment of the spine and the response of bone cells to mechanical stimuli.14 This can lead to the development of implants with enhanced biocompatibility and mechanical properties, including 3D-printed implants that mimic native bone architecture.15,16 The feedback loop between surgeons and engineers can guide implant development and optimization, ultimately improving the success rates of spinal fusion surgery and the quality of life for patients with spinal disorders.
Methods
Search Strategy
This article reviews the impact of implant material and surface technology on osseointegration and interbody fusion in spinal cages, along with describing the role of mechanobiology and mechanotransduction in these processes. Databases used to search for eligible studies included Embase, MEDLINE, Springer, and Cochrane Library. The foremost vital terms were mechanobiology, mechanotransduction, spinal fusion, interbody cages, surface technology, and osseointegration. Search fields chosen for these terms were title, author keywords, and abstract. Boolean operators (OR and AND) combined the keywords and retrieved all relevant articles.
Literature Selection
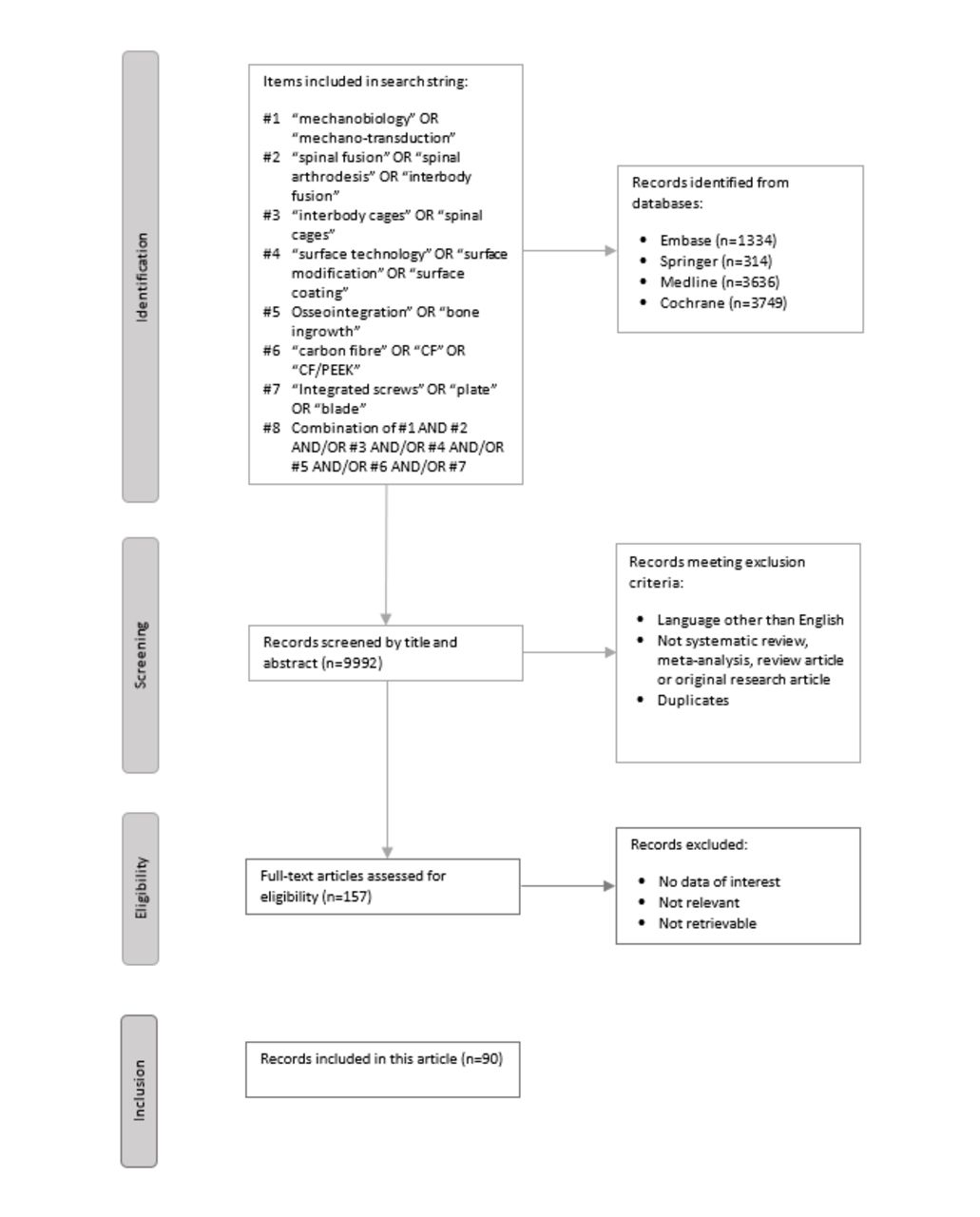
Only systematic reviews, meta-analyses, review articles, and original research articles were included. Articles in languages other than English were excluded. Titles and abstracts of articles that met the inclusion criteria were screened, followed by the retrieval of the relevant articles in full text. The eligibility of full-text articles was assessed, and irrelevant articles that did not have data of interest or could not be retrieved were excluded. Two researchers independently performed the literature search to reduce errors. Figure 1 illustrates a flowchart of the search strategy and study selection process.
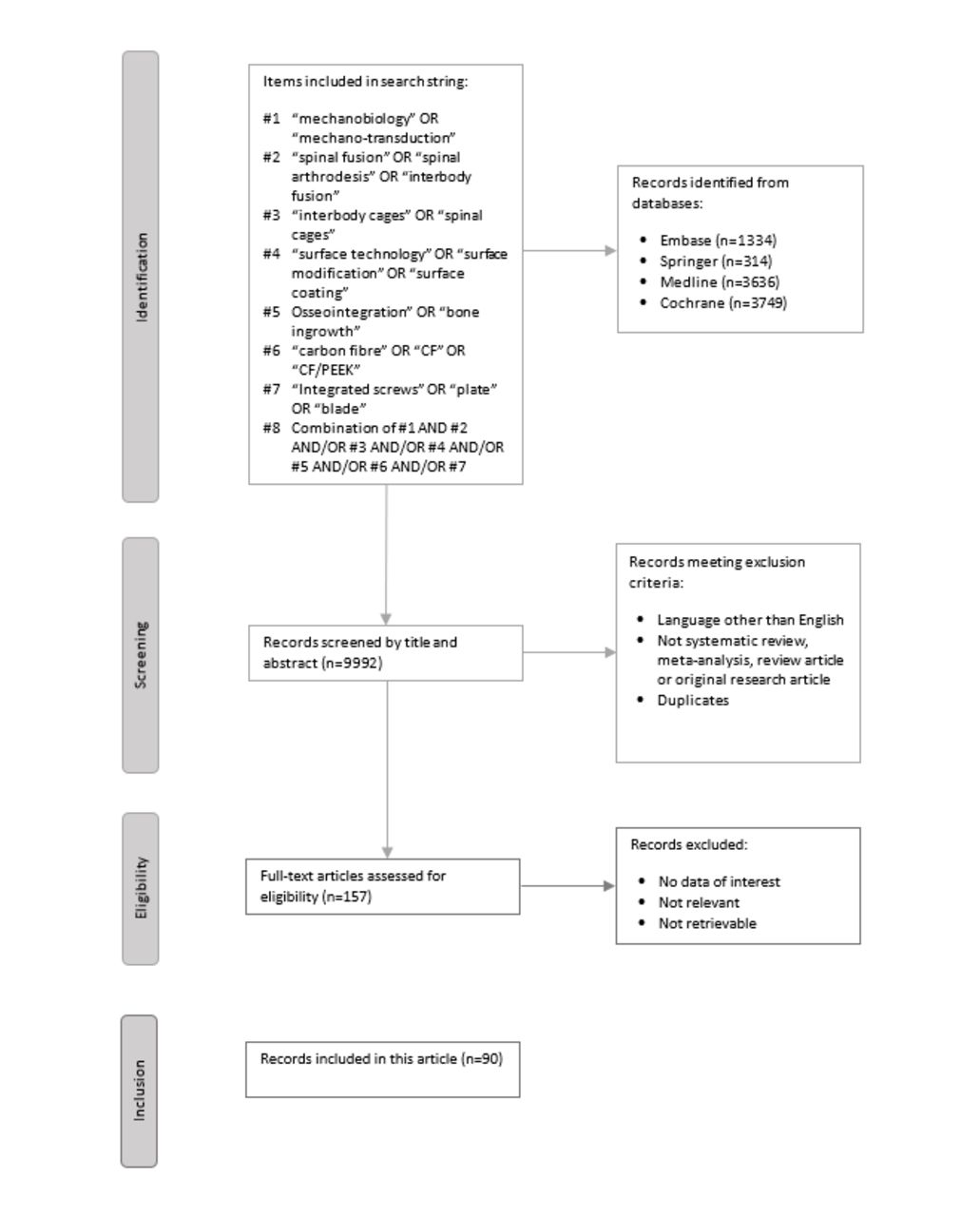
Flowchart of the search strategy and selection process for this article.
Basics of Mechanobiology
Force is essential to cell biology as it is crucial in physiological events such as cell division. Researchers have developed micro- and nanosensors to quantify cellular forces and measure the mechanical properties of cells, including the elastic modulus.17 However, cells and tissues exhibit viscoelastic behavior and can store and dissipate mechanical energy over time, which can be characterized using rheological models such as the standard linear solid model.18
The ECM is a 3D structure that provides biochemical and biophysical signals to guide cellular functions. Cells can modify the ECM through synthesis, degradation, and chemical alterations. The characteristics of the ECM, such as stiffness and porosity, play a crucial role in maintaining tissue homeostasis and directing cell fate.19 The ECM contains complex macromolecules and proteins, creating a unique microenvironment governing cell behavior. Cells can transduce mechanical signals from their surroundings through the adhesive binding sites on ECM components. However, the complexity of the native microenvironment makes it challenging to understand the mechanisms by which cells process these signals fully.
Research Techniques in Mechanobiology
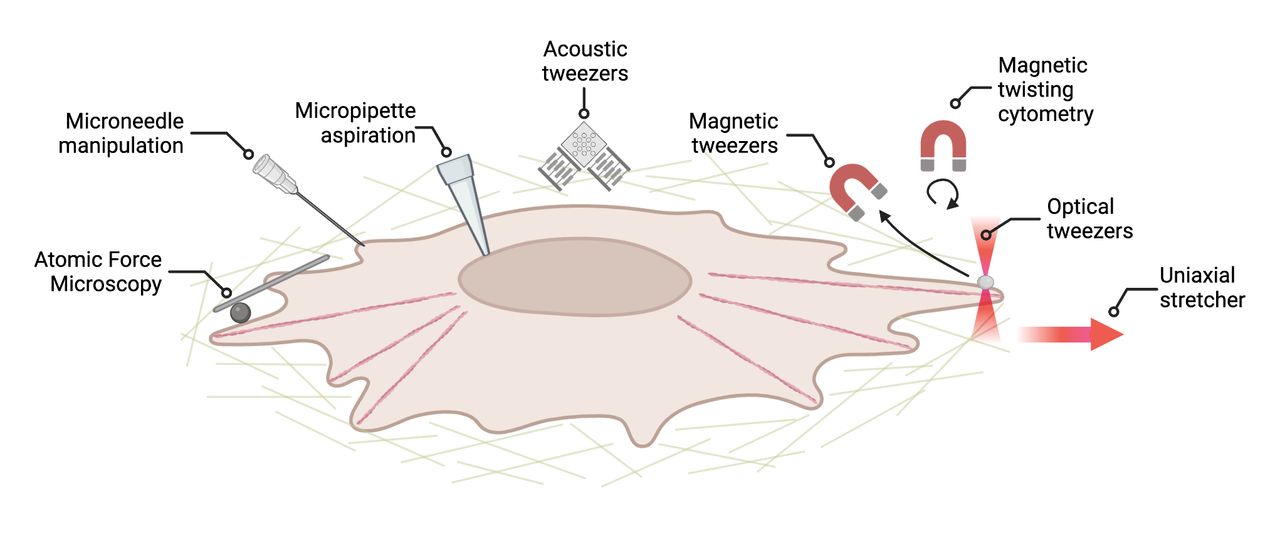
Smart hydrogels, 3D culture systems, coculture systems, and microfabrication techniques are promising alternatives to standard plastic dishes for cell culture.20 Various techniques, including cell stretching, microscopy, bioreactors, genetic manipulation, computational modeling, and tissue engineering, are employed to study mechanobiology. These techniques provide insights into mechanotransduction mechanisms by manipulating cell adhesion patterns and applying well-controlled forces to living cells and tissues to measure signaling pathways.21 Additional tools include optical and magnetic tweezers, micropipettes, and uniaxial stretchers (Figure 2).3,22
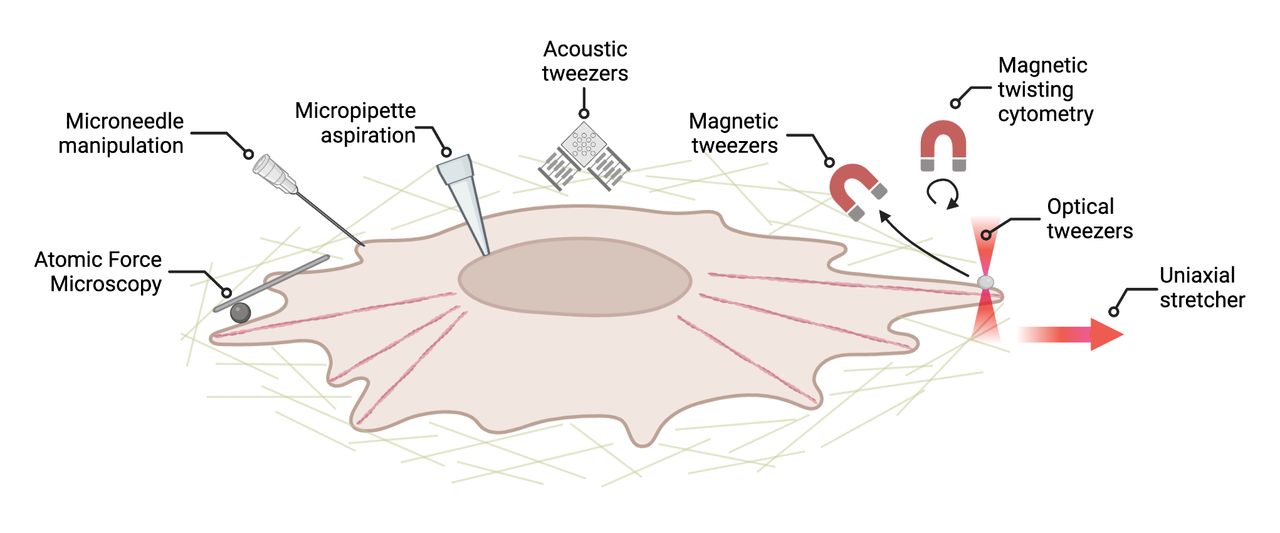
Different techniques are available to investigate mechanotransduction pathways, including atomic force microscopy, microneedle manipulation, micropipette aspiration, acoustic tweezers, magnetic tweezers, twisting cytometry, and a uniaxial stretcher (left to right). Adapted from Mohammed et al3 in accordance with Frontiers Creative Commons license. Copyright 2019 Mohammed, Versaevel, Bruyère, Alaimo, Luciano, Vercruysse, Procès, and Gabriele. Published by Frontiers Media.
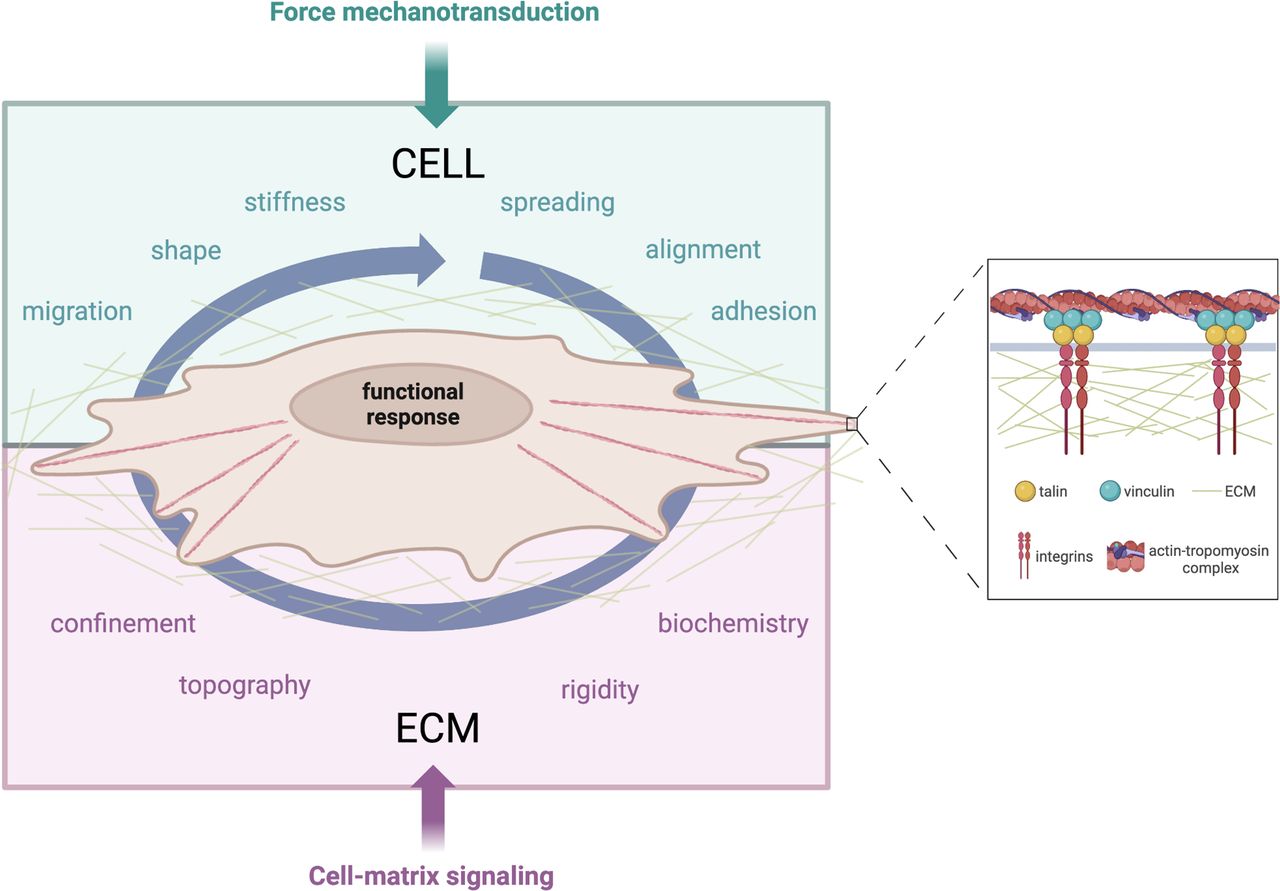
Integrins and transmembrane receptors connect adherent cells and the ECM. Mechanical signals are detected by focal adhesion sites, which trigger a biochemical response through the integrin signaling pathway, leading to actomyosin contractility. The mechanism by which mechanical signals are converted to biological responses is still under investigation. However, integrins are essential in mediating outside-in and inside-out signals (Figure 3).3
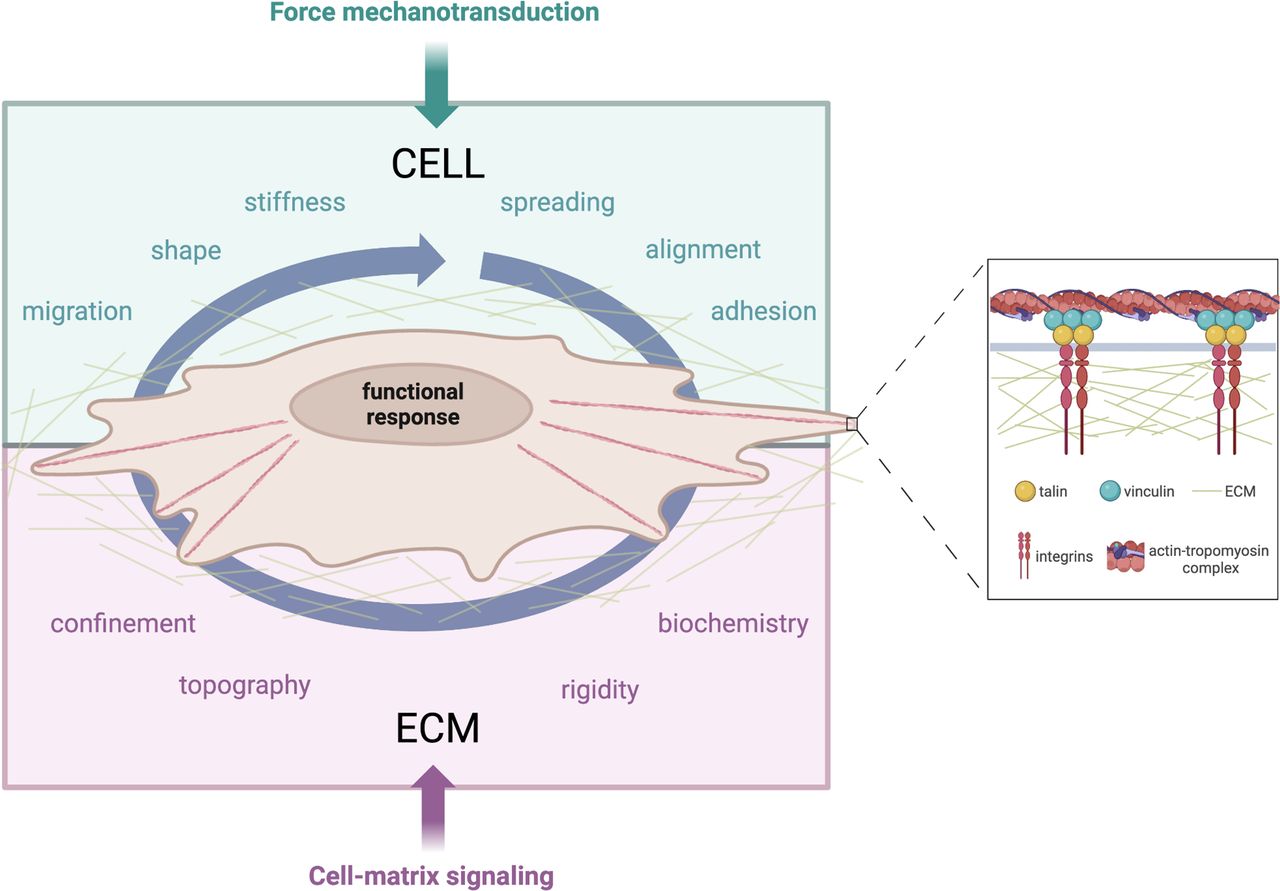
Illustration of force mechanotransduction (green) and cell-matrix signaling (purple) in a 3D fibrous matrix where a cell grows. Eukaryotic cells respond to external forces by modifying their migration, shape, stiffness, spreading, alignment, or adhesion behaviors. The extracellular matrix (ECM) presents several cues to cells, such as confinement, topography, rigidity, and biochemistry. Both types of mechanotransduction are facilitated by focal adhesion, which recruits transmembrane integrins. The nucleus converts mechanical signals (small arrows) into biological responses. Adapted from Mohammed et al3 in accordance with Frontiers Creative Commons license. Copyright 2019 Mohammed, Versaevel, Bruyère, Alaimo, Luciano, Vercruysse, Procès and Gabriele. Published by Frontiers Media.
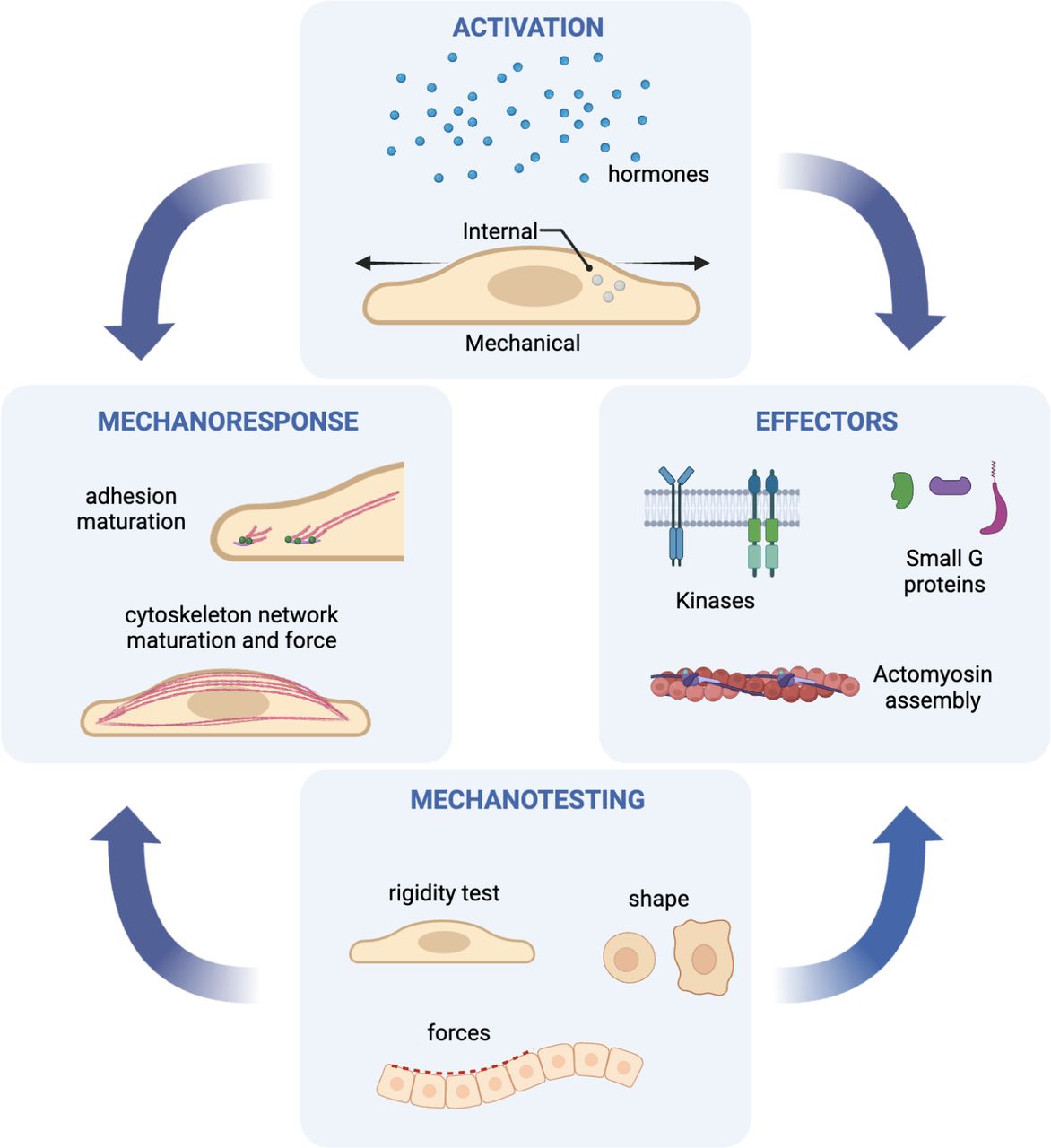
The cell adhesion process starts with actomyosin contractions of the integrin adhesions on the newly attached matrix. This causes them to adjust their size, strength, and dynamics in response to the applied forces and resistance of the matrix. Stiffer matrixes result in more extensive adhesions and more force-dependent signaling. Muscular adhesions activate the additional lamellipodial extension and retraction, leading to the next round of mechanosensing to evaluate matrix rigidity. Repeated patterns of cell edge activity, adhesion formation, and matrix testing determine the final cell morphology when it reaches a steady state.23 Once the cell has attached, it spreads and flattens out on the surface of the ECM or neighboring cells (Figure 4). This process involves the reorganization of the cell’s cytoplasm and the formation of new adhesion sites at the cell’s leading edge.22,23
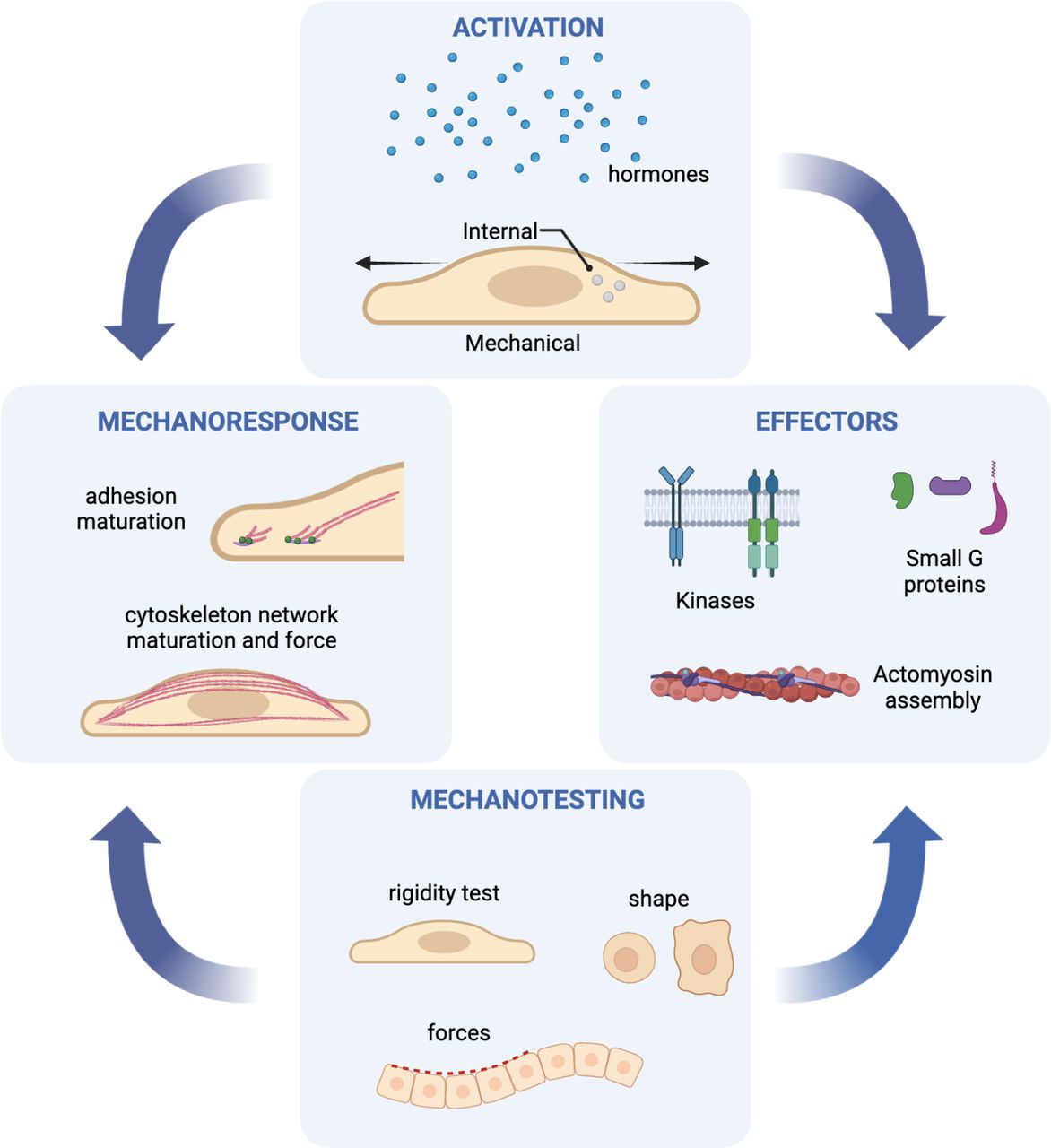
A diagrammatic representation of the primary cycles underlying cell and tissue shaping. In most instances, activation of the motility process is initiated by intrinsic cell signals involving G proteins, kinases, and actomyosins. These structures alter cell morphology or stimulate neighboring cells to allow testing of the mechanical environment, consequently producing cellular responses that maintain cell morphology. Adapted from Wolfenson et al with permission from Annual Reviews. Copyright 2019 Wolfenson, Sheetz, Yang. Published by Annual Reviews.
Challenges in Studying Cell Behavior
Studying cell behavior in vitro presents challenges due to various limitations of the experimental setup. These include the artificial laboratory environment, which may not accurately reflect the in vivo environment, and the lack of cell-to-cell interaction, which can influence signaling pathways and cellular responses. Cells in vitro may lose polarity and shape, particularly when cultured on flat surfaces, affecting their functions and behaviors. Additionally, in vitro experiments are often limited in timescale, making the study of long-term processes such as tissue development challenging.21 Inadequate nutrients and oxygen in vitro can also affect cellular behavior and limit experimental outcomes. In vitro studies may produce models with limited predictive power due to artifacts from reagents, substrates, or experimental conditions that must accurately reflect the in vivo environment, leading to false or misleading results and complicating the interpretation of empirical findings.24
The Relationship Between Mechanobiology and Spinal Fusion
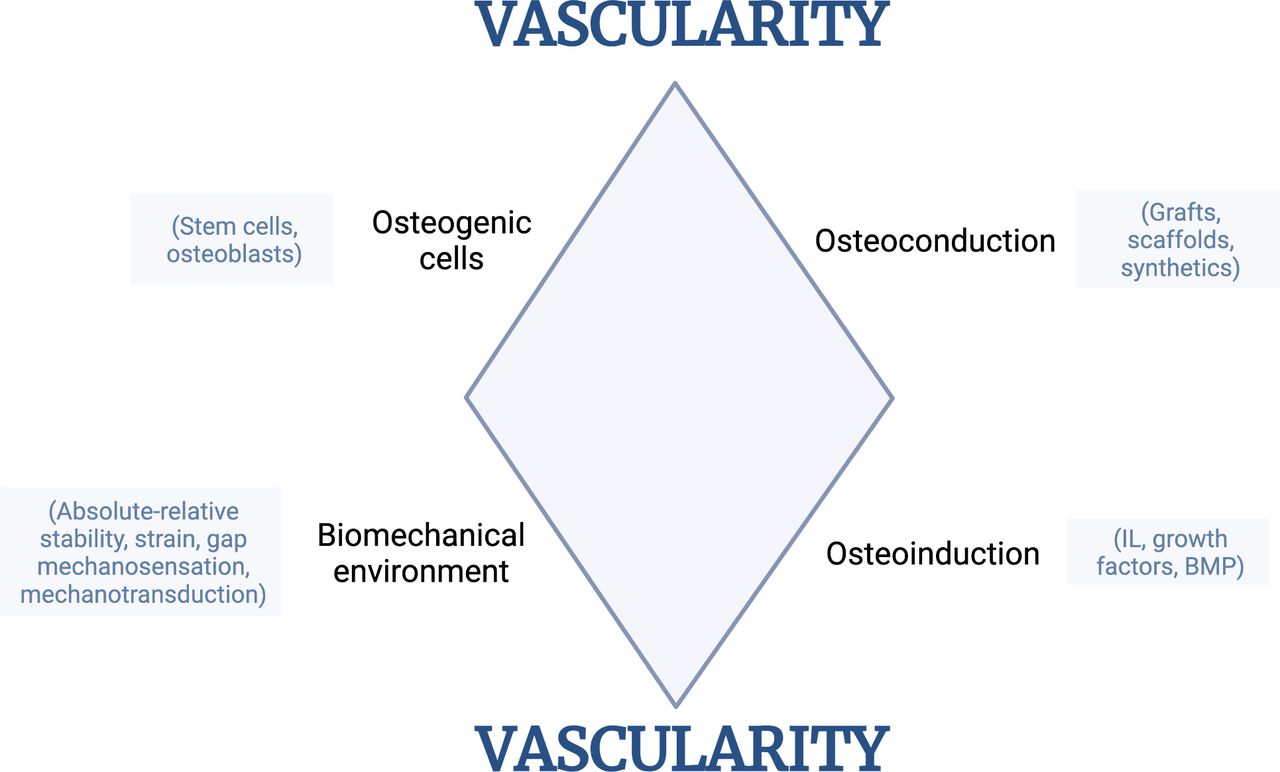
The principles of mechanobiology can help surgeons optimize the mechanical environment to promote bone formation and fusion during spinal fusion surgery. Successful fusion depends on osteoblasts generating new bone tissue at the fusion site, and mechanical loading and stress are critical for successful bone healing and regeneration. An ideal graft material for spinal fusion should meet biological prerequisites, including osteogenic, osteoinductive, and osteoconductive factors and mechanical stability (Figure 5).25 Understanding the complex bone healing process is crucial for spine surgeons to achieve successful fusion.26
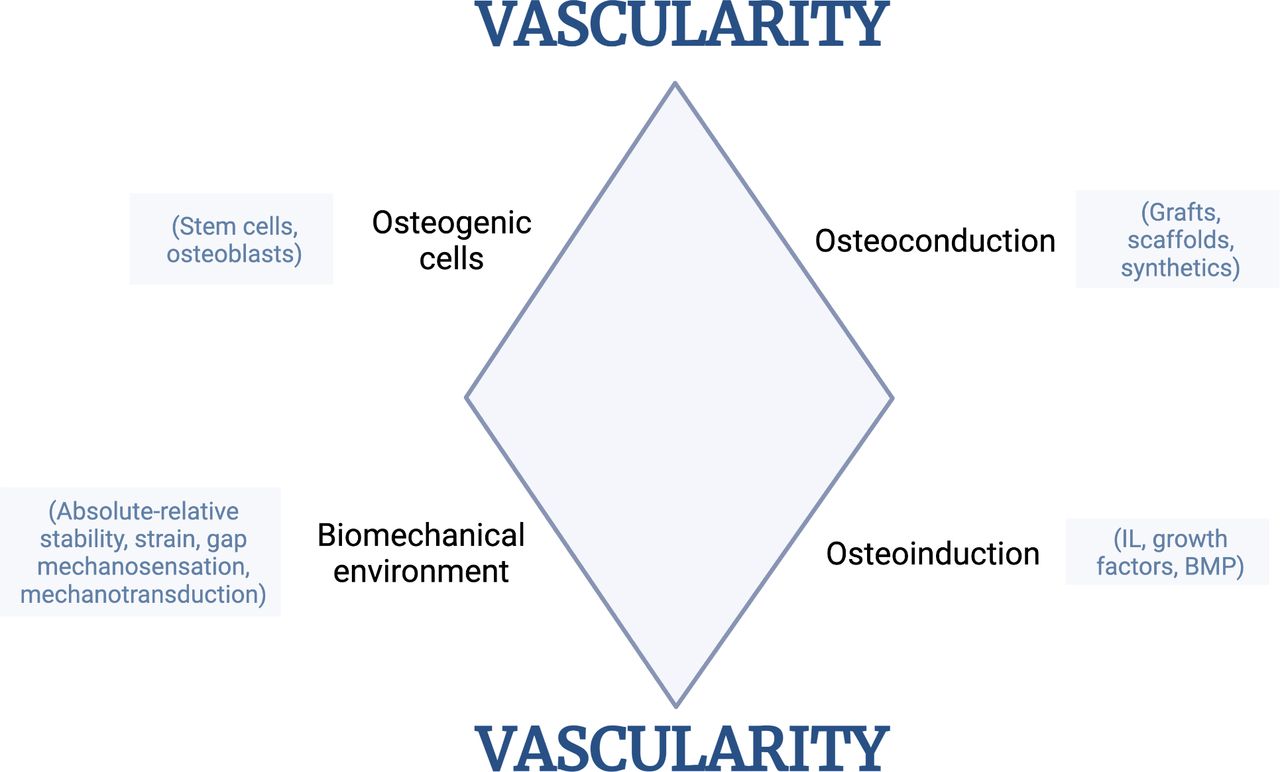
The diamond model of bone healing interaction.25,27
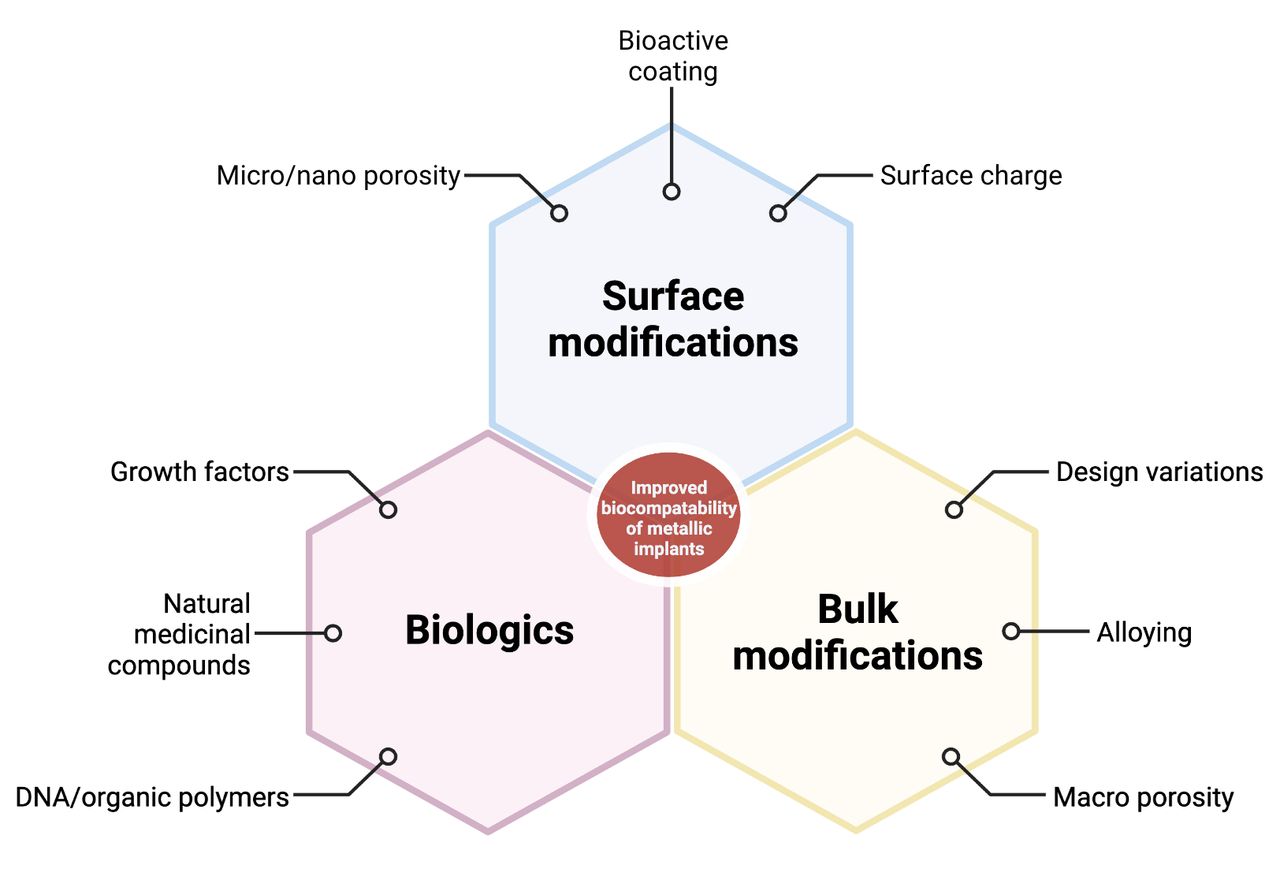
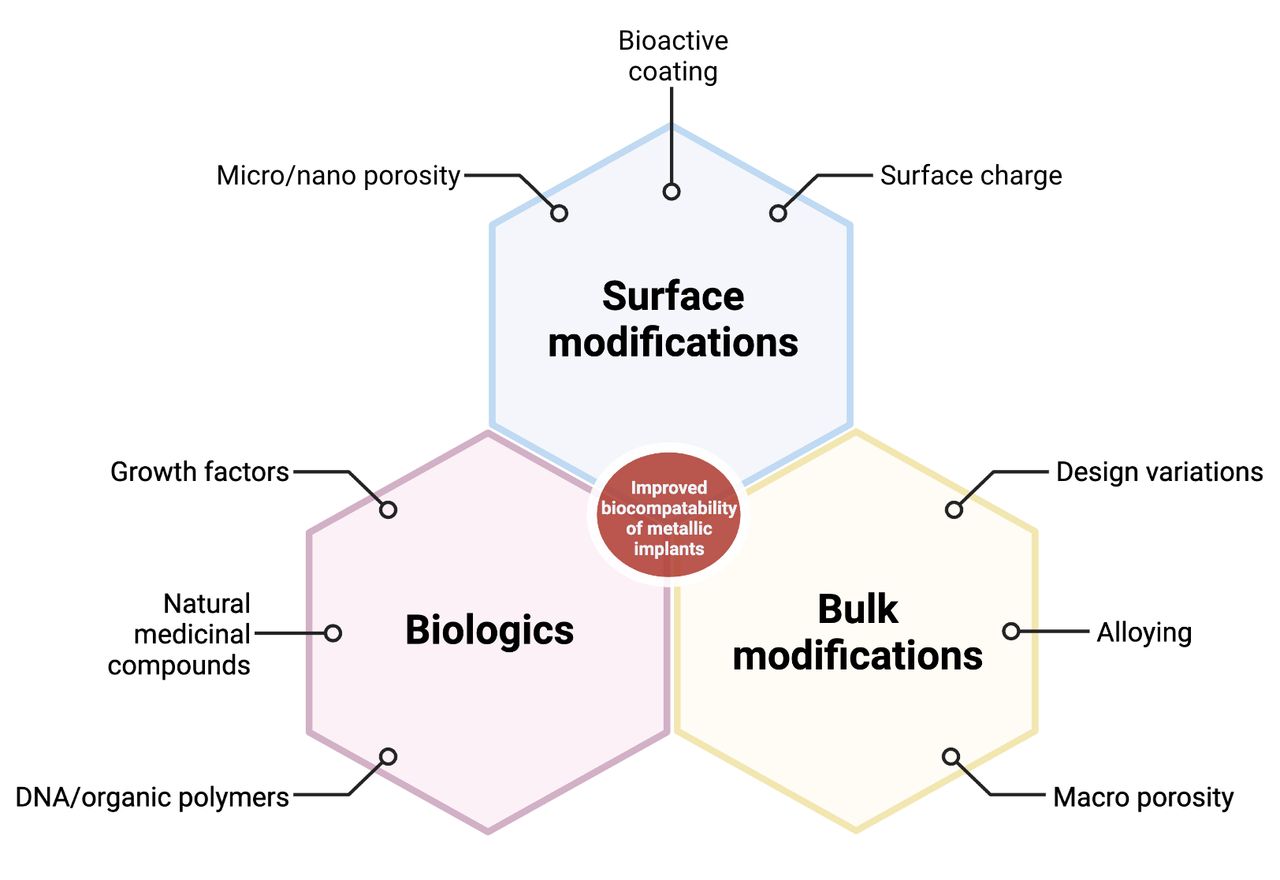
This diagram highlights the role of biologics, bulk modifications, and surface modifications in collectively improving the biocompatibility of metallic implants. Adapted from Bandyopadhyay et al28 with permission from Elsevier. Copyright 2022 Bandyopadhyay, Mitra, Goodman, Kumar, and Bose. Published by Elsevier Ltd.
Discussion
Titanium (Ti), polyetheretherketone (PEEK), and tantalum (Ta) devices are commonly used in interbody fusion cages.29,30 In their unmodified state, these materials have limited bioactivity. To achieve bioactivity, the constituent materials of an orthopedic implant must elicit a specific biological response at the interface of the material, promoting the formation of a bond between the tissues and the implant. Surface treatments modify the interaction between the implant and the body, creating a bioactive layer that promotes osseointegration. This, in turn, results in a powerful implant-bone interface, providing structural, biochemical, and functional stabilities.
Cages can also be modified by utilizing additive and subtractive manufacturing techniques. Additive manufacturing involves building the spinal fusion cages layer by layer using materials like metal or plastic. This can be done using methods like 3D printing or stereolithography. Additive manufacturing allows for complex and customized shapes and designs that are impossible with traditional subtractive manufacturing techniques. Additionally, additive manufacturing can reduce material waste and lead time compared with subtractive manufacturing. On the other hand, subtractive manufacturing involves cutting, drilling, and shaping raw materials like metal or plastic to create the desired shape of spinal fusion cages. This can be done using techniques like milling, turning, or grinding. Although subtractive manufacturing may be less precise and customizable than additive manufacturing, it is still widely used in the medical device industry due to its long-established manufacturing processes and familiarity.
Polyetheretherketone
PEEK is a high-performance thermoplastic polymer used in spinal fusion implants due to its excellent mechanical properties, biocompatibility, radiolucency, and lightweight properties.31–35 The bioinert nature of PEEK restricts its osseointegration. It is hydrophobic in nature, which limits its interaction with biological fluids and tissues.36 This limitation can be overcome through surface modification, structural modification, incorporation of bioactive materials, incorporation of growth factors, and microsurface texturing.
Surface modification techniques, such as plasma treatment, chemical etching, and coating with bioactive materials or metals, can alter the surface properties of PEEK to promote osseointegration.37 Structural modification techniques, such as porous PEEK, fiber-reinforced PEEK, surface roughening, and interconnected channels, can improve osseointegration by altering the material’s internal structure.38 Incorporating bioactive materials and growth factors, such as hydroxyapatite (HA), calcium phosphate, bioactive glass, and bone morphogenetic proteins, can promote the attachment and growth of bone cells and stimulate the formation of new bone tissue.39 Finally, microtexturing techniques, such as laser ablation, microbead blasting, and electrospinning, can create surface features that enhance the attachment and growth of bone cells and promote the formation of new bone tissue.40 Hydrophilic modifications can improve PEEK’s wettability and surface energy, enhancing its interaction with biological fluids and tissues. This can lead to better cell adhesion, proliferation, and differentiation, essential for successful implant integration and long-term stability. Moreover, hydrophilic modifications can promote the formation of a mineralized layer on the surface of PEEK, which improves its osteoconductivity and osseointegration.
Titanium
Medical-grade titanium refers to a specific type of alloy composed of at least 99% titanium and small amounts of other elements, such as 6% aluminum and 4% vanadium. The exact composition of the alloy may vary depending on the specific application.
Titanium cages are commonly used for spinal fusion surgery because of their biocompatibility, strength, radiolucency, corrosion resistance, versatility, stability, and long-term durability.40 However, the structural modification of these cages can enhance their mechanical properties, biocompatibility, or ability to promote bone growth and fusion (Figure 6).
Some common changes include surface roughening, coating, porosity, and geometry modification.41 Surface roughening involves creating a rough surface texture on the cage to promote bone growth and fusion. Coating the cage with materials like HA or bioactive glass can improve its biocompatibility and encourage bone growth. Porosity modification involves creating a porous surface on the cage to promote bone ingrowth and vascularization, which can enhance fusion. The porosity of titanium cages can be modified through several methods, such as plasma spraying, electrochemical etching, laser ablation, sintering, and 3D printing. Geometry modification involves changing the shape, size, or number of the cage’s struts or adding features like spikes or anchors to improve fixation.
These modifications can help promote better bone growth, fusion, and fixation, allowing for customized implants that provide optimal support and stability for the spine. Ultimately, the structural modification of titanium cages can help improve the success of spinal fusion surgery by promoting bone growth and integration with the surrounding tissue.
Tantalum
Porous tantalum has been increasingly used in spine surgery due to its excellent biomechanical and biomaterial properties, including high porosity and anticorrosive surface oxide formation.42 This allows for bony ingrowth and a closer modulus of elasticity to trabecular bone, reducing subsidence and stress shielding.43 Studies comparing stand-alone porous tantalum cages to autograft and plating for anterior cervical discectomy and fusion (ACDF) have reported similar fusion and adjacent segment degeneration rates but lower maintenance of segmental lordosis with tantalum cages.43,44 Different studies have found higher fusion rates for tantalum in lumbar spine fusions, but autograft had higher fusion rates in ACDF.26,43 A retrospective study on single- and two-level cervical corpectomy using porous tantalum cages reported high fusion and low subsidence rates but no significant differences in postoperative cervical lordosis outcomes.45
PEEK vs Titanium
In their meta-analysis, Tan et al46 evaluated 11 articles, including 1 randomized control trial and 2 prospective studies, comparing PEEK and conventional titanium cages for cervical and lumbar fusion. When comparing surgery for noninfective conditions, titanium cages had a higher subsidence rate than PEEK. Regarding fusion rate, overall, they found no difference at 12 months or final follow-up. However, their lumbar fusion subgroup analysis showed higher fusion rates for titanium cages. In their 6-study meta-analysis, Seaman et al47 compared PEEK and titanium cages for ACDF and transforaminal lumbar interbody fusion (TLIF). They reported no differences in fusion rates, albeit with moderate heterogeneity. The subsidence was significantly higher for titanium cages, although their findings had moderate heterogeneity.
ACDF: PEEK vs Titanium
A systematic review by Noordhoek et al48 assessed 71 ACDF studies, reporting a mean subsidence incidence of 21%, with lower rates present in PEEK cages than in titanium cages.
Onyedimma et al49 included 37 studies in their meta-analysis, comparing single- and two-level ACDF using stand-alone PEEK, titanium, and titanium cages. They reported no significant difference in fusion rate between PEEK vs titanium groups.
The meta-analysis by Li et al50 included 4 studies (2 randomized and 2 nonrandomized) comparing PEEK and titanium cages for ACDF. They reported similar fusion rates and postoperative segmental angles but found that titanium cages had a higher subsidence rate (OR = 3.14 and I2 = 8%).
In their retrospective study of 154 patients undergoing single-level ACDF, Cabraja et al51 compared PEEK and titanium cages. They reported similar fusion and subsidence rates and commented that subsidence rates were not affected by cage size or disc height.
In their prospective study of PEEK vs titanium cages for ACDF, Igarashi et al52 found that PEEK cages had significantly less subsidence than titanium cages when the cage height was >5 mm but equivocal subsidence rates for cage heights <5 mm. The impact of cage height on subsidence was also noted by Yamagata et al53 in their stand-alone titanium ACDF cage assessment. They reported a significantly higher risk of subsidence for cage heights of 6.5 to 7.5 mm than for cage heights of 4.5 to 5.5 mm.
Niu et al54 prospectively evaluated 53 patients undergoing single- and two-level ACDF with PEEK and titanium cages. Similar levels of lordosis were achieved in both groups. However, the PEEK group had a significantly higher fusion rate and lower subsidence rate.
Lateral Lumbar Interbody Fusion: PEEK vs Titanium
Amini et al55 retrospectively analyzed patients receiving stand-alone lateral lumbar interbody fusion (LLIF) using PEEK and 3D-printed titanium cages. Fusion assessment with computed tomography (CT) revealed a higher fusion rate at their early timepoint (8.2 months) in the 3D titanium group, but at their late t (18.9 months), there was no significant difference between groups. In a separate publication, the same authors reported that stand-alone lateral interbody fusion with PEEK cages had a significantly higher subsidence rate than titanium (18.5% vs 3.0%).56
Campbell et al57 performed a retrospective analysis of prospective data involving 113 patients under LLIF using PEEK and titanium cages. Following Marchi’s criteria, they assessed subsidence on postoperative x-rays.58 They found that the PEEK group had significantly higher subsidence rates at 2, 3, and 12 months postoperatively. A multivariate analysis identified age as a correlating risk factor for subsidence.
PLIF/TLIF: PEEK vs Titanium
Khan et al59 performed a retrospective registry matched-cohort study on 228 TLIF patients receiving PEEK or 3D-printed titanium cages. They reported significantly lower fusion rates and subsidence levels for PEEK cages than 3D-printed titanium (73% vs 90% and 40% vs 23.5%, respectively).
Massaad et al34 performed a meta-analysis of 11 posterior lumbar interbody fusion (PLIF) studies comparing PEEK and titanium. They reported no difference in subsidence rates but noted a lower fusion rate in the PEEK group. However, a major confounding issue with this study is that their titanium group included both conventional and titanium-coated cages.
In their retrospective cohort of 137 patients undergoing single-level TLIF, Canesco et al60 compared PEEK and titanium cages. They reported no significant difference between subsidence rate, fusion rate, or lordosis correction between the 2 groups at 12 months.
Cage Coating/Surface Modifications
Direct PEEK Surface Modifications
Surface modifications to PEEK can be made directly without creating additional layers. Methods include wet chemical treatment, plasma, laser, ultraviolet, ozone, and accelerated atom beam surface treatments.61–65
Titanium Coating
Titanium coating aims to increase the bone-implant contact area, surface roughness, and osseointegration potential of biomaterials such as PEEK.66,67 The development of titanium-coated PEEK (TiPEEK) cages has continued to increase.68,69
Different methods are available to achieve titanium coating on PEEK without damaging the material. Low-temperature vacuum-plasma spraying can achieve roughened titanium coatings between 6 and 12 microns.35,70 An alternative technique involves titanium oxide coating through arc-ion plating. An electron beam evaporator can achieve low-temperature deposition of a thin uniform titanium layer.71
In certain instances, however, adding surface modifications can lead to the formation of particle debris. Kienle et al72 demonstrated that shear loading forces imparted during TiPEEK implant impaction could result in partial delamination of titanium coatings. The particles produced ranged in size from 1 to 191 µm, with around half of the particles being nonphagocytosed because of the size (>5–10 µm), thus raising concerns for causing potential inflammatory and osteolytic reactions. Similarly, Torstrick et al73 compared TiPEEK with smooth and porous PEEK and found that impaction caused a significant loss of titanium coating.
HA Coating
HA (Ca10[PO4]6[OH]2) is a bioactive ceramic that is present in natural bone minerals. It has a long track record for use in orthopedic and dental implants, including evaluating optimal coating strategies.74–78
Compared with titanium-coated implants, some authors have reported better fusion rates and radiological outcomes when using HA-coated implants.79
Chin et al80 retrospectively assessed single-level ACDF patients receiving PEEK vs HA-PEEK cages. They reported a trend toward earlier fusion at 3 to 5 months in the HA-PEEK on x-ray evaluation, although they did not comment on the statistical significance or final fusion rate.
PEEK vs Titanium-Coated PEEK
Godlewski et al81 assessed 104 randomized patients receiving PEEK and TiPEEK for single- and multilevel ACDF. They found an overall subsidence rate of 21%, without significant differences between the groups. However, they reported that subsidence was associated with low implant-to-bone ratios.
In their prospective randomized study, Hasegawa et al82 compared PEEK and TiPEEK in single-level open TLIF and PLIF. They assessed fusion according to the modified Bridwell classification, using serial CT assessments up to 12 months postoperatively. They reported earlier fusion for TiPEEK at 6 months, although at 12 months there was no significant difference in fusion rates between PEEK and TiPEEK. Subsidence rates between groups were not significantly different.
Schnake et al83 performed a prospective randomized study comparing PEEK to TiPEEK in single- and two-level PLIF. Fusion was assessed with x-ray and CT at 6 and 12 months, using fusion criteria defined by McAfee30 and Abbushi et al.84 They reported no significant difference between groups for fusion rate through or around the PLIF cages.
Similarly, in their cohort of PLIF patients, Sakaura et al85,86 reported that TiPEEK and PEEK cages demonstrated no difference in fusion rates when assessed using x-ray and CT.
The randomized pilot study by Rickertt et al87 evaluated PEEK TLIF cages with and without titanium coating for single- and two-level fusions. They reported a fusion rate of 91.7%, with no difference in total or partial fusion rates between the 2 groups.
Singhatanadgige et al88 compared PEEK with TiPEEK for single- and two-level minimally invasive surgery-TLIF in their prospective randomized study of 82 patients. They reported a significantly higher fusion rate in the TiPEEK group on initial 6-month CT. However, on the 12-month CT, there was no significant difference in fusion rate between groups.
Kashii et al89 prospectively evaluated PEEK vs TiPEEK in 26 patients undergoing single-level PLIF. Their novel design saw each fusion level PLIF pairing receive 1 PEEK and 1 TiPEEK cage. On postoperative x-rays and CT, they assessed fusion rate, subsidence, and “vertebral cancellous condensation.” They reported an 88% fusion rate on CT at 3 months, with persistent angular instability on dynamic x-rays at 12 months. The authors noted that TiPEEK had significantly higher rates of vertebral cancellous condensation than uncoated PEEK, suggesting the presence of bone on-growth.
Titanium vs Surface-Modified PEEK
In their meta-analysis, Massaad et al34 reported similar subsidence rates for TiPEEK cages vs titanium for PLIF. Still, they noted that fusion odds for TiPEEK cages were 0.62 times those of titanium cages.
Makino et al90 studied 59 patients undergoing single- and two-level PLIF using TiPEEK and 3D-printed titanium. Using CT color mapping, they evaluated the amount of bone on-growth, following Walsh’s method.67 The presence of bone on-growth for TiPEEK and 3D-printed titanium increased from 6 (58.0% and 69.0%, respectively) to 12 months (63.5% and 75.0%, respectively). During that time, the grading of bone on-growth progressed in 3D-printed cages at both union and nonunion segments, as opposed to only in the union segments for TiPEEK. The same authors91 later reported similar fusion and lordosis alignment between groups in a 63-patient cohort, although overall fusion rates at 12 months were notably low (75% TiPEEK and 83.3% 3D-printed titanium). They also noted that the 3D-printed titanium group had a significantly lower subsidence rate and vertebral endplate cyst sign formation.91
Conclusion
Mechanobiology is a field that focuses on understanding how mechanical forces impact biological processes at the cellular and molecular levels. In the context of spinal fusion, the design and modification of implants play a crucial role in achieving successful outcomes. The principles of mechanobiology are fundamental in spinal fusion because the mechanical forces and stresses applied to implants can affect the surrounding bone tissue. In contrast, the mechanical properties of the implant itself can influence bone growth and fusion. Therefore, it is essential to optimize the mechanical properties of the implants and modify their surfaces to promote a conducive environment for bone growth and fusion while also ensuring that the implants can withstand patient-generated mechanical forces.
This field focuses on improving patient outcomes by understanding the interactions between mechanical forces and biological processes in spinal fusion. Engineers and surgeons are collaborating to develop implant designs that better mimic the natural mechanical environment of the spine, considering factors such as load distribution, stress transfer, and bone remodeling. By incorporating principles from mechanobiology into implant design, researchers aim to enhance bone healing and fusion rates, reduce complications, and improve the long-term stability and functionality of spinal fusion procedures.
Several trends can be observed in the current research. One trend is the use of advanced materials and fabrication techniques to optimize the mechanical properties of implants. For example, developing bioactive materials and surface modifications that promote bone growth and integration has shown promising results. Additionally, researchers are exploring using biodegradable materials that can gradually transfer the load to the surrounding bone, allowing for better integration and minimizing stress shielding.
Another trend is using computational modeling and simulation techniques to understand better implants’ mechanical behavior and their interaction with the surrounding tissues. These models can provide valuable insights into the effects of different implant designs and loading conditions, allowing for virtual testing and optimization before clinical implementation. By combining computational modeling with experimental studies, researchers gain a more comprehensive understanding of the complex biomechanical factors involved in spinal fusion.
Overall, the current body of work in mechanobiology and spinal fusion highlights the importance of considering mechanical forces in implant design and modification. By leveraging principles from mechanobiology, engineers and surgeons are making strides in optimizing implant mechanical properties and surface characteristics to improve patient outcomes. Integrating advanced materials, computational modeling, and interdisciplinary collaborations between engineers and clinicians contribute to the advancements in this field. Nonetheless, it is essential to note that further research is still needed to fully elucidate the complex interactions between mechanical forces and biological processes in spinal fusion and effectively translate these findings into clinical practice.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declarations This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors have no conflicts of interest to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.