


Abstract
Background Biologic-reactivity to implant-debris is the primary determinant of long-term clinical performance. The following reviews: 1) the physical aspects of spinal-implant debris and 2) the local and systemic biologic responses to implant debris.
Methods Methods included are: 1) gravimetric wear analysis; 2) SEM and LALLS; 3) metal-ion analysis; 4) ELISA, toxicity testing, patch testing; and 5) metal-lymphocyte transformation testing (metal-LTT).
Results Wear and corrosion of spine-implants produce particles and ions. Particles (0.01–1000 μm) are generally submicron ( <1 µm). Wear rates of metal-on-polymer and metal-on-metal disc arthroplasties are approximately 2–20 and 1 mm3/yr, respectively. Metal-on-metal total disc replacement components have significant increases in circulating metal (less than 10-fold that of controls at 4 ppb-Co and 3 ppb-Cr or ng/mL). Debris reactivity is local and systemic. Local inflammation is caused primarily by ingestion of debris by local macrophages, which produce pro-inflammatory cytokines TNFα, IL-1β, IL-6, and PGE2. Systemic responses associated with implant-debris have been limited to hypersensitivity reactions. Elevated amounts of in the liver, spleen, etc of patients with failed TJA have not been associated with remote toxicological or carcinogenic pathology to date. Implant debris are differentially bioreactive. Greater numbers are pro-inflammatory; the smaller-sized debris are more bioreactive by virtue of their greater numbers (dose) for a given amount of implant mass loss (one 100-μm-diameter particle is equivalent in mass to 1 million 1-μm-diameter particles). Elongated particles are pro-inflammatory (ie, aspect ratio of greater than 3). Metal particles are more proinflammatory than polymers, ceteris paribus.
Conclusion Spinal arthroplasty designs have been in use for more than 20 years internationally; therefore, concerns about neuropathology, toxicity, and carcinogenicity are mitigated. Debris-induced inflammation still depends on the individual and the type of debris. The consequence of debris-induced inflammation is continued; vigilance by physicians is recommended monitoring of spinal implants using physical exams and testing of metal content and bioreactivity, as is planning for the likelihood of revision in younger individuals.
- Implant debris
- Inflammation
- Total disc arthroplasty
- Osteolysis
- Hypersensitivity
- Metal debris
- Particulate
- Implant
- Spine
- Cytokines
- Inflammasome
- Wear
- Wear debris
Bioreactivity (pro-inflammatory reactivity) to orthopedic implants debris is generally the main determinant of clinical performance of established total joint arthroplasties (TJA).1 Aseptic osteolysis has been reported as high as more than 75% of TJA of all implant failures and is the central factor limiting the longevity of current total joint arthroplasties; other reasons for failure include infection (7% of failures), recurrent dislocation (6% of failures), periprosthetic fracture (5% of failures), and surgical error (3% of failures).2 Debris-induced aseptic failure has been reported to be as high as 5% at 7 years postop in current generation metal-on-metal total hip arthroplasties.3–5 Wear and corrosion products that are attributed with these local inflammatory responses leading to aseptic failure.6–10 In fact, a 15% revision rate at 20 years has been singularly correlated/ predicted by a wear rate of greater than 0.1 mm per year of older model UHMWPE acetabular liners (nonhighly crosslinked).11 To date, wear remains the strongest correlate of aseptic osteolysis and implant loosening. Understanding what the difference is between popular misconceptions and what is known of spinal implant debris is key for physicians to understand the risks associated with modern spine arthroplasty implants. The following review addresses 2 questions: 1) What kinds of spinal implant debris are produced and 2), clinically, what exactly is implant debris reactivity locally and systemically? Unfortunately, the amount of data from total disc arthroplasty studies is limited. Thus extrapolation from hip and knee arthroplasty experience to the spine is still necessary.
Methods
Methods included in this review are those associated with physical characterization of implant debris and those associated with measuring the biologic responses to implant debris: 1) gravimetric wear analysis; 2) particle characterization by scanning electron microscopy (SEM) and low-angle laser light scattering (LALLS); 3) metal ion analysis; 4) enzyme linked immunoassay (ELISA); and 5) lymphocyte transformation testing (LTT).
Wear
Gravimetric wear is measured by the weight loss of the individual component after simulator or in vivo use. The accuracy of this testing is typically on the order of 0.02 mg. Wear involves the loss of material (weight or mass) as a consequence of relative motion between 2 surfaces. The amount of wear depends on predictable factors: the amount of force pressing the 2 materials together; ie, the contact force, amount of relative sliding distance, type of bearing materials, and the type and amount of lubrication.
Particle characterization
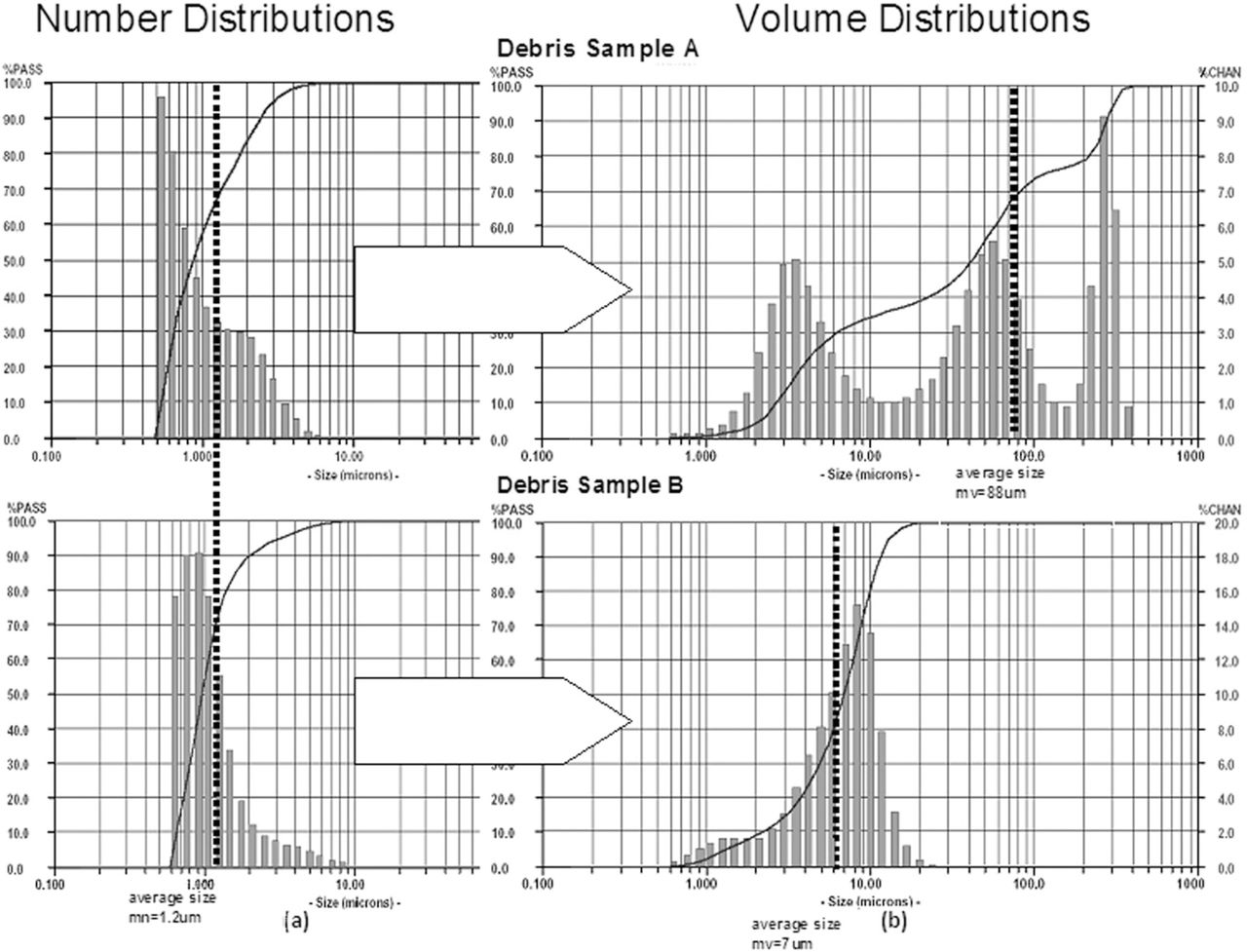
Traditional particle sizing techniques, such as SEM or transmission electron microscopy (TEM) (number-based counting methods), indicated that the majority of the wear (mass loss) from an implant is comprised of particles in the nanometer to submicron range. This understanding stems largely from the relatively low numbers of particles (hundreds to thousands) used in traditional number-based analysis techniques such as SEM. Newer analytical techniques, such as LALLS which samples millions to billions of particles, catch the one-in-a-million large particle that comprises a significant portion of the total mass loss (total debris). This contribution of large particles to the total debris mass, but insignificant contribution to the total number of particles, is made apparent in graphical representation of number and volume particle size distributions (Figure 1). The counting of millions to billions of particles facilitates not only a number-based analysis, but because the one-ina-million larger particle is also counted a volume-based analysis is also facilitated.

These analyses of (a) volume and (b) number distributions of two debris samples demonstrate how similar number distributions can result from very different actual size distributions as evident in (a) the volume distributions. Note: The x-axis represents increasing particle diameter and the y-axis is (a) percentage of total number of particles in each size range and (b) the percentage of total mass of each sample that is of that size range. (Courtesy of BioEngineering Solutions Inc.)
The ability to accurately, and as comprehensively as possible, characterize implant debris is critically important to the new generation of bearing surfaces used in novel spinal implants where weight loss from the implant after a year of use (eg, less than 0.2-mm3 volume loss after a million cycles of use) could be attributed to the loss of a relatively few large particles or hundreds of millions of small particles (200 particles of 100-μm diameter are equivalent in mass to 200 million particles only 1 μm in diameter). This phenomenon is illustrated in Fig. 1, where different samples of particles look demonstrably very different when viewed as a volume-based distribution, though they look very similar when analyzed using a number-based distribution. This shows how important it can be to have number- and volume-based distributions of the same particles to characterize fully the types of particles in the mix.
Biologic assays
Cell culture. Growth medium for the human cell lines such as macrophage THP-1 (ATCC) is typically RPMI 1640 supplemented with L-Glutamine, Penicillin, Streptomycin, 25 mM Hepes (Lonza, Walkersville, MD) and 10% heat inactivated fetal bovine serum (FBS; Hyclone Laboratories, Logan, UT). Implant debris that are usually produced using implant components in a cryo-milling or cryo-pulverization techniques (Bioengineering Solutions Inc, Chicago, IL) were generated from metal orthopedic implant components (Cobalt alloy, ASTM F-75). Collected metal particles are characterized for size and number by laser diffraction technology and have a mean diameter of less than 10 μm, usually approximately 1–2 μm (number-based analysis) with a size range of 1–10 μm.
Isolation of different cell types for study of human peripheral blood monocytes and CD4 + T cells. Peripheral blood mononuclear cells (PBMCs) are typically isolated from heparanized whole blood from healthy donors by Ficol-Hypaque density gradient separation and collected for further cell isolation. Peripheral blood CD14+ monocytes are isolated from collected PBMCs by negative selection with a magnetic bead antibody cocktail specific for CD3, CD7, CD16, CD19, CD56, CD123, and Glycophorin A (Miltenyi Biotec). All isolated cell populations are typically assessed for purity by flow cytometry analysis.
ELISA/Luminex assays. Cytokines and chemokines secretion by cells, such as THP-1 monocytes, human primary macrophages, and CD4+ T cells, are analyzed with ELISA or Luminex suspension multiplex array technology. Supernatants from both metal-challenged monocytes and co-culture experiments are collected after 30 minutes to 5 days and stored at −80°C. Monocyte-macrophage supernatants are typically analyzed for IL-6, IL-1β, TNFα, GMCSF, PGE2, and IL-8 with pro-inflammatory multi-plex cytokine array kits (millipore).
Testing for metal sensitivity. Testing for metal sensitivity has historically been conducted in vivo by skin testing (ie, so-called patch testing or intradermal testing) and in vitro by lymphocyte transformation testing (LTT). While general patch testing protocols and commercial kits do exist for a variety of commonly antigenic substances12, 13 (eg, TrueTest, Glaxo Dermatology, Research Triangle Park, NC), there is continuing concern about the applicability of skin testing to the study of immune responses to implants regarding the questionable equivalence of dermal Langerhans cells to peri-implant antigen presenting cells14, 15 and/or the possible induction of hypersensitivity in a previously nonsensitive patient.16
Metal-LTT testing is lymphocyte proliferation testing (also known as lymphocyte transformation testing, hence LTT), and involves measuring the proliferative response of lymphocytes obtained from peripheral blood by routine blood draw (eg, Orthopedic Analysis Inc, Chicago, IL). Metal-LTT assays are typically performed using 96-well cell-culture plates (Sigma) at a density of approximately 0.2 × 106 cells/well for 6 days in 150 µl/ well of complete media (DMEM 10% FBS) at 37°C and 0.5% CO2, with or without metal treatments. Radiolabeled thymidine (1 mCi/well) is added during the last 12 hours of the 6-day culture period, where it is incorporated into dividing cells. Cell proliferation is normalized to that of cells treated with media alone (controls) producing a ratio, referred to as the proliferation index or stimulation index (SI). The formula is SI = (mean cpm cells + treatment) / (mean cpm cells + medium alone). All tests should be conducted in triplicate to facilitate an average and standard deviation.
Results
The following results are broken into 2 main sections: a review of the physical aspects of spinal implant debris production and local and systemic biologic responses to implant debris.
Physical aspects of spinal implant debris production
The fiction is that there are many different kinds of implant degradation processes. The fact is that there are only 2. Immediately upon implantation all implants begin to degrade through 2 mechanisms, wear and corrosion. Wear is a mechanical/physical degradation of materials (abrasive, adhesive, etc), whereas corrosion is a chemical (electrochemical) form of degradation. Of these 2 degradation mechanisms, wear is the primary source of articulating implant debris.
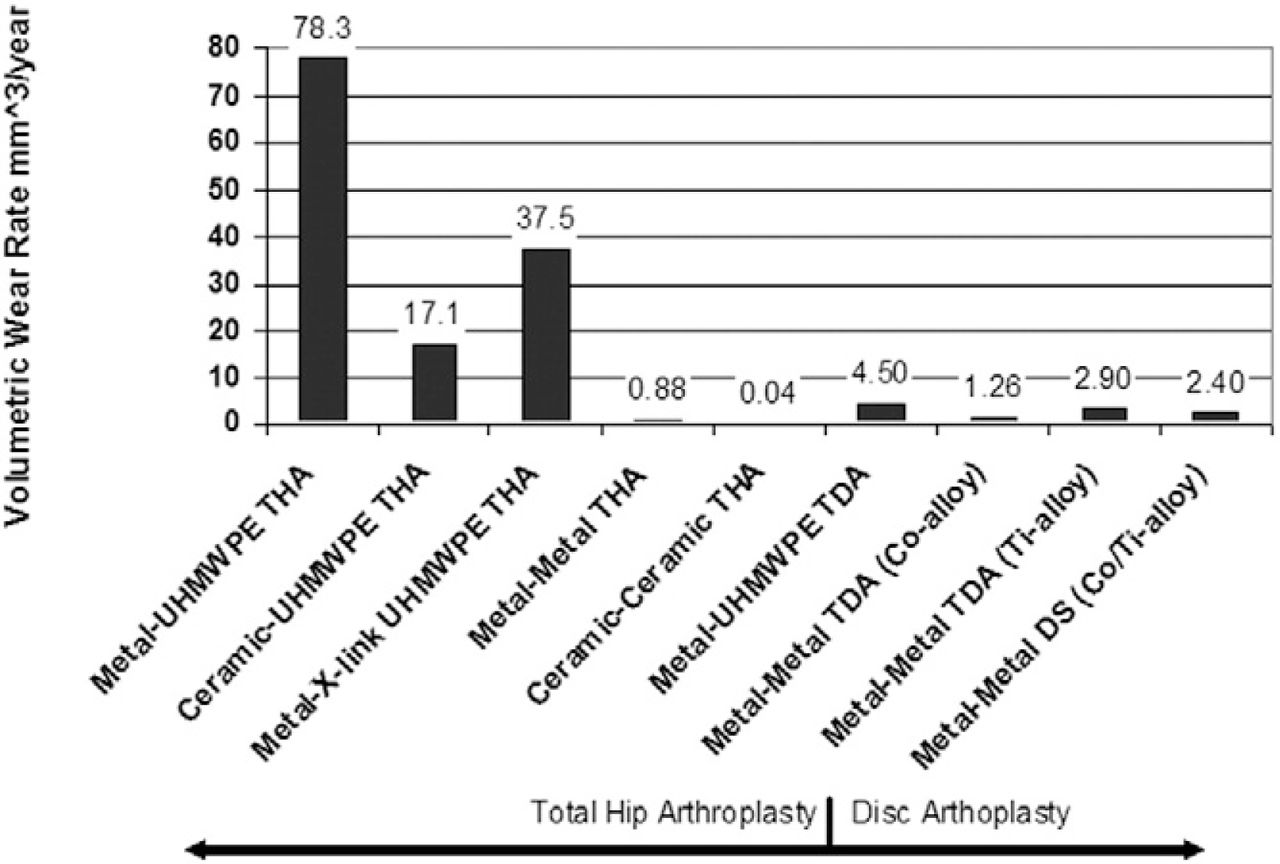
Wear. The fiction is that wear-resistant newer materials, like highly cross-linked polyethylene and ceramic, do not wear and release debris. The fact is that all bearing surfaces wear to some degree. Different types of orthopedic materials and couples produce different amounts and kinds of wear debris. Hard-on-hard material couples, such as metal-on-metal articulations, generally produce less wear (weight loss) than metal-on-polymer (Fig. 2). These 2 basic types of articulating bearing designs are available in spine, knee, and hip arthroplasties.

A graphical comparison of data showing the amount of wear debris generated from different types of total joint arthplasties demonstrating that there is relatively less (10×) polymeric debris generated by a total disc arthroplasty with a metal-on-polymer articulation. However, this difference is not apparent with metal-on-metal articulating implants. Note: Figure References: Metal-Poly:24Ceramic-Poly:25, Metal-X-linked Poly: 22 Metal-X-linked Poly: 26, Metal-X-linked Poly: 27, Metal-X-linked Poly: 28, Metal-Metal: 29, Ceramic-Ceramic: 30, Metal-UHMWPE TDA: 17, Metal-Metal TDA: 18.
Metal-on-polymer spine arthroplasty wear. In vitro analysis of wear has demonstrated wear rates of metal-on-polymer bearing lumbar total disc arthroplasty devices range from 2 to 20.8 mm3/million cycles,17, 18 where the size of the wear debris generally ranges from 0.1 to 100 μm in diameter UHMWPE.17, 19–21 This amount of debris is 10-fold less wear than THAs and TKAs that are composed of metal on highly-crosslinked polyethylene (x-UHMWPE) bearing surfaces.22, 23
Metal-on-metal spinal arthroplasty wear. In general, the wear of metal-on-metal TJA is well below that of metal-on-polymer (Fig. 2).22, 24–30 The few published reports on the wear rates of metal-on-metal disc arthroplasty prostheses indicate a wear rate of 0.93–1.26 mm3/million cycles (Cobalt-alloy).18, 31 Another study of an all titanium-6% Al-4%V alloy disc arthroplasty found wear rates to be as high as 3 mm3/million cycles.32 These values are similar to those reported for metal-on-metal hip replacements, which have been shown to range from approximately 0.05– 6 mm3/ million cycles (Cobalt-alloy).29, 33, 34 Long-term follow-up of patients undergoing total disc arthroplasty is required to assess how intimately wear will correlate with inflammation and poor implant performance.
Corrosion. The fiction is that some metals do not corrode in vivo. The fact is that all metals corrode in vivo. Corrosion can be defined as an electrochemical attack of a metal by its environment. Implant corrosion reduces structural integrity and causes the release of by-products that interact locally and systemically. Orthopedic alloys rely on the formation of passive films on their surface for corrosion protection. Some alloys are better than others at resisting this chemical degradation; for instance, stainless steel alloys generally corrode to a greater extent than either cobalt or titanium alloys.35–37 Special types of corrosion, such as fretting, can take place, where a combination of chemical degradation is enhanced by mechanical factors such as a crevice and abrasive wear, as is common in the screw-plate junction of spine implants. In modern practice, gross evidence of corrosion in screw-plate interfaces is less common.38 Corrosion products are typically oxides (Cr2O3, CoO, TiO2, Al2O3, etc), metal phosphates, metal salts, metal-ions bound to proteins, or organometallic complexes.39–43
Implant debris types: particles and ions. The degradation products of all orthopedic implants are 1 of 2 basic types of debris: particles or soluble debris (metal ions). While there is typically a large distinction between the 2, this distinction becomes a gray area as the size of particles decreases into the nanometer range. Typically, particulate wear debris (metal, ceramic or polymer) exist from the submicron size up to thousands of microns (mm), while so-called “soluble debris” are limited to metal ions that are bound to plasma proteins.
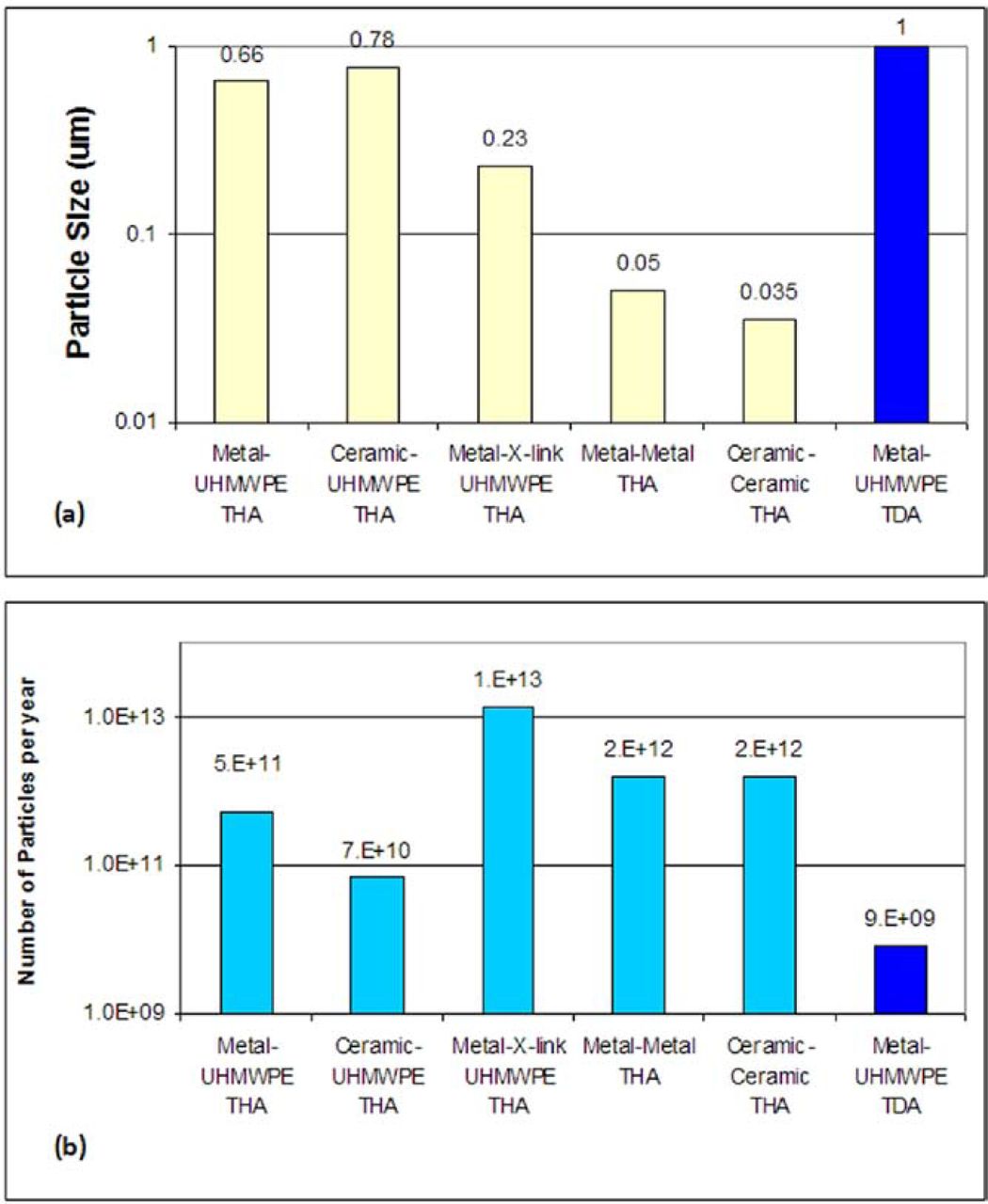
Particulate debris. The fiction is that all implant debris are approximately 1 µm in size. The fact is that the easiest (most numerous) debris to measure is typically less than 1 µm in size. But all implant debris cover a range of sizes from nanometers to tenths of a millimeter (0.01 to hundreds of µm in diameter). Currently, there is a lack of comprehensive information regarding the debris retrieved from spinal implants. However, we do know that particles generated in simulator studies of articulating spinal implants match the sizes and types of particles produced from hip and knee arthroplasty (Fig. 3).22, 24–30 Generally, hard-on-hard material couples, such as metal-on-metal articulations, generally produce smaller-sized (nanometer and sub-micron), fairly round debris, whereas traditional metal-on-polymer bearings produce larger (micron-sized) debris that are more elongated in shape (Figs. 2 and 3). The particles produced from articulating bearing in any metal-on-polymer bearing implants are dominated by polymer particles with little metallic debris, unless there are other sources of metal release such as corrosion at metal-metal connections. Polymeric particles produced from implants generally fall into the range from 0.23–1 µm (Fig. 3A). Past investigations, primarily of UHMWPE wear debris in peri-implant tissues, have shown that 70–90% of recovered particulates were submicron, with the mean size being approximately 0.2–1 µm.43–45 Newer polymer implant debris from highly crosslinked polymers have demonstrated the production of smaller, more rounded debris in the submicron range as small as 0.1 µm in size.29;46 Metal and ceramic particles have generally been characterized as an order of magnitude smaller than polymer particles (at approximately 0.05 µm in diameter, in the nanometer range). Given the relative wear rates in Fig. 2 and the average particle sizes in Fig. 3A, this translates to a theoretical increase in the yearly production of metal-on-metal particles of 1-3 orders of magnitude over that produced by metal-on-polymer articulating surfaces, even though the amount of mass loss is over an order of magnitude less for metal-on-metal bearings (Fig. 3B). Different types and sizes of particles have been found histologically in peri-implant tissues.19, 35, 47–51 Stainless steel: At steel screw-plate junctions, which contain particles of chromium compound ranging in size from 0.5 to 5.0 µm, stainless steel has been found in the peri-implant tissues as closely packed, plate-like particle aggregates.52 Cobalt alloy: Cobalt alloy corrosion produces a chromium-phosphate (Cr(PO4)4H2O) hydrate rich material termed “orthophosphate”, which ranges in size from sub-micron to aggregates of particles up to 500 µm.52, 53 Titanium alloy: The degradation products observed in histologic sections of tissues adjacent to titanium base alloys generally have the same elemental composition as the parent alloy (which often is detected as titanium oxide, the thick oxide layer that forms on all titanium implants and protects the bulk alloy), as opposed to precipitated corrosion products which occur with stainless steel and cobalt-chromium alloys (Fig. 4).
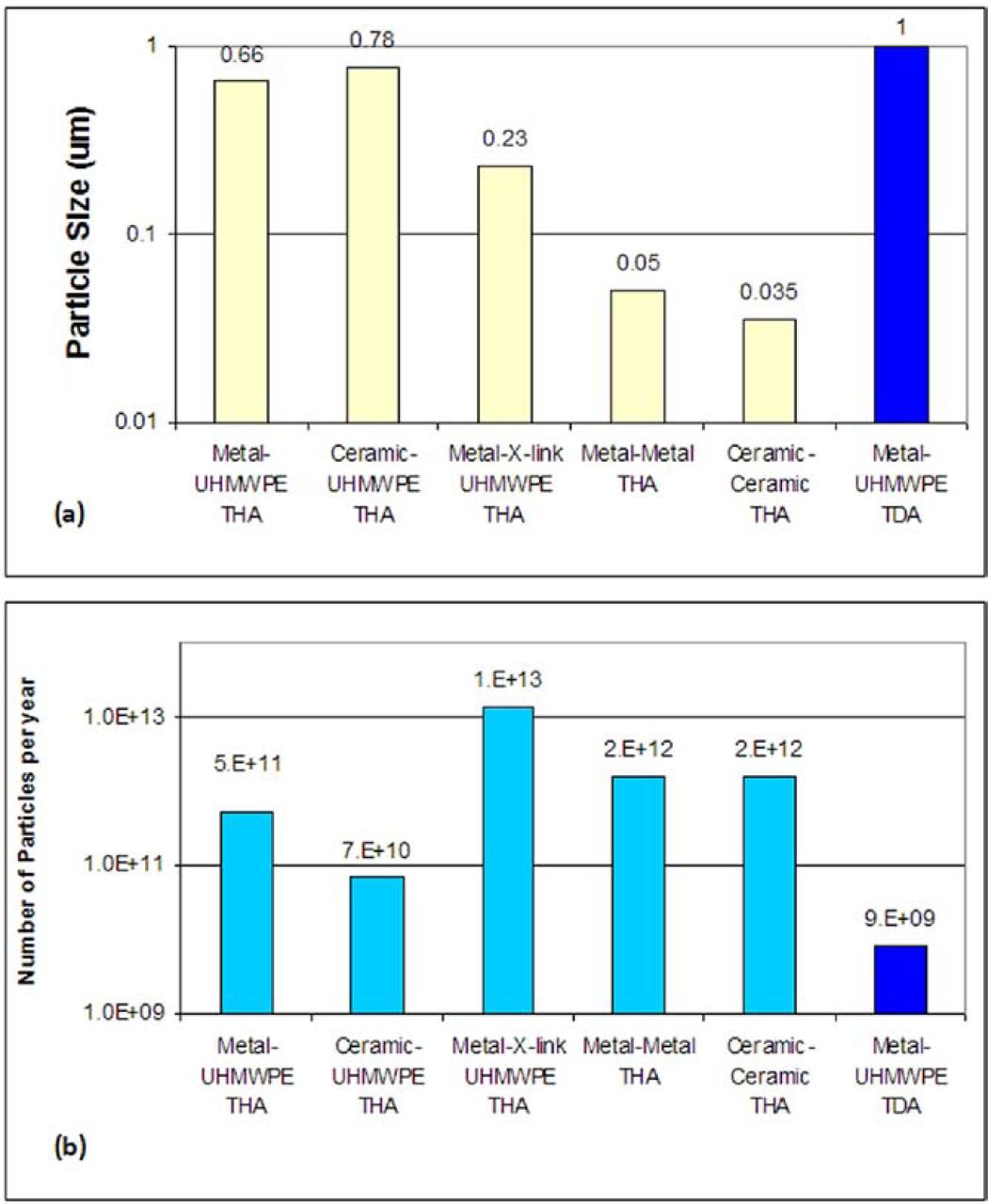
A graphical comparison of data showing (a) the reported size of implant debris generated from different types of total joint arthplasties and (b) the amount of particles per year this results in using the gravimetric data shown in Fig. 1. The smaller size of the particles reported in highly crosslinked polymer particles (copared to traditional poly) combined with the modest reductions in wear rate results in metal on Metal-X-linked Poly. Note: Fig. References: Metal-Poly:24Ceramic-Poly:25, Metal-X-linked Poly: 22 Metal-X-linked Poly: 26, Metal-X-linked Poly: 27, Metal-X-linked Poly: 28, Metal-Metal: 29, Ceramic-Ceramic: 30, Metal-UHMWPE TDA: 17, Metal-Metal TDA: 18.
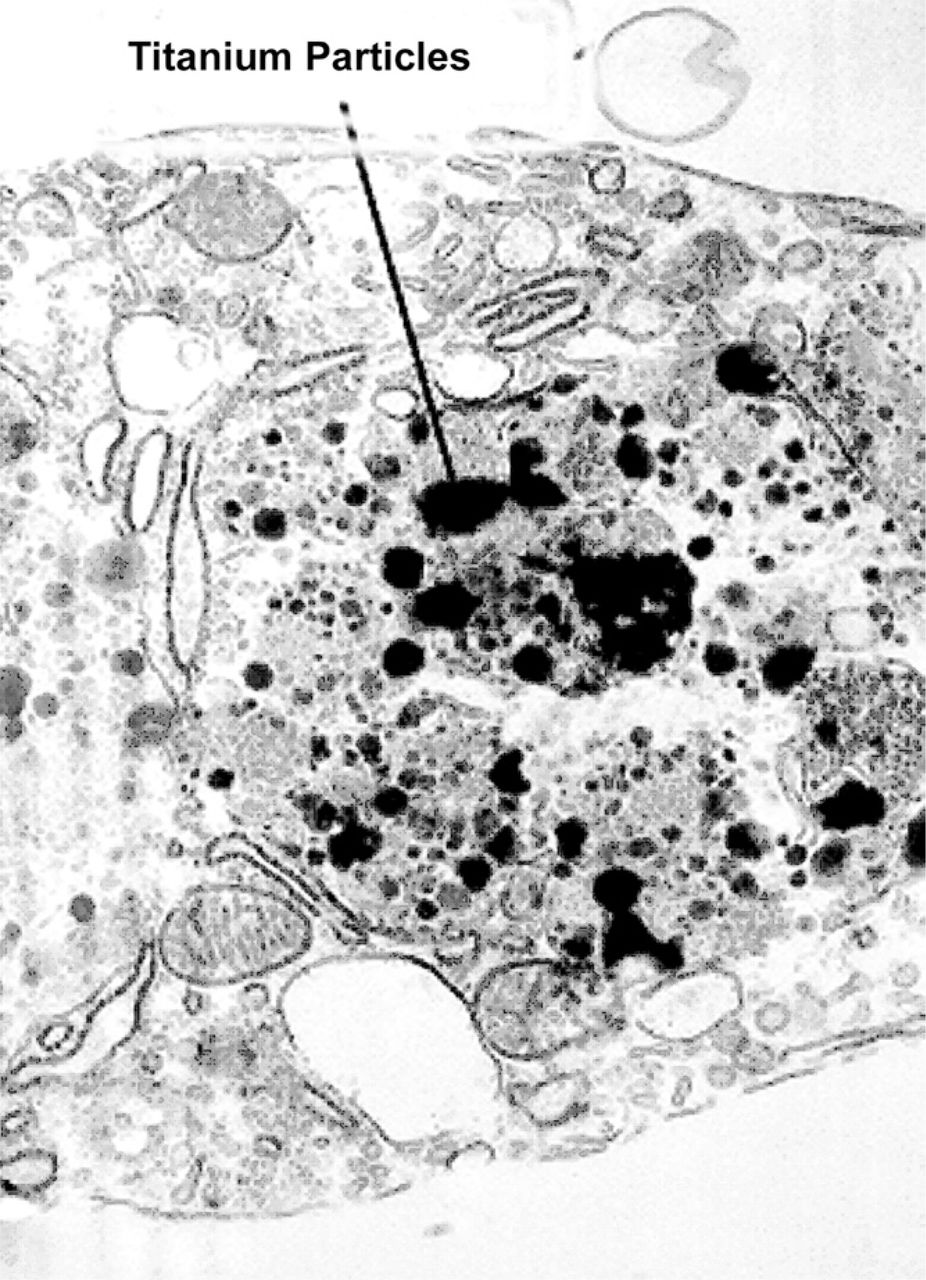
Transmission Electron Photomicrographs: (a) Macrophage containing phagocytized titanium particles. (b) Endothelial cell lining with embedded titanium debris. These specimens were obtained from a tissue sample overlying the posterolateral fusion mass (sixteen-week autograft + titanium) (TEM magnification = 20,000×) (courtesy of Bryan Cunningham).
Approximate average concentrations of metal in human body fluids with and without total joint replacements. Note: where ranges were reported they are included here within parentheses, eg (1– 4). All concentrations are reported in ppb (ng/mL)
Particle characterization. The fiction is that scanning electron microscopy is the best way to analyze the size of particles. The fact is that newer techniques, such as lowangle laser light scattering (LALLS), can increase the number of counted and sized particles from hundreds to millions or billions facilitating catching the one in a million large particle. Traditional particle-sizing techniques, such as SEM or TEM (number-based counting methods), indicated that the majority of the wear (mass loss) from an implant is comprised of particles in the nanometer to submicron range. This understanding largely stems from the relatively low numbers of particles (hundreds to thousands) used in traditional number-based analysis techniques such as SEM. Newer analytical techniques catch the one-in-a-million large particle that comprises a significant portion of the total mass loss (total debris). This contribution of large particles to the total debris mass, but insignificant contribution to the total number of particles, is made apparent in graphical representation of number and volume particle size distributions (Fig. 1). The counting of millions to billions of particles facilitates not only a number-based analysis, but because the one-in-a-million larger particle is also counted, a volume-based analysis is facilitated.
The ability to characterize accurately, and as comprehensively as possible, implant debris is critically important to the new generation of bearing surfaces used in novel spinal implants, where weight loss from the implant after a year of use (eg, less than 0.2 mm3 volume loss after a million cycles of use) could be attributed to the loss of a relatively few large particles or hundreds of millions of small particles (200 particles of 100 µm diameter is equivalent mass to 200 million particles only 1 µm in diameter). This phenomenon is illustrated in Fig. 1, where different samples of particles look demonstrably very different when viewed as a volume-based distribution, though they look very similar when analyzed using a number-based distribution. This shows how important it can be to have number- and volume-based distributions of the same particles to fully characterize the types of particles in the mix.
Metal ions (soluble debris). The fiction is that due to the smaller loads, spine arthroplasty implants release less metal ion into the body than hip or knee arthroplasties. The fact is that metal levels measured in people with disc arthroplasties have comparable levels of circulating metal ions as people with other TJA implants. There is continuing concern regarding the release of chemically active metal ions, which bind to proteins and remain in solution from which they can then disseminate into the surrounding tissues, bloodstream, and remote organs. Particulate metallic wear debris present an enormous surface area for electrochemical dissolution, which, in all likelihood, is a major factor contributing to observed systemic elevations in metals of patients with titanium implants.35 Normal human serum levels of prominent implant metals are approximately: 1-10 ng/ml Al, 0.15 ng/ml Cr, <0.01 ng/ml V, 0.1-0.2 ng/ml Co, and <4.1 ng/ml Ti. Following total joint arthroplasty, levels of circulating metal have been shown to increase (Table 1). The values in this table show that following successful primary total joint replacement there are measurable elevations in serum and urine Co, Cr, and Ti. Transient elevations of urine and serum Ni have also been noted immediately following surgery.
Recent studies of metal-on-metal TDA find serum levels of cobalt and chromium after TDA are elevated at concentrations of 3– 4 ng/mL or parts per billion (ppb) for cobalt and 1–2 ng/mL or ppb for chromium, which were significantly elevated over control values.54, 55 The concentrations of circulating Cr/Co measured in the serum of people with a metal-on-metal TDA are similar to levels measured in well functioning metal-on-metal total hip arthroplasties. This is not true for nonarticulating implants, where recent studies have failed to detect elevated amounts of circulating Cr or Ni from stainless steel scoliosis rod fixation systems.56 The long-term effects of presumably much higher elevations of metal proximal to the spinal implant remain unknown and are under careful surveillance by implant companies, the FDA and orthopedic researchers.57
There are subject dependent conditions that complicate using metal ion analysis as a diagnostic technique; eg, altered renal function has been reported to cause variability in circulating metal levels. Brodner et al have reported that renal failure is associated with highly elevated levels of serum Co and Cr (over 100-fold) in comparison with individuals with similar prostheses and normal renal function.58 At this time, there is no established toxicity threshold for the degradation products of metal implants.
Particulate debris reactivity characterization. The fiction is that, generally, different types of implant debris elicit the same level of inflammation. The fact is that different types of implant debris elicit different types of biologic response. However, despite the large number of published studies examining the effect of metal, polymer and ceramic particles on peri-implant cells (eg, macrophages, fibroblasts, osteoblasts, and osteoclasts), there is surprisingly little consensus on what type of debris are most pro-inflammatory. That said, there are a few general particle characteristics on which local inflammation has been shown to depend: 1) particle load (particle size and total volume), 2) aspect ratio, and 3) chemical reactivity. Thus, theoretically, a bioreactivity index of particulate would take the mathematical form:
Particle Pro-inflammatory Index
 1
1
where Ks are constants that depend on the testing environment and particle load is a function of both particle size and total debris volume.
Greater particle load: (size and volume) increases inflammation. The inflammatory response is proportional to the particle load (the concentration of phagocytosable particles per tissue volume, which is characterized by both the size and total volume).59, 60 If a given amount of debris (mass loss from an implant) is comprised of small diameter particles, there will be far greater numbers than if that same mass of debris was composed of larger diameter particles.60 The degree to which equal numbers (dose) of large versus small particles (eg, 10 µm vs 1 µm diameter) induce a inflammatory response on a per-particle basis in vivo has not been thoroughly investigated and remains an issue of debate. However, several past investigations have shown that for an equal amount of debris mass, smaller particles (eg, 0.4 µm) produce a greater inflammatory response than larger particles (eg, 7.5 µm).60–62 In these studies, the challenge doses used generally contain many thousands more small particles per cell than larger particles; this is largely responsible for these responses and the popular misconception that smaller particles are always more proinflammatory regardless of dose.
Elongated (fibers) particles are more pro-inflammatory than round particles. 63, 64 This phenomenon has been well established with the first such investigations over 30 years ago, involving asbestos fibers, which similarly cause inflammation through “danger signaling,” inflammasome activation and production of IL-1beta, IL-18, IL-33, etc, and activation of general macrophage pathogen associated molecular pattern pathways (NFkb and p38 production of proinflammatory cytokines IL-6, TNFα and PGE2 through as yet unknown mechanism).65, 66 This is discussed further in the following section on local implant induced inflammation. However, it remains unknown at what point (aspect ratio: length/width) in the transition of round particles to fibers that elevated inflammation is generally initiated. Currently, fibers can be categorized as particles with aspect ratio greater than 3, as has been shown in metal and poly retrieved from tissues.29, 44, 67
More chemically-reactive particles are more pro-inflammatory. There is a growing evidence that metal particles are more proinflammatory to macrophages (in general) when compared to polymers (ceteris paribas) and that some metals are more reactive than other metal particles.68 This opinion is not unanimous.69 More complicated still, there have been reports that have shown no differences between similar sized metal and polymer particles.70–72 Despite these reported differences, there is a growing consensus that metallic particles that are capable of corroding and releasing ions that have been associated with hypersensitivity responses, cytotoxicity, and DNA damage are thus more capable of eliciting proinflammatory responses when compared to relatively inert polymers and ceramics.73–75
Controversial particle characteristics. Does particle size matter? While there seems to be a large consensus that in vitro inflammatory responses require particles less than 10 μm in diameter, there continues to be debate on exactly what size particle produces the greatest inflammatory response.60–62, 76 Thus, to produce an in vitro inflammatory response, particles need to be less than 10 µm, that is, within a phagocytosable range. Purportedly, particles with a mean size of 0.2–10 µm are generally the most proinflammatory. Within this range there is no consensus as to which specific sizes and/or dose of particles (particles/cell or particles/tissue volume) are maximally inflammatory.60, 77–79
Endotoxin (bacterial-derived lipopolysaccharides) on wear particles is presumably important because it has been found in periprosthetic tissue of failed implants, even in the absence of clinical signs of infection.80 The relationship between bacteria and aseptic loosening has also been inferred, because antibiotic-eluting bone cement and systemically administered antibiotics reportedly reduce the frequency of aseptic loosening.81
Local and systemic bioreactivity of implant debris
The fiction is that implants generally “wear out” over time. The fact is that describing to patients that implants simply wear out over the long term mischaracterizes the main reason for long-term revision, aseptic loosening. Implant debris from wear cause local inflammation and granulomatous invasion of bone-implant contact that, over time, results in implant loosening and pain, necessitating revision arthroplasty.
Implant debris is known to cause inflammation, osteolysis, and, in some cases, hypersensitivity, and concerns about implant debris becoming carcinogenic and/or toxic persist. Macrophages are part of the innate immune system and, in the context of implant debris, are dedicated to phagocytosing debris, eliciting danger signals, and presenting antigen for T-cell recognition (ie, metal-protein complexes). Once debris is ingested by macrophages and other peri-implant cells, a host of pro-inflammatory reactions occur such as activation of metal-reactive T-cells through antigen presentation,73 release of pro-inflammatory mediators,60, 82–84 cytotoxicity,74 DNA damage,74, 85, 86 and oxidative stress.87 The central pro-inflammatory cells in this response are macrophages, which are generally responsible for mediating debris-induced inflammation leading to device loosening.
The following section will detail what is known of these different pathologies induced by implant debris and the primary suspects (kinds of implant debris for each pathology). Given that TJAs have been in use for over half a century with constant increases in biocompatibility and materials technology over that time frame, implant concerns about toxicity and carcinogenicity have been largely mitigated.
Debris-induced local effects. The fiction is that the amount of wear and corrosion debris produced from spine arthroplasty and modular spinal fixation implants are inconsequential and not likely to provoke a deleterious immune response. The fact is that biologic reactivity to spinal implant debris has been clinically observed with all the hallmarks of traditional particle-induced osteolysis; ie, granulomatous epithelioid membranes coating the metal implants have been reported, similar to the fibrous membranes associated with loose total hip replacements.19, 49, 50, 88–92
Although few, case reports of painful granuloma associated with spinal implant debris93, 94 demonstrate that spinal implant debris induced inflammation can result in bonedestroying granuloma.95 It is generally accepted that decreased wear and corrosion debris will lead to increased longevity of orthopedic implants. This rule of thumb has yet to be well established over the long term in newer types of articulating spinal implants; however, it is well established that debris induced inflammation and pain can be caused by spine implant debris.49, 94, 96–99
Macrophages are the major cell type responsible for mediating the pro-inflammatory response to implant debris that leads to inflammation and device loosening over time. Once implant debris is ingested by macrophages and other peri-implant cells, a host of biologic reactions can occur such as activation of T-cells through antigen presentation,73 release of pro-inflammatory mediators,60, 82–84, 100 cytotoxicity,74 DNA damage,74, 85, 86 and oxidative stress.87 Of these reactivity types, it is the pro-inflammatory response to wear debris in the local environment that has been the only known correlate of implant performance.11
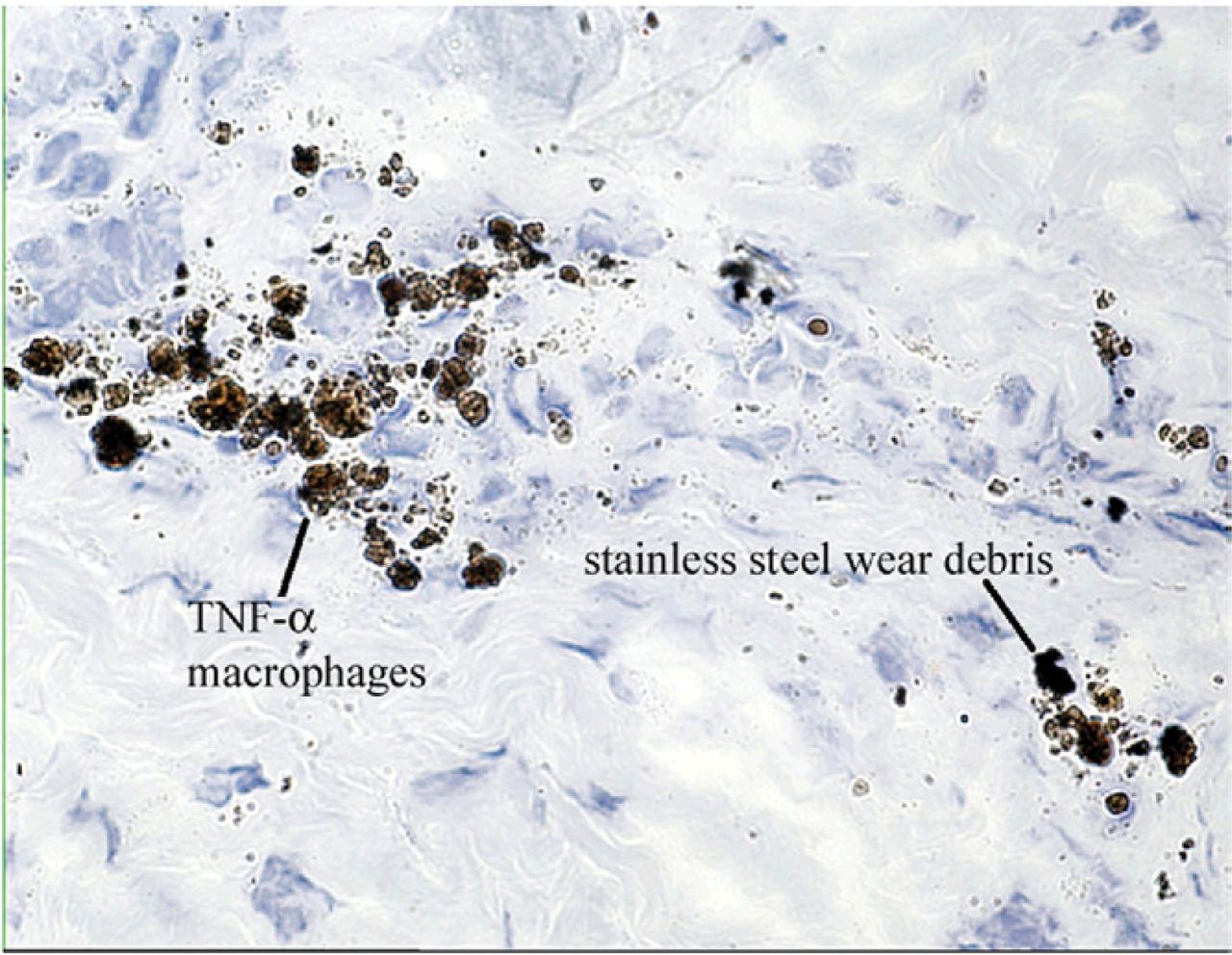
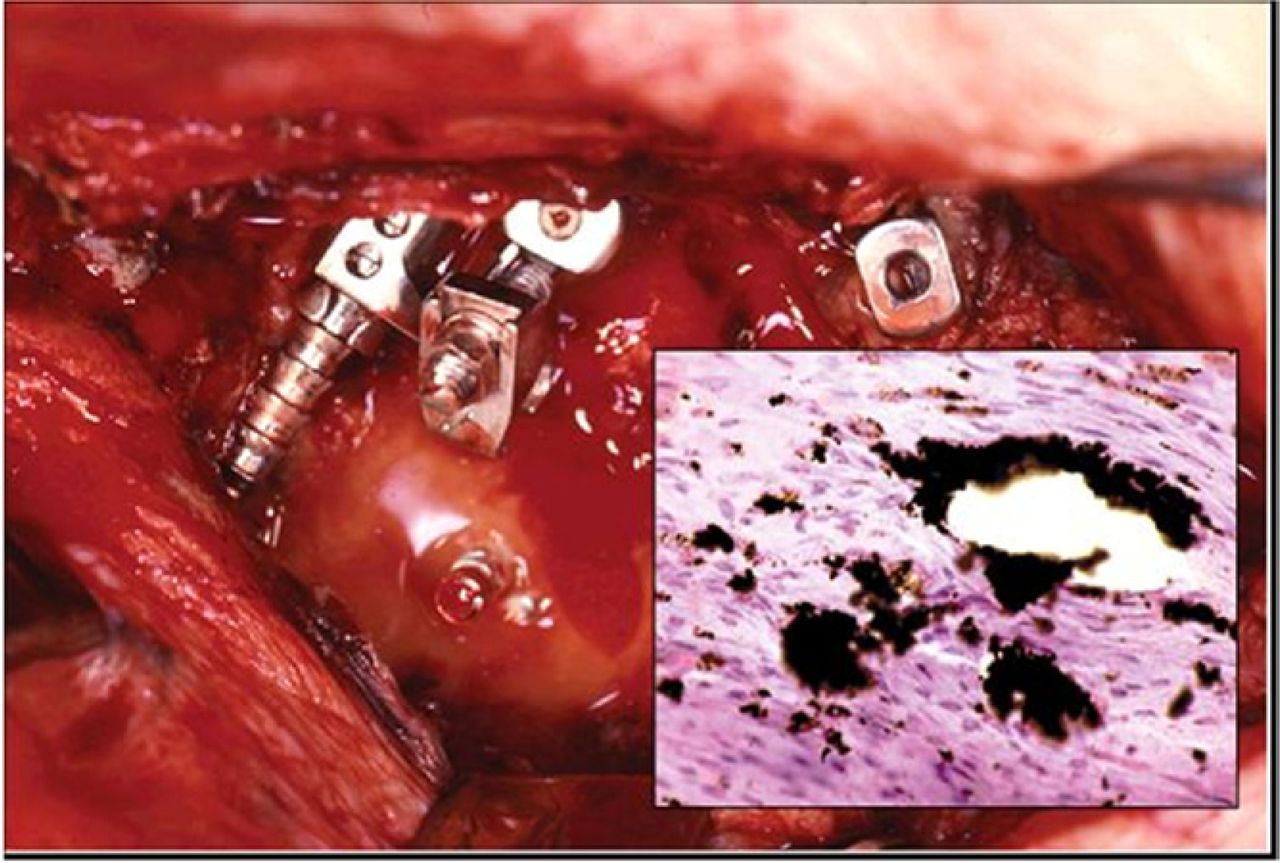
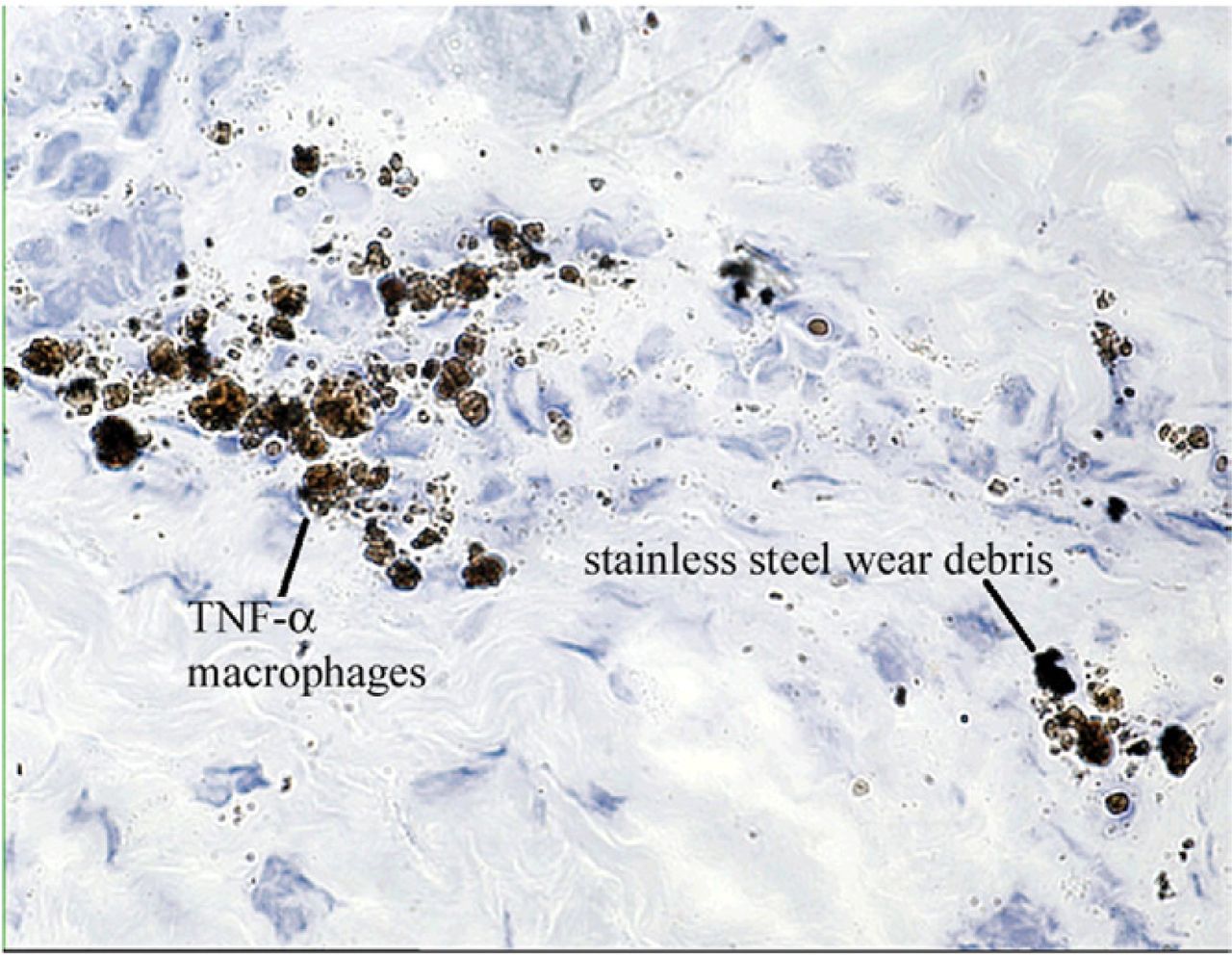
In the relatively few reports of human retrieval studies of loose spinal implants, granulomatous epithelioid membranes coating the metal implants have been shown similar to the fibrous membranes associated with loose total hip replacements.19, 49, 50, 89–92 However, before this phenomenon of wear debris can be well established in disc arthroplasty, larger series of implant retrievals will be needed to characterize the biologic responses to increased particle generation. When osteolysis or granulomas occur in the presence of metal debris, it is termed particle disease. In the case of metal debris, this is often accompanied by metallosis (aseptic black staining). Metallosis often accompanies metal implant debris-related osteolysis, aseptic fibrosis, local necrosis, or loosening. In a cohort of 12 loosened spinal implant cases, metallosis of the internal membrane was associated with the outer layer of membrane containing an infiltrate of leukocytes and macrophages (see Fig. 5). All 12 patients had radiolucency around part of the spinal instrumentation. Seven of the patients had titanium implants and 5 of the patients had stainless steel implants, showing this phenomenon is not limited to 1 type of material. Eleven of 12 clinical cases demonstrated elevated TNFαlevels and an increased osteoclastic response in the vicinity of wear debris caused by dry frictional wear particles of titanium or stainless steel (see Fig. 6). The focal areas of osteolysis most commonly involved loose transverse connectors. Resection of the wear debris stained tissue and surrounding fibroinflammatory zones resulted in resolution of clinical symptoms in all 12 cases.88

At surgical exploration the broken and dislodged instrumentation was accompanied by stainless steel particulate debris. Anteroposterior radiograph in a patient with breakage of a longitudinal rod connecting pedicle screws two years post-operatively. (Courtesy of Bryan Cunningham.)
TNF-α Cytokine Expressing Macrophages: Membrane-bound or intracellular TNF-α, contained in the tissue layer overlying the posterolateral sites, produced yellow to brown chromagen label as shown in this sixteen-week autograft + stainless steel particles in a rabbit model. (Avitan-Biotin Complex horseradish peroxidase technique for TNF-α, magnification 40). (Courtesy of Bryan Cunningham.)
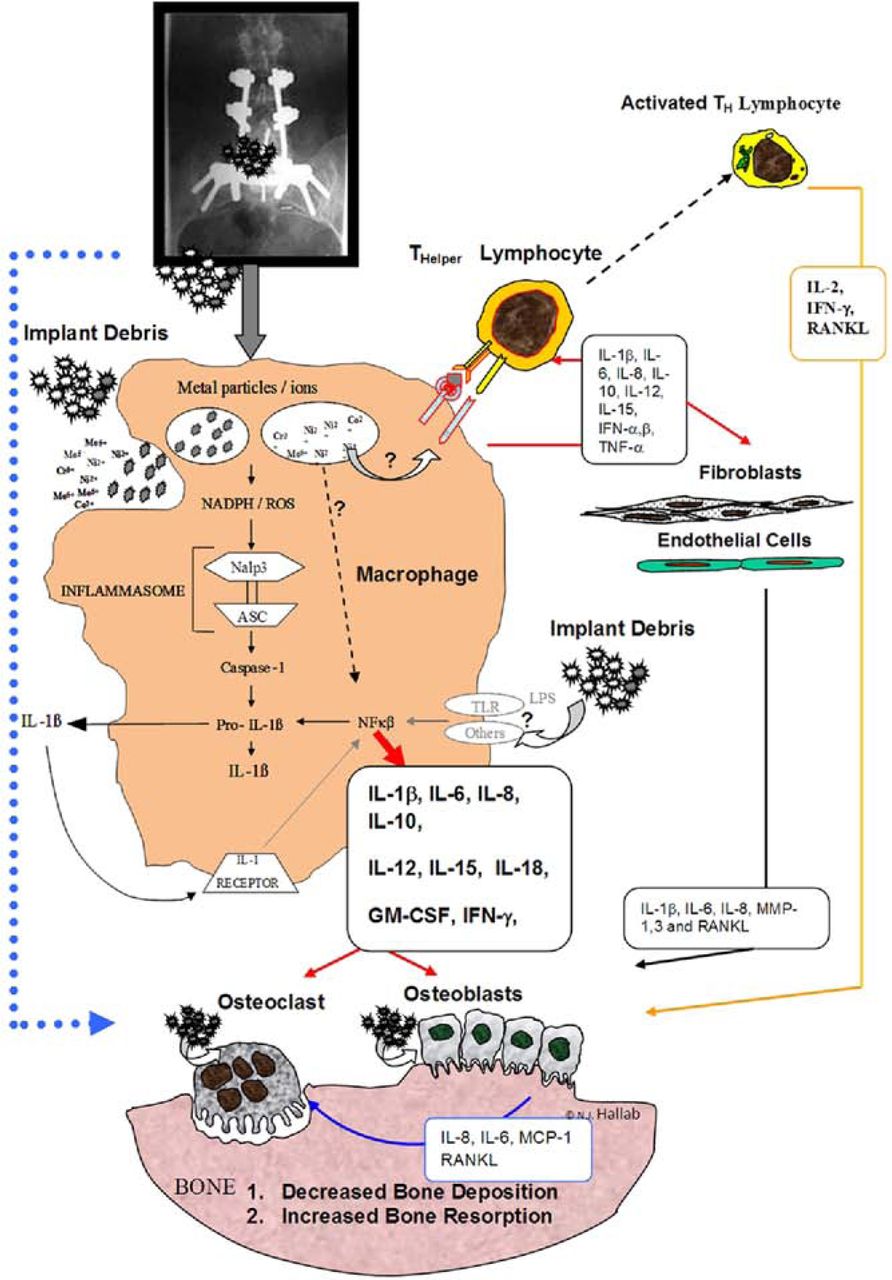
Particle-induced proinflammatory responses. The fiction is that implant debris looks like a pathogen and is recognized by the immune system through pathogen receptors. The fact is that implant debris elicits both general and “danger” signals in immune cells similarly to UV light, stress, and particulate adjuvants used in vaccines. The hallmark of implant debris in tissues101 is that it disrupts bone homeostasis through a number of pro-inflammatory responses. Particles activate macrophages that secrete TNFα, IL-1β, IL-6, and PGE2, stimulating differentiation of osteoclast precursors into mature osteoclasts and increasing peri-prosthetic bone resorption (see Fig. 7).102 Wear debris particles have also been shown to compromise mesenchymal stem cell differentiation into functional osteoblasts,103 and particles can directly inhibit collagen synthesis by mature osteoblasts104 and induce apoptosis of osteoblasts.105 Thus, it is not surprising that over time debris particles induce a net bone loss around implants that precipitates implant loosening.
Only recently have we learned how sterile, nonpathogenic stimuli, such as implant debris, can elicit an immune response. Immunologic reactivity responses can be divided into 2 categories: pathogenic stimuli and nonpathogenic stimuli, which act as “sterile” danger signals such as UV light and asbestos particles. In the constant battle with pathogens, we have evolved pattern recognition receptors (PRRs) in cell membranes and cytosol of immune cells that selectively detect pathogen-associated molecular patterns (PAMPs).106, 107
Sterile challenges, such as implant debris, produce DAMPs (danger-associated molecular patterns) which are different than PAMPs. Implant debris was first identified as DAMPs in 2008, and acts through the inflammasome pathway which leads to the release of IL-1β, a powerful proinflammatory cytokine.108 Cobalt, chromium, molybdenum, nickel ions, and Co-Cr-Mo alloy particles were found to activate the inflammasome pathway in part through NADPH-mediated monocyte/macrophage production of reactive oxygen species,65, 108 which suggests that metal-induced ROS is involved in inflammasome activation and IL-1β secretion. This is important to spinal implants debris, because activation of the inflammasome leads to cleavage of intracellular pro-IL-1β and pro-IL-18 into their mature forms, ultimately leading to their secretion and induction of a broad array of pro-inflammatory responses through autocrine and paracrine activation of NFκβ that initiates a powerful pro-inflammatory response (Fig. 7).106 Identification of inflammasome involvement in particle- and metal ion-induced inflammation will likely provide new therapeutic strategies to pharmacologically treat implant debris-induced inflammation and hypersensitivity by specifically interrupting the initiation of the inflammatory response that leads to aseptic osteolysis.

This schematic shows the numerous pro-inflammatory mediators produced by peri-implant tissue and immune cells reacting to implant debris, which can negatively affect bone turnover. The pro-inflammatory cytokines IL-1, IL-6, and TNF-alpha are thought to be some of the most potent cytokines in this cascade of signaling. The inflammasome pathway within cells such as macrophages has recently been reported to be central to implant debris mediated pro-inflammatory reactivity. Ingestion of the debris phagocytosis results in the release of pro-inflammatory cytokines that affect local cell types and induce a widening zone of soft-tissue damage and inflammation. (Courtesy of BioEngineering Solutions Inc)
Debris-induced systemic effects. Homogenates of remote organs and tissue obtained postmortem from subjects with Co base alloy total joint replacement components have indicated that significant increases in Co and Cr concentrations occur in the heart, liver, spleen, and lymphatic tissue (Table 1). However, these values have yet to be well established. Elements used in modern orthopedic implant alloys, including disc arthroplasty implants, are theoretically bioreactive through: metabolic alterations; alterations in host/parasite interactions; immunologic interactions of metal moieties by virtue of their ability to act as haptens (specific immunological activation) or anti-chemotactic agents (nonspecific immunological suppression), and chemical carcinogenesis. Implant metals such as Co, Cr, V, and possibly Ni are essential trace metals required for normal homeostasis. In nonorthopedic contexts of excessive exposure, all these metals have been linked to specific pathologies such as polycythemia, cardiomyopathy, carcinogenesis, and nephropathy. However, toxicity associated with any orthopedic alloy materials has not been reported. Also, it is important to note that despite the potential toxicologic possibilities, the association of metal release from orthopedic implants with any metabolic, bacteriologic, immunologic, or carcinogenic toxicity remains speculative; cause and effect have not been well-established in humans with knee and hip TJAs.118 The following discussion of the systemic effects of implant debris are divided into 4 areas: neuoropathic effects, hypersensitivity effects, carcinogenicity, and general toxicity.
Neuropathic effects of spinal implant debris. The fiction is that direct neuropathic effects of implant debris have been observed clinically. The fact is that neuropathies have been reported around both well-functioning and failing articulating implants, but were generated from a granulomatus (immune) response to implant debris, not directly from the implant debris.121–123 Patients have been reported to develop pain and inflammation of unknown etiology associated with spinal implants (screws) and shown resolution after implant removal.94, 95 However, adjacent tissues in these case studies of spinal implants have shown the presence of synovial-like granulomatous tissue, osteolysis, and elevated inflammatory mediators such as PGE2 speculated to be produced by the micromotion or debris of implants, such as a loose pedicle screw.94, 95 Thus, granulomatous inflammatory responses and not direct neuropathic effects were likely. Similarly, animal models of peri-spinal implant osteolysis using large amounts of particulate debris (>4 mg) have not resulted in observable neuropathy.84, 124 Conclusions from such studies remain guardedly optimistic, where observable debris induced inflammation was reportedly limited to the epidural space around injected (or placed) particles.125
Hypersensitivity to implant debris: Metal allergy. The fiction is that issues of metal sensitivity are not applicable to spine implants. The fact is that although rare, spinal implants have been implicated in case and group studies of hypersensitivity.126 Implant-related metal sensitivity is well documented in case and group studies, though overall it remains a relatively unpredictable and poorly-understood phenomenon in the context of orthopedic implant materials.127–129 Metal-protein complexes are considered to be candidate antigens (or more loosely termed, allergens) for eliciting hypersensitivity responses. The terms “metal sensitivity,” “metal allergy,” and “metal hypersensitivity” all refer to the same adaptive immune response to metal antigens by lymphocytes, typically characterized as a type IV delayed type hypersensitivity response. However, the specific T-cell subpopulations, the cellular mechanism of recognition and activation, and the antigenic metal-protein determinants created by these metals remain incompletely characterized.130–132
Metals known as sensitizers (haptenic moieties in antigens) are beryllium,133 nickel,133–136 cobalt,133 and chromium,133 while occasional responses have been reported to tantalum,137 titanium,138, 139 and vanadium.137 Nickel is the most common metal sensitizer in humans followed by cobalt and chromium.127, 134–136 The prevalence of metal sensitivity among the general population is approximately 10-15% (Fig. 8), with nickel sensitivity the highest (approximately 14%).127 The amounts of these metals found in medical grade alloys are shown in Table 1. Nonbiodegradable polymeric biomaterials used for load bearing in TJA are not easily chemically degraded in vivo and have not been intensely investigated or implicated in case or group studies as sources of hypersensitivity type immune responses.
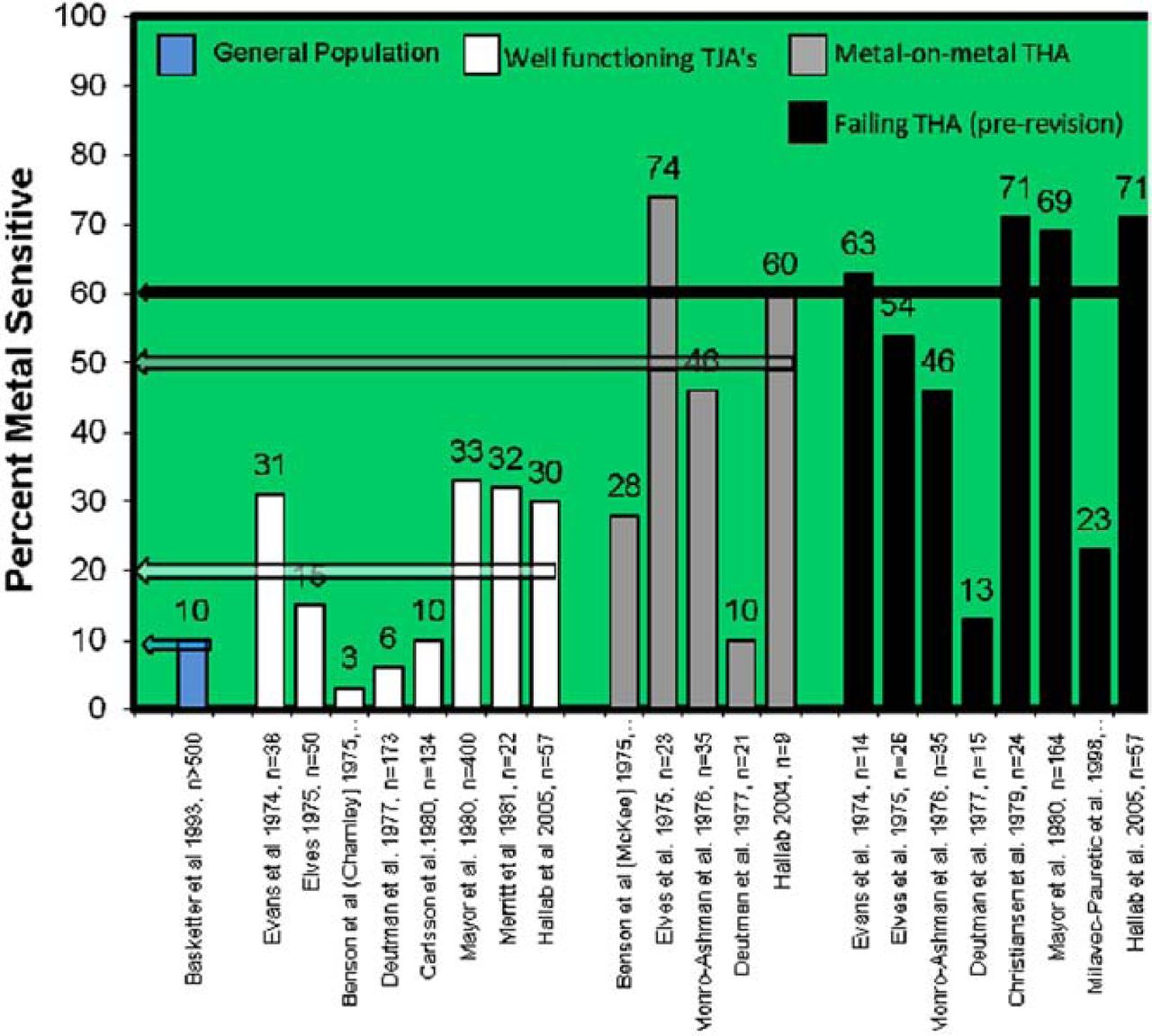
A compilation of investigations showing the averaged incidence percentages of metal sensitivity for nickel, cobalt or chromium among 1) the general population, 2) patients after receiving a metal containing TJA, 3) patients with metal-on-metal bearing arthroplasty and 4) patient populations with significant osteolysis or due to be revised. Note: Studies by Hallab et al used LTT to measure hypersensitivity, all other used dermal patch testing.
Testing for metal sensitivity. The fiction is that the only kind of testing for metal allergy is patch testing. The fact is that proliferation testing has been well established as a method for testing metal sensitivity in a variety of clinical settings.73, 140, 140–149 While patch testing and metal-LTT testing generally yield the same results, LTT testing may be equally or better suited for the testing of implant related sensitivity, because there is no risk of inducing metal sensitization using skin exposure; metal-LTT is highly quantitative and thus less dependent on the expertise of an observer to grade a response from +1 to +3; and the test is less costly, involves less patient discomfort, and is not subject to the same environmental susceptibility as patches that must be kept dry for 2-3 days.148, 150–152
Clinical studies of metal implant-related metal sensitivity. The fiction is that there are only a few case reports of this relatively rare phenomenon. The fact is that over the past 25 years, growing numbers of case reports link immunogenic reactions with adverse performance of metallic cardiovascular,153–155 orthopedic,128, 156–160 plastic surgical,161 and dental162–168 implants, which have sometimes required device removal.153, 156, 158–160, 169 Some of these reactions of severe dermatitis,139, 155, 158, 170 urticaria (intensely sensitive and itching red round wheels on the skin),154, 169 and/or vasculitis (patch inflammation of the walls of small blood vessels) have been linked with the relatively more general phenomena of metallosis, excessive periprosthetic fibrosis, and muscular necrosis.160, 171, 172 Generally, there are more case reports of hypersensitivity reactions associated with stainless steel and cobalt alloy implants than with titanium alloy components.128, 157–159, 169, 170, 173, 174
Cohort studies over the past 30+ years have generally indicated a correlation between metal implants and metal sensitivity.73 Data (from these different investigations) regarding the prevalence of metal sensitivity are compiled in Figure 8. The average prevalence of metal sensitivity among patients with a failed or poorly functioning implant (as judged by a variety of criteria) using the 7 investigations is 154 Hallab / SAS Journal 3 (2009) 143–160 approximately 60%.173, 175–178 Overall, the prevalence of metal sensitivity in patients with failed or failing implants is approximately 6 times that of the general population and approximately 2-3 times that of all patients with metal implants.
Despite the association of implant debris release from implants with adverse immunologic response, cause and effect have not been established in symptomatic patients with spine implants. Specific types of implants with a greater propensity to release metal in vivo may be more prone to induce metal sensitivity, as has been shown in total hip prostheses with metal-on-metal bearing surfaces (Fig. 8).176, 179 Metal sensitivity can be a contributing factor to implant failure.13, 157, 180 Spinal implants have been only rarely implicated in case or group studies of hypersensitivity.126 Thus metal-LTT may be warranted for people with a history of metal allergy prior to receiving an implant. The importance of this line of investigation is growing, as the use of metallic spinal implants is increasing and as expectations of implant durability and performance increase.36, 181
Carcinogenicity. The fiction is that there have been documented cases of etiologically linked implant debris and cancer. The fact is that the carcinogenic potential of the metallic elements used in TJA remains an area of concern, but one that has not been verified by any etiological evidence.182 Animal studies have documented the carcinogenic potential of orthopedic implant materials. Small increases in rat sarcomas were noted to correlate with high serum cobalt, chromium, or nickel content from metal implants. Furthermore, lymphomas with bone involvement were also more common in rats with metallic implants. Implant site tumors in dogs and cats (primarily osteosarcoma and fibrosarcoma) have been associated with stainless steel internal fixation devices.
The association of metal release from orthopedic implants with carcinogenesis remains conjectural, as causality has not been definitely established in human subjects. The actual number of cases of tumors associated with orthopedic implants is likely under-reported. However, with respect to the number of devices implanted on a yearly basis, the incidence of cancer at the site of implantation is relatively rare. Continued surveillance and longer-term epidemiological studies are required to fully address these issues.182–186
Toxicity. The fiction is that metals released from implants are not toxic to peri-implant cells. The fact is that previous nonclinical investigations of implant alloys using selected metals and selected cell lines show that high concentrations of metals can negatively impact cellular function.74, 187 However, the degree to which this occurs clinically is not known. Past investigations of implant-related metal toxicity include a variety of cell types (fibroblasts, endothelial cells, and nonhuman osteoblast-like cells),188, 189 but have, generally, been limited to in vitro studies and animal studies.190–192 Thus toxicity effects of implant debris around spinal implants remain speculative. However, given past in vitro and animal studies previously discussed, it is likely that metal toxicity effects can contribute to osteolysis in the periimplant area if present in sufficient concentration. However, the concentrations at which this will occur are not known and the degree to which soluble metals are able to contribute to clinical pathology is not well understood. However, metal induced toxic effects will likely be difficult to distinguish from well-established pro-inflammatory effects of metal particles.
The use of animal models to evaluate host biological response to spinal implant debris. The fiction is that there are strict definite limits to the amount of implant debris allowed by federal agencies. The fact is that there is no single limit for the amount debris generation from spinal implants. Each implant is put through a series of tests to determine the amount of debris expected, then a relative amount of similar debris is evaluated in an animal model. The evaluation of the biologic response to implant debris has been traditionally conducted using mice, rats, rabbits, and sheep animal models under such standards as ASTM F981-04 Standard Practice for Assessment of Compatibility of Biomaterials for Surgical Implants with Respect to Effect of Materials on Muscle and Bone. Larger animal models, such as primates, that may more closely approximate human responses to implant debris have prohibitively high costs and have been generally limited in use.84, 88, 193 Thus much of what we know of debris induced in vivo mechanisms/pathways of inflammation comes from small animal (mouse, rat, and rabbit) models194–197 and human clinical observations.19, 49, 50, 88–92 Small models have been used to investigate particulate debris of many different kinds and sizes.194–197 Generally, mouse and rat models have been used to assess inflammatory reaction and bone loss in calvaria, where particles are placed on the top of skull and the resulting inflammatory responses and bone loss are measured.196, 198–207 Rabbit models are typically used to assess new implant-related forms of particulate implant debris prior to FDA approval and the start of clinical studies. In these investigations, debris is injected or placed at the site of implantation.
Generally, the methods of testing particles in animals for the purposes of evaluating the biocompatibility of spinal implants involves: ascertaining the size and amount of debris that can be expected under implant appropriate loading conditions using mechanical simulator studies; producing similar-sized particulate debris in vitro; dosing animals with a bolus amount of debris equivalent to 10–50 years of implant use by placing debris onto the site of interest; and sacrificing the animals at 3 and 6 months to histologically examine peri-implant tissue either qualitatively or by quantitative immunohistochemical analysis, where tissue sections are stained for specific proinflammatory mediators (eg IL-6 and TNFα) and quantitatively compared to control animals with sham operations.84
The concentrations of powder typically implanted at the implant sites to induce osteolysis require using 1–30 mg particulate challenge (with a average particle size of 1–5 μm diameter) for a mouse of 25 g (0.0004 – 0.12% body weight),202, 208 where the debris (dry delivery to the implant site) is spread over a calvarial defect measuring 1 cm2. For rabbits, typically 0.01–200 mg of powder for a rabbit of 4.0 kg (<0.005% body weight) is typically used84, 193 and spread over implant sites at a concentration of 100 mg/6 cm2. The weight of a 50-kg human is 12.5 times that of a rabbit, and thus the 1– 4 mg of mass loss typical of an articulating human spinal implant is roughly equivalent to 50 –200 mg of debris over 50 years of implant use. This 50 –200 mg of debris in a 50-kg human scales down to 4 –16 mg of debris for a 4-kg rabbit for a 50 years of implant use. However, bolus injection testing challenges the animal with years of implant debris at a single time point, and using a 50 years worth of debris may erroneously elicit non-physiologically representative inflammation. Thus debris amounts equivalent to 10 years of implant use (approximately 10 million loading cycles) have been recommended as an appropriate proxy for small animal studies. This amount of debris is generally far above that required by the FDA for bolus injection studies in rabbits for simulated testing to 10 million cycles (10 years) of use (Guidance for Industry and FDA / Staff Preparation and Review of Investigational Device Exemption Applications (IDEs) for Total Artificial Discs, Document issued on: April 11, 2008: http://www.fda.gov/cdrh/ode/guidance/1637.html). However, the possible synergistic pro-inflammatory effects of multiple types of debris produced in modern spinal implants (eg, polyurethane + cobalt-alloy + titanium alloy) have not been tested together and the outcome of these types of challenge conditions remains unknown.
Discussion and conclusion
Given the reality of pro-inflammatory responses to debris produced from articulating spinal implants, 2 things are certain: 1) implant longevity will be limited by implant debris inflammation where eventual revision is likely in younger individuals, and 2) regular follow-up is necessary to ascertain the yearly extent of debris-induced bioreactivity. New techniques can be used to aid follow-up evaluations; for example, reliably measurement metal ion levels in low ranges (parts per billion) have shown clinical utility and can be used to indicate excessive implant wear. However, basic contamination precautions must be adhered to (eg, verifying all processing containers used for ICP-MS analysis are metal ion free). While several centers now have the capability of performing this testing routinely (eg, Mayo Clinic, Rochester MN), most hospitals and medical centers do not have this testing available.
The potential of released spinal implant debris to induce inflammation and osteolysis in the spine is well accepted, yet it remains unknown how to determine what tolerable thresholds are for each individual. It is generally accepted that the most important determinant of inflammation is particle dose (assuming particles are in the range of <10 μm and able to be phagocytosed by cells).79 However, not all types of particles are equally bioreactive. Particle bioreactivity general rules of thumb are: greater numbers of particles are more pro-inflammatory, and this inflammatory response is proportional to the particle load (the concentration of phagocytosable particles per tissue volume, which is characterized by both the size and total volume)59, 60; elongated particles (fibers) are more pro-inflammatory than round particles63, 64; and more chemically reactive (degradable and bioavailable) particles are more pro-inflammatory (ie, metals). There is a growing consensus of investigations that have shown metal particles are more proinflammatory when compared to polymers.68
The central hallmark of particle induced inflammation is innate immune cell (macrophages) secretion of TNFα, IL-1β, IL-6, and PGE2, which stimulate differentiation of osteoclast precursors into mature osteoclasts and increase peri-prosthetic bone resorption.102
With the growing number of people receiving spine arthroplasty implants and the issue of biologic reactivity looming, there is a growing need for more comprehensive diagnosis and intervention of untoward inflammation. Given that some versions of modern spinal arthroplasty designs have been in use for over 20 years internationally, implant concerns about neuropathology, toxicity, and carcinogenicity have been somewhat mitigated, yet remain incompletely addressed. New discoveries of how sterile nonpathogen implant debris lead to immune activation continue to be discovered, such as the inflammasome “danger signaling” pathway.108 Consequently, new therapies (such as Anti-TNF-Infliximab, Anti-IL-1β [IL-1β -receptor-antagonist Anakinra] etc) and diagnostic testing (metal-LTT and metal ion analysis) are continually being developed to help mitigate the subtle low-grade local inflammation which leads to eventual poor implant performance in some people more than others.
- © 2009 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.