


Abstract
Background L5 radiculopathy is a common problem that has several causes. Entrapment of the L5 nerve root by anterior osteophytes at the L5-S1 junction is rarely reported. Posterior decompression of the L5 nerve root is commonly performed, but anterior decompression of the L5 nerve root is not a frequently performed procedure. The purpose of this case report is to describe an uncommon case of L5 radiculopathy caused by the entrapment of the L5 nerve root by an anterior osteophyte.
Methods We report the case of a 79-year-old man with a right lower extremity L5 radiculopathy causing excruciating pain, worsening with transitioning between seated and standing positions. Radiologic evaluation showed a large osteophyte coming off of the right anterolateral border of L5-S1. The osteophyte was excised through a right-sided anterior retroperitoneal approach. An anterior interbody fusion was performed at L5-S1.
Results Postoperatively, the patient's pain was completely resolved. Six months after surgery, he remained symptom free.
Conclusions Osteophytes at the L5-S1 junction can entrap the L5 nerve root. If nonoperative treatment fails, the osteophyte can be excised and the nerve can be safely decompressed through an anterior retroperitoneal approach.
Compression of the L5 nerve root by abnormal anatomy at the lumbosacral junction causing sciatica was first cited in 1925 by Danforth and Wilson,1 who performed lumbosacral anatomic cadaveric dissections. They noted that the L5 nerve root could be compressed by bone spurs located at the junction of L5-S1. Osteophytic spurring from the L5-S1 vertebral bodies was identified in 7 of 29 geriatric cadavers examined by Matsumoto et al.2 Six of those cadavers showed entrapment of the L5 nerve root as compared with 1 of 22 cadavers without osteophytes (P < .05). Decompression of the L5 nerve root using a posterior approach has been reported in a very limited number of case reports.2–8 In a series of 4 patients, Matsumoto et al2 performed an anterior laparoscopic resection of an L5-S1 osteophyte in 1 of the patients. The purpose of this report is to describe a case of an L5 nerve root compression caused by a large L5-S1 osteophyte and its resection using an open anterior retroperitoneal approach.
Case report
A 79-year-old man presented with signs and symptoms of a right-sided L5 radiculopathy for approximately 6 months. The patient's medical history was significant for coronary artery disease, hypertension, colon cancer, stomach ulcers, and gout. He rated his leg pain as 8 of 10 and stated that the pain was worse with sitting and changes in position between sitting and standing. There was no complaint of back pain. His history also showed neurogenic claudication symptoms on the right side that improved with rest.
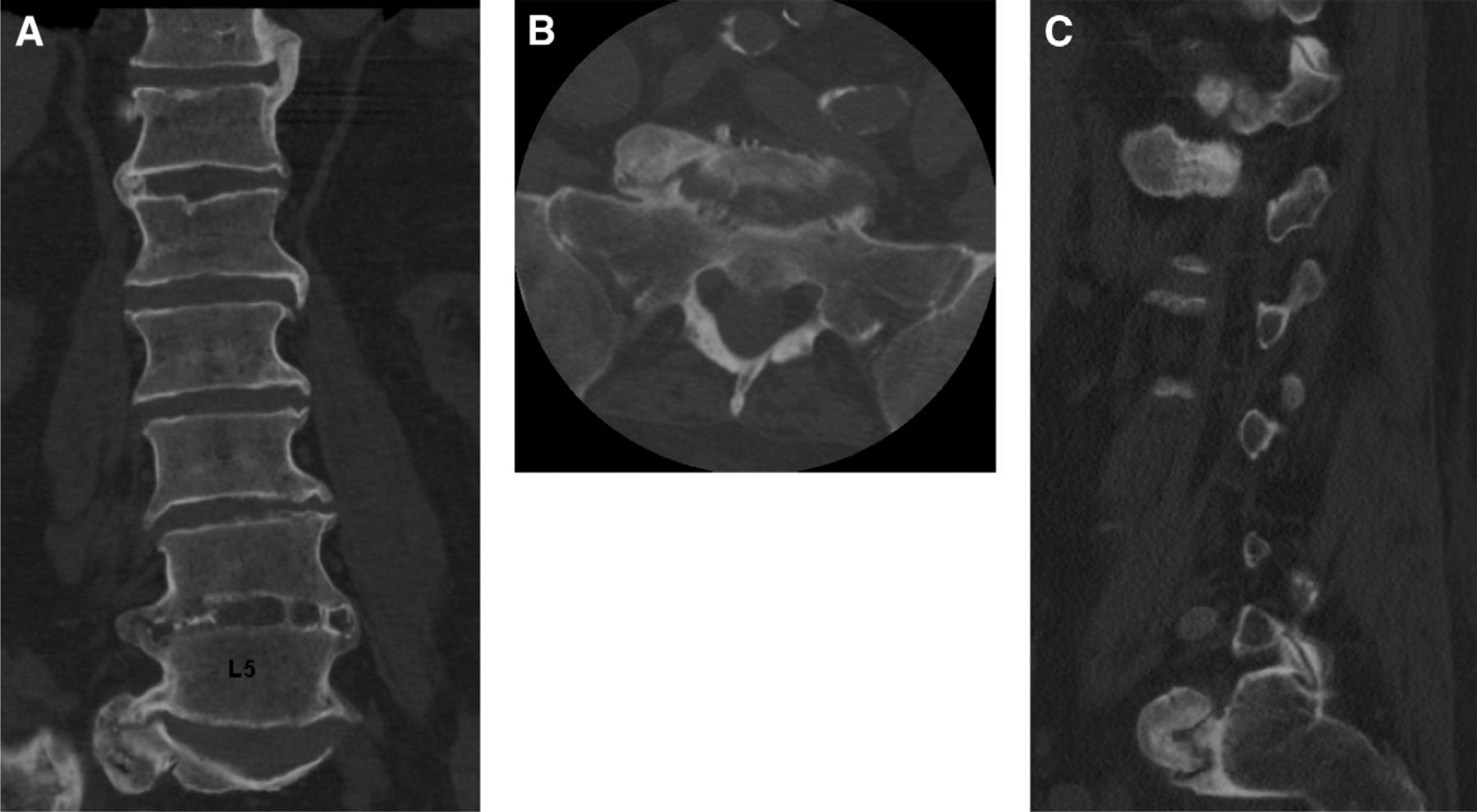
Physical examination showed normal motor strength on manual testing and a normal sensory examination. The patient did have reproducible pain with right-sided straight leg raise. X-ray (Fig. 1) and computed tomography (CT) scan (Fig. 2) of his lumbar spine showed a large anterior osteophyte at L5-S1 that appeared to contact the sacral ala.

Anteroposterior X-ray showing osteophyte at junction of L5-S1 on right side (arrow).
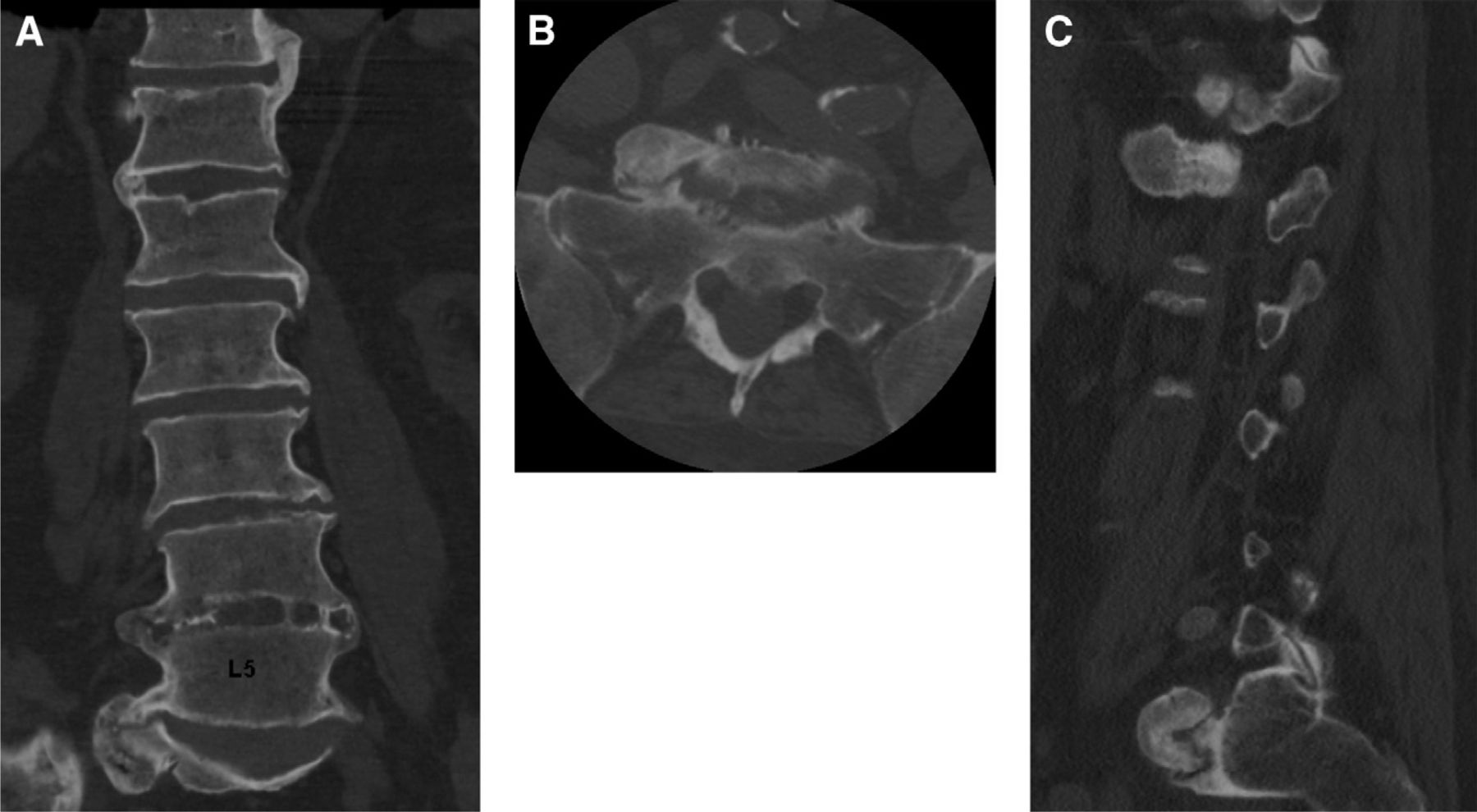
(A) Coronal CT image showing osteophyte at L5-S1. Axial (B) and sagittal (C) CT images of osteophyte coming into contact with sacral ala.
A selective transforaminal L5-S1 nerve root injection was performed, which resulted in significant improvement of the patient's symptoms during the anesthetic phase of the injection. After continued pain and exhaustion of nonoperative therapies, including medications, physical therapy, and injections, the patient elected to undergo surgical intervention. He underwent L5-S1 anterior lumbar interbody fusion with BAK cages (Zimmer Spine, Minneapolis, MN) with resection of the anterior osteophyte and decompression of the right L5 nerve root through a retroperitoneal approach. The L5-S1 space was approached from the right side because of the osteophyte being on the right. The disc space was exposed through the bifurcation of the vessels. After complete removal of tissue from the disc space, BAK cages were placed and filled with graft material. Once the cages were confirmed to be in position by anteroposterior and lateral imaging, the osteophyte was then exposed. It was found to be lateral to the right iliac vein and artery. The surgeon was able to identify the medial corner of the osteophyte where it attached to the anterior vertebral body at L5. A 12-mm osteotome was used to release the osteophyte from the vertebral body. Once the osteotome was positioned at the attachment point, it was tapped until the osteophyte released. At this point, the L5 nerve was readily identified but not further dissected. The resected osteophyte correlated closely to a 3-dimensional (3D) model reconstruction (prepared courtesy of DePuy Spine, Raynham, Massachusetts) used for further interpretation of the anatomy from the patient's CT scan (Fig. 3). The patient had complete resolution of his leg pain immediately after surgery. Six months after surgery, he was still pain free and participating in active rehabilitation.
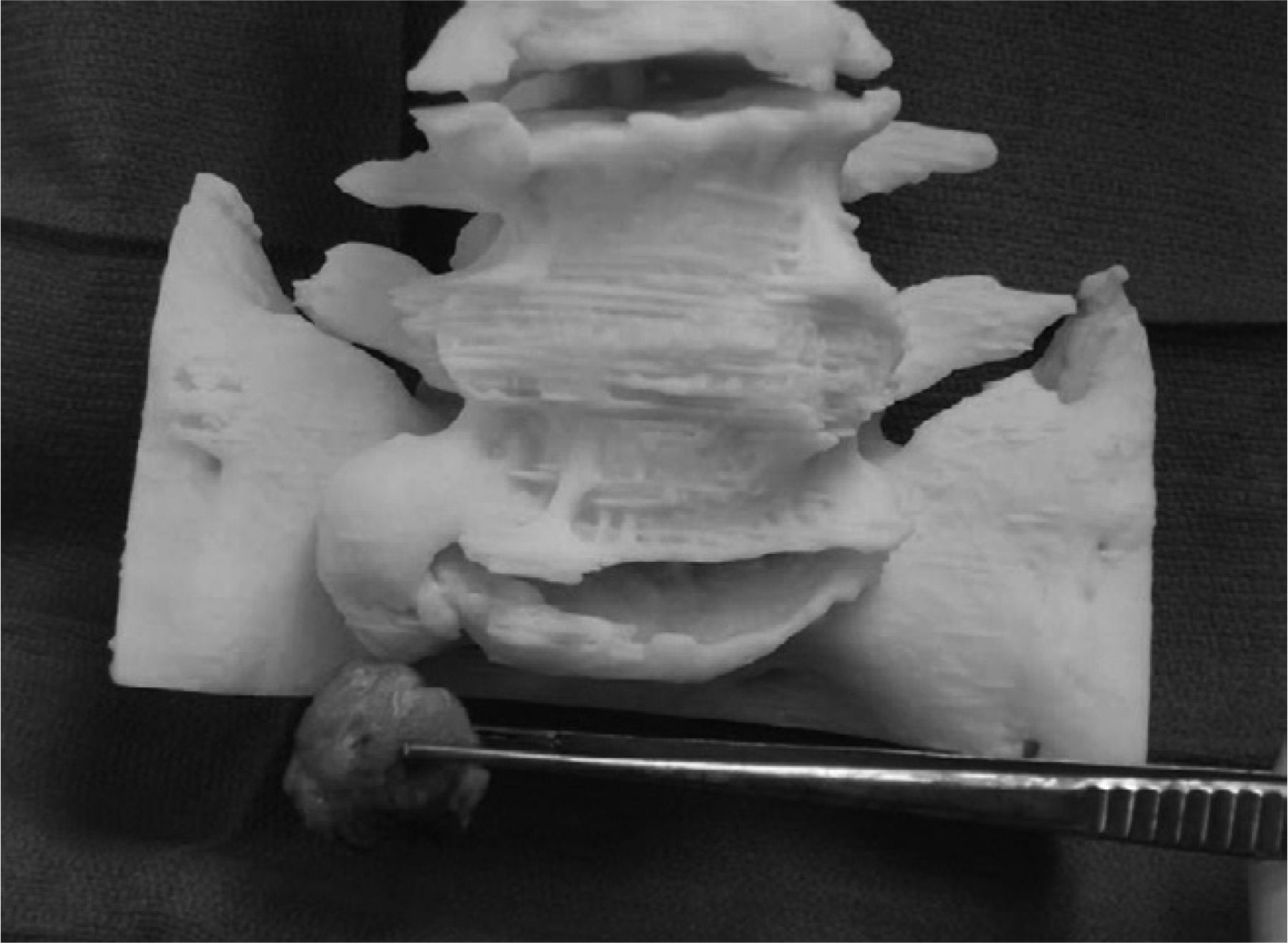
A 3D model created from CT scans accurately portrayed the location and size of the osteophyte.
Discussion
There have been only a few case reports of L5 radiculopathy caused by anomalous bony articulations between L5 and S1. Although this patient had an L5 radiculopathy, it is different from the “far-out syndrome” traditionally described by Wiltse et al.8 He did not fit into any of the categories described in their series that included elderly patients with degenerative scoliosis and a younger group of patients with isthmic spondylolisthesis with at least 20% slip who showed symptoms of an L5 radiculopathy caused by entrapment of the L5 nerve root between the transverse process of L5 and the sacral ala. This patient had entrapment of the nerve root by a large anterior osteophyte protruding anterolaterally from the L5-S1 disc space.
Matsumoto et al6 reported on a series of 28 patients with extraforaminal entrapment of the L5 nerve root at the lumbosacral junction. CT imaging showed the presence of marked osteophytes at the posterolateral margin of the L5-S1 vertebral bodies. By use of a microscopic or microendoscopic posterior approach, they were all decompressed with partial resection of the sacral ala, L5 transverse process, and L5-S1 facet joint along the L5 root. The authors did not make any attempt to resect the osteophyte to avoid damage to retroperitoneal vascular structures, nor was any patient initially fused. All patients in their series had immediate pain relief; however, 4 underwent revision with posterior interbody fusion for recurrent radicular pain due to intraforaminal stenosis in 3 patients and inadequate extraforaminal decompression in the other. In contrast, in our case report, an anterior retroperitoneal approach was used to directly visualize the osteophyte, which was resected, and anterior lumbar interbody fusion was performed concurrently.
Abe et al9 first reported on the use of an anterior approach in a single patient to decompress the L5 nerve root compressed by an anomalous alar transverse process. In addition to diagnostic injections and traditional imaging, they used selective radiculography to confirm the diagnosis and believed that this was the most useful diagnostic test to diagnose this condition. Selective radiculography was not used in our case, because there was no evidence of traditional spinal canal or foraminal pathology present on imaging. However, it could have been used to gain further confirmation and accurate localization of the entrapment. Furthermore, the use of diagnostic injections should absolutely be performed diagnostically and exhausted therapeutically, before proceeding with any type of surgical intervention.
The use of advanced imaging was critical to the diagnosis of our patient's condition. Moon et al10 found that 77% of patients in their retrospective review of preoperative CT scans in 27 patients showed an asymmetric enlargement of the anterior primary division of the L5 nerve root that was significantly associated with foraminal or extraforaminal compression of the root at the lumbosacral junction. In our case, even more valuable than the CT scan was its extrapolation to create a 3D model. This was helpful to the surgical team's understanding and visualization of the patient's anatomy and pathology. Intraoperatively, the surgeons repeatedly referred to the model. The resected osteophyte closely resembled what was expected. In such cases, use of the 3D model is recommended because most surgeons will be unfamiliar with this rather rare pathoanatomy.
Osteophytes and other anomalous bony abnormalities account for some cases of entrapment, but thickened lumbosacral ligaments (LSL) can also contribute to root compression. In a cadaveric study of 42 specimens, large osteophytes on the inferior border of L5 and tightness of the LSL were found to contribute to entrapment of the L5 nerve root.11 Olsewski et al12 identified an 11% rate of LSL compression of the L5 nerve root in 102 specimens. Although a thickened LSL may contribute to compression in cadavers, it may not always be symptomatic in vivo. Extraforaminal disc herniations may also play a role in entrapment of the L5 nerve root at the lumbosacral junction. O'Toole et al13 reported a case of microendoscopic discectomy performed at the lumbosacral junction with successful relief of the patient's symptoms.
In our case, the decision was made to perform a concurrent arthrodesis based on the patient's history of increased pain with transition to sitting or standing. It was thought that this would increase the chances of achieving a successful outcome by eliminating movement across the joint as a potential source of compression. In other case reports, this has not been routinely performed concurrently, but there is not an abundance of evidence to support or negate its use.
In conclusion, extraforaminal entrapment of the L5 nerve root has many different causes and must be considered in patients presenting with an L5 radiculopathy. In this case, a large anterior L5-S1 osteophyte was removed safely using the anterior retroperitoneal approach, which yielded a good clinical result.
- © 2012 Published by Elsevier Inc. on behalf of ISASS - International Society for the Advancement of Spine Surgery.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.