


Abstract
Background Morbidity and mortality scores are useful to control for medical comorbidities in study populations where either effects of an illness or benefits of a treatment are examined. Our study examined if a direct relationship existed between the American Society of Anesthesiologists Physical Status (ASA) score and the Charlson Comorbidity Index (CCI) in an osteoporosis population where patients had sustained a vertebral compression fracture.
Methods A retrospective chart review of patients with osteoporotic compression fractures treated by the same orthopedic surgeon between June 2000 and June 2004 was performed. The primary endpoint was death by the close of the study period (September 2006). A board certified Anesthesiologist blindly assigned all of the ASA scores as well as the Charlson Scores independently in a blinded manner. All patients were assumed to be undergoing surgery as they were assigned. A statistical relationship was examined between ASA and CCI scores through a cross table analysis with chi-squared testing as both scoring systems were considered categorical. A Pearson correlation was completed to examine the quality of a linear relationship between the categorical variable ASA compared to the continuous variable Charlson. A value of p < 0.05 was considered significant.
Results Ninety patients elected conservative therapy with oral analgesics and an orthosis, while 94 patients elected for kyphoplasty. The CCI by log rank testing was not significant (p= 0.2027) for the surgery population; however, the test resulted in a highly significant value (p = 0.0161) in non-operative population. The ASA Score was correlated with significance to mortality (p= 0.0150) for the surgery population, while the test was not significant (p = 0.1439) in non-operative population. Treating both ASA and CCI scores as categorical variables, a relationship between them was examined and found to be highly significant (p= 0.000001) meaning patients with low ASA scores were likely to have low CCI scores.
Conclusion The ASA score was predictive of mortality in a surgical population, while CCI was highly predictive of mortality in a non-surgical population. There is great agreement between the CCI score and the ASA score, reflecting that anesthesiologists subjectively consider the same elements of the patient's medical history when assigning ASA scores as the CCI objectively uses. This was a Level III Study.
- american society of anesthesiologists physical status score (asa)
- charlson comorbidity index (cci)
- mortality
- vertebral compression fracture
Introduction
Morbidity and mortality scores are useful to control for medical comorbidities in study populations where either the effects of an illness or the benefits of a treatment are examined. In particular, the American Society of Anesthesiologists Physical Status (ASA) score and the Charlson Comorbidity Index (CCI) have been used in a multitude of studies to assign patient groups, ensure minimal group variability, and relay mortality or morbidity.
In 1941, Rovenstein, Saklad, and Taylor published a grading system defining six degrees of physical state specifically “for the collection and tabulation of statistical data in anesthesia.” Five categories of the American Society of Anesthesiologists Physical Status (ASA) Score was proposed by Dripps et al. in 1961 1 and accepted by the ASA in 1963.2 In October 2014, the American Society of Anesthesiologists adopted a six category classification system.3 The ASA score has become widely used to describe preoperative physical status (See Table 1). It is also used to predict peri-operative risk, 4, 5 despite the fact that it was never designed for this purpose.6 The Charlson Comorbidity Index was originally designed as a measure of the risk of one year mortality attributable to comorbidity in a longitudinal study of general hospitalized patients. Its contents and weighting scheme were created on the basis of Cox proportional hazards modeling.7 It was later adapted for International Classification of Diseases, Ninth Revision (ICD-9), codes to be used to calculate the Charlson Comorbidity Index with existing data.8 A weighted index of comorbidity is determined objectively based on the presence of nineteen medical conditions. This weighted index is then added to an age-related risk to determine an overall comorbidity score (See Table 2).
ASA Physical Status (PS) Classification System.
Comorbidity Weights for Calculation of the Charlson Comorbidity Index.
The purpose of this study was to examine if a direct relationship exists between the ASA score and the CCI in an osteoporosis population in which a patent has sustained a vertebral compression fracture. This study population was chosen because recent literature has found that osteoporosis, marked by vertebral compression fractures, may be a potential marker for increased mortality. Fractures of the hip and vertebral body are the most commonly associated injuries with increased post-injury mortality.9–15 Mortality after vertebral fractures has been reported to range between 16% and 60% greater than an unaffected population.15–17 In a previous publication, these two morbidity scores provided a control for the medical comorbidities of patients with osteoporosis who sustained vertebral compression fractures treated either surgically or conservatively.17 We found both instruments to be statistically predictive of survival for the entire patient population. At that time, we did not examine the relationship between the two morbidity scales or whether either score was a better predictor of morbidity in the surgical versus non-operative patient population. Others have found a direct relationship between the CCI score and ASA score for survival in patients with genitourinary and head and neck cancer.18, 19
Methods
A retrospective chart review of patients with osteoporotic compression fractures treated by the same orthopedic surgeon between June 2000 and June 2004 was performed. Patients received either non-operative care consisting of oral analgesia and an orthosis, or surgical care with a kyphoplasty procedure. Patients with multiple myeloma, metastatic bone disease, or a burst fracture were excluded. Patients were diagnosed with a new vertebral compression fracture based on history and physical examination combined with plain radiographs and a bone scan and/or magnetic resonance imaging (MRI) when necessary to confirm the diagnosis and document fracture acuity.
The primary endpoint was death by the close of the study period which ended September 2006. Data were considered censored if the patient survived to the end of this study period. Patients were followed at an outpatient office. If recent follow-up was not obtained from the chart, patients were contacted by telephone to confirm their survival. Additionally, the Social Security Death index was reviewed for patient death during the study time period. Patient factors including age at the time of the initiation of conservative treatment, gender, and the presence of a previous non-acute compression fracture diagnosed by imaging at the time of the patient's assessment were also recorded. Medical comorbidity data were also collected from the patient's hospital and office charts. A CCI score was assigned to all patients by one physician following the guidelines established by Charlson et al.7 The online Charlson calculator provided by the Institute for Algorithmic Medicine was utilized to calculate the CCI. Charlson scores were grouped into 1, 2, 3, or 4+ to facilitate statistical evaluation. A single attending anesthesiologist assigned all patients an ASA score. A board certified Anesthesiologist blindly assigned all of the ASA scores as well as the Charlson Scores independently in a blinded manner. All patients were assumed to be undergoing surgery as they were assigned. This study only considered the medical comorbidity analysis as we have published on the effect of surgery (kyphoplasty) in a previous paper.
Statistical Methods
Data were recorded in an Excel Spreadsheet. NCSS/ PASS statistical analysis software (Kaysville, UT) was used to analyze the data. Patient survival curves were constructed for each of the study populations and subpopulations. Differences in survival based on comorbidity scoring were examined through log rank testing. A statistical relationship was examined between the ASA and CCI scores through use of a cross table analysis with chi-squared testing as both scoring systems were considered categorical. A Pearson Correlation was completed to examine the quality of a linear relationship between the categorical variable ASA compared to the continuous variable Charlson Score. A value of p < 0.05 was considered significant.
Results
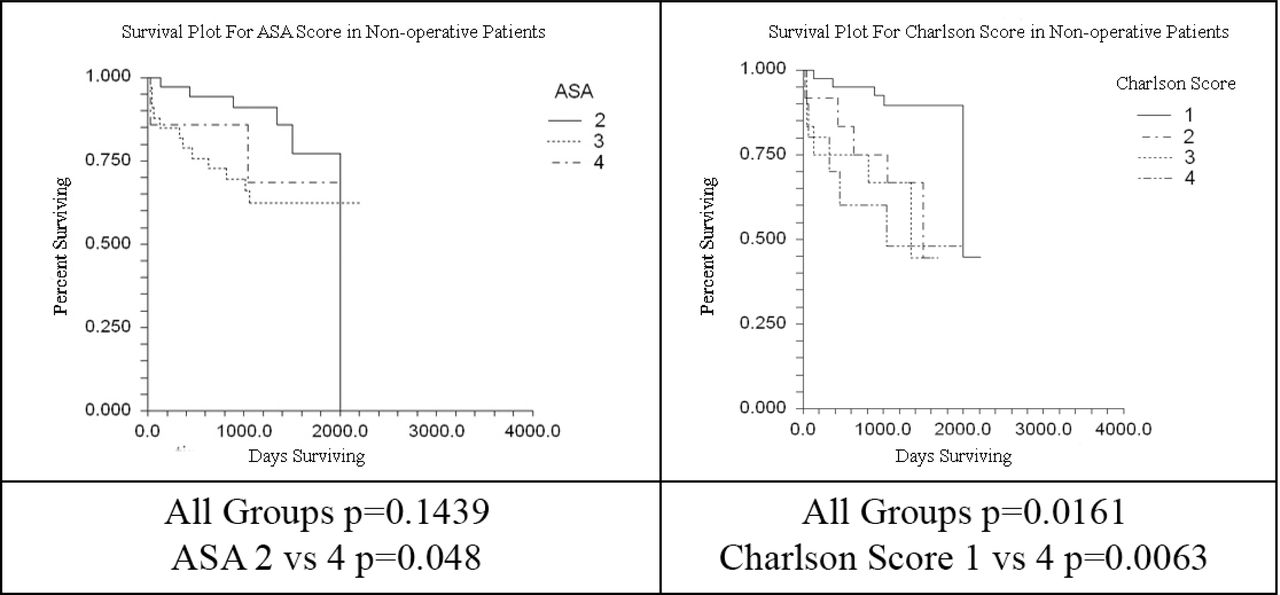
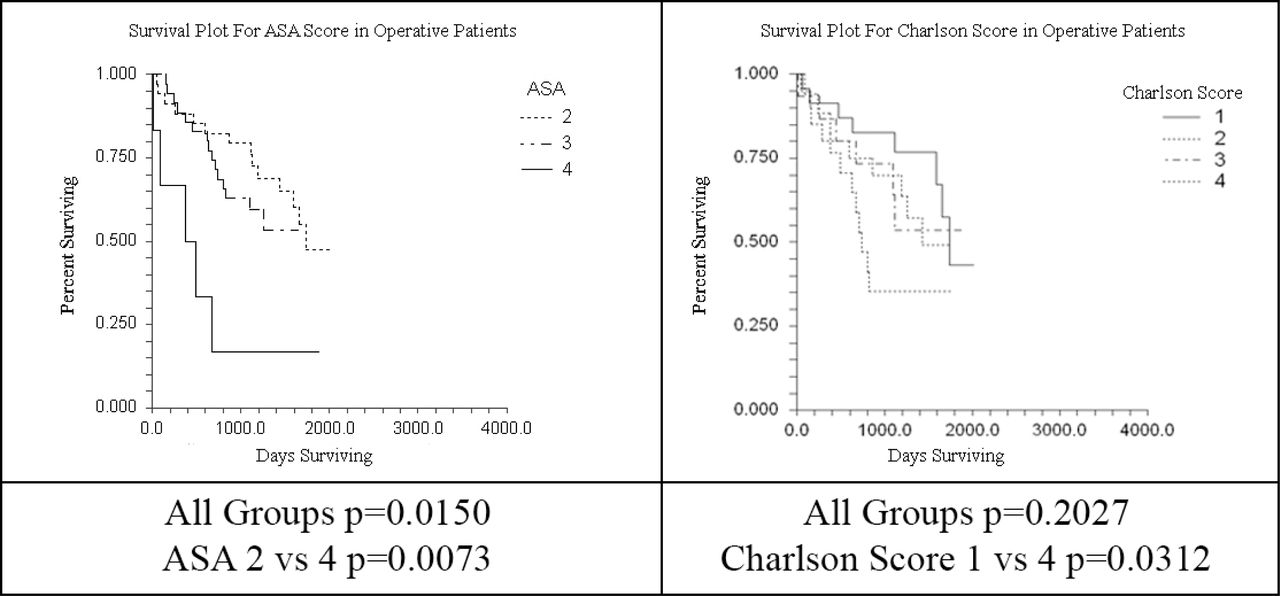
Ninety patients elected for conservative therapy with oral analgesics and an orthosis, while 94 patients elected for kyphoplasty. All vertebral body fractures of fragility were included in the study. The survival plots for both surgical and non-surgical patients with their correlation to the ASA and CCI scores are seen in Figure 1 and Figure 2. The CCI by log rank testing was not significant (p= 0.2027) for the surgery population while the test resulted in a highly significant value (p = 0.0161) in the non-operative population (See Table 3). The opposite was seen with the ASA score. The ASA Score was correlated with significance to the mortality (p= 0.0150) for the surgery population while the test was not significant (p = 0.1439) in the non-operative population.

Survival Plots for non-operative Patients.

Survival Plots for Operative Patients.
Log Rank Tests for Operative versus Non-operative Patients.
Treating both the ASA and the Charlson scores as categorical variables, a relationship between the two was examined and found to be highly significant (p= 0.000001) meaning that patients with a low ASA scores were likely to have low CCI scores.
A linear regression model was created using Charlson Score as a dependent and continuous variable. An R squared value of 0.330 was found with a significance value of (p = 0.001). Table 4, Table 5, and Table 6 demonstrate the percentage of patients with each of the morbidity assessments. Table 7 demonstrates the mean morbidity scores for the operative and non-operative populations.
Total Population Morbidity Scores.
Non-Operative Morbidity Scores.
Operative Morbidity Scores.
Comparison of Mean Morbidity Scores.
Discussion
The American Society of Anesthesiologists (ASA) classification is a readily available and widely accepted method for stratification of surgical patients according to their peri-operative risk.19 ASA scores have been seen in multiple studies to have low inter-observer reliability, but are frequently incorporated in studies to cite reduced variability and predict mortality. ASA scores are typically assigned at the bedside immediately before surgery. These scores have been found to be predictive of mortality for a variety of other conditions.7, 19 The ASA is a subjective assessment without a rigid formula used to assign a score; therefore, it is inclusive of all available medical history and easily assigned.
In contrast, the Charlson Comorbidity Index instrument rigidly assigns a score based on the presence of specific comorbidities which possess various weights. To this end, Charlson scores are much less subjective, yet all conditions are not addressed by a Charlson score. CCI scores are a useful way to examine medical records as they may be calculated using recorded ICD-9 codes.
The goal of our analysis was to determine the agreement between these two comorbidity classification systems and to determine if one system predicted morbidity more reliably in surgical versus non-operative subpopulations. Our data may suggest that the ASA is a better instrument for stratifying operative patients while the CCI score is better for non-operative patients. However, this may be an effect of the population size of each group. It is more likely that this study merely illustrates that patients with poor scores in both systems are at a higher mortality risk while those identified at low risk in either system survived longer. Both systems have somewhat more difficulty stratifying patients of intermediate risks. This is where both systems are lacking. In comparisons made for other disease processes, such as cancer, authors have chosen to combine comorbidity classification subgroups when listing morbidity percentiles. Therefore, patients were regarded as either having a high or low degree of morbidity. It is not surprising that in both of our patient populations, when the lowest scoring and highest scoring patients were compared, both systems were highly significant for both surgical and non-operative patients. The relationship between these variables was examined categorically through a Chi Squared test which would imply that the Charlson scores for ASA groups differed statistically between each group. This relationship was also examined through a linear regression model. As the ASA score is not a continuous variable this would not be an ideal model to examine a potential relationship. Specifically, if treating the Charlson score as a continuous variable there are few patients with a score of greater than a four. This is why our assessment was completed in a categorical manner. Table 4 demonstrates that the percentage of patients with a categorically low ASA also had a categorically low Charlson Score.
Certainly a limitation of this study is that a single physician assigned either the ASA or Charlson score in a retrospective manner. Although an assignment of the Charlson score has little bias, multiple studies have determined that the ASA score has low inter-observer reliability. The design through the use of a single anesthesiologist purposefully eliminated this variability for patient ASA assignments. However, the anesthesiologist who assigned these scores may simply assign scores which correlate more readily with mortality. A study with a larger group of anesthesiologists assigning both ASA and Charlson scores would eliminate this inherent bias. Additionally, all patients were assumed to be undergoing surgery when they were assigned ASA and Charlson scores. Since the anesthesiologist was not made aware of what treatment was given, this should not affect or cause bias to the scoring. On the other hand the surgeon would potentially select healthier patients on which to perform surgery. This may have had an effect on the differences seen in the survival curves for each of the study populations; however, our analysis revealed slightly worse Charlson Scores for the patients who had received surgery.
This study has definitively illustrated that there is a great deal of agreement between the Charlson Comorbidity Index score and the ASA score. This reflects that anesthesiologists subjectively consider the same elements of the patient's medical history when assigning ASA scores as the Charlson system objectively uses. This data may prove valuable for future studies as either of these pieces of data may be available in database reviews such as those of large insurance databases. As these resources become more available, tools such as comorbidity stratifying systems will be necessary for data analysis. They will potentially allow physicians and epidemiologists to make improved data comparisons. As our ability to mitigate tremendous public health concerns such as cancer and heart disease improves, we find an ever increasing osteoporotic population. Perhaps, our next frontier of healthcare will be identifying these more chronic and often thought benign diseases such as osteoporosis and attempting to improve upon patient quality of life and potential geriatric patient survival.
Disclosures
The authors declare no relevant financial disclosures.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
References
In this issue




{kind=link}
{kind=link}