


Abstract
Background Spinal injuries following an air crash can be fatal, and recognizing the patients who need immediate attention and early management could save those patients from ending up with lifelong disabilities and other consequences. However, taking appropriate actions in a pandemic situation presents additional challenges. We present our report of air crash victims with spinal injuries, along with their patterns, morphology, management, and outcomes during the COVID-19 pandemic.
Methods An analysis was performed on the spinal injuries of victims of the Boeing 737 crash landing at the Karipur Airport (Calicut International Airport, Kerala, India) who were treated at a tertiary care referral hospital in August 2020. Details of the initial triage, patterns of injury, morphologies, mechanisms, management principles, and outcomes at 9 months postinjury were recorded and analyzed.
Results Of the 47 patients received at our center, 44 survivors were triaged and 13 patients (29.5%) were identified to have spinal injuries of varying severities. The majority of the injuries were chance fractures at the lumbar level, followed by burst and compression fractures. A total of 6 patients underwent surgery, following all COVID-19 guidelines based on priority. All survivors had positive outcomes with our management. No complications such as secondary infections, worsening of neurological deficits, or implant failures were recorded.
Conclusion A high incidence of spinal injuries is seen in air crash victims. Early prioritized surgical management in selected patients provides excellent outcomes. Disaster management during a pandemic situation is a difficult task, where proper planning and execution is necessary to provide optimal results.
Introduction
In a disaster situation, quick assessment of the injuries, along with appropriate prehospital triage and safe transport to tertiary care centers, influence the final outcome of the victims’ condition. Fortunately, across the world, air crash disasters are rare compared with motor vehicle accidents. However, the rarity of air crash disasters means that the literature is sparse concerning spinal injuries in the context of air crashes. Spinal injuries, which are most frequently due to falling or motor vehicle accidents, may be fatal, and survivors may end up with lifelong disabilities and impairments of varying degrees.1 The COVID-19 pandemic is nothing less than a disaster in itself, and managing orthopedic and spine trauma has been a challenge for all surgeons during this period. The question of whether to follow textbook indications, follow the latest organization guidelines, or go with our “gut” feelings in deciding whether to operate or conserve is a dilemma. The risks involved in potential exposure to COVID-19 and the complications caused by anesthesia and surgery if the patient is positive for COVID-19 only makes the dilemma more difficult.
An amalgamation of disasters in the form of an air crash during a pandemic situation is what we witnessed in August 2020. The Air India Express 1344 Boeing 737 aircraft from Dubai (United Arab Emirates) to Calicut (Kerala, India) crashed at the Karipur International Airport on the evening of 7 August 2020. The aircraft was carrying 184 passengers, 4 cabin crew members, and 2 pilots.2 While landing, it failed to stop before the end of the tabletop runway and plunged 9 to 10.5 m (30–35 ft) into a gorge, splitting the fuselage into 2 sections upon impact3 (Figure 1). This aircraft was run as a part of the Vande Bharat Mission, which helped repatriate Indian citizens from different parts of the world, as most routine international travel was suspended due to the COVID-19 pandemic. Such incidents during the pandemic could become challenging, not only to the rescue workers at the site of accident, but also to those doing triage at the emergency facilities.

Scene at the site of the accident showing the crashed aircraft split into pieces.
In this study, we investigate the difficulties encountered in identification of, communication with, and management of these patients in full personal protective equipment (PPE) kits during the COVID-19 era. We also assess the patterns of spinal injuries, their morphology, and their management. In addition, we report the clinical and radiological outcomes at the 9-month follow-up point in these patients.
MATERIALS AND METHODS
A detailed analysis was performed on the spinal injuries of all victims of the Boeing 737 crash landing at the Karipur Airport who were treated at a single center tertiary care referral hospital in August 2020. Preliminary data about patient demographics and seat details during the flight were recorded. The method of the initial triaging system in the emergency setting, the level of spinal injury, the fracture classification (AO Spine classification of injuries), and the type of treatment were documented. Clinical and radiological outcomes at 9 months postinjury for all of the survivors treated at our center were recorded and analyzed. Victims and flight crew members who were treated at other hospitals are omitted from this report.
Initial Response
Mobile intensive care units and ambulances with medical teams in full PPE were immediately sent for rescue at the site of the accident, which was around 2 miles from the airport and 20 miles from the hospital. Patients in the emergency department were transferred to wards during the extrication time to provide space for receiving patients of the mass casualty. More than 75 doctors and nurses from various specialties arrived at the emergency department, donned PPE, divided into multiple teams, and immediately started to triage the 44 patients we received from the site. Difficulties were encountered in maintaining social distancing, identifying each other, checking patients’ identification, and coordinating for further investigations; these were noted in the chaotic environment. However, all patients were triaged per the Advanced Trauma Life Support protocol (Table 1). A total of 3 patients were dead upon arrival, including the pilot and copilot of the aircraft. A total of 7 patients who were hemodynamically unstable were shifted to the intensive care unit immediately and stabilized. The rest of the patients under different triage categories proceeded to imaging investigations after a thorough primary survey and initial aid based on priority. COVID-19 testing was done for all of the patients using the TrueNat COVID-19 chip-based real-time duplex polymerase chain reaction test, as this system yielded quick results. A total of 2 patients were reported to be positive based on the results.
Triage workup of all injured patients showing number of patients in each category and the list of injuries.
RESULTS
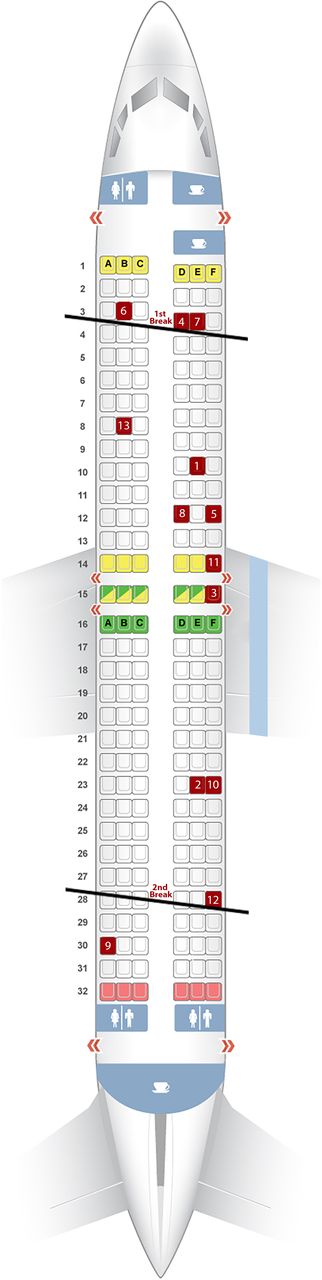
Aboard the Boeing 737 flight (Air India Express 1344) that crash landed at the airport on 7 August 2020, there were reportedly 190 passengers, including the crew. The crash ended up killing 19 passengers and both pilots. There were 4 cabin crew members and 165 passengers who survived. More than 100 of them were injured and taken to multiple hospitals and major tertiary care centers around the vicinity of the site of accident. Our center received 47 patients, including both of the pilots who were brought dead. Of the 44 survivors, 13 patients (29.5%), including 4 women and 9 men, were identified to have spinal injuries of varying severity (Table 2). In our case series, almost all of the patients were wearing a seat belt at the time of the accident, and their seat layout is shown in Figure 2.
Table showing management of all patients with spinal injuries, length of stay in the hospital, neurological improvement, and present functional status.

Seat layout of the flight showing the sections of the aircraft (marked in black lines as first and second break) and seat numbers of passengers who sustained spinal injuries (marked in red, patient ID as given in Table 1).

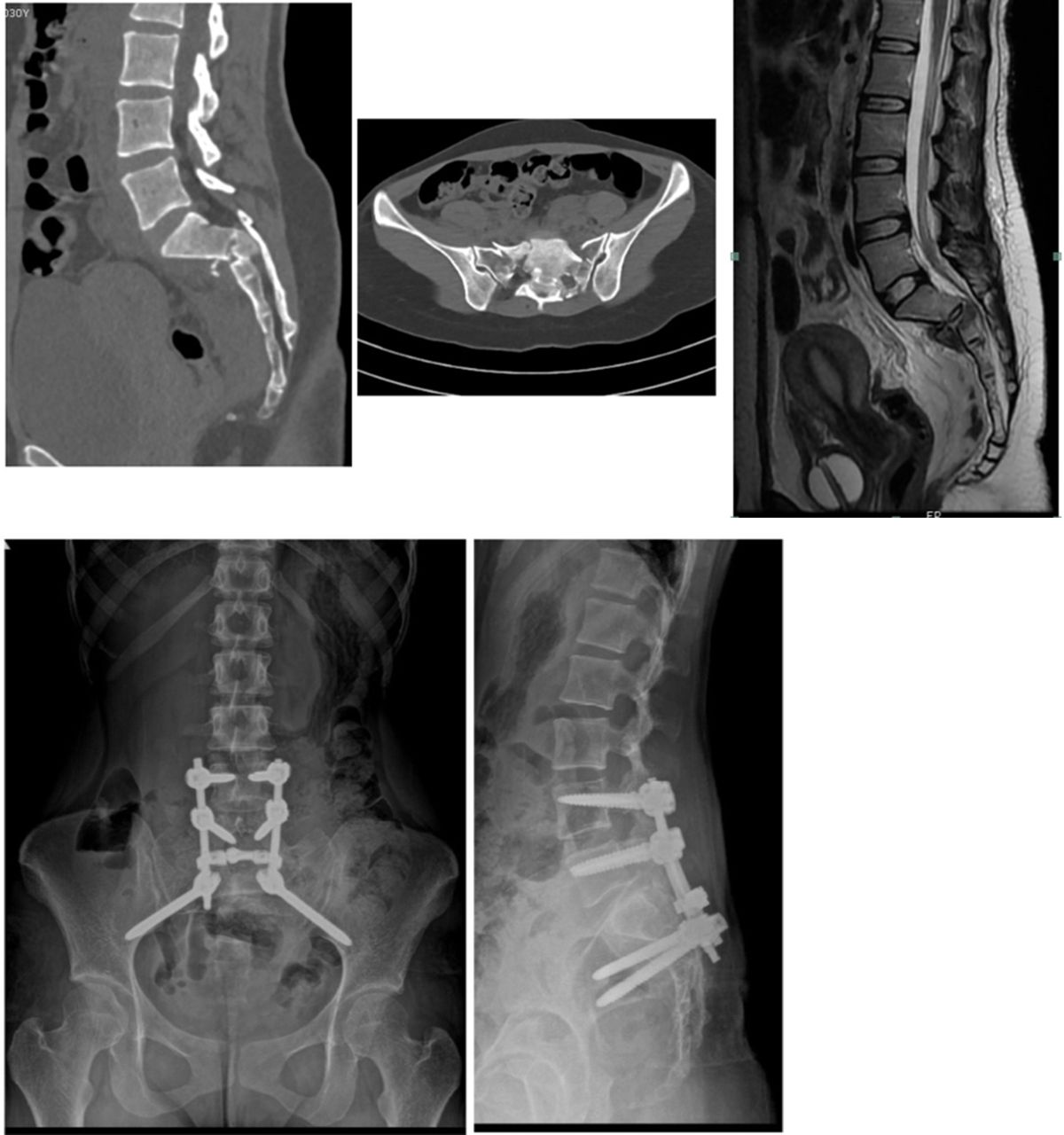
A 26-year-old woman sustained an uncommon injury (patient ID No. 2) and presented with American Spinal Injury Association (ASIA) grade B injury including bowel and bladder deficits. Computed tomography image/magnetic resonance imaging showed “H”-shaped fracture of the sacrum with sacropelvic dissociation. She underwent spinopelvic fixation with decompression of S2 foramina. She started weight-bearing mobilization at as early as 4 weeks and recovered completely to ASIA grade E, including full recovery of bowel and bladder control.

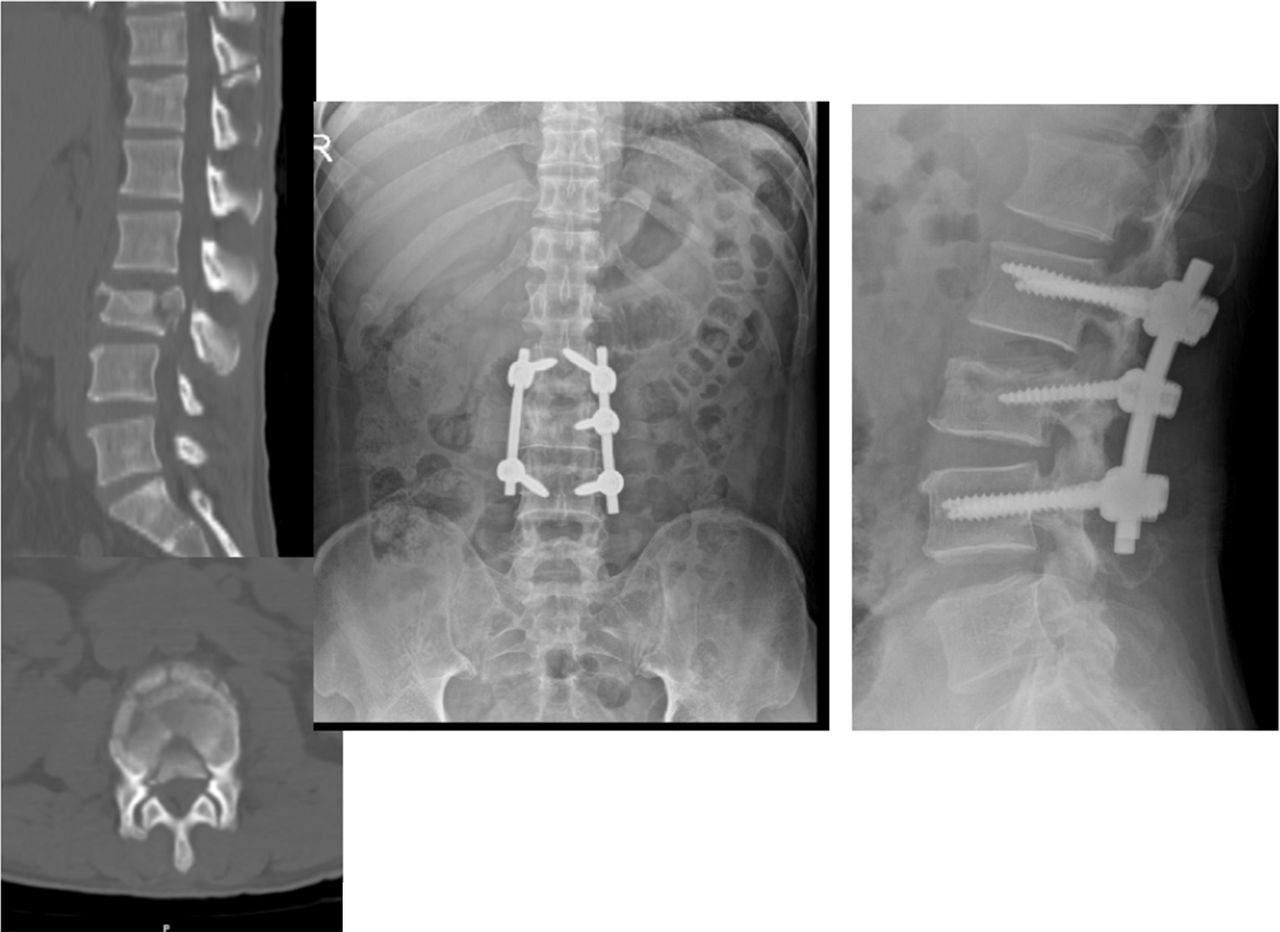
Case illustration of surgically managed patient (patient ID No. 5): 52-year-old man with L3 burst fracture, American Spinal Injury Association grade C injury. Short segment fixation with intermediate screw was performed with decompression.

Case illustration of conservatively managed patient (patient ID No. 9 in Table 1): 24-year-old woman with multilevel dorsal level compression fractures with injuries of spinous processes, American Spinal Injury Association grade E.
A common pattern of injury was found to be chance fractures at the lumbar levels (L2:2, L3:1) followed by burst fractures (L5:1, L3:2) and compression fractures, predominantly in the thoracic spine. A total of 6 patients with compression fractures and 1 patient with a burst fracture, all with intact neurological status, were managed conservatively. Surgical management was planned in 7 patients, and priority was given to patients based on their neurological status. As the patients had international travel, as per guidelines, all surgeries were planned in COVID-19–designated ORs, irrespective of their COVID-19 status. Performing these surgeries in a negative pressure operating room and wearing multiple layers of clothing (full PPE, lead aprons, and surgical gowns) and face shields was draining, and it was highly stressful to all of the staff involved. Multiple orthopedic and spine surgeries were planned in the operating room over the next 3 days, and a total of 6 patients underwent spine surgery during that time. One patient with a D3 chance fracture with a American Spinal Injury Association (ASIA) grade E impairment refused surgery and was discharged home. One patient tested positive for COVID-19, but he was asymptomatic.
Only 2 patients sustained multilevel noncontiguous injuries in our cohort, including one patient with a sacral injury and upper thoracic injury and a second patient with a lumbar fracture associated with a lower cervical injury. Patients were classified on the basis of the AO spine classification system4 into 5 type A injuries, 6 type B injuries, and 1 type C injury.
All patients were managed conservatively, and 5 of the 6 were functionally independent at the latest follow-up and showed significant neurological improvement (Table 3). No complications such as secondary infections, worsening of neurological deficits, or implant failures were recorded in any of the 13 patients. A 50-year-old man with an L2 chance fracture with complete paraplegia (ASIA grade A) showed significant recovery to ASIA grade D status and is functioning independently. A 31-year-old man with a D3 chance fracture who refused surgery was also doing well on follow-up and was functioning independently but had upper back pain while walking.
Master chart of patients showing patient morphology, mode of injury, associated injuries, and COVID-19 status on admission to the hospital.
The patient who had the longest hospital stay (75 days) was a 36-year-old man with multiple injuries (facial injuries, open fractures of the lower limbs and humerus, talar bone loss) and burn injuries over the back at the site of the lumbar burst fracture (L3 level). This patient had to undergo multiple operations and revision spinal debridement surgeries before plastic surgeons could intervene and provide a flap cover. At the 9-month follow-up, the patient had normal neurological status with implants in situ and started non–weight-bearing mobilization.
DISCUSSION
Fortunately, aircraft accidents are rare worldwide when compared with high-velocity road traffic accidents and trauma caused by falling. Baker et al5 showed that aviation-related injuries result in approximately 1000 hospitalizations each year in the United States, with an in-hospital mortality rate of 2%. Spinal injury incidence, mechanisms, and management are well described in the literature regarding the common modes of injury,6 but the evidence is limited with respect to spinal injuries secondary to aircraft accidents. The literature suggests predominant lower limb injuries in these patients.5,7 Older literature8–10 regarding aircraft accident management may suggest a higher rate of incidence of missed fractures due to the lack of availability of modern imaging, like CT images and MRI. There also is a discrepancy in the incidence of spinal injuries, as diagnosing spinal injuries in fatal accidents11–14 is often excluded. There have been many scenarios where air crashes have led to high mortality rates, and the incidence of spinal injuries therefore cannot be analyzed.
Although MRI was available at the center, a CT image was considered the investigation of choice to save time, establish a diagnosis, and prioritize the patients who needed surgery first. Also, following COVID-19 guidelines for sanitation was more difficult to manage with MRI than with the CT image. When there was sufficient time available during the waiting period for surgery, an MRI was also performed. Lack of utilization of MRI due to timing, resources, and sanitization protocol may be responsible for the underestimation of posterior osteoligamentous tension band injuries and the discrepancy in classification for some patients.
Analysis of the 2011 Iran Air Boeing 727 crash by Mirzatolooei et al15 showed 78 people were killed and 27 people survived out of 105 passengers. A total of 15 out of the 27 patients had fractures to their spine, predominantly at the thoracolumbar junction (7 burst fractures, 5 compression fractures, and 3 fracture dislocations). A relatively lower number of deaths in our case series is probably for 2 reasons. First, the brunt of the injuries were suffered by the pilots, as the nose of the flight hit the ground from the tabletop runway, which helped reduce the speed during deceleration. Also, there was no fire accident following the crash in this case, which saved lives of most of the passengers. This was unlike many other air crash incidents, including a strikingly similar air crash on a tabletop runway in Mangalore (India) in 2010, which had only 8 survivors and 158 deaths; most of the bodies were charred beyond recognition).16 Lee et al17 reported only 3 cases of spine fracture caused by a commercial airplane accident in 2013, with 307 passengers aboard. Each of the 3 patients suffered a compression fracture at the midthoracic and thoracolumbar junction.
As observed in our patients, the majority of the severe spinal injuries presented with varying degrees of neurological deficits. Whether the injuries were primary in nature at the time of incident or secondary as the patients were pulled out of the jammed seats and shifted to hospital in available vehicles other than ambulances without spine board is something to ponder upon. Analyzing the severity of injury with the seating position, it was found that majority of patients with severe injuries were seated in the front third of the plane. Though conclusions cannot be made with this evidence, suggestions to improve the energy absorbing capacity of the seats in the front half of the plane could help in preventing severe injuries in future air crash events. Attempts by flight engineers to design better seat belts, similar to the crew seat supports with 4-point contact rather than the present 2-point contact seat belts would be helpful in prevention of flexion distraction injuries. Trials to lower the gravitational force in vertical deceleration phase of accident could be game changing in the future.
As described earlier, this study distinguishes itself due to the timing of the air crash, which was during the peak of the COVID-19 pandemic in India. COVID-19, just by itself, warrants consideration as a “mass casualty” incident.18 Disaster management during a pandemic is not a simple task, and following the principles of the “disaster cycle” is important. Mitigation of an air crash is not possible, but adequate preparedness in terms of preventing a shortage of manpower and equipment (eg, PPE) and infrastructure organization take precedence. Disaster planning takes exercise, practice, and revision.19 Like in most institutions across the world, the pandemic was not anticipated to this extent, and proper planning to escalate the demand of manpower and PPE was necessary at the time of the air crash, which was excellently done.
As far as an air crash disaster management plan is concerned, a mock disaster drill was performed at the same site (Calicut International Airport) in 2012. Medical personnel from our institution, with the specified role of disaster management team, were involved in performing the mock exercise. The mock drill definitely helped those who were present in the emergency department on the day of the air crash to triage and manage effectively. None of the staff members involved in managing air crash patients from the emergency ward, and none of the surgeons and staff members involved in their surgeries, became positive for COVID-19. These outcomes speak for themselves about how following standard guidelines is in everyone’s best interest.
CONCLUSION
Early prioritized surgical management in selected patients provides excellent outcomes in spinal injuries caused by air crashes. Disaster management during a pandemic situation is a difficult task, and proper planning and execution are necessary to provide optimal results. This study emphasizes the need for mock disaster management drills for better planning and preparation for such untoward events. Analysis of the results may help to enhance air travel safety if measures are taken to prevent such injuries in future incidents.
Acknowledgments
The authors would like to acknowledge all of the medical and nonmedical staff members of our institute involved in managing air crash victims. A special acknowledgment goes to all doctors of the departments of emergency medicine, anesthesia, and orthopedics.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.