


Abstract
Proximal junctional kyphosis (PJK) is a common complication following long-segment thoracolumbar fusions for patients with adult spinal deformities. PJK is described as a progressive kyphosis at the upper instrumented vertebra or 1 or 2 segments adjacent to the instrumented vertebra. This condition can lead to proximal junction failure, which results in vertebral body fractures, screw pullouts, and neurological deficits. Revision surgery is necessary to address symptomatic PJK. Research efforts have been dedicated to elucidating risk factors and prevention strategies. It has been postulated that minimally invasive surgery (MIS) techniques may help prevent PJK because these techniques aim to preserve the soft tissue integrity at the top of the construct and maintain posterior element support. In this article, the authors define PJK, describe MIS strategies to prevent PJK, and compare PJK rates after MIS with PJK rates after open approaches for long-segment thoracolumbar fusion.
INTRODUCTION
Proximal junctional kyphosis (PJK) is a common complication of long-segment thoracolumbar instrumented fusions after surgery to correct adult spinal deformity (ASD). PJK is described as a kyphotic deformity developing at or proximal to the upper instrumented vertebra (UIV). Many cases of PJK are diagnosed on the basis of radiographic findings only, and patients who are asymptomatic can be managed conservatively. However, certain cases progress to proximal junctional failure (PJF), which results in vertebral body fracture or subluxation, screw pullout, or neurological deficit.1 Patients with PJK or PJF often require additional operations to correct or stabilize the deformity, resulting in patient morbidity and increased cost of care.2–4 Thus, preventing PJK is crucial to optimizing patient outcomes and preventing revision surgeries.5
Techniques that prevent disruption to the posterior column elements and musculature may help prevent PJK from developing in patients undergoing long-segment thoracolumbar instrumented fusion. Augmenting the posterior ligamentous complex with tension cables during open pedicle screw placement for ASD correction may reduce the number of PJK cases requiring revision surgery.6,7 Minimally invasive surgery (MIS) techniques are thought to potentially prevent PJK because they help maintain the integrity of the spinal soft tissue.8 Herein, we define PJK, describe minimally invasive strategies to prevent PJK, and compare PJK rates after MIS and open approaches for long-segment thoracolumbar fusion.
DEFINING PJK
There is no exact consensus on the definition of PJK in the literature,9 but the most widely accepted description is a sagittal Cobb angle of 10° or greater and a proximal junction angle of at least 10° higher than the preoperative measurement, which is the Cobb angle between the inferior endplate of the UIV and the superior endplate of the vertebral body at UIV +2.2,10–12 This definition is the most reliable method to diagnose PJK and has been consistently used in the literature.13 The incidence of PJK after spinal fusion is relatively high but also widely varies. Glattes et al was one of the first to investigate PJK and reported the prevalence to be approximately one-fourth of patients undergoing long-segment thoracolumbar fusion.10 A meta-analysis of 14 studies with 2215 total patients reported rates of PJK following spinal fusion ranging from 17% to 62%.14 A systematic review examined 53 studies involving patients undergoing long-segment fusions for ASD and reported rates of PJK and PJF ranging from 5% to 46%.15 A study that directly evaluated PJK in 81 patients with ASD found that 26% developed PJK by the 2-year follow-up after undergoing an open long-segment fusion.10 Thus, the incidence of PJK is high, and preventing PJK is a topic of interest in the spinal surgery community.
The variability in reported PJK rates in the literature could be due to the fact that patients may be asymptomatic at initial presentation. A study of 157 consecutive patients undergoing fusion for scoliosis found that postoperative disability and pain scores were not significantly different between patients who did or did not develop PJK.16 Even though patients may be initially asymptomatic, their kyphosis may progress over time and become symptomatic. To investigate this hypothesis, Park et al retrospectively analyzed 73 ASD patients with an average follow-up of 92.4 months.17 They found that patients with PJK progressed from a proximal junctional angle of 6.5° to 21.2° over the follow-up period, with worsening clinical outcome scores. PJK progresses over time, and the detection of PJK in this patient population could, therefore, depend on the point between the surgery and the last follow-up at which the patient is evaluated.
Another reason for prevalence variability could be that PJK diagnosis is made on the basis of radiographic findings, with inherent measurement errors and bias in calculating the PJK angle. A study of 460 radiographs evaluating PJK in 98 patients who underwent prior fusion for adolescent idiopathic scoliosis found that inter- and intrarater reliability were relatively low and that PJK was often not diagnosable on subsequent films.18 The authors hypothesized that the inconsistency was due to differences in methodology and that the angles could only be determined on 31% to 49% of postoperative films.
PJK can progress to PJF, which is described as the pathological development of bony fracture, subluxation between the UIV and UIV +1, neurological deficits, or pseudarthrosis.7 These sequelae often result in revision surgery that significantly adds to patient morbidity. The most common mode of PJF is fracture. Hostin et al evaluated the incidence and mode of PJF in 1218 consecutive patients with ASD and found that 5.6% developed acute postoperative PJF.19 Fracture was the cause of PJF in 47% of these cases, whereas soft tissue issues were the cause of PJF in 44%.
Because revision surgeries are associated with morbidity and additional financial costs,4 multiple strategies have been developed to prevent PJK-associated complications. One strategy is to bolster the posterior ligamentous complex. Safaee et al conducted a retrospective review evaluating whether ligament augmentation during open posterior spinal fusion for ASD had any effect on preventing PJF and subsequent reoperations.6 They compared 242 patients undergoing posterior spinal fusion with ligamentous augmentation with 77 patients from a historical cohort without ligamentous augmentation and found that the revision rate for PJF was significantly lower in the ligamentous augmentation group (3.3%) than in the nonaugmentation group (15.6%). Another study by the same group showed that the reduction in reoperations was cost-effective as well.20 With MIS strategies, the concept is to maintain the integrity of the posterior ligamentous complex rather than reinforce it after an open approach.
PJK Risk Factors
Multiple studies have described PJK risk factors to identify high-risk patients. Liu et al conducted a meta-analysis of 2215 patients and showed that risk factors included patient age older than 55 years, fusion to S1, preoperative thoracic kyphosis Cobb angle greater than 40°, low bone mineral density, and a pre- to postoperative sagittal vertical axis change of greater than 5 cm.14 These risk factors have been verified by other literature reports.21,22 Another study of 206 patients with a 2-year follow-up showed that, among older patients, those with overcorrected postoperative lumbar lordosis and larger sagittal balance corrections were more likely to develop PJK that required additional surgery.12 Lafage et al created a scoring system for PJK risk stratification based on risk factors described in the literature.23 They examined PJK in 417 ASD patients undergoing fusion with at least a 2-year follow-up. They reported an overall PJK rate of 43%. Age older than 55 years, fusion to the pelvis, UIV in the lower thoracic spine, UIV in the upper thoracic spine, and a greater than 10° surgical reduction in thoracic kyphosis to lumbar lordosis increase are used as variables in their scoring system, with each variable being weighted evenly. The scale is graded, and patients with more risk factors are more likely to develop PJK.
Case Illustration
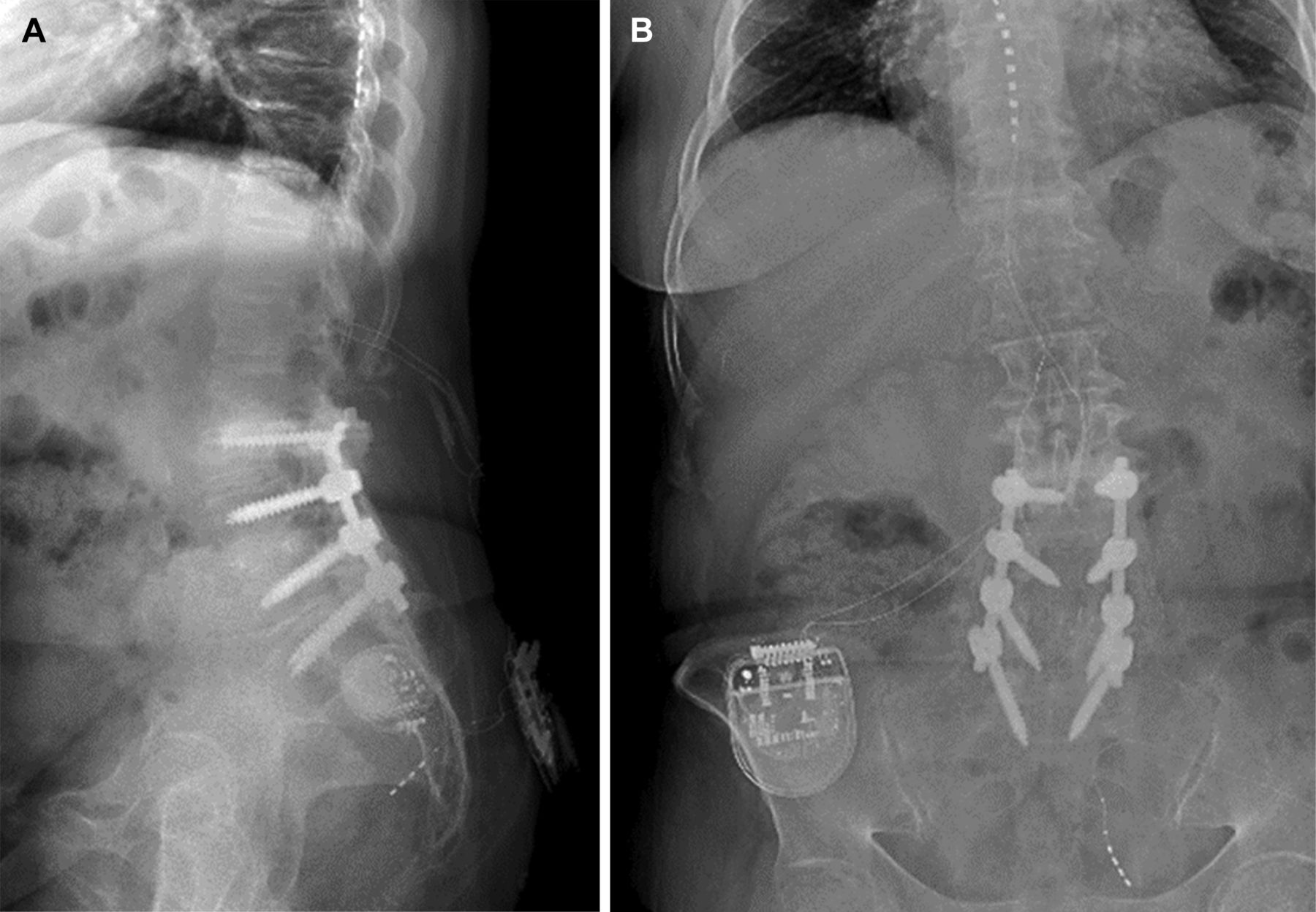
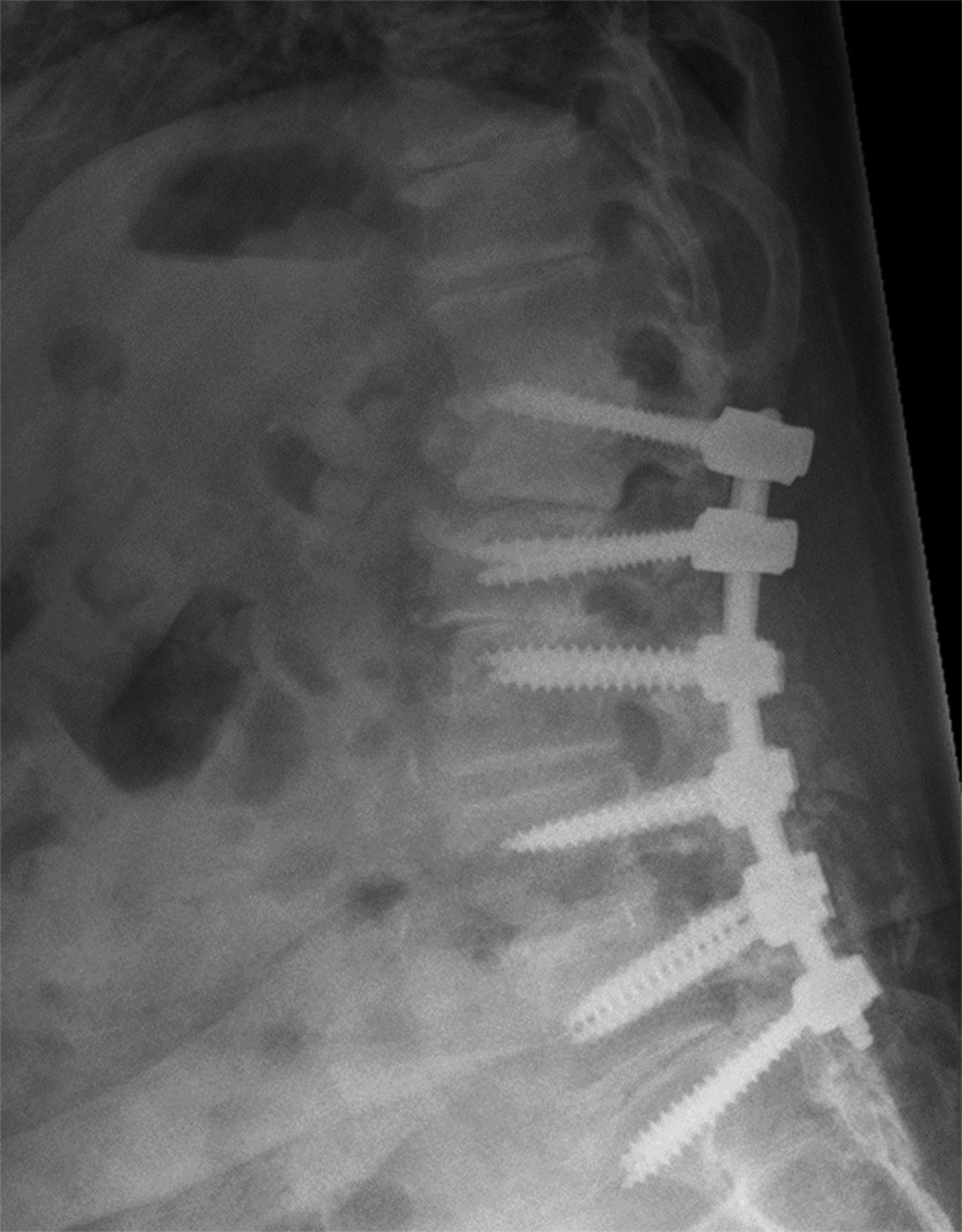
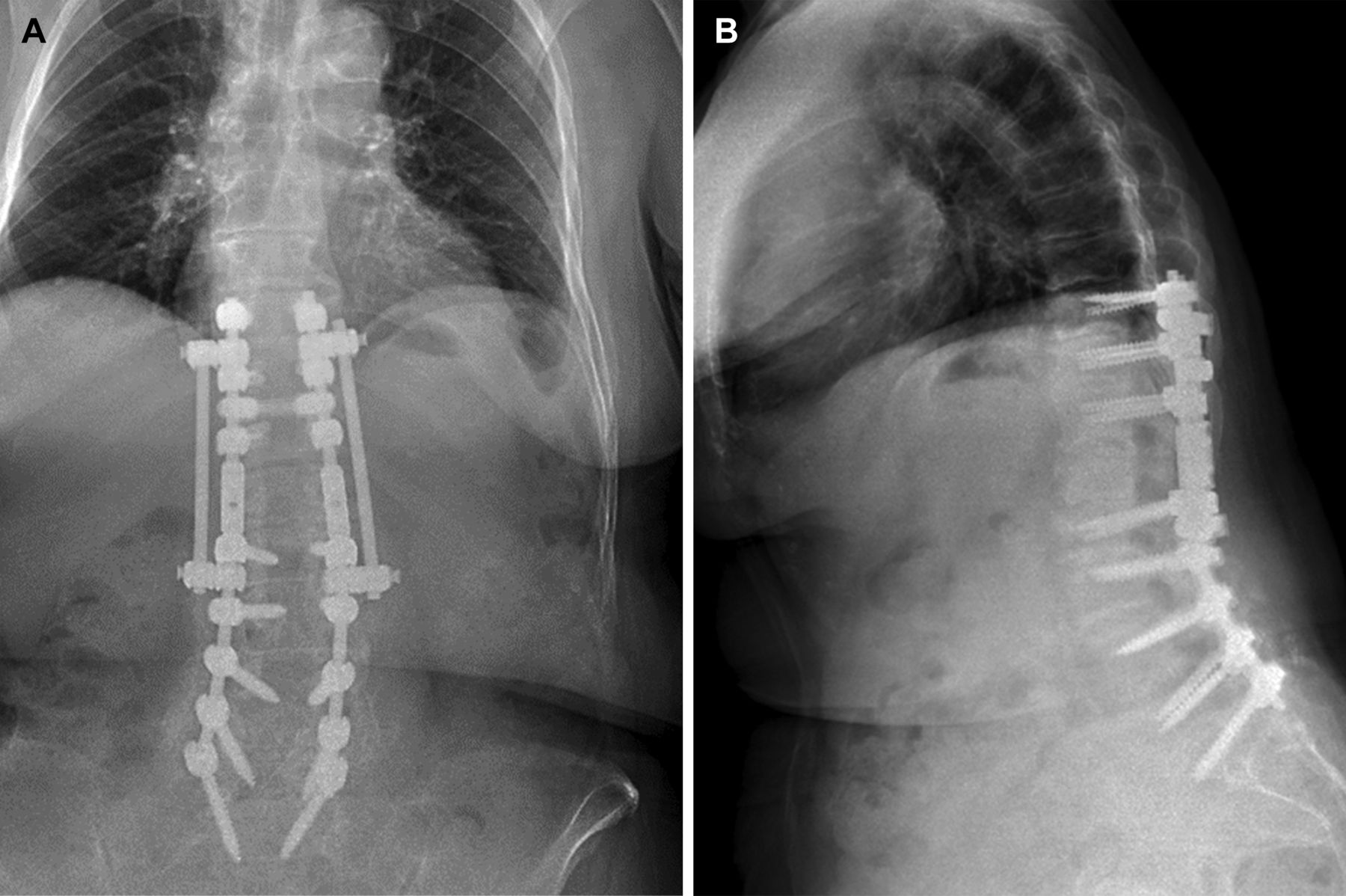
A woman aged in her early 70s with prior L3-S1 posterolateral fusion and spinal cord stimulator presented with worsening low back pain and lumbar radiculopathy (Figure 1). She underwent an extension of her fusion to L1 with L1-L2 laminectomies and removal of her spinal cord stimulator. She presented approximately 1 year later with bilateral lower extremity pain and weakness secondary to PJK (Figure 2). She underwent Smith-Peterson osteotomies at T12-L1, removal of L1 pedicle screws, T12-L2 laminectomies, and extension of the fusion to T10 with accessory rod-connector placement from T10 to L2. This surgery corrected the patient’s PJK, and her symptoms improved postoperatively (Figure 3).

Preoperative lateral (A) and anteroposterior (B) standing 3-feet plain scoliosis films show the patient’s prior fusion and spinal cord stimulator. Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.

Lateral standing 3-feet plain scoliosis film shows the development of proximal junctional kyphosis. Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.

Postoperative anteroposterior (A) and lateral (B) standing 3-feet plain scoliosis films show correction of proximal junctional kyphosis at 3-mo follow-up. Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
MIS STRATEGIES FOR MINIMIZING PJK RISK
Posterior Tension Band Biomechanics
Part of the rationale for using MIS techniques to prevent PJK is that they theoretically help preserve the posterior tension band, which is one of the main resistances to flexion and kyphosis of the thoracolumbar spine. This hypothesis has been derived from previous biomechanical studies. A cadaveric study by Heuer et al24 of 8 lumbar segment specimens investigated stepwise reductions in functional parts of the spine and found that removal of the posterior ligaments resulted in increased specimen flexion when bending force was applied. Widmer et al25 studied 50 lumbar segments and determined that the ligamentum flavum specifically was a major contributor to flexion range of motion, while the interspinous and supraspinous ligaments were minor contributors. A study by Wu et al26 of a finite element model constructed from a thoracolumbar (T12-L1) computed tomography image found that removing the supraspinous ligament, interspinous ligament, and ligamentum flavum significantly increased the range of motion and instantaneous axes of rotation during flexion, implying that the posterior ligaments contribute significantly to stability. Spine biomechanical principles are the basis for why MIS techniques may prevent PJK—they maintain the integrity of the ligaments that resist excessive flexion.
Percutaneous Pedicle Screw Placement
Tissue preservation associated with percutaneous pedicle screw placement is 1 reason MIS may help prevent PJK. These benefits are thought to be derived from less tissue and muscle disruption associated with an MIS percutaneous approach. A study comparing multifidus muscle atrophy and trunk extension muscle strength in patients undergoing percutaneous (n = 8) and open (n = 11) pedicle screw placement found that the percutaneous group had no significant postoperative muscle atrophy compared with preoperative imaging, whereas the open group had significant postoperative muscle atrophy and weakness.27 MIS preservation of the paraspinal musculature and posterior elements is supported in the literature.28–30 Maintaining normal tissue and muscle integrity is thought to biomechanically support the top of the construct and prevent the thoracic spine from leaning forward and creating a kyphotic deformity. This has been substantiated in experimental models, as Cammarata et al developed a biomechanical simulation that concluded posterior ligament resection was one of the major factors leading to a PJK angle.31 Clinical comparisons of PJK rates after percutaneous MIS vs open pedicle screw placement are discussed in the “MIS vs Open Approaches” section.
Vertebral Body Cement Augmentation
One MIS strategy for preventing PJK is to augment the vertebral body above the construct. This strategy was hypothesized in a biomechanical cadaveric study that evaluated how cement augmentation affected axial loading on the proximal junction.32 This study used 18 cadaveric specimens to investigate the effect of prophylactic vertebroplasty at UIV and UIV +1 on preventing vertebral compression fractures at the proximal junction of an instrumented spine.33 Pedicle screws and connecting rods were placed from L5 to T10 in all specimens, which were divided into the following groups: control, vertebroplasties at the UIV, and vertebroplasties at UIV and UIV +1. Each spine was axially loaded until failure, which was defined as the inflection point in the force vs deformation curve. Specimens in the group with vertebroplasties at UIV and UIV +1 were the least likely to fracture after axial loading. The authors concluded that prophylactic vertebroplasties may prevent PJK deformities. This finding was substantiated in a recent systematic review of biomechanical studies, which found that vertebroplasty resulted in a lower incidence of vertebral compression fractures at the top of the construct in axial loading experiments.32
In the clinical setting, the results appear to be more mixed.34,35 In an assessment of the effectiveness of vertebroplasties, a study of 41 patients who underwent long-segment posterior spinal fusion and prophylactic 2-level vertebroplasty at the UIV and suprajacent level found that only 8% of patients developed PJK and 5% developed PJF; these rates were much lower than reported elsewhere.36 Ghobrial et al aimed to evaluate the effect of prophylactic vertebroplasty on the incidence of PJK.37 They examined 85 patients undergoing long-segment (>5 levels) fusions to compare the rates of PJK in patients with and without vertebral body cement augmentation and found that PJK was significantly lower in the treatment group than in the control group. Han et al also investigated prophylactic vertebroplasty at the UIV and UIV +1 in a retrospective cohort study and found no difference in the incidence of PJK between the 2 groups, although patients who underwent vertebroplasty were less likely to experience disease progression over time.38 Another prospective cohort study of 39 ASD patients undergoing spinal fusion showed prophylactic vertebroplasty had no effect on the incidence of PJK at 5-year follow-up.39 A recent systematic review of the literature found inconsistent and conflicting evidence for the efficacy of prophylactic vertebroplasty.34 More research is required before prophylactic vertebroplasty or kyphoplasty can become the standard of care.
MIS VS OPEN APPROACHES
MIS techniques may prevent PJK because they require minimal disruption to the facet joints, paraspinal musculature, and posterior ligamentous complex.8 This hypothesis has not been proven, and the results of studies evaluating PJK rates after MIS are mixed. Mummaneni et al conducted a multicenter propensity-matched study of 53 total patients undergoing either MIS pedicle screw placement or a hybrid approach that involved open pedicle screw placement.40 The mean duration of follow-up in their study was 32.8 months. Although the overall rates of PJK were lower in the MIS group than the open group (31.3% vs 52.9%), the statistically significant difference was eliminated when accounting for the number of levels instrumented (48.1% vs 53.8%). Study limitations included a small sample size and the retrospective design of the study. More recent data have shown that PJK may be reduced in patients undergoing an MIS approach to posterior pedicle screw placement. Chan et al conducted a larger retrospective study comparing 197 total ASD fusion patients undergoing either open pedicle screw placement or MIS techniques and showed that patients undergoing an MIS approach were significantly less likely to develop PJK than those undergoing an open approach (6.5% vs 18.0%) at last follow-up (mean [SD], 39.0 months [13.3] vs 39.9 months [16.8]).41 This PJK rate of 6.5% is lower than the rates after open surgery described in the literature.10,14,15
The sustainability of this low PJK rate associated with MIS pedicle screw placement is unclear. Anand et al evaluated the rate of PJK in ASD patients who underwent MIS pedicle screw placement with long-term follow-up.42 The authors queried a prospective database of ASD patients, with 184 patients meeting their inclusion criteria. The mean follow-up was 85.2 months with a maximum duration of 158.9 months. Anand et al42 found that 10.8% of the patients developed PJK; of these patients, approximately one-half experienced progression to PJF and required revision surgery. The revision rates were low, but there was no direct comparison with an open surgery cohort. Mundis et al conducted a propensity-matched study comparing percutaneous vs open pedicle screw placement among ASD patients undergoing surgery and found no difference in PJK rates at 1-year follow-up.43 The propensity matching controlled for spinopelvic parameters and the number of levels fused as well as demographic characteristics. PJK cases were divided into mild (10° change) and severe (20° change) cases. There was no difference between the MIS and open groups with respect to the percentage of mild (19.5% vs 28.6%) or severe (3.9% vs 2.6%) cases of PJK. The limitations of the study were its retrospective nature and the follow-up time.
Some surgeons have attempted to combine open and MIS approaches to prevent PJK. Park et al described a technique in which the majority of the exposure was performed using an open technique, but the musculature and posterior elements of the uppermost levels were left intact.44 A standard subperiosteal exposure was performed, but the top 3 instrumented levels were left with the muscle and posterior ligamentous complex intact. The rationale for this technique is that it may help prevent PJK. This approach also has the benefit of obtaining proper arthrodesis or wide decompression of neural elements, and it may be effective in preventing PJK. However, to date, no studies have directly examined its efficacy, and future research is required.
CONCLUSIONS
PJK is a phenomenon that often develops after long-segment thoracolumbar instrumented fusions and is likely to be caused by multiple factors, including advanced aged, poor bone quality, and correction of spinopelvic parameters. MIS approaches may help mitigate the development of PJK because they maintain soft tissue integrity. Literature comparing PJK rates in MIS and open cohorts are limited, and the results are mixed, which implies that MIS approaches are only 1 factor in preventing PJK. Appropriate patient selection is crucial to optimizing functional outcomes and minimizing revision surgeries after thoracolumbar instrumented fusion to correct ASD.
Acknowledgments
We thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Juan S. Uribe receives royalties from NuVasive Medical, Inc., consulting fees and royalties from SI-BONE, Inc., and consulting fees from Aclarion, Inc., Misonix, Inc., Viseon, Inc., and Mainstay Medical, Inc. The remaining authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.