


Abstract
Background Anterior cervical discectomy and fusion (ACDF) is a common procedure for neck arthritis, typically alleviating pain and improving function. Preoperative dehydration has been correlated with postoperative infection, acute renal failure, deep vein thrombosis, and increased hospital length of stay. However, some studies have suggested that preoperative dehydration has a minimal relationship with postoperative outcomes, specifically in arthroplasty and lumbar surgery candidates.
Methods Patients who underwent ACDF from 2015 to 2020 as part of the American College of Surgeons National Surgical Quality Improvement Program database were identified. We excluded patients who presented with acute trauma. Dehydration was determined using the accepted definition of preoperative blood urea nitrogen to creatinine ratio greater than 20. Lengths of stay and 30-day postoperative adverse events were compared between dehydrated and nondehydrated cohorts, adjusting for baseline features using standard multivariate regression.
Results We identified 14,932 patients, and 4206 (28.1%) of whom were preoperatively dehydrated. Dehydrated patients had significantly higher odds of wound, hematological, and pulmonary complications; Clavien-Dindo grade IV, delayed length of stay (>5 days); and a lower likelihood of being discharged home (P < 0.005), even after controlling for demographic features (eg, sex, age, body mass index, race, and ethnicity). Furthermore, linear regression suggested an overall half-day increased length of hospital stay for dehydrated patients (95% CI [0.36, 0.60], P < 0.001).
Conclusion Preoperative dehydration is common among ACDF surgery patients and appears to correlate with an increased risk of postoperative complications and prolonged length of hospital stay. Evaluation of a patient’s hydration status from standard preoperative laboratory metrics can be employed for risk stratification, patient counseling, and timing of ACDF surgeries.
Level of Evidence 3.
- ACDF
- preoperative
- dehydration
- cervical spine
- fusion
- discectomy
- NSQIP
- risk
- complications
- length of stay
- big data
INTRODUCTION
Cervical spine surgeries are increasing due to anterior cervical discectomy and fusion (ACDF) utilization, which improves function and relieves pain in neck arthritis patients.1 Multiple risk factors for cervical spine surgery have been studied, including anemia, medical comorbidities, and socioeconomic status.2,3 Studies have investigated preoperative dehydration in orthopedic patients, with some indicating an increased risk of complications and delayed hospital stay.4–6 The importance of fluid management is debated, and few universal recommendations exist for preoperative fluid management in orthopedic patients.7–9
The relationship between preoperative fluid management and postoperative complications in ACDF is unclear. To address this gap, our study uses the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database to investigate 30-day postoperative complications, hospital length of stay, and discharge for ACDF patients.10 We aimed to identify differences in postoperative complications and hypothesized that preoperative dehydration increases the risk of complications.
METHODS
We performed a retrospective analysis of the ACS NSQIP database.10 The ACS NSQIP is a multi-institution and multicenter database that collects more than 270 patient variables from >500 hospitals. Patient variables are extracted via trained clinical reviewers who match each patient with their respective Current Procedural Terminology code and record preoperative, intraoperative, 30-day postoperative, and discharge data. The database undergoes various levels of audits and quality checks.
We utilized Current Procedural Terminology codes to identify all adults who underwent ACDF from 2015 to 2020. We collected patient demographics, length of stay, discharge destination, and postoperative complications that occurred within 30 days of surgery. Various complications were grouped under their corresponding organ system. For example, occurrences of pneumonia, pulmonary embolism, unplanned intubation, ventilator >48 hours, and ventilator dependence were grouped under pulmonary complications. We calculated patient body mass index (BMI), Clavien-Dindo scores, and our preoperative modified comprehensive complication index risk assessment tool. Patients with a preoperative blood urea nitrogen/creatinine (BUN/Cr) ratio greater than 20 were considered dehydrated, based on prior studies.7,8,11,12
Statistical Analysis
After proper exclusion of incomplete and missing variables, the sample was divided into two cohorts based on hydration status as assessed by BUN/Cr ratio >20: those in the dehydrated group and those in the hydrated group. Next, SPSS suite (IBM Corp) was utilized to analyze the data. Finally, University of California Los Angeles’s Advanced Research Computing Statistical Methods and Data Analysis G*Power Statistics tool was used to perform power analysis. Confidence intervals were set at 95% with a P value of 0.05 being considered statistically significant.
Each group then underwent analysis to compare complication rates and means of various variables. Furthermore, multiple linear and logistic regression models were created to elucidate the connection between dehydration and various linear and categorical complications and variables. These regression models controlled for age, sex, ethnicity, race, and BMI.
Categorical results are reported as counts with column percentages. Continuous data are reported as means and SDs; SEs are given where appropriate. All data were initially analyzed to ensure a correct statistical assessment was chosen and that the variables met the requirements and assumptions for each statistical test. Comparison of normally distributed data was performed with independent sample t tests. For non-normally distributed data, the Wilcoxon rank-sum test was performed. Categorical variables were assessed with Fisher’s Exact Test or χ 2 with Kendall Tau. Both multiple linear and logistic regression models were analyzed to ensure all assumptions were met. Where appropriate, residuals were assessed for normal distribution, and no multicollinearity was observed. All variables in the multiple linear logistic regression model were first run separately to ensure that no artifact P values were present and that all effect sizes were reported honestly.
RESULTS
Patient Demographics
A total of 14,932 patients were identified who underwent ACDF between 2015 and 2020, a majority of ACDF procedures were elective (93.6%). The mean age was 56 years (SD 12), and the mean BMI was 30.62 (SD 6.53). Among all patients, 50.5% were men, 12.7% were Black, and 6.3% were Hispanic (Table 1).
Patient demographics, operative time, length of hospital stay, and probability of morbidity and mortality for the dehydrated and not dehydrated groups.
Patients with preoperative dehydration were more likely to be older (59.5 vs 54.7 years; P < 0.001), women (61.2% vs 45%; P < 0.001), and Hispanic (6.7% vs 6.2%; P < 0.001). Patients with preoperative dehydration also had a higher modified comprehensive complication index (1.95 vs 1.14) and more severe American Society of Anesthesiologists class (Table 2). The estimated probabilities of mortality and morbidity were 0.3% vs 0.18% and 2.60% vs 2.26%, respectively. Total operation time was 135 (SD 76) vs 130 (SD 71) minutes. Length of stay was 2.39 vs 1.83. There were no significant differences in BMI.
ASA scores, comorbidities, and MCCI for the dehydrated and not dehydrated groups.
Postoperative Complications
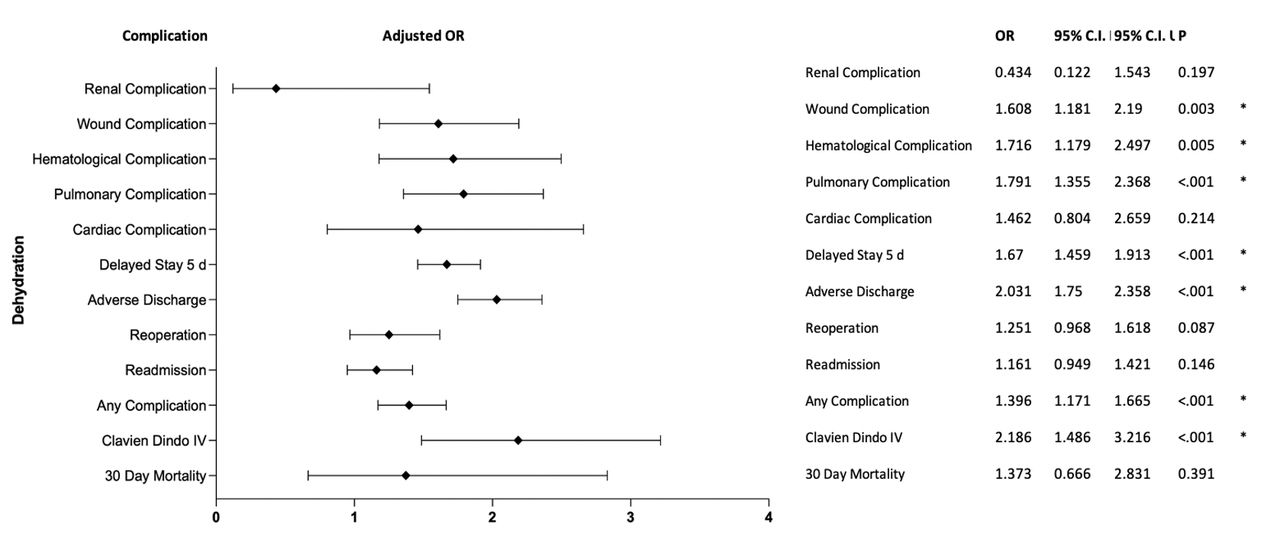
Preoperative dehydration was associated with a higher odds of any complication (OR = 1.40, 95% CI [1.17, 1.67], P < 0.001). Preoperative dehydration had a higher odds of wound complications (OR = 1.61, 95% CI [1.18, 2.19], P = 0.003), hematological complications (OR = 1.72, 95% CI [1.18, 2.50], P = 0.005), pulmonary complications (OR = 1.79, 95% CI [1.36, 2.37], P < 0.001), and Clavien-Dindo grade IV (OR = 2.19, 95% CI [1.49, 3.22], P < 0.001). However, preoperative dehydration did not increase the odds of 30-day mortality, cardiac complications, renal complications, reoperation, or readmission, as shown in Table 3, Figure 1, and Figure 2.
30-day complications, Clavien-Dindo grade IV, and mortality for the dehydrated and not dehydrated groups.

Plot displaying the odds ratios for postoperative complications when comparing dehydrated and not dehydrated patients. Age, sex, ethnicity, race, and body mass index were adjusted for.

Plot displaying bar graph representation of 30-day mortality, postoperative complications, modified comprehensive complication index 50+, and Clavien-Dindo grade IV when comparing dehydrated and not dehydrated patients.
Length of Stay and Discharge
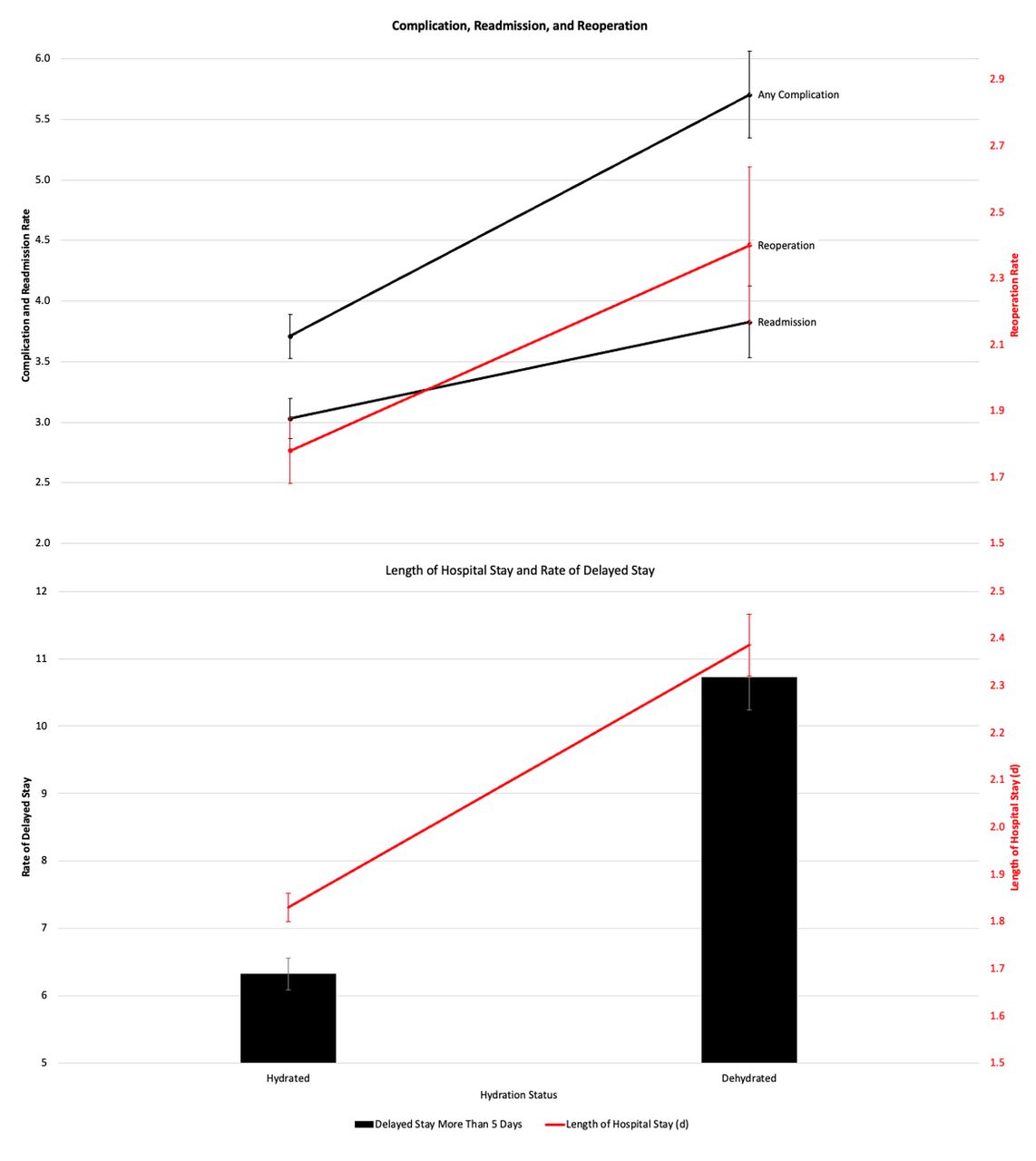
Patients with preoperative dehydration had a higher odds of delayed length of stay >5 days (OR = 1.67, 95% CI [1.46, 1.91], P < 0.001) and a lower likelihood of being discharged home (OR = 2.031, 95% CI [1.75, 2.36], P < 0.001), as shown in Table 4 and Figure 3.
Readmission, reoperation, discharge destination, and delayed hospital lengths of the stays ( >5, >7, >10, and >15 d) for the dehydrated and not dehydrated groups.

Plot displaying bar graph representation of complications, reoperation, readmission, and hospital length of stay when comparing dehydrated and not dehydrated patients.
DISCUSSION
Our study compared postoperative complications and hospital length of stay between dehydrated and nondehydrated ACDF patients. We hypothesized that dehydrated patients would experience more complications and longer hospital stays. Our results showed that dehydrated patients had higher odds of wound, hematological, and pulmonary complications, Clavien-Dindo grade IV, delayed length of stay >5 days, and a lower likelihood of being discharged home (P < 0.005). Clavien-Dindo grade is an ordinal classification system that describes complications after surgery. In the standard form of this grading system, Clavien-Dindo grade IV represents life-threatening complications after surgery.13 They also had a half-day longer hospital stay (P < 0.001). The BUN/Cr ratio, previously supported as a dehydration marker, was highlighted for risk stratification.7,8,11,12
Preoperative dehydration is common in various types of surgery, with reported prevalence rates ranging from 34.5% in lumbar spine patients to as high as 47% in arthroplasty patients.7,8 In our study, we found the prevalence of dehydration in ACDF patients to be 28.1%, with older and female patients being more likely to be dehydrated. Chan et al also found dehydration to be more prevalent in women undergoing orthopedic surgery and associated with a greater prevalence of postoperative urinary tract infections (UTIs) when compared with patients in the hydrated group (P < 0.0001).4 This may be due to women having lower muscle mass than men, resulting in a higher BUN/Cr ratio.6,14 Mukand et al found that dehydration was significant in older orthopedic surgery patients with prerenal azotemia, leading to a longer length of stay and more frequent discharge to nursing care facilities (P < 0.01).5 Their findings align with ours, where preoperative dehydration had higher odds of occurring in older patients and in women with a delayed length of stay >5 days and lower odds of being discharged home (P < 0.001). Rowat et al also found that being older, female, and prescribed diuretics were dehydration risk factors (P < 0.001).6
Preoperative dehydration has been associated with an increased risk of complications. Chan et al found that preoperative dehydration in orthopedic patients older than 65 years was associated with significantly higher rates of respiratory (P = 0.045), gastrointestinal (P < 0.001), and hematological (P < 0.001) complications as well as increased mortality rate.4 Preoperative dehydration in our study also increased the odds of pulmonary complications (OR = 1.79, 95% CI [1.36, 2.37], P < 0.001). Poor hydration can disrupt mucociliary clearance, ion transport, and epithelium nourishment while exacerbating pulmonary conditions.15 Moghadamyeghaneh et al and Rowat et al found similar results in patients undergoing colon surgery and stroke patients, respectively.6,12 Goodarzi et al found that preoperative hydration via intravenous fluids significantly reduced postoperative nausea, vomiting, fever incidence, and thirst but had no effect on postoperative pain.16 Prolonged fasting may lead to fluid deficits, contributing to perioperative discomfort and morbidity.17 Administering 1 L preoperatively or intraoperatively significantly reduced postoperative symptoms related to dehydration.17 Hydration status also has implications in disc degeneration, affecting effective stress distribution and increasing stiffness in intervertebral discs.18
Renfree et al investigated preoperative dehydration affecting elective lumbar surgery complications using the NSQIP database from 2006 to 2013. Contrary to the findings in our study, their results showed that dehydration did not negatively impact perioperative outcomes or readmission. Preoperative dehydration was shown to increase the risk of deep vein thrombosis (P = 0.002), UTI (P < 0.001), and the need for postoperative transfusion (P < 0.001).8 Renfree et al inclusion of only elective spine surgery and operating in a different region of the body may partially elucidate the differences in our conclusions. Moore et al also found that dehydration before total joint arthroplasty did not increase the risk for postoperative cardiac, renal, or cerebrovascular complications.7 These findings highlight the importance of considering the types of surgeries conducted and how dehydration may impact a patient’s recovery depending on the procedure.
Contrary to the findings in our study, Renfree et al investigated preoperative dehydration affecting elective lumbar surgery complications using the NSQIP database from 2006 to 2013. Their results showed that dehydration did not negatively impact perioperative outcomes or readmission. While largely noncontributory, preoperative dehydration was shown to increase the risk of deep vein thrombosis (P = 0.002), the risk of UTI (P < 0.001), and the need for postoperative transfusion (P < 0.001).8 Renfree et al inclusion of only elective spine surgery and operating in a different region of the body may partially elucidate the differences in our conclusions. Moore et al also found that dehydration before total joint arthroplasty did not increase the risk for postoperative cardiac, renal, or cerebrovascular complications.7 When compared with Renfree et al, these findings draw attention to the types of surgeries conducted and how dehydration may impact a patient’s recovery depending on the procedure. The impact of preoperative dehydration on postoperative complications may vary depending on the type of surgery performed. For instance, open and closed laparoscopic intra-abdominal surgeries, as studied by Moghadamyeghaneh et al, may involve more significant fluid changes compared with laparoscopic colon and rectal surgery or arthroplasty procedures. Furthermore, evidence suggests that preoperative dehydration may have a less significant impact on postoperative morbidity in certain orthopedic cases. Thus, the relationship between hydration status and postoperative complications is complex and varies on a case-by-case basis.
Our study fills a gap in the literature on preoperative dehydration in ACDF surgery. The differences pointed out in the studies can be explained by the circumstances of surgery and the organ systems involved. Future studies could include prospective randomized controlled trials involving preoperative IV fluid administration to further investigate the impact of preoperative dehydration on postoperative outcomes. Additionally, there should be a focus on differences between specific surgical procedures and associated risks of preoperative dehydration and postoperative complications in each circumstance.
Limitations
Weaknesses of our study include its retrospective nature and limited access to patient-reported outcomes. Additionally, the study only assessed complications within the first 30 days postoperatively and did not evaluate long-term complications. Furthermore, we recognize that the preoperative laboratory values in the NSQIP database represent hydration status preceding the 30-day preoperative period. Future studies with preoperative laboratory values obtained closer to the procedure date are needed to confirm or refute these findings. We were also limited by the lack of socioeconomic data, which made it difficult to control for potentially impactful variables that can affect patient outcomes. Finally, it is important to note that a BUN/Cr ratio can be falsely elevated and should be correlated with urine osmolality or a clinical examination for the best assessment of hydration status.
CONCLUSION
The relationship between preoperative dehydration and 30-day postoperative outcomes for elective ACDF surgery has not been previously studied. Utilizing multivariate analysis, we found that dehydration before ACDF surgery can increase the risk of various complications and increase the length of hospital stay by half a day.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.