


Abstract
Background Trauma to the thoracic, thoracolumbar (TL), and lumbar spine is common and can cause disability and neurological deficits. Using a cohort of patients suffering from thoracic, TL, and lumbar spine trauma in a tertiary hospital in East Africa, the current study sought to: (1) describe demographics and operative treatment patterns, (2) assess neurologic outcomes, and (3) report predictors associated with undergoing surgery, neurologic improvement, and mortality.
Methods A retrospective cohort study of patient records from September 2016 to December 2020 was conducted at a prominent East Africa referral center. The study collected data on demographics, injury, and operative characteristics. Surgical indications were assessed using the AO (Arbeitsgemeinschaft für Osteosynthesefragen) TL fracture classification system and neurological function. Logistic regression analysis identified predictors for operative treatment, neurologic improvement, and mortality.
Results The study showed that 64.9% of the 257 TL spine trauma patients underwent surgery with a median postadmission day of 17.0. The mortality rate was 1.2%. Road traffic accidents caused 43.6% of the injuries. The most common fracture pattern was AO Type A fractures (78.6%). Laminectomy and posterolateral fusion were performed in 97.6% of the surgical cases. Patients without neurological deficits (OR: 0.27, 95% CI: 0.13–0.54, P < 0.001) and those with longer delays from injury to admission were less likely to have surgery (OR: 0.95, 95% CI: 0.92–0.99, P = 0.007). The neurologic improvement rate was 11.1%. Univariate analysis showed a significant association between surgery and neurologic improvement (OR: 3.83, 95% CI: 1.27–16.61, P < 0.001). However, this finding was lost in multivariate regression.
Conclusions This study highlights various themes surrounding the management of TL spine trauma in a low-resource environment, including lower surgery rates, delays from admission to surgery, safe surgery with low mortality, and the potential for surgery to lead to neurologic improvement.
Clinical Relevance Despite challenges such as surgical delays and limited resources in East Africa, there is potential for surgical intervention to improve neurologic outcomes in thoracic, TL, and lumbar spine trauma patients.
Level of Evidence 4.
INTRODUCTION
Traumatic spinal injury (TSI), which includes spinal column fractures and spinal cord injuries (SCIs), is a major global cause of disability and mortality.1,2 The incidence is higher in low- and middle-income countries (LMICs), at 13.69 per 100,000 people, than in high-income countries (HICs), at 8.72 per 100,000 people.3 Most patients with TSI require surgical intervention; however, surgery rates are low in LMICs due to limited access to health care, lack of trained personnel, financial barriers, limited infrastructure and resources, and cultural and societal factors.2 LMICs account for only 3.5% of the projected 234 million surgeries despite accounting for more than one-third of the global population.4 Furthermore, although urgent decompression and stabilization have been proven to improve neurologic outcomes in patients with SCI,5,6 this is yet to be translated in LMICs as the timing for surgery is still prolonged. In a 2022 systematic review conducted by Chanbour et al, it was revealed that the delay from the time of injury to reaching the operating room was approximately 36 hours longer in LMICs compared to HICs.2 Such delays in surgical intervention can lead to complications, prolonged hospital stays, and increased health care costs.7
Anatomically and functionally, the thoracolumbar (TL) spine refers to the region comprising the thoracic spine (T1-T10), the TL junction (T10-L2), and the lumbar spine (L3-L5).8 TL spine injuries are prevalent and can cause substantial disability, deformity, and neurological deficit.9 Approximately 50% to 60% of injuries to the TL region affect the transitional zone (T10-L2), while 25% to 40% involve the thoracic spine and 10% to 14% affect the lower lumbar spine and sacrum.10 These injuries are more common in young men aged 20 to 40 years, with motor vehicle accidents and fall from heights accounting for 65% of all cases.11,12
Approximately 50% of TL injuries are considered unstable,9 and posttraumatic neurological deficits are common. The region involved and the fracture type determine the likelihood and severity of neurologic deficit. Due to its rigid structure, the thoracic spine has a high prevalence of neurological deficits because of its narrow spinal canal and the energy required to induce fractures in this region.13 Conversely, the lumbar spine has a lower incidence of neurological impairments due to the larger size of the neural canal and the greater resilience of the cauda equina nerve roots.13 In a multicenter study, the incidence of neurological deficit ranged from 22% to 51% depending on the fracture type (22% in type A, 28% in type B, and 51% in type C fractures), according to the AO classification, a system used to classify spine trauma with good reliability and using descriptive terms for each injury.14,15
Despite significant advances in spinal imaging and management procedures over the past 2 decades, a shortage of rigorous clinical studies has contributed to a debate over the best management for patients with thoracic, TL, and lumbar spine injuries.16 Using a population of thoracic, TL, and lumbar spine trauma patients from a major East Africa referral center, our goals were to (1) describe demographics and operative treatment patterns, (2) assess neurologic outcomes, and (3) report predictors associated with undergoing surgery, neurologic improvement, and mortality among patients managed at a primary referral center for spine trauma in Tanzania.
METHODS
Study Design and Clinical Setting
We retrospectively analyzed prospectively collected data from the Muhimbili Orthopedic Institute (MOI), a major referral hospital in Dar es Salaam, Tanzania. MOI houses 380 general ward beds, 18 intensive care unit beds, 16 high dependency unit beds, 10 emergency department beds, and 9 operating rooms. Onsite imaging includes x-rays, computed tomography (CT), and magnetic resonance imaging (MRI). The local institutional review board approved the current study, and informed consent was obtained from all patients.
Patient Identification
All consecutive patients admitted for TSIs at the thoracic, TL, and lumbar levels from September 2016 to December 2020 (52 months) were included. Exclusion criteria included those <14 years old and those with moderate or severe traumatic brain injury. Additionally, we excluded patients with C-spine injuries or fractures.
Clinical and Operative Data
Several demographic and injury-specific data points were collected, including age, gender, and mechanism of injury. Injury levels were categorized according to prior studies.17 Due to the difficulty in deciphering the extent of decompression, this variable was kept binary (yes/no). Insurance status was classified as public (had to provide all funds before receiving hospital services) or private (no additional funds required to receive hospital services).
Classification of Fractures, Neurologic Status, Surgery, and Timing
We classified fractures according to the AO TL classification.18 If applicable, we also documented the degree of listhesis by using the following classification: Grade I = 25% of listhesis, Grade II = 50%, Grade III = 75%, and Grade IV = 100%. Spondyloptosis had a listhesis of >100%.19 Neurological examinations were obtained on admission and discharge, according to the American Spinal Injury Association (ASIA) Impairment Scale.20 The type of surgery was classified into 2 groups:
Posterior laminectomy and fusion with pedicle screws.
Decompression only.
We recorded time in days for the following time points: injury to admission, admission to the operating room, and total length of stay.
Surgical Indication
All patients were retrospectively reviewed by a team of 2 individuals (a neurosurgery trainee and a consultant) to determine whether an indication for surgery was present using a combination of the AO fracture classification system and neurologic function in accordance with prior studies.18,21 An injury was considered to have a surgical indication in 1 of 2 ways: (1) the fracture was considered unstable (AO type A4, B, or C) or (2) the fracture was potentially unstable, classified as A0-A3 but with neurologic impairment (ASIA A–D) and neurological compression confirmed by the imaging. Given the limited resources, some patients only had x-ray images available, and in these cases, the best estimation of fracture type was made.
Statistical Methods
All continuous data were presented as mean (SD) and/or median with interquartile range (IQR), whereas all count data were presented as n (%). Mann-Whitney U and χ2 tests or the Fisher’s exact test was used to assess differences among continuous and categorical variables, respectively. Univariate logistic regression, followed by multivariate logistic regression, was used to evaluate predictors of 3 outcomes: operative treatment, improvement in neurologic function, and mortality. Any variable with P < 0.10 after univariate regression was included in the multivariate model. The second outcome of improved neurologic function was subdivided into a surgical group. The statistically significant level was set at 0.05, and statistical analysis was performed using R version 4.1.2 (Vienna, Austria).
RESULTS
Patient Demographics
During the study period, 257 patients were admitted to MOI with a TL spine injury. One hundred sixty-seven patients (64.9%) were treated operatively on a median (IQR) of the postadmission day 17.0 (7.0–30.0), whereas 90 were managed conservatively (Table 1).
Demographics, injury, and hospitalization information of patients with thoracic, thoracolumbar, and lumbar spine injuries.
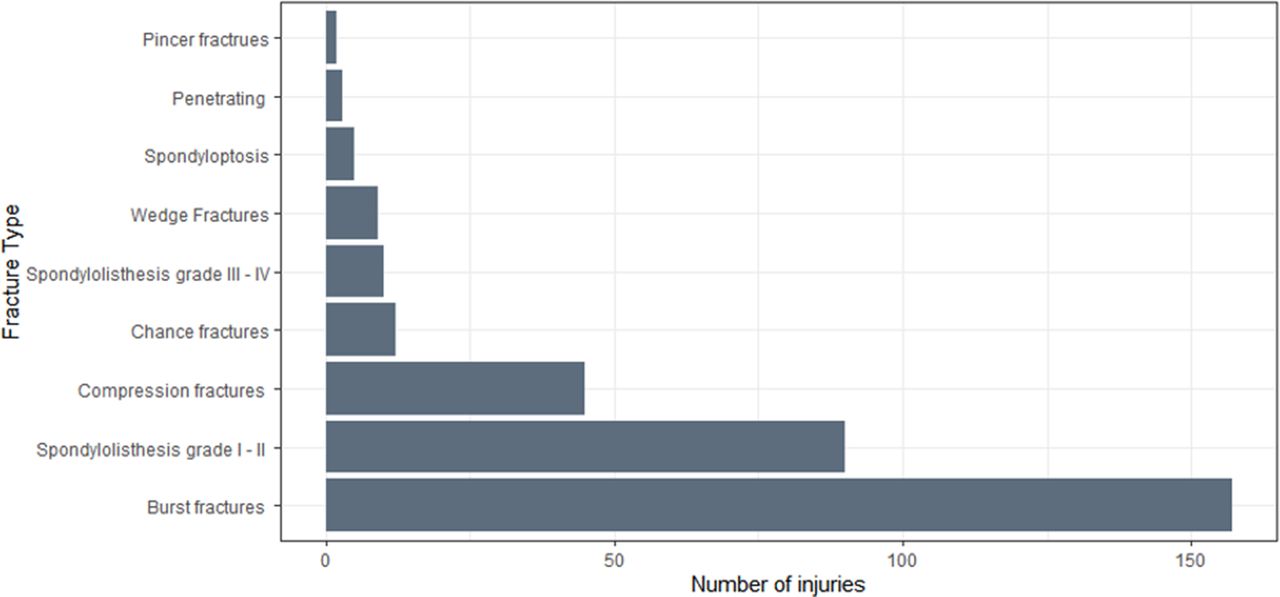
The cohort’s mean age was 35.2 years ± 11.3, with the nonoperative group slightly older. Regarding the cohort of 257 patients, road traffic accidents were the most common injury mechanism, and most patients had public insurance (87.5%). Almost all patients were admitted to an outside hospital before MOI (99.2%), leading to a median time from injury to MOI admission of 3.0 days (IQR: 1.0–7.0). X-ray images were obtained for most patients (80.5%). The most common fracture pattern was compression fractures (AO type A) (n = 202, 78.6% of patients), and among them, burst fractures (AO type A4) were the most common subclassification (n = 157, 61.1% of patients), followed by AO type C fractures associated with spondylolisthesis grade I/II (n = 90, 35.0% of patients). When comparing the operative and nonoperative groups, we noticed no difference in imaging between the 2 groups. Operative patients had more incomplete injuries, whereas nonoperative patients had more intact injuries. Interestingly, 72.2% of patients in the nonoperative group had an indication for surgery. Mortality was low in both groups, with 1 patient (0.6%) dying in the operative cohort and 2 (2.2%) in the nonoperative cohort (Figure 1).
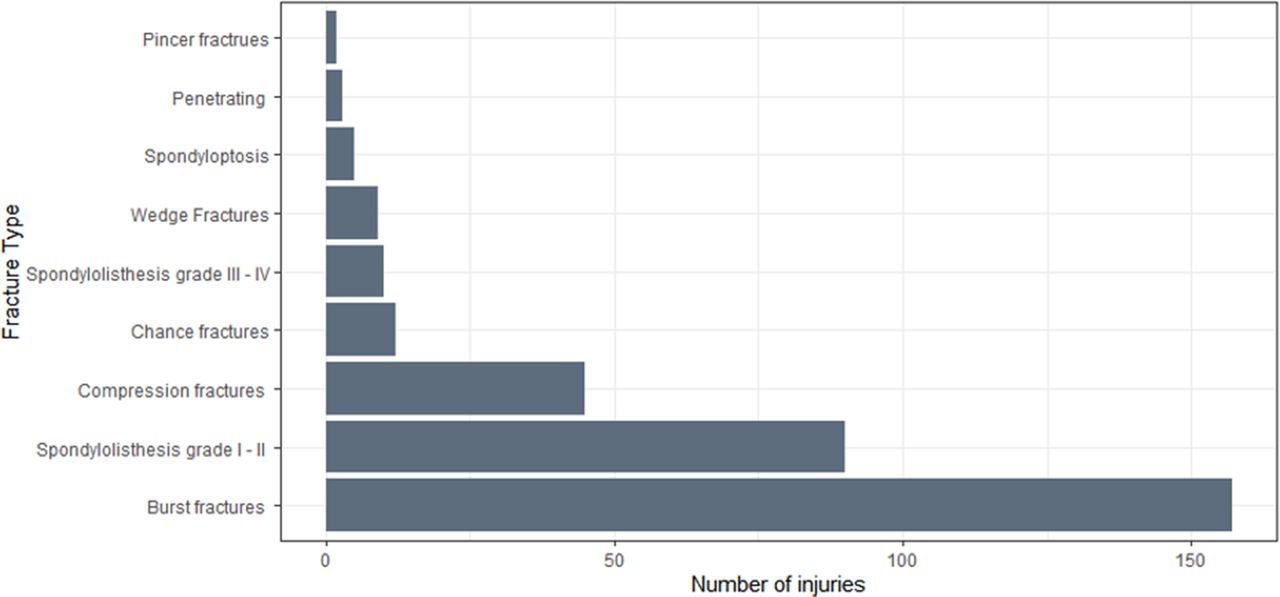
Fracture types among 257 thoracic, thoracolumbar, and lumbar spine trauma patients (each fracture type counted separately when more than 1 injury was present).
Operative Variables
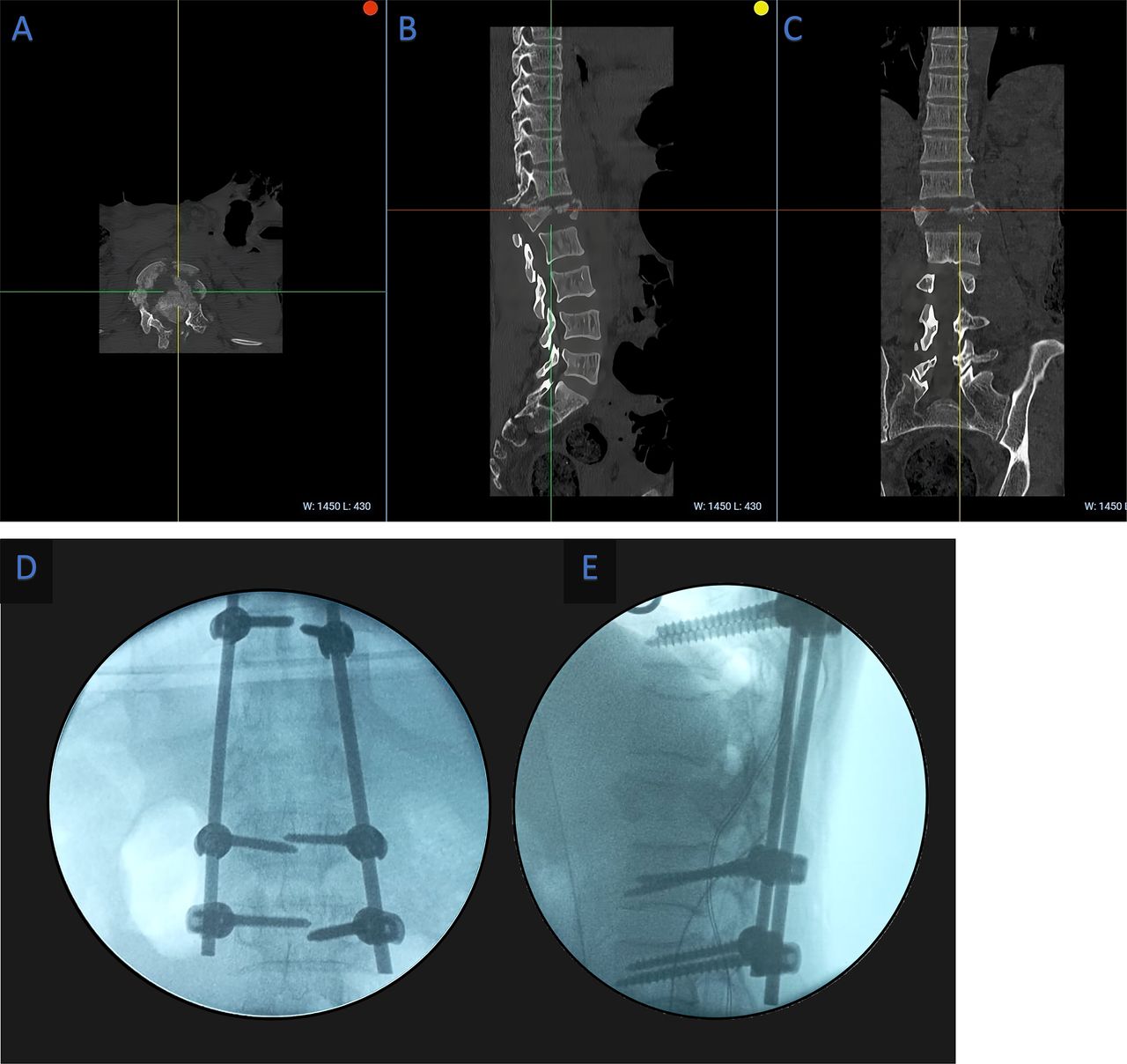
Approximately 232 thoracic, TL, and lumbar spine trauma patients (90.3%) had an indication for surgery, but only 167 patients (64.9% of the total sample; 71.9% of those with an operative indication) underwent to surgery. The 65 other patients (28% of those with an operative indication) did not undergo surgery despite the surgical indication. Of the 167 operative patients, posterolateral fusion (PLF) ± laminectomy was the most common operation (97.6%); only 3 patients underwent decompression only (Table 2). The mean numbers of screws and levels fused were 5.6 ± 1.7 and 2.7 ± 1.1, respectively, indicating that short-segment fusion was commonly done. A representative case of a surgically treated TL burst fracture is shown in Figure 2. The median time from admission to the operating room was 17.0 days (0–184). Approximately 52.6% of patients underwent postoperative imaging, almost exclusively radiography.
Operative details of those undergoing surgery.

(A–C) Axial, sagittal, and coronal preoperative computed tomography images of a patient with L1 burst fracture. (D, E) Intraoperative x-ray anteroposterior and lateral views after instrumentation.
Neurologic Status
Of the 252 patients with an examination recorded at discharge (98%), most had no ASIA change (n = 222, 88.1%). Twenty-eight patients (11.1%) improved neurologically by at least 1 ASIA grade. Among them, the ASIA score at admission was A for 5 patients, B for 11 patients, C for 6 patients, and D for 6 patients (Table 3). Twenty-five of the patients (89%) who improved were in the operative group. Only 2 patients worsened in the cohort, 1 in each subgroup, and both with ASIA-B on admission (Table 4).
Neurologic status: changes in ASIA score from admission to discharge
Neurologic status: classification of ASIA score changes, n (%).
Predictors of Undergoing Surgery
Logistic regression was used to assess predictors of undergoing treatment. After univariable logistic regression, the following factors emerged as factors associated with reduced odds of undergoing surgical treatment: (1) having an ASIA A/E compared to an ASIA B-D (incomplete injury) (OR: 0.45, 95% CI: 0.25–0.81, P = .009); (2) having an intact injury (ASIA E) compared to complete or incomplete injury (ASIA A-D) (OR: 0.29, 95% CI: 0.16–0.53, P < 0.001); and (3) longer time from injury to admission reduced the odds of getting surgery (OR: 0.97, 95% CI: 0.94–0.99, P = 0.048) (Table 5). Following multivariable logistic regression, 2 independent predictors of undergoing operative treatment emerged: (1) having an intact injury (ASIA E) compared to complete or incomplete injury (ASIA A-D) (OR: 0.27, 95% CI: 0.13–0.54, P < 0.001) and (2) longer time from injury to admission reduced odds of getting surgery (OR: 0.95, 95% CI: 0.92–0.99, P = 0.007). Hence, patients with intact injuries and a longer duration before admission are less likely to undergo surgical intervention.
Predictors of operative treatment.
Predictors of Neurologic Improvement
After univariable logistic regression, the following factors emerged as predictors of neurologic improvement: (1) having an upper thoracic/lumbar injury compared to a lower thoracic injury (OR: 3.97, 95% CI: 1.67–10.56, P = 0.002); (2) having a lumbar injury rather than a thoracic injury (as indicated by the OR of 0.14 for thoracic injuries [95% CI: 0.05–0.33, P < 0.001], suggesting reduced odds of neurological improvement for thoracic injuries); (3) having surgical treatment compared to nonoperative treatment (OR: 3.83, 95% CI: 1.27–16.61, P = 0.034); and (4) having an incomplete injury compared to complete injury (OR: 8.71, 95% CI: 3.38–27.05, P < 0.001) (Table 6). However, following multivariable logistic regression, only 1 independent predictor emerged: having an incomplete injury (ASIA B-D) compared to a complete injury (ASIA A) (OR: 5.74, 95% CI: 1.94–18.00, P = 0.002). In the subset of 138 patients who underwent surgery, univariable logistic regression showed that (1) patients with an upper thoracic/lumbar injury had higher odds of neurological improvement compared to those with a lower thoracic injury (OR: 3.36, 95% CI: 1.34–9.22, P = .012) and (2) patients with a thoracic injury were less likely to have neurological improvement compared to those with a lumbar injury (OR: 0.17, 95% CI: 0.06–0.42, P < 0.001). Following multivariable logistic regression, only 1 independent predictor emerged: patients with a thoracic injury were less likely to have a neurological improvement compared to those with a lumbar injury (OR: 0.09, 95% CI: 0.00–0.51, P = 0.027).
Predictors of neurologic improvement among all patients and operative patients. Multivariable logistic regression controlling for age, sex, admission neurologic exam, and level of injury.
Predictors of Mortality
Only 3 patients in the cohort died—1 patient (0.6%) in the operative group and 2 (2.2%) in the nonoperative group—for an overall mortality rate of 1.2%. After regression analysis, no factor was significantly associated with increased odds of mortality. A trend for operative treatment being associated with reduced odds of mortality was seen, although statistical significance was not achieved (OR: 0.27, 95% CI: 0.01–2.80, P = 0.281) (Table 7).
Predictors of mortality among all patients (N = 257).
DISCUSSION
Injuries to the thoracic, TL, and lumbar spine are common in the trauma population, and patients who suffer from them have a life-changing event, especially in low-income countries. This study addressed the patterns of presentation, operative treatment, neurologic improvement, and mortality following TL spine trauma at a large East African referral facility. While 90.3% of all patients had a surgical indication, it is notable that 72.2% of patients managed nonoperatively had indications. One hundred sixty-seven patients underwent surgery at a median of 17 days after admission. Almost all patients underwent a PLF, with an average of 2.7 levels fused with 5.6 screws. Patients with intact injuries and a longer duration before admission were less likely to undergo surgery. Neurologic improvement rates were low at 11.1%, with the majority (89%) occurring in the surgical group. Furthermore, compared to patients with lumbar injuries, patients in the surgical group with thoracic injuries had decreased odds of improvement. The cohort’s mortality rate was low, at 1.2%. Overall, this study highlights the relatively low surgical rates, delayed timing of surgery, safe surgery with minimal mortality, and the potential for neurological improvement associated with surgical intervention in thoracic, TL, and lumbar spine trauma patients in low-resource settings.
Lack of Operative Treatment Overall
A key finding of this study was the low surgery rates. Among the patients managed without surgery, 72.2% had indications for surgery. Surgical procedures for traumatic spinal injuries are performed in several LMICs, and they remain relatively scarce and carry significant risks as evidenced by a study reporting increased complications and mortality rates among patients who underwent surgery.22 Low surgery rates are not specific to spine trauma alone but are commonly observed across various surgical specialties in LMICs. A study demonstrated that only a disproportionately small percentage, approximately 6.3% globally,23 of surgical procedures are performed in LMICs, despite the substantial burden of surgical conditions experienced in these regions.24
Several barriers, including financial constraints, inadequate referral systems, and poor health care–seeking behavior, result in reduced surgery rates in LMICs.25 Limited financial resources often impede access to surgery, necessary implants, surgical care, and comprehensive clinical management.26 For instance, in a Nigerian study by Nwanko et al,27 strut grafts and interspinous wiring were utilized to minimize costs, yet 43% of the remaining 68 patients with indications for surgery could not undergo operative treatment due to their inability to pay. Similarly, in this study, 87.5% of patients lacked health insurance and had to cover their medical expenses out-of-pocket, which may have influenced the decision to undergo surgery. Our group’s initial study also highlighted that implant availability and economic factors such as insurance status significantly influence the decision to perform surgery and the timing of surgery.19,28
Furthermore, the choice of construct size may have been affected by the ability to pay as short-segment fixation was predominantly utilized, with an average fusion level of fewer than 3. While long-segment fixation does not necessarily offer substantial advantages over short-segment fixation, there are inherent risks associated with short-segment constructs when the upper and lower instrumented vertebrae involve the fractured levels or when constructs end at junctional levels.19 These risks could be effectively mitigated with improved access to implants.
Predictors of Surgery
Surgery is vital for managing spine trauma by restoring spinal anatomy, ensuring mechanical stability, and preserving or improving neurological function.9 Our research indicates that patients with intact injuries are less likely to undergo surgery than those with incomplete or complete injuries. This distinction arises from the fact that surgery is typically reserved for cases involving instability, deformity, or compression of neural structures that could lead to neurological deficits. Conversely, conservative management approaches such as brace or orthotic immobilization, pain management, and physical therapy are often sufficient for promoting healing and recovery in patients with intact injuries.13
Furthermore, our findings reveal that patients with a longer duration before seeking medical attention are less likely to undergo surgery. The delayed presentation can give rise to increased complications, including the development of pressure sores, chest infections, and other medical conditions. Additionally, the delayed admission may contribute to the natural fusion of the injured spine, reducing the necessity for surgical intervention.
It is important to emphasize that the decision regarding surgery for thoracic, TL, and lumbar spine trauma is complex and should be based on a comprehensive evaluation of the individual patient’s clinical presentation, imaging findings, neurological status, and overall health. This process typically involves a multidisciplinary approach involving spine surgeons and other health care professionals. By considering these factors, the most appropriate treatment plan can be determined for each patient.
Neurological Improvement
Timely surgical intervention, particularly within the first 72 hours, significantly impacts the potential for neurological improvement in patients with thoracic, TL, and lumbar spine injury.29 Surgery plays a crucial role by facilitating the removal of retropulsion bone fragments, decompressing nerve roots, and providing structural support. When performed early, surgery enables early mobilization, reduces complications, and leads to shorter hospital stays and less time in intensive care units.
Our study noted a median time of 17 days from admission to surgery, which likely explains our cohort’s relatively low rate of neurological improvement of 11.1% at discharge. Despite this delay, we found that surgery showed potential neurological improvement. Patients who underwent surgery had more than three times the likelihood of experiencing improvement than those who did not. Remarkably, a similar study conducted in India revealed that even with a mean interval of 24.45 days between injury and spine surgery, 51.5% of patients achieved an increase of at least 1 in their ASIA grade at the 1-year follow-up.30 This highlights that there is still a significant chance of neurological improvement even after delayed surgery. These findings are intriguing as they underscore the potential for neurological improvement even in cases of delayed surgical intervention, often encountered in resource-limited settings. Consequently, they emphasize the critical role of surgical decompression in thoracic, TL, and lumbar spine trauma patients, irrespective of any delay in the surgical procedure.
In addition to surgery and timing, neurological improvement in thoracic, TL, and lumbar spine trauma is influenced by multiple factors, including injury severity (measured by admission ASIA grade) and the specific spinal cord region affected.31 A study focusing on neurologic improvement after thoracic, TL, and lumbar spine injuries revealed that patients with lumbar impairment had a significantly higher likelihood of improvement in ASIA levels (up to 90%) compared to those with thoracic and TL injuries (22.4% improvement).32 Their study also revealed that incomplete injuries (ASIA B–D) exhibited significantly higher rates of improvement (95.2% for ASIA D) compared to complete injuries (7.7% for ASIA A).
Our study identified incomplete injury (ASIA B–D) as the sole independent predictor of neurological improvement, with patients experiencing nearly a 6-fold increase in the likelihood of improvement compared to those with complete injuries. Furthermore, among patients who underwent surgery, individuals with thoracic injuries had a lower chance of improvement (9%) compared to those with lumbar injuries. This discrepancy can be attributed to several factors. The lower rates of improvement in the thoracic spine can be linked to the prevalence of complete neurological deficits typically associated with thoracic fractures.33 A smaller canal diameter characterizes the thoracic region and is often implicated in high-energy mechanism injuries due to its inherent rigid structure, which may predispose it to complete injuries.13,34 In contrast, the lumbar region benefits from a higher proportion of lower-to-upper motor neurons in the distal spinal cord and the potential for “root escape.”35
Mortality
Mortality is a common complication following spine trauma, and it has consistently been observed that mortality rates are significantly higher in cervical injuries compared to thoracic, TL, and lumbar injuries.28 In northeast Tanzania, rural India, and Nigeria, the reported mortality rates for cervical trauma were 27.2%,36 30%,37 and 72%,38 respectively. Conversely, mortality rates following thoracic, TL, and lumbar injuries in the same regions were comparatively lower, with 17.9% in northeast Tanzania,36 4.3% in rural India,37 and 28% in Nigeria.38 The higher mortality rates associated with cervical injuries can be attributed to the involvement of upper segments of the spinal cord responsible for vital functions like respiration.39Additionally, cervical injuries are more likely to result in complete injuries, which are known to be associated with higher complications.
This study examined mortality rates following thoracic, TL, and lumbar spine injuries, which were 1.2%. This finding aligns with the existing literature, as a meta-analysis reported in-hospital mortality rates ranging from 0% to 10% for thoracic, TL, and lumbar spine injuries.40 Similarly, a recent study conducted in Cameroon described a mortality rate of 5.7%.41 Although our regression analysis did not reveal any predictors of mortality, there was a noticeable trend suggesting a reduction in mortality among patients who underwent surgical intervention. This trend can be attributed to several factors, including early mobilization facilitated by surgery.5 Moreover, advancements in surgical skills, anesthesia techniques, and postoperative nursing care have significantly contributed to the improved safety and success of surgical procedures in treating thoracic, TL, and lumbar spine injuries. These findings underscore the importance of surgical management in achieving favorable outcomes and reducing mortality rates in the context of thoracic, TL, and lumbar spine injuries in Africa.
Areas of Improvement
The management of thoracic, TL, and lumbar spine injuries in Tanzania has experienced significant advancements thanks to international collaboration and partnerships, including the collaboration between the Department of Neurosurgery at MOI and the Department of Neurosurgery at Weill Cornell Medical College.42–44 These collaborative efforts, training programs, and accumulated experiences have been crucial in improving TSI management. However, despite these positive developments, the outcomes of TSI patients in Tanzania still fall behind those observed in HICs.2 It is worth noting that in our series, road traffic accidents account for nearly half of the cases. This underscores the urgent need for targeted interventions aimed at improving road safety.
While prevention should be a key focus, it is also essential to direct attention toward other areas of improvement. One such area is the need to establish additional spine trauma centers. A previous study by our group revealed that patients, on average, have to travel a distance of 278 km to access proper care.28 This significant travel distance delays receiving necessary surgical interventions, ultimately impacting patient outcomes. This study’s median time from injury to admission was 3 days, highlighting the urgent need to address this delay. Furthermore, there is an overwhelming number of trauma patients in Tanzania. According to estimates,45 approximately 5,227 trauma patients are admitted daily to only 105 district and regional hospitals designated for trauma cases. Increasing the number of spine centers in the region can effectively reduce the time gap between trauma and timely medical or surgical intervention. However, it is crucial to recognize that establishing, accrediting, and maintaining such centers can be resource-intensive and costly, despite their potential cost-effectiveness.46
There is also an urgent need to improve surgical skills. While the surgical expertise at MOI is commendable, there is room for further enhancement by adopting new approaches, such as anterior or lateral approaches. One potential avenue for improvement is to allow local surgeons to participate in short-term spine fellowship programs, which would facilitate acquiring new skills and techniques.47,48
Finally, there is a need to implement the consistent use of a region-specific spine trauma protocol. Standardized management protocols in health care have demonstrated benefits, including increased consistency, reduced heterogeneity in patient care, prevention of harm, improved adherence to evidence-based recommendations, reduced cognitive strain, and enhanced communication among health care providers.49 Currently, there is no consistent use of a trauma protocol for this patient group in the region. Implementing a region-specific protocol for trauma patients is expected to yield better outcomes. Our objective moving forward is to ensure the consistent use of a region-specific trauma protocol.
By focusing on these areas of improvement, including preventive measures, establishing additional trauma centers, addressing discrepancies in fusion techniques, enhancing surgical skills, and consistent use of a region-specific trauma protocol, Tanzania can make significant strides in the management of thoracic, TL, and lumbar spine injuries, ultimately improving patient outcomes and narrowing the gap between local practices and international standards.
Limitations
This study has certain limitations. First, there are missing data in the dataset, which were handled using pairwise deletion, although it may not be the optimal method. However, since the missing data were <5%, it is unlikely to affect the results significantly. Second, the study relied on data from a single institution, limiting the generalizability of the findings. Nevertheless, the hospital is a prominent spine trauma referral center with a diverse patient population, as indicated by patients traveling an average distance of approximately 280 km. Therefore, the results may apply to other emerging countries with similar demographics. Third, neurologic evaluations were only conducted at the time of discharge, preventing assessment of subsequent improvement or decline. Fourth, the data were retrospectively analyzed despite the cohort derived from a prospectively maintained spine database. Fifth, our data collection is limited to pressure sores, omitting other nonspine-related complications like pneumonia. This oversight could be significant as these complications often increase with nonoperative or delayed operative treatments. Future studies will seek to broaden data collection to encompass a broader range of nonspine-related complications. In summary, while the lack of follow-up data hampers our analysis, it also underscores the challenges of conducting research and performing surgeries in low-resource settings. Nonetheless, we hope that the scientific conclusions can enhance the care provided to spinal trauma patients in Tanzania.
CONCLUSION
This study has illuminated key aspects of managing thoracic, TL, and lumbar spine trauma patients in a resource-constrained setting. Approximately two-thirds of patients with thoracic, TL, and lumbar spine trauma underwent surgical decompression and stabilization. The median duration from admission to surgery was found to be 17 days. Notably, patients who had no neurological deficits and those with a longer time interval between injury and admission had lower rates of undergoing surgery. However, it was observed that surgery was associated with improvements in neurological function. Surgical intervention has proven crucial, particularly for patients with incomplete injuries, offering potential neurological improvement even after delayed surgery.
To further enhance patient care and outcomes, addressing road safety, establishing additional spine trauma centers, improving surgical skills, and implementing a region-specific trauma protocol are essential steps. These measures can help bridge the gap between local practices and international standards in managing spine trauma patients in Tanzania and similar resource-limited contexts. Despite its study limitations, our study’s findings contribute to the ongoing efforts to enhance spinal trauma patient care in such settings.
Acknowledgments
We thank the interdisciplinary team, including nurses, residents, and fellows, who cared for these patients.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.While this research did not receive specific funding, some implants used in the management of patients in this study were donated by DePuy Synthes. This support did not influence any aspect of the study.
Disclosures Roger Hartl reports royalties from Zimmer Biomet, consulting fees from DePuy Synthes and Brainlab, and serving as an advisor with RealSpine and 3D Bio. The remaining authors report no disclosures.
Ethical Considerations For the quality improvement database utilized in this study, participants were identified through daily reviews of admitted patients. Routine clinical data were entered into the quality improvement database by clinicians caring for the patients. The ethical review committees of the Muhimbili University of Health and Allied Sciences (Dar es Salaam, Tanzania) and Weill Cornell Medicine (New York, USA) reviewed the database (20-01021336). It was determined that further institutional board review and patient consent were not required for entry into the quality improvement database or anonymous analysis of the database. For the images used in this study, written informed consent was obtained from the patient before submission.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.