

Abstract
Background This study evaluated discrepancies between the expected intervertebral disc height (DH) and segmental lordosis (SL), defined as predicted values based on the rotations of the expandable cage driver, and the actual DH and SL achieved postoperatively in lateral lumbar interbody fusion (LLIF) using expandable cages.
Methods A retrospective review was conducted on patients who underwent LLIF with expandable cages between May 2022 and May 2024. The study included 51 patients (28 men and 23 women; mean age: 70.6 ± 11.7 years). Surgical outcomes measured included SL, anterior DH, posterior DH, average DH, canal diameter, and central canal area (CCA). Pre- and postoperative measurements were compared to evaluate cage effectiveness.
Results Postoperative measurements showed significant improvements: SL increased from 3.5° to 4.8° (P = 0.002), anterior DH from 5.9 to 10.7 mm (P < 0.001), PDH from 3.4 to 7.7 mm (P < 0.001), and average DH from 4.6 to 9.2 mm (P < 0.001). Despite these gains, the actual SL (4.8°) was significantly lower than the predicted SL (8.7°, P < 0.001). Canal dimensions also improved, with canal diameter increasing from 5.0 to 8.3 mm and CCA from 55.8 to 89.7 mm² (P < 0.001 for both). A significant correlation was found between changes in posterior DH and CCA (r = 0.272, P = 0.017).
Conclusion Expandable cages in LLIF significantly improved DH, SL, and canal dimensions, contributing to better clinical outcomes. However, achieving the ideal SL remains challenging, highlighting the need for further refinement in surgical techniques and cage design.
Clinical Relevance Expandable cages in LLIF significantly enhance DH, SL, and spinal canal dimensions, which contribute to improved clinical outcomes such as pain relief and functional recovery. However, the difficulty in achieving the ideal SL suggests further advancements are needed in surgical techniques and cage design to optimize patient outcomes and long-term spinal alignment.
Level of Evidence 3.
- lateral lumbar interbody fusion
- expandable cage
- indirect decompression
- segmental lordosis
- disc height
Introduction
In recent years, the efficacy of indirect decompression using lateral lumbar interbody fusion (LLIF) has been increasingly reported.1–3 LLIF involves inserting a large interbody cage into the intervertebral disc space, which can improve dural compression and enhance local alignment while minimizing damage to posterior support structures. Compared with minimally invasive transforaminal lumbar interbody fusion, LLIF is recognized as a beneficial minimally invasive approach for reducing postoperative complications such as dural tears and postoperative hematomas.4–6
Previous reports have generally shown favorable clinical outcomes with LLIF,3,7,8 though restoring sagittal alignment, including intervertebral disc height (DH) and segmental lordosis (SL), remains a topic of debate. Proper sagittal alignment is crucial, as it is associated with better clinical outcomes and overall spinal function.9,10 While indirect decompression may be achieved depending on the cage’s position, achieving optimal SL can be compromised.11,12 Cage-related factors, such as the cage’s size, shape, and position within the intervertebral disc space, likely play a significant role in achieving both indirect decompression and optimal sagittal alignment. When the intervertebral DH is narrow, inserting the cage becomes more challenging, complicating the surgical procedure. As the intervertebral disc space narrows, inserting a large cage forcibly increases the risk of endplate injury. This injury can lead to cage subsidence (CS), where the cage sinks into the vertebral body, compromising the surgery’s stability, alignment, and effectiveness. This may ultimately fail in achieving indirect decompression.
To address these challenges, expandable LLIF cages have been developed. These cages can be inserted into the intervertebral disc space in a collapsed state and then expanded to restore DH.13 The design of these cages aims to optimize surgical outcomes by improving the ease of insertion and ensuring better restoration of the intervertebral DH and SL, even in narrowed disc spaces.14,15 The expected DH and SL refer to the predicted height and angle based on the number of rotations of the expandable cage driver, with each rotation corresponding to a specific increase in DH and SL as specified by the manufacturer. The expected DH and SL are then compared with the actual postoperative DH and SL measured on imaging to assess the accuracy of the expansion.
Studies have reported the range of intervertebral DH and SL that can be achieved by rotating the driver several times, allowing surgeons to customize the expansion based on intraoperative needs and patient-specific anatomical considerations. However, while the use of expandable cages in LLIF is increasing, the effectiveness of cage expansion in radiographic outcomes for the intervertebral space remains unclear. Radiographic outcomes are critical in assessing the long-term success of the surgery, including the maintenance of intervertebral height and alignment. Moreover, there is a lack of studies investigating the discrepancy between the predicted alignment of expandable cages and the actual postoperative intervertebral DH and SL achieved, which is crucial for understanding the reliability of these devices.
Considering these gaps in knowledge, the present study aimed to evaluate whether there is a difference between the predicted and actual DH and SL in LLIF using expandable cages. Understanding this discrepancy is critical for optimizing surgical outcomes and improving patient care by guiding future practices and enhancing the reliability of LLIF techniques.
Materials and Methods
Patient Population
Starting in May 2022, expandable cages were used for LLIF procedures. After obtaining ethics committee approval, we conducted a retrospective review of the medical records of patients who underwent LLIF using expandable cages and posterior fixation at a single academic institution between May 2022 and May 2024. The inclusion criteria were patients aged 18 years or older with lower back pain, leg pain, and/or leg numbness who had undergone ineffective conservative treatment for at least 3 months before surgery. Additionally, patients had to have pre- and postoperative computed tomography (CT) and magnetic resonance images (MRIs) available. Criteria for fusion surgery included >3 mm of sagittal translation or >10° segmental angulation on dynamic radiographic evaluation, or posterior widening of the disc space by >5° on a flexion radiograph. Exclusion criteria included a previous history of posterior lumbar fusion, significant lumbar scoliosis >30°, grade 2 spondylolisthesis, or inability to cooperate due to mental illness. All patients were diagnosed preoperatively based on a detailed history, neurological and radiographic examinations, CT images after myelography, and/or MRI. The operating surgeon evaluated the location of stenosis based on preoperative imaging studies.
Surgical Technique
Patients underwent minimally invasive LLIF surgery using the previously described technique.16–21 Under general anesthesia, patients were placed in the lateral decubitus position and secured to the operating table with adhesive tape. The O-arm2 imaging system (Medtronic plc, Dublin, Ireland) was used to navigate the insertion of percutaneous pedicle screws (PPS) in the lateral decubitus position. The PPS was inserted with reference to the computer-aided design obtained from the navigation system. A skin incision was made along the virtual line of the computer-aided design model, and a suitable pilot hole was created using the Stealth-Midas system (Medtronic, Minneapolis, MN, USA). After creating the pilot hole, the PPS was inserted in the lateral decubitus position. Following the PPS insertion, LLIF was performed.
The psoas muscle was palpated, and the intervertebral space was confirmed using navigation. A retractor was placed using an anterior-to-psoas approach.22–24 Subsequently, a discectomy and endplate preparation were performed. An expandable cage was filled with artificial bone and bone marrow fluid, placed in a folded state, and gradually expanded within the intervertebral space under fluoroscopic guidance. The expandable cage used in this study was the RISE-L adjustable lordotic expandable cage (Globus Medical, Inc., Audubon, PA, USA), which is made of titanium alloy.
Fluoroscopic imaging and tactile feedback from contact between the cage and the intervertebral disc space determined the cage’s expansion. The expected DH could be estimated by counting the number of driver rotations. One rotation corresponds to an expansion of 0.5 mm in anterior disc height (ADH). The number of rotations was counted using the markings on the back of the driver.15 Table 1 shows the changes in DH and SL corresponding to the number of driver rotations for the expandable cage. As the number of driver revolutions increases from 0 to 14, ADH increases from 7 to 14 mm, PDH increases from 6 to 9.3 mm, and SL increases from 3° to 15°. These expected changes with the expandable cage are defined as the predicted DH and SL.
RISE-L adjustable lordosis expansion.
Characteristics of the subjects in the present study (N = 51).(Table 2)
Radiographic Assessment
Figure 1 shows each measurement. The intervertebral DH and SL were measured using CT before and approximately 2 weeks after the LLIF surgery. The ADH and posterior disc height (PDH) were evaluated, and the average disc height (AvDH) was defined as the average of the ADH and PDH. SL was determined based on the disc angle between lines perpendicular to the inferior end plate of the superior vertebra and the superior endplate of the inferior vertebra at each treated level (Figure 1).

Measurement of radiographic parameters. (A) Preoperative sagittal computed tomography (CT). (B and C) Postoperative sagittal CT. (a) Segmental lordosis. (b) Anterior disc height. (c) Posterior disc height. (d) Foraminal area was measured on CT images.
The left and right foraminal area (FA) was analyzed using sagittal CT images of the section showing the narrowest cross-sectional area of the LLIF. FA was defined as the space bounded by the superior and inferior pedicles, the posterior border of the disc anteriorly, and the facet joint complex posteriorly. The symbol ∆ indicates the change from before to after the operation.
Endplate injuries observed on x-ray or CT images taken during hospitalization were classified as early cage subsidence (ECS). If no endplate injury was evident within 2 weeks postoperatively but subsidence was detected during follow-up, it was classified as delayed cage subsidence (DCS). The number of patients who experienced CS was defined as the total number of patients classified as ECS and DCS.25
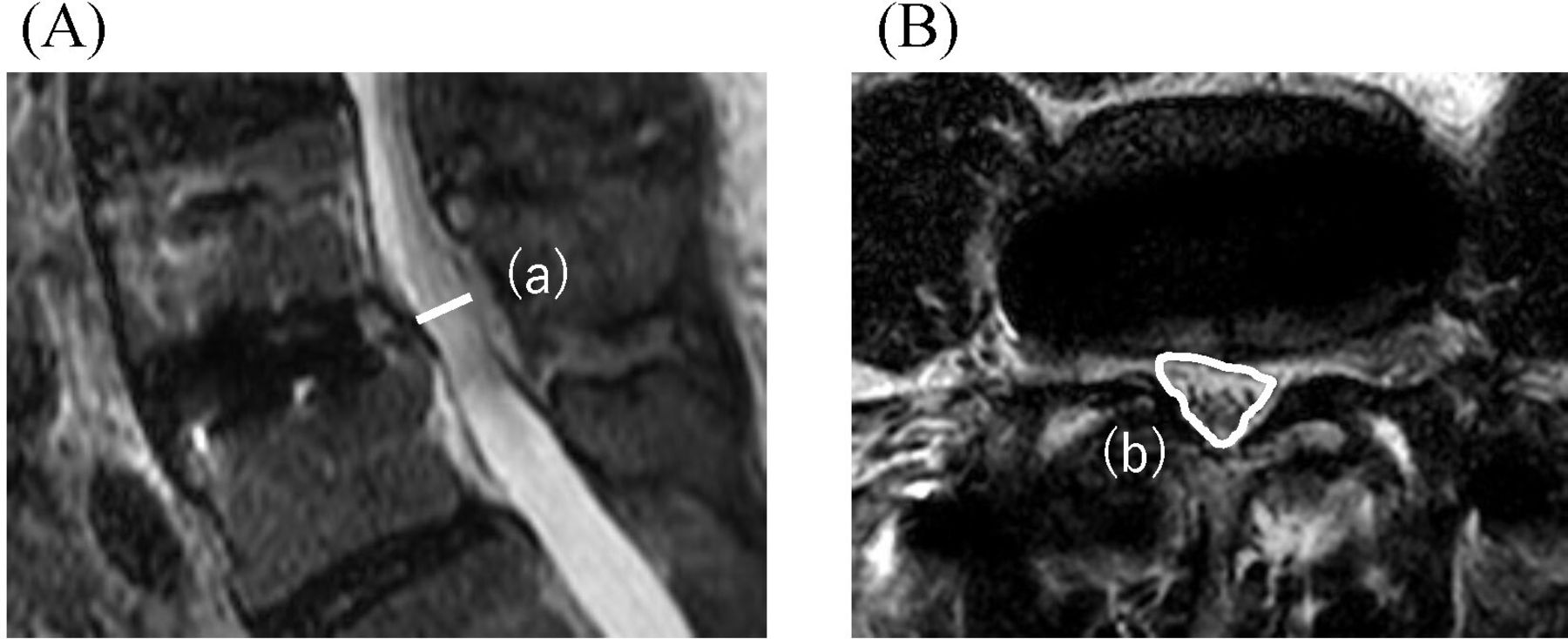
The position of the interbody cage was evaluated based on the relative position between the midpoint of the cage and the length of the inferior endplate. The center of the cage was defined as the midpoint between the anterior and posterior radiopaque markers of the cage. Specifically, if the position of the cage is less than 50%, it is considered to be positioned anteriorly, and if it is 50% or more, the cage is considered to be positioned posteriorly.17 Additionally, within 2 weeks before and after surgery, the midsagittal canal diameter (CD) and axial central canal area (CCA) of the thecal sac were measured using a 1.5T or 3.0T MRI system (Ingenia or Achieva; Philips Medical Systems, Best, Netherlands; Figure 2).26,27 The average image measurements used for the analyses were determined by reviewers who are also authors of this study (A.H. and D.S.).

Measurement of magnetic resonance imaging (MRI) findings. (A) Postoperative sagittal MRI. (B) Postoperative axial MRI. (a) Canal diameter and (b) central canal area were measured as the enclosed area of the spinal canal on sagittal and axial MRI.
Correlation Matrix of Parameters
We calculated the correlation matrix for the various parameters collected in our study to explore the relationships among the pre- and postoperative measurements. The parameters included were SL, ADH, PDH, AvDH, and cage position. Spearman correlation coefficients were used to quantify the strength and direction of the linear relationships between these parameters. The results were presented in the form of a heatmap.
Sensitivity Analysis
To evaluate the influence of various preoperative parameters on the accuracy of postoperative SL outcomes, we conducted a sensitivity analysis using feature importance scores derived from a random forest regression model, a well-recognized machine learning technique. The detailed approach was as follows:
Data Preparation: The analysis focused on 6 primary parameters: pre-ADH, pre-PDH, pre-AvDH, predicted ADH, predicted PDH, and predicted AvDH. These features were chosen for their presumed impact on the postoperative SL.
Model Training: We trained the random forest regression model with the selected parameters to predict the postoperative SL. This model was chosen for its ability to manage complex, nonlinear relationships effectively while minimizing overfitting. By utilizing an ensemble approach with multiple decision trees, the random forest model averages the predictions to achieve higher accuracy and robustness in performance.
Feature Importance Calculation: After training the model, we computed the feature importance scores to determine each parameter’s contribution to the SL predictions. The importance of a feature was assessed based on the decrease in model performance—measured by an increase in mean squared error—when the feature was removed or shuffled. Parameters that led to a substantial decline in performance were identified as more crucial. To improve reliability, we repeated the model training 5 times.
Statistical Analysis
Continuous variables were presented as means with SDs, and categorical variables were presented as frequencies and percentages. The Kolmogorov-Smirnov test was used to check for normal distribution in all continuous variables. The χ 2 test was used for categorical variables, while for continuous variables, t tests, analysis of variance, and the Mann-Whitney U test were employed. Pre- and postoperative continuous variables were analyzed using paired-samples t tests. Correlation analyses were conducted based on Pearson or Spearman correlation coefficients, depending on the data distribution. Data analysis was performed using SPSS Statistics software (version 23.0; IBM Corp., Armonk, New York, USA). A P value of less than 0.05 was considered statistically significant.
Results
Based on the inclusion criteria, 51 patients (28 men, 23 women; mean age: 70.6 ± 11.7 years) were included in the study. Key demographics, such as age, sex, height, weight, BMI, tobacco use, and steroid use, were recorded (Table 2). Most patients (86%) had lumbar canal stenosis with degenerative spondylolisthesis, and surgeries primarily targeted the L3 to L4 (43%) and L4 to L5 (47%) levels, with an average of 1.5 segments fused. The mean operative time was 128.1 ± 25.6 minutes, estimated blood loss was 92.7 ± 58.8 mL, and length of hospital stay was 15.5 ± 4.1 days.
Regarding the cage details, the mean dimensions were a height of 10.3 mm (after expansion), a width of 18 mm, and a length of 50.8 mm, with the cage placement at 51.4% of the intervertebral disc. In terms of specific placement locations, 27% of the cages were positioned anteriorly (<45%), 29% centrally (between 45% and 55%), and 44% posteriorly (>55%). ECS was not observed, but DCS occurred in 8% of cases. Additionally, 8% of patients experienced transient motor weakness, 12% had thigh pain or numbness, and 8% required revision surgery at another level or the same site.
Table 3 summarizes the preoperative, postoperative, and changes from pre- to postoperative sagittal measurements. Significant improvements were observed across several parameters following the LLIF surgery. Specifically, the mean SL angle showed an increase, improving from a preoperative value of 3.5° ± 4.2° to a postoperative value of 4.8° ± 2.8° (P = 0.002), indicating a mean change of 1.3° ± 3.6°. This improvement in SL is clinically meaningful, as it reflects the surgical objective of restoring spinal alignment. Similarly, DH measurements demonstrated substantial improvements postoperatively. The ADH increased significantly from 5.9 ± 3.3 mm preoperatively to 10.7 ± 1.8 mm postoperatively (P < 0.001), nearly doubling in size. This increase in ADH suggests effective decompression and restoration of the intervertebral space. The PDH also showed a marked improvement, increasing from 3.4 ± 2.6 mm to 7.7 ± 1.8 mm (P < 0.001). The AvDH, a composite measure, increased from 4.6 ± 2.7 mm to 9.2 ± 1.5 mm (P < 0.001), further confirming the overall success of the surgical intervention in expanding the disc space and correcting spinal alignment. Additionally, the FA significantly increased, improving from 96.7 ± 37.0 mm² preoperatively to 130.7 ± 39.3 mm² postoperatively (P < 0.001), representing a mean change of 33.9 ± 30.2 mm². This increase in FA is crucial because it suggests enhanced foraminal decompression, which is vital for relieving nerve compression.
Preoperative, postoperative, and change from pre- to postoperative sagittal measurements.
The differences between actual and predicted postoperative measurements are detailed in Table 4. Notably, the actual postoperative SL was 4.8° ± 2.8°, which fell short of the predicted SL of 8.7° ± 2.0°, resulting in a significant difference of 3.9° ± 3.5° (P < 0.001). This discrepancy highlights the challenge of achieving ideal postoperative alignment, suggesting potential areas for further refinement in surgical technique or patient selection. However, no significant differences were observed between actual and predicted postoperative measurements for ADH, PDH, or AvDH, with P values of 0.287, 0.721, and 0.494, respectively. These findings indicate that while SL may be difficult to perfect, DH restoration was consistent with preoperative predictions.
Postoperative vs ideal postoperative.
Table 5 provides a detailed analysis of changes in spinal canal dimensions, as measured by MRI before and after surgery. The mean CD increased significantly from 5.0 ± 2.4 mm preoperatively to 8.3 ± 2.5 mm postoperatively, reflecting a substantial improvement of 3.3 ± 2.0 mm (P < 0.001). In addition, the CCA increased significantly from 55.8 ± 35.8 mm² to 89.7 ± 36.1 mm² postoperatively, representing a mean increase of 33.9 ± 22.9 mm² (P < 0.001).
Radiographic evaluation of canal dimension changes (canal diameter and central canal area) in patients pre- and postoperatively using MRI.
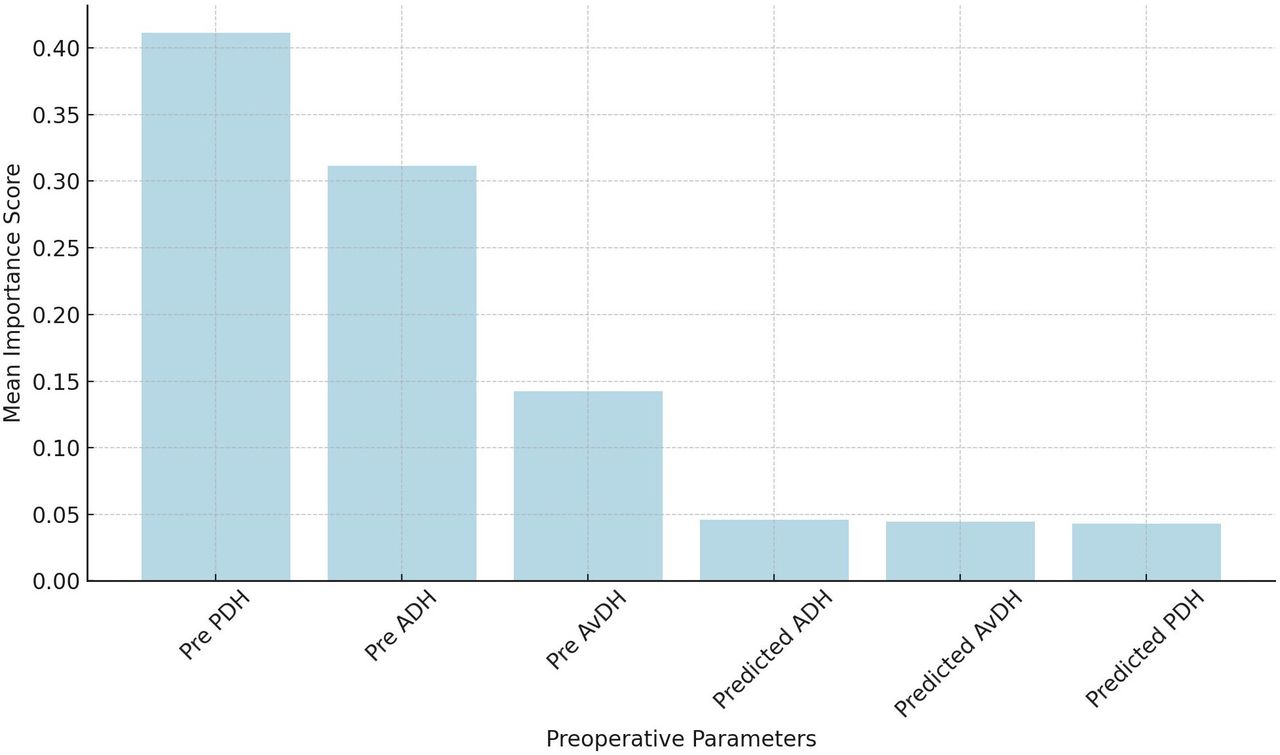
We performed a sensitivity analysis using feature importance scores from a random forest regression model to assess the influence of preoperative parameters on postoperative SL outcomes. The analysis revealed that pre-PDH had the highest importance score, indicating it as the most influential parameter for predicting postoperative SL, followed by pre-ADH and pre-AvDH. Predicted AvDH showed a lower importance score but still contributed to the model’s performance (Figure 3). This analysis emphasizes the significant impact of pre- and postoperative PDH on predicting postoperative SL outcomes. It suggests that further consideration of pre- and postoperative PDH could optimize surgical planning and outcome prediction before surgery.

Bar graph showing the feature importance scores derived from the random forest regression model used in the sensitivity analysis. The graph illustrates the relative impact of 6 key parameters. Pre-PDH demonstrated the highest importance, indicating its significant influence on postoperative SL outcomes. Abbreviations: ADH, anterior disc height; AvDH, average disc height; PDH, posterior disc height; SL, segmental lordosis;.
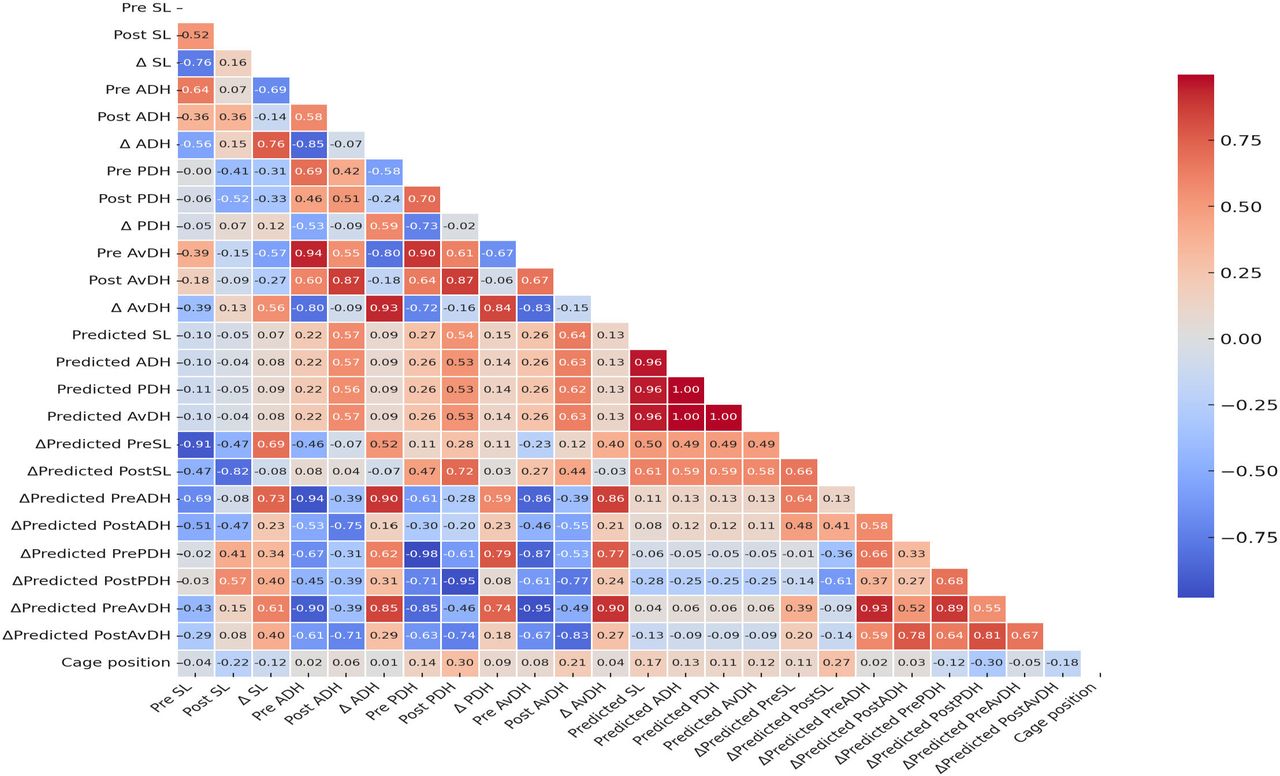
Next, we evaluated the correlation matrix to understand the relationships among key pre- and postoperative parameters, including SL, ADH, PDH, AvDH, and cage position. The analysis revealed weak-to-moderate correlations between these parameters, indicating that DH and SL interact in complex ways postoperatively (Figure 4).

Correlation matrix of parameters. The heatmap illustrates the correlation coefficients between key pre- and postoperative parameters. SL, ADH, PDH, AvDH, and cage position are evaluated for their linear relationships. Positive correlations are shown in shades of blue, while negative correlations are depicted in shades of red. The color’s intensity indicates the correlation’s strength, with darker shades representing stronger relationships. Abbreviations: ADH, anterior disc height; AvDH, average disc height; PDH, posterior disc height; SL, segmental lordosis;.
Finally, Table 6 examines the correlation between pre- and postoperative DH parameters (ADH, PDH, and AvDH) and SL with changes in CD (ΔCD) and CCA (ΔCCA). The preoperative analysis did not reveal any significant correlations between these DH parameters and changes in ΔCD or ΔCCA, indicating that preoperative measurements may not be reliable predictors of changes in spinal canal dimensions. Similarly, the postoperative analysis found no significant correlations between the same parameters and changes in ΔCD or ΔCCA, suggesting that the immediate postoperative state does not strongly influence these outcomes.
Correlation between DH and SL with changes in CD and CCA.
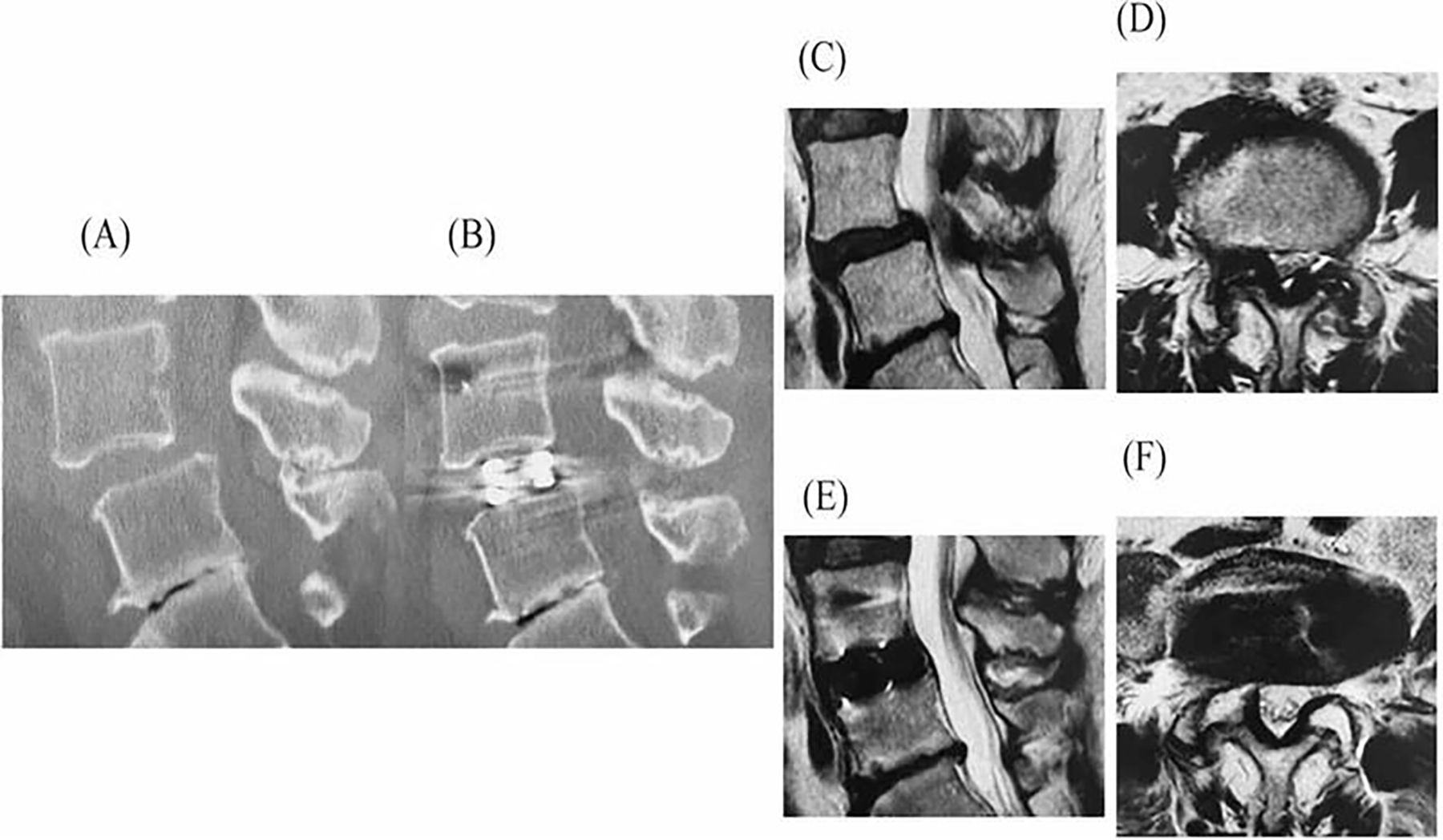
However, when examining changes in measurements (Δ), a significant correlation was observed between the change in PDH (ΔPDH) and the change in CCA (ΔCCA; r = 0.272, P = 0.017). This finding indicates that increases in PDH are associated with corresponding increases in CCA, suggesting that PDH may play a role in influencing spinal canal dimensions. Other measurements, including ΔADH, ΔAvDH, and ΔSL, did not show significant correlations with changes in ΔCCA, highlighting the complex relationship between DH and spinal canal dimensions. Figure 5 shows a typical case of LLIF with PPS using the expandable cage in this study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A 55-year-old woman underwent LLIF with PPS for L4 spondylolisthesis. Sagittal CT images before (A) and after surgery (B) are shown. Sagittal MRIs before surgery are shown in (C), and after surgery in (E), while axial MRIs before surgery are shown in (D), and after surgery in (F). Preoperative ADH, PDH, AvDH, and SL were 8.7, 5.8, 7.3, and 6.9 mm, respectively. The predicted values for ADH, PDH, AvDH, and SL were 11.0, 7.9, 9.5, and 9.8 mm, respectively. Postoperative CT showed actual ADH, PDH, AvDH, and SL measurements of 12.8, 9.5, 11.2, and 7.2 mm, respectively. While the DH was greater than predicted, the SL was smaller than expected. MRI revealed significant improvement in dural sac compression. Abbreviations: ADH, anterior disc height; AvDH, average disc height; CT, computed tomography; LLIF, lateral lumbar interbody fusion; MRI, magnetic resonance imaging; PDH, posterior disc height; PPS, percutaneous pedicle screw; SL, segmental lordosis.
Discussion
There is limited evidence regarding the use of expandable cages for indirect decompression with LLIF, and few studies have directly compared the clinical outcomes and imaging evaluations of expandable vs static cages. Among these, Frisch et al, in a prospective study of 56 patients who underwent LLIF, reported a higher subsidence rate in the static polyetheretherketone cage group (16.1% vs 0% in the expandable polyetheretherketone cage group). However, other radiologic indicators and clinical outcomes were similar between the 2 groups.28 Our previous short-term radiographic and clinical evaluation also demonstrated no significant differences in outcomes between static and expandable cages in LLIF without facet resection or other posterior techniques.14 Huo et al reported that the static cage group had a significantly higher subsidence rate and lower fusion rate compared with the expandable cage group. They also noted significant improvements in pain and quality of life in the expandable cage group compared with the static cage group.15 These findings suggest that while expandable cages may offer advantages in preventing CS, their overall effectiveness in achieving optimal clinical and radiologic outcomes remains uncertain and warrants further investigation.
Since LLIF achieves indirect decompression without resecting the posterior elements, the actual DH and SL may be less than anticipated. Thus, this study aimed to evaluate the discrepancies between predicted and actual DH and SL achieved in LLIF using expandable cages. The results revealed critical insights into the performance of expandable cages, particularly regarding their ability to restore DH and SL.
First, our findings demonstrate significant improvements in SL, ADH, PDH, and AvDH following LLIF surgery with expandable cages. The mean SL increased from 3.5° to 4.8° postoperatively, ADH increased from 5.9 to 10.7 mm, PDH from 3.4 to 7.7 mm, and AvDH from 4.6 to 9.2 mm. These improvements suggest that expandable cages effectively restore DH, which is crucial for proper spinal alignment and overall spinal function. Moreover, the significant increase in FA from 96.7 to 130.7 mm² indicates effective foraminal decompression, which is essential for relieving nerve compression.
However, a significant discrepancy was observed in SL when comparing actual postoperative measurements with predicted cage measurements. The actual postoperative SL was 4.8°, while the predicted cage SL was 8.7°, resulting in a significant difference of 3.9° (P < 0.001). This discrepancy indicates that while expandable cages can improve SL, achieving the predicted SL remains challenging. Such a performance gap may impact long-term clinical outcomes and highlight the need to consider factors beyond cage design in surgical planning. Furthermore, the measurements of the vertebral endplates, rather than the cage itself, underscore this discrepancy. Although the expansion of the cages is designed to correspond to a specific number of rotations, the lack of intraoperative measurements of cage expansion prevents a complete understanding of the reasons behind these discrepancies, representing a limitation of the current study.
Several factors may contribute to these discrepancies. First, while ADH, PDH, and AvDH measurements were consistent with predicted values due to the cages’ direct and controlled expansion mechanism, SL proved to be more variable. External forces, soft tissue tension, and the presence of osteophytes at the fusion segment may resist lordotic correction. Second, patient-specific anatomical characteristics, such as spinal morphology variations and degenerative changes in the posterior facet joints, may limit the cage’s ability to achieve the desired lordosis. In contrast, ADH, PDH, and AvDH may be less affected by these external factors, making them more predictable outcomes. Additionally, technical factors related to cage placement and the surrounding soft tissues’ biomechanics during and after surgery could further contribute to the observed discrepancy in SL.
Device-related factors, such as the material composition, design, and expansion mechanism of the cage, likely also play a role. For example, the reliability of the expansion mechanism, which relies on a specific number of rotations, may introduce variability when interacting with different patient anatomies. Future research should prioritize evaluating these device-related factors and optimizing cage designs to improve predictability.
The study found significant increases in CD and CCA postoperatively regarding canal dimensions. The mean preoperative CD increased from 5.0 to 8.3 mm, and the CCA increased from 55.8 to 89.7 mm². These findings indicate that LLIF with expandable cages effectively alleviates dural compression and enhances canal dimensions, contributing to better clinical outcomes. Interestingly, correlation analysis revealed a significant relationship between changes in PDH (ΔPDH) and changes in CCA (ΔCCA; r = 0.272, P = 0.017), suggesting that increases in PDH are particularly associated with improved canal dimensions, emphasizing the importance of PDH in achieving optimal decompression.
Moreover, the average hospital stay in this study was 15.5 ± 4.1 days, which is longer than typical durations reported for lumbar fusion surgeries in other regions. This is influenced by factors specific to Japan’s health care system, where the national insurance covers extended hospitalization for thorough postoperative monitoring and rehabilitation. The high mean age of the patients (70.6 years) also contributes, as elderly caregiving by other elderly individuals is a societal challenge, and discharge is often delayed until patients regain sufficient mobility. These unique health care and societal factors explain the extended hospitalization observed in this study.
The observed discrepancy between predicted and actual SL is concerning, as it may significantly affect long-term patient outcomes. Inadequate restoration of SL may lead to suboptimal spinal alignment, which can, over time, contribute to accelerated degeneration of adjacent segments, increased stress on posterior elements, and the potential for persistent or recurrent symptoms, such as low back pain or radiculopathy. Moreover, failure to achieve the expected SL might reduce the efficacy of indirect decompression, increasing the risk of residual neural compression.29 This, in turn, could compromise the overall success of the surgery, leading to a need for revision procedures due to indirect decompression failure.30,31
Our analysis highlighted that preoperative PDH was the most influential preoperative parameter for predicting postoperative SL, suggesting that greater emphasis on preoperative assessment of PDH might improve surgical outcomes. This insight provides a foundation for more tailored surgical planning and patient selection in future cases. Achieving the predicted SL is not merely a matter of surgical precision but is also a critical factor in ensuring the long-term success of LLIF procedures. Therefore, further refinement of surgical techniques and cage design is needed to enhance the predictability and accuracy of LLIF outcomes.
Future research should include larger sample sizes to evaluate the factors contributing to this discrepancy and explore whether adjustments in surgical techniques or cage design could mitigate these risks. Additionally, long-term follow-up studies are necessary to determine whether SL discrepancies result in clinically significant differences in patient outcomes over time. This study’s retrospective design and relatively small sample size are limitations. Prospective studies with larger cohorts are needed to validate these results and provide more robust evidence. Such studies should identify specific patient characteristics and technical factors influencing success and guide future surgical strategies.
Conclusions
Expandable cages in LLIF significantly improved DH and contribute to enhanced canal dimensions, which are associated with favorable clinical outcomes. The observed significant increase in FA further emphasizes the effectiveness of expandable cages in achieving indirect decompression, providing relief from nerve compression. However, achieving the ideal SL remains challenging, with an apparent discrepancy between predicted and actual SL values. This discrepancy is likely due to patient-specific anatomical characteristics (e.g., spinal morphology and degenerative changes in the facet joints), surgical technique, and the biomechanical behavior of the spine. Our findings underscore the critical need to address the variability in SL outcomes, as inadequate lordosis restoration may compromise long-term spinal stability and lead to adverse clinical sequelae.
Therefore, further improvements in the design of expandable cages and surgical techniques are necessary. Future research should focus on evaluating the impact of these discrepancies on long-term clinical outcomes. Additionally, prospective studies should explore whether preoperative parameters, such as PDH, can be optimized to achieve better postoperative results, and how advancements in cage technology can improve outcome predictability.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was conducted by ethical standards and received approval from the Ethics Committee and the Profit Reciprocity Committee (reference number 24R-084).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.