


ABSTRACT
Background: Anatomic variation in the relationship between the lumbar spine and sacrum was first described in the literature nearly a century ago and continues to play an important role in spine deformity, low back pain (LBP), and pelvic trauma. This review will focus on the clinical and surgical implications of abnormal lumbosacral anatomy in the context of sacroiliac joint (SIJ) disease, spine deformity, and pelvic trauma.
Methods: A PubMed search using the keywords “lumbosacral transitional vertebrae,” “LSTV,” “transitional lumbosacral vertebrae,” “TLSV,” and “sacral dysmorphism” was performed. The articles presented here were evaluated by the authors.
Clinical Significance: The prevalence of LSTV varies widely in the literature from 3.9-% to 35.6% in the spine literature, and sacral dysmorphism is described in upwards of 50% of the population in the trauma literature. The relationship between LSTV and LBP is well established. While there is no agreed-on etiology, the source of pain is multifactorial and may be related to abnormal biomechanics and alignment, disc degeneration, and arthritic changes.
Surgical Implications: Understanding abnormal lumbosacral anatomy is crucial for preoperative planning of SIJ fusion, spine deformity, and pelvic trauma surgery. LSTV can alter spinopelvic parameters crucial in planning spine deformity correction. Traditional safe zones for sacroiliac screw placement do not apply in the first sacral segment in sacral dysmorphism and risk iatrogenic nerve injury.
Conclusions: LSTV and sacral dysmorphism are common anatomic variants found in the general population. Abnormal lumbosacral anatomy plays a significant role in clinical evaluation of LBP and surgical planning in SIJ fusion, spine deformity, and pelvic trauma. Further studies evaluating the influence of abnormal lumbosacral anatomy on LBP and surgical technique would help guide treatment for these patients.
- lumbosacral transitional vertebrae
- LSTV
- sacral dysmorphism
- transitional lumbosacral vertebrae
- low back pain
- Bertolotti syndrome
- sacroiliac joint fusion
INTRODUCTION
Anatomic variation in the relationship between the lumbar spine and sacrum was first described in the literature almost a century ago and continues to play an important role in spine deformity, low back pain (LBP), and pelvic trauma.1,2 As the indications for posterior pelvic screw fixation have expanded, the recognition of sacral dysmorphism as an important consideration has grown. Additionally, the understanding of the importance of lumbosacral transitional vertebrae (LSTV) in spine mechanics and surgical fixation has evolved. LSTV are a congenital anomaly and common anatomic variant that occurs when there is partial or complete fusion between the final lumbar vertebra and first sacral segment. Lumbarization of the first sacral segment occurs with separation, either partial or complete, of S1 from the rest of the sacrum, creating a sixth lumbar vertebra. Sacralization of the last lumbar vertebra occurs when the last lumbar vertebra is incorporated into the sacrum, resulting in 4 lumbar vertebrae.3 Sacralization of L5 (7.5%) is slightly more common in the general population compared with lumbarization of S1 (5.5%).4
Genetic factors may play a role in the development of LSTV. Hox genes (Hox-10, Hox-11) have been found to play a significant role in the process of vertebral body segmentation and development.5 The development of vertebral bodies and disc formation occurs during the fourth week of embryonic development; however, the process by which the vertebrae consolidate and fuse into adult lumbosacral anatomy occurs through the fourth decade of life.6 The relative number of lumbar and sacral segments is influenced by load transmission through the lumbosacral region during development and is associated with the bipedal evolution of humans.3,7
CLASSIFICATION AND PREVALENCE
The spectrum of anatomic variation in this population was described by Castellvi et al8 in 1984 (Figure 1). Using radiographs, the authors classified 7 different patterns of transitional vertebrae into 4 types based on morphology (types I–IV) and 2 variations based on laterality (for types I–III, A = unilateral and B = bilateral). Type I, also known as a dysplastic transverse process, is a large transverse process triangular in shape with dimensions measuring at least 19 mm in rostrocaudal width. Type II, or incomplete lumbarization/sacralization, is a large transverse process that follows the contour and articulates with the sacrum but is not fused, creating a diarthroidal joint between the final lumbar vertebra and the first sacral segment (Figure 2). Type III, or complete lumbarization/sacralization, is a large transverse process with bony fusion to the sacrum (Figure 3). Type IV exhibits lumbarization/sacralization that is incomplete (type II) on one side and complete (type III) on the contralateral side.

Castellvi–Chan classification system of lumbosacral transitional anatomy.
Image reprinted with permission from Castellvi et al.8

Castellvi–Chan type IIB lumbosacral transitional vertebra identified on pelvis outlet view radiograph.

(A) Castellvi–Chan type IIIA and (B) Castellvi–Chan type IIIB lumbosacral transitional vertebra identified on pelvis outlet view radiographs.
O'Driscoll et al9 developed a classification system based on T1- and T2-weighted magnetic resonance imaging (MRI) and the disc morphology between the uppermost sacral segment and the remainder of the sacrum. Type 1 describes no disc material present. Type 2 has small residual disc that does not extend the whole diameter from anterior to posterior. Type 3 has a well-formed disc extending the entire anteroposterior (AP) diameter of the sacrum. Type 4 has a well-formed disc extending the entire AP diameter of the sacrum and an associated abnormal upper sacral segment. The authors found good association between type 4 on MRI and fused LSTV on radiographs.
Sacral dysmorphism has been described in the orthopedic trauma literature more recently. Miller and Routt6 described several important findings on pelvic radiographs of sacral dysmorphism. The 7 characteristics may be present to varying degrees and include (1) collinearity of the upper portion of the sacrum and iliac crests on the outlet radiograph, (2) presence of mammillary bodies at the sacral ala on outlet radiograph, (3) noncircular anterior sacral foramina on outlet radiograph, (4) residual upper sacral disks on lateral radiograph, (5) tongue-and-groove sacroiliac joint surface on axial computed tomographic (CT) scan, (6) cortical indentation of the ala on the inlet radiograph, and (7) acute alar slope on the lateral radiograph (Figures 4 and 5). The subtler findings may be better appreciated on CT of the pelvis.

Mammillary bodies and abnormal sacral neural exit present in the uppermost sacral segment of a dysmorphic sacrum.
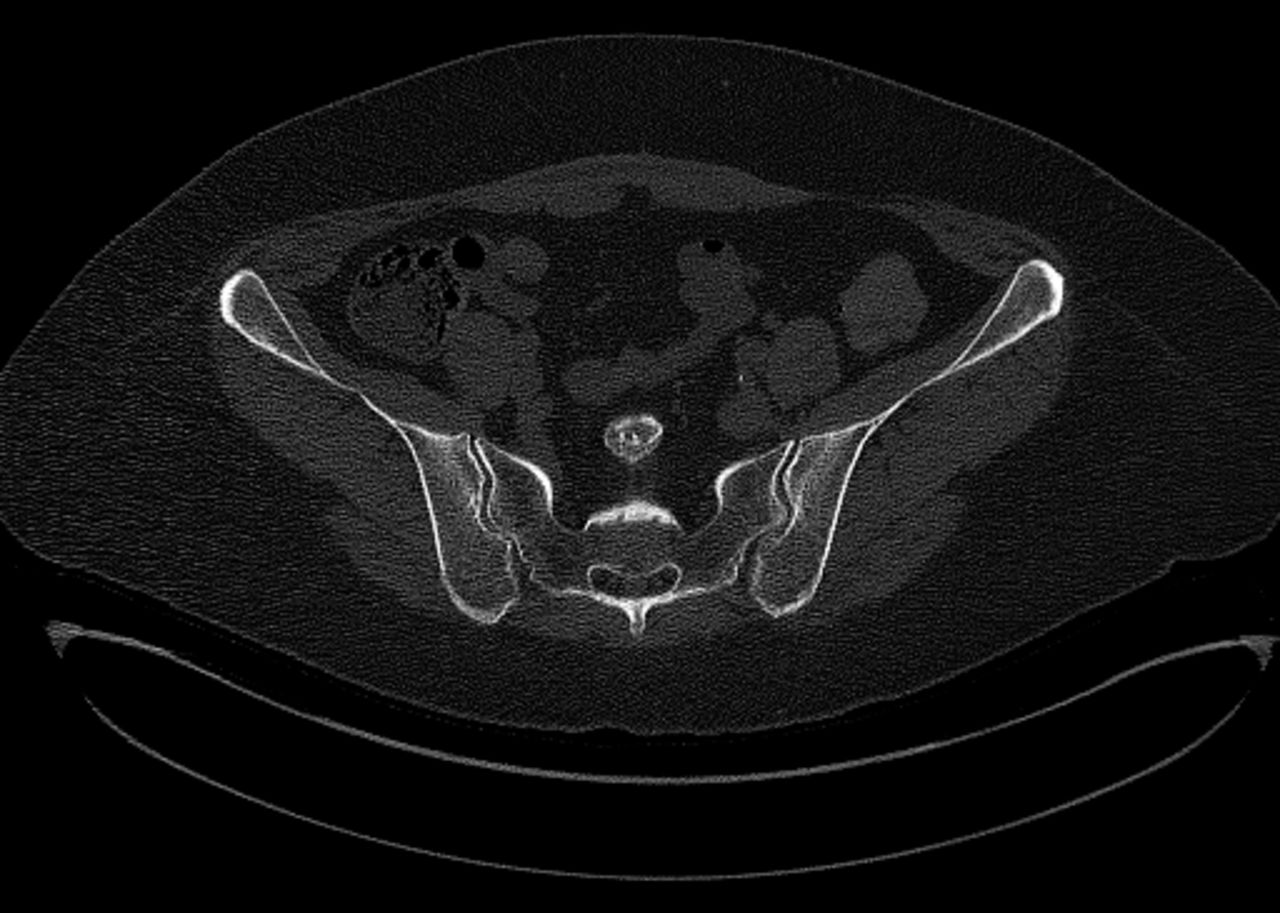
Tongue-and-groove sacroiliac joint surface of sacral dysmorphism identified on CT scan.
The prevalence of LSTV in the general population varies significantly in the literature, ranging from 4% to 35.6% in the spine literature.2,4,8,10–16 Nardo et al14 evaluated radiographs of 4636 participants and determined the overall prevalence of LSTV to be 18.1%, with types I and II comprising nearly 80% of LST. The authors also found a significantly higher rate in men compared to women (28.1% vs 11.1%). Apazidas et al11 reported the highest rate of LSTV at 35.6% and determined the prevalence of each of the Castellvi–Chan classification groups; type IA was most common at 14.7%. The prevalence of sacral dysmorphism described in the trauma literature is estimated to be upwards of 50% (Table 1).13,17
Incidence of lumbosacral transitional vertebrae or sacral dysmorphism.
CLINICAL SIGNIFICANCE
LSTV and sacral dysmorphism result in distinct anatomic changes at the lumbosacral junction and in the surrounding structures. Mahato18 found that LSTV articulations at L5–S1 were associated with increased lordotic curves, L5 vertebral heights, and pedicle and angular dimensions. Furthermore, L5–S1 fusions were associated with smaller disc heights, wider and shorter L5 pedicles, narrower and taller transverse processes, and straighter spines overall. According to Mahato19, sacralization reduces S1 pedicle height and sagittal angulation of the pedicles while increasing the downward slope. Lumbarization was associated with more obtuse pedicles in the sagittal plane and a smaller length between the facet and sacral promontory. The anatomic variations may affect spinal instrumentation at this level and must be taken into consideration with regard to preoperative planning.
Mechanical LBP is one of the most common musculoskeletal concerns. LBP has been associated with sacroiliac dysfunction as well as LSTV. The association between LSTV and LBP was first established in 1917 by Mario Bertolotti20 and is known as Bertolotti syndrome. Tang et al15 found a significant relationship between LSTV and low back and buttock pain. The authors demonstrated odds ratios of 2.56 and 4.28 for LBP and 5.38 and 6.82 for gluteal pain in Castellvi–Chan types II and IV LSTV, respectively. While the exact mechanism is not understood, many studies have suggested that pain may be related to degeneration of the adjacent disc segments and facet joints due to hypermobility and increased forces at the level just cephalad to the transitional segment.12,16,21,22 As described previously, Mahato18 demonstrated numerous ways in which LSTV affects the load-bearing mechanics of the lumbosacral spine and contributes to mechanical LBP, including hypolordosis associated with L5–S1 fusion and hyperlordosis associated with L5–S1 articulation. Farshad-Amacker et al23 demonstrated a protective effect for the disc at the transitional segment and increased degenerative changes at the adjacent cephalad disc, particularly for Castellvi–Chan types III and IV LSTV. The relationship between LSTV and disc degeneration was further evaluated by Ahn et al,22 who determined that patients with LSTV undergoing microdiscectomy have clinically worse outcomes compared to those with “normal” lumbosacral anatomy. Illeez et al12 evaluated the relationship between LSTV and sacroiliac joint dysfunction and LBP in 700 subjects. The authors found statistically significant associations between LSTV and sacroiliac dysfunction (28.5%) and between LSTV and LBP (26%). While the disc adjacent to the LSTV may experience increased stresses leading to degenerative change, the relative segmental innervation is unchanged in patients with sacral lumbralization compared to those with 5 lumbar vertebral bodies based on electromyographic findings.24,25
SURGICAL IMPLICATIONS
LSTV has implications in the preoperative planning for surgical correction in spine deformity cases. Spinal correction surgery depends on accurate measurements of spinopelvic and global spinal parameters. A number of these parameters rely on the accurate identification of the sacral endplate and may be influenced by the relative height and translation of the sacral endplate. In patients with LSTV, the identification of the sacral endplate may not be entirely clear around the transitional segment. Zhou et al25 measured these spinal parameters for patients with Castellvi–Chan types III and IV LSTV using both the cephalad and the caudal segments as the sacral endplate. The authors found that the pelvic incidence (PI) differed by ∼20° between cephalad and caudal. Most of the parameters measured, including PI, lumbar lordosis (LL), PI–LL mismatch, pelvic tilt, sacral slope, sagittal vertical axis, and T1–pelvic angle, demonstrated significant differences between cephalad and caudal measurements. Thoracic kyphosis and spinal inclination (T1SPi) were not affected by cephalad and caudal positioning of the sacral endplate. The significant differences in the measurements may have adverse effects on the preoperative surgical planning for spine deformity cases. Furthermore, Khalsa et al26 found significant variability between surgeons in assessing spinopelvic parameters in patients with LSTV. While there are not yet standardized measures or agreed-on alignment goals for patients with LSTV, the variations caused by the deformity must be taken into consideration and play an important role in preoperative planning.
Pelvic ring injuries can cause widening of the sacroiliac joint or a sacral fracture, and treatment typically involves percutaneous reduction methods and fixation. The treating surgeon must understand the safe zones for screw placement in normal anatomy in order to avoid the risk of iatrogenic damage to nerves traversing through the sacral neural tunnels. Additionally, sacroiliac joint fusion utilizes similar safe zones in the placement of implants. Normal anatomy exhibits bilateral, ellipsoid, osseous areas bounded cranial-anteriorly by sacral alar cortical bone and caudal-posteriorly by first sacral neural tunnel. The most constrained area is between the sacral ala and the first sacral neural tunnel. On a true lateral radiograph, screw trajectory caudal and posterior relative to the sacral ala is important in order to avoid injury to the L5 nerve root.6
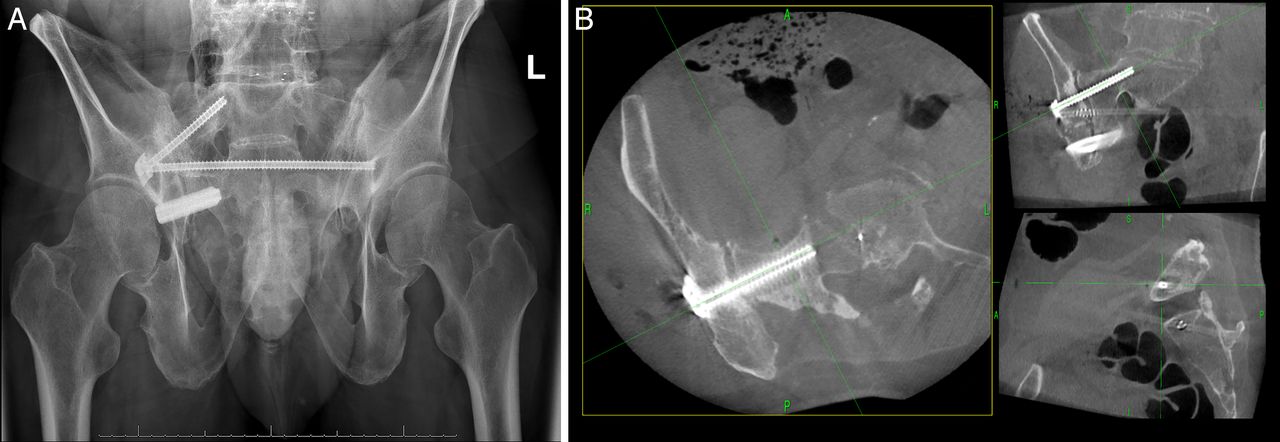
A dysmorphic sacrum has a distorted, misshapen, and ellipsoid upper sacral segment that limits the area available for screw placement. Oblique dysmorphic alar osteology makes transiliac, transsacral screw fixation unavailable in S1. The preferred safe zone for a sacroiliac screw in S1 is oblique from caudal to cranial and posterior to anterior, and there is not a safe corridor for horizontal screw placement in the AP plane. Alternatively, the safe zone is similar to normal in the S2 segment and is amenable to transiliac, transsacral screw (Figure 6). Preoperative evaluation of the pelvic CT scan is important in planning the appropriate sacral segments and trajectories for safe percutaneous instrumentation. In addition, intraoperative CT navigation may be useful in avoiding potential complications for patients with sacral dysmorphism requiring SIJ fusion or posterior pelvic ring fixation.27

The dysmorphic first sacral segment did not allow for a transiliac, transsacral screw at this level, as was used at S2.
Footnotes
Disclosures and COI: Each author certifies that he or she has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted work. This paper is exempt from institutional review board review, as it is not human subjects research. There was no external source of funding for this study.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.