


Abstract
Background Multifidus muscle degeneration and atrophy have been demonstrated following traditional open spine surgery. The purpose of this study was to quantify multifidus muscle atrophy and fatty infiltration following a 1-level minimally invasive (MIS) lumbar discectomy.
Methods Magnetic resonance imaging (MRI) of 24 patients who underwent a primary 1-level MIS microdiscectomy were reviewed. Demographics, operative levels, and time from surgery to imaging were assessed. Total and lean cross-sectional areas (CSA), T1-signal intensity ratio between the multifidus and psoas muscles, and lean-to-total CSA ratio were measured. Pre- and postoperative values were compared within each patient utilizing paired sample T-tests.
Results The mean age was 47.8±14.2 years. MRI was obtained 182.5±194.4 days following index surgery. On the ipsilateral side, total CSA decreased at the index level (-4.9%) and the lean CSA decreased at the index (-6.2%), inferior pedicle (-13.0%), and inferior disc levels (-18.6%). On the contralateral side, no significant decreases in total or lean CSA were demonstrated. T1-signal intensity ratios increased at all levels, but the differences were not statistically significant. The lean-to-total CSA ratio was decreased at the superior disc (-5.2%), inferior pedicle (-8.4%), and inferior disc levels (-17.2%) on the ipsilateral side and at the contralateral inferior disc level (-5.3%).
Conclusions Primary 1-level MIS discectomy results in minimal short-term atrophy and fatty infiltration of the multifidus at the index level. Total CSA atrophy was mainly confined to the ipsilateral side at the index level. Lean CSA atrophy was observed mainly at and below the index level on the ipsilateral side. Fatty infiltration, as measured by the lean-to-total CSA ratio, ranged 1.2-17.2% on the ipsilateral and 0-5.3% on the contralateral side with greater fat content demonstrated caudally to the surgical level.
Clinical Relevance Overall, the majority of the multifidus muscle appears to be radiographically preserved following an MIS lumbar discectomy.
- Multifidus atrophy
- multifidus fat infiltration
- T1 signal intensity
- MRI multifidus
- paraspinal atrophy
- minimally invasive multifidus
Introduction
The multifidus is a part of the deeper paramedian layer of paraspinal muscles that runs along the thoracolumbar spine. Many regard it to be the primary stabilizer of the lower lumbar spine.1, 2 The anatomy of the multifidus muscle is complex with growing research interests in its normal physiology as well as its pathologic states.3, 4 Specifically, the association between multifidus degeneration and chronic low back pain, degenerative disc disease, radiculopathy, and scoliosis have been demonstrated.5–9 Traditional midline posterior lumbar surgery remains a common means of spinal decompression and stabilization despite well-demonstrated bilateral atrophy and fatty degeneration of the paraspinal muscles.10, 11 These changes result in decreased biomechanical capacity of the trunk and potentially unfavorable long-term clinical outcomes.12–14
A fundamental principle of minimally invasive surgery (MIS) is to reduce approach-related damage to the multifidus via muscle splitting techniques utilizing tubular retractors. Potential clinical benefits include decreased blood loss, pain, length of stay, and incidence of infection.15, 16 There are limited studies that quantify in detail changes in the multifidus after MIS techniques.17–20 With the increased availability of high-resolution magnetic resonance imaging (MRI), non-invasive and reproducible cross-sectional information regarding the multifidus size and content can be studied in greater detail. The purpose of the current study is to quantify the atrophy and fatty infiltration of the multifidus muscle following a 1-level MIS lumbar decompression.
Materials and Methods
Patient Population
Institutional review board approval was obtained (ORA # 14051301). Patients who underwent MRI before and after primary 1-level MIS lumbar microdiscectomy by either of two fellowship-trained spine surgeons at a single institution were identified. Exclusion criteria included revision surgery, fusions, and irrigation/debridement for infections. Indications for postoperative imaging included either new onset or recurrent radicular symptoms.
Surgical Techniques
Common MIS microdiscectomy techniques have been described.21 The following surgical technique was utilized for all cases of primary procedures. The patient was placed in the prone position on a Jackson table. Fluoroscopy was utilized to identify and confirm the target level. A 1-2 cm incision was made lateral to the midline at the level of interest. Sequential dilation was performed until an 18 mm tubular retractor was placed as a surgical working channel. A burr and Kerrison rongeur were utilized to perform a hemilaminotomy of the superior lamina over the target disc space. The ligamentum flavum was resected and the traversing nerve root was identified and safely retracted medially. The disc space was localized and incised. Pituitary rongeurs were then utilized to perform the discectomy.
Imaging Analysis
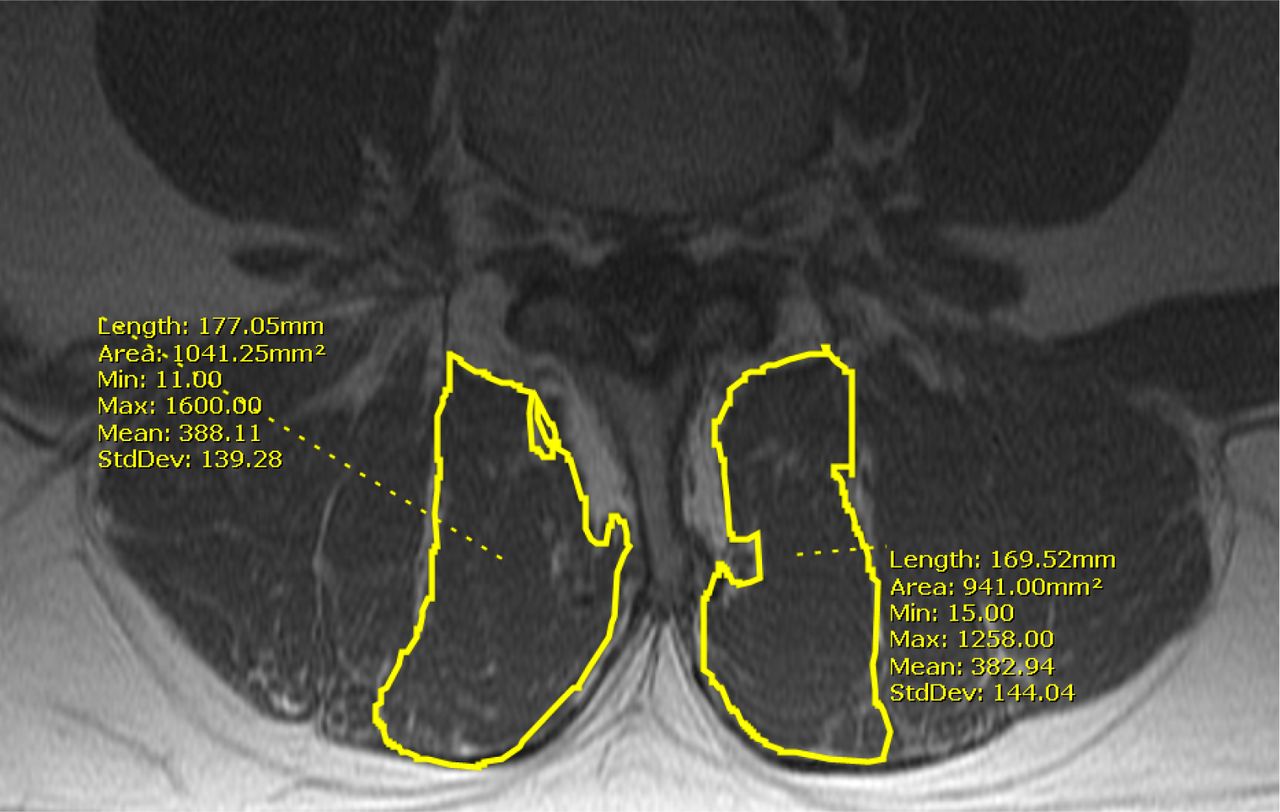
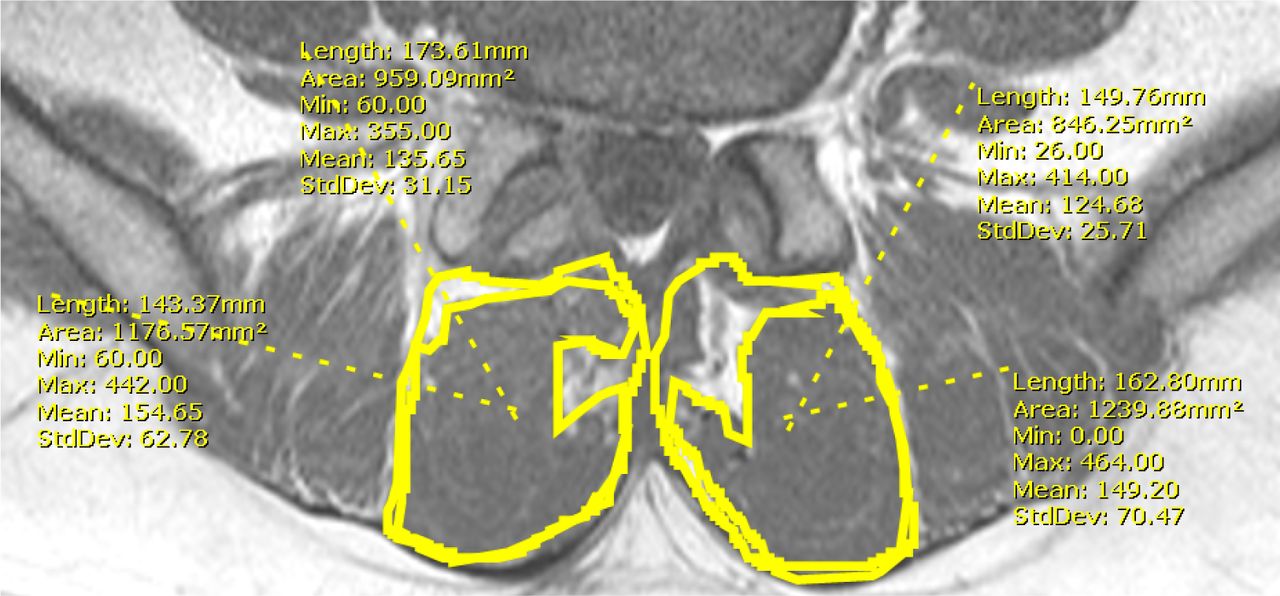
In order to minimize radiographic artifact, all postoperative MRIs utilized a 3.0 Tesla machine. Measurements were performed with the institution's image viewing software (Opal, Viztek, Garner, NC). Measurements included the total cross-sectional area (CSA), lean CSA, T1 signal intensity, ratio of lean-to-total CSA, and ratio of T1 signal intensity between the multifidus and psoas muscles. Atrophy was measured utilizing CSA measurements (mm2) of the multifidus muscle using the axial T1-weighted sequences. The mean T1 signal intensity was quantified utilizing a grayscale histogram software with higher scores signifying greater intensity. The T1 signal intensity ratio between the multifidus muscle and the psoas muscle at each level were obtained and recorded. The ratio of lean-to-total CSA was utilized as an additional measurement of fatty infiltration as described in rotator cuff research.22 The measurements were performed at the ipsilateral and contralateral sides in reference to the surgical level and laterality. Measurements were made at the disc level above (supra disc), pedicle level above (supra pedicle), operative level (index), pedicle level below (infra pedicle), and the disc level below (infra disc) (Figure 1, Figure 2).

41 year-old male presents with a herniated nucleus pulposus at L4-5. Preoperative axial T1-weighted MRI image demonstrates lean cross-sectional area measurements at the index level (L4-5).
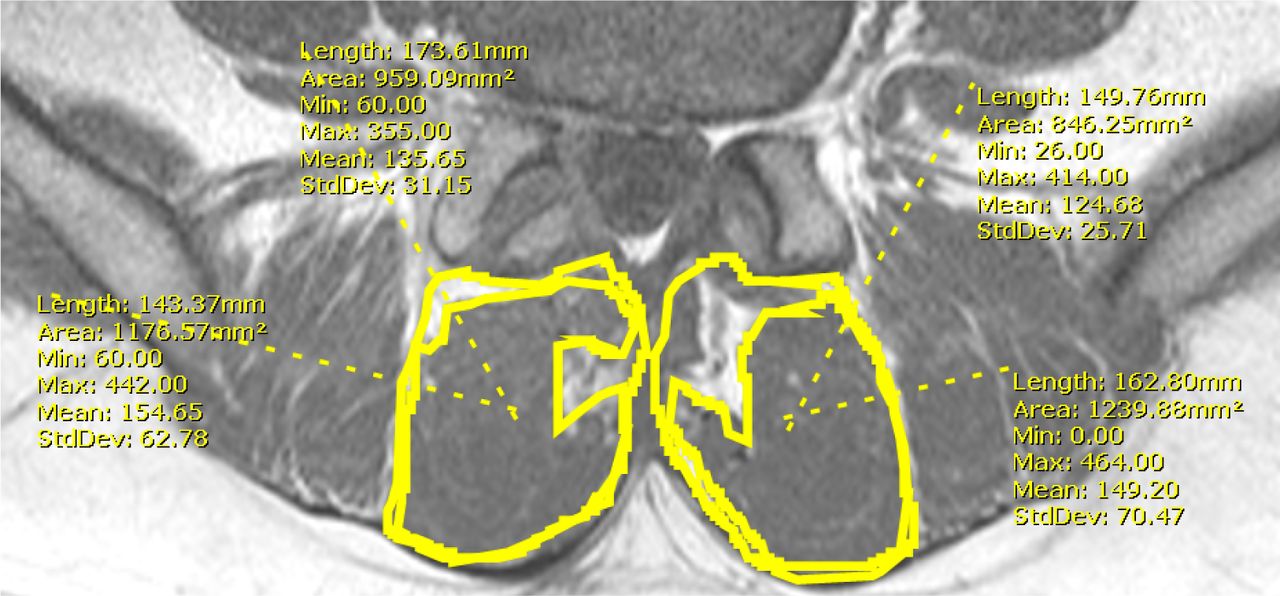
Postoperative axial T1-weighted MRI image demonstrates total and lean cross-sectional measurements at the index level (L4-5).
Statistical Methods
Statistical analysis was performed utilizing a paired sample T-test. A p-value of <0.05 denoted statistical significance.
Results
Of the 24 patients included in the study, 14 were female and the mean age was 47.8±14.2 years. Demographics of the patient population are detailed in Table 1. Overall, the majority of patients underwent single-level decompression for radiculopathy at the L45 (58.3%, n = 14) or L5S1 (25.0%, n = 6) disc level. Preoperative MRI was obtained at a mean of 2 months prior to the surgery while postoperative MRI was obtained at a mean of 6 months following surgery (Table 1).
Patient Characteristics, Operative Levels, and Timing for Primary 1-level MIS Lumbar Decompression.
MRI-Documented Changes in Multifidus Muscle Following Primary 1-Level MIS Lumbar Decompression.
On the ipsilateral side, the total and lean CSA were significantly decreased at the index level by 4.9% (p < 0.01) and 6.2% (p < 0.05), respectively. In addition, the lean CSA was significantly decreased at the inferior pedicle (-13.0%, p < 0.01) and the inferior disc levels (-18.6%; p < 0.01; Table 2. On the contralateral side, a decrease in the lean CSA at the index level was demonstrated, but was not statistically significant (Table 2).
The lean-to-total CSA ratios were significantly decreased at the superior disc (-5.2%, p < 0.05), inferior pedicle (-8.4%, p < 0.01), and the inferior disc levels (-17.2%, p < 0.001) on the ipsilateral side (Table 2). On the contralateral side, the lean-to-total CSA ratio was significantly decreased by 5.3% at the inferior disc level (p < 0.05; Table 2.
The T1 signal intensity ratios were increased at all levels following surgery with greater changes observed caudal to the microdiscectomy on the ipsilateral side. However, no significant differences were demonstrated in the T1 signal intensity ratios at any level (Table 2).
Discussion
Traditional open approaches to the lumbar spine are known to result in atrophy of the multifidus muscle.10, 11 Published studies regarding multifudus muscle degeneration and fatty infiltration following MIS techniques have been limited. A study by Bresnahan et al demonstrated a significant increase in the paraspinal muscle cross sectional area on MRI in patients who underwent an MIS decompression.17 Although the imaging analysis was blinded, the results of postoperative paraspinal muscle hypertrophy were counterintuitive.
Fan et al compared the atrophy in the multifidus muscle in patients who underwent either an MIS or open posterior lumbar interbody fusion (PLIF).18 The authors demonstrated significantly lower multifidus muscle atrophy in the MIS cohort as compared to the open cohort.18 However, the indications for PLIF ranged from spondylolisthesis to large lumbar disc herniations.18 Similarly, Min et al demonstrated significantly decreased multifidus muscle degeneration following minimally invasive lumbar fusion when compared to open techniques.20 However, the open patients underwent either a PLIF or a postero-lateral lumbar fusion (PLF) while all MIS patients underwent a transforaminal lumbar interbody fusion (TLIF).20 As such, the purpose of this study was to rigorously quantify the multifidus muscle degeneration and fatty infiltration following a MIS lumbar mi crodiscectomy as demonstrated on MRI utilizing each patient as his or her own control.
The current study was able to quantify the anatomic changes to the multifidus muscle at an average of 6 months following a primary 1-level MIS lumbar de compression. Atrophy, as determined by the change in total CSA, was minimal and isolated to the index level. The lean CSA decreased most significantly at and below the index level, while fatty infiltration (as measured by the lean-to-total CSA ratio) increased at the adjacent levels. Additionally, a pattern of increasing atrophy and fatty infiltration caudal to the site of surgical intervention was demonstrated in the ipsilateral lean CSA and lean-to-total CSA ratio.
Although fatty degeneration, as measured by the T1 signal intensity ratio, demonstrated substantial percent change following surgery, no statistical significant differences were demonstrated between pre- and postoperative values. Recently, Zhi-Jun et al as sessed the accuracy of this measurement in a rat model.23 The Pearson correlation coefficient demonstrated high correlation between T1 intensity ratios and histological fat scores (r = 0.804).23 Despite these findings, the current study only demonstrated a trend in postoperative T1 intensity ratio changes. This finding may be due to the wide range of values over a proportionally smaller surgical area attributed to MIS techniques in humans as compared to open multi-level techniques in a rat model.23
Other studies have focused on T2 intensity ratios as an accurate reflection of multifidus muscle disruption.19, 24 T2 signal intensity ratio measurements appear to be a better reflection of muscle edema and in flammation. These studies differ from the current study in that the analysis was performed on patients who had undergone open procedures with short-term follow up. In our analysis, the average postoperative imaging was obtained 6 months after surgery, which may have been well into the fibrotic regenerative stage of the injury response minimizing the post-surgical changes potentially observed on T2 imaging.
Fatty infiltration, as determined by the lean-to-total CSA ratio, demonstrated post-surgical changes in the current study. Given the variability in the shape and CSA of the multifidus muscle between patients, it appears intuitive that this ratio more accurately reflects true amount of fatty infiltration. Currently, there is insufficient evidence regarding the utility of the CSA ratio and its validity and reproducibility should be the subject of future research. Neverthe-less, this pattern of fatty infiltration does support previous studies regarding the complex anatomy and innervation of the multifidus muscle.3, 4 In addition, theses results are favorable when compared to data regarding paraspinal anatomy after traditional open posterior approaches.11, 19
Despite small heterogeneous patient populations18, 20 and some counterintuitive results17, studies comparing changes to paraspinal musculature between open and MIS procedures have consistently favored MIS techniques. Bresnahan et al compared the paraspinal CSA in a cohort of 18 patients (9 undergoing open vs. 9 undergoing microendoscopic decompression). At an average of 16 months, the open patients demonstrated an average decrease in CSA of 5.4% while the microendoscopic decompression of steno sis (MEDS) grouped CSA ironically increased by 9.9%.17
There are clear limitations to the current study. First, the sample size was relatively small, which may have contributed to the lack of statistical significance when comparing pre- and postoperative T1 signal intensity ratios. However, consistent differences were detected across all measurements. In addition, to the best of our knowledge, the current study is the largest radiographic analysis of patients undergoing primary MIS microdiscectomies. Second, no clinical correlations were made with the radiographic findings. As such, the clinical significance of these radiographic changes cannot be ascertained. Third, although the pre- and postoperative measurements were compared with each patient operating as their own control in the paired sample T-test, the study may have benefited from a control group that included patients undergoing open decompression procedures. Additionally, the date of the pre- and postoperative imaging was not standardized and varied be tween patients. Changes demonstrated in the postoperative imaging may have been independent of the procedure and potentially due to the timing of the postoperative imaging. In addition, two surgeons performed the surgeries potentially introducing some intra-operative variability amongst differing MIS techniques. Lastly, the authors of the study matched the MIS patients to those patients who underwent an open approach lumbar microdiscectomy according to age, operative levels, and timing to imaging relative to the index surgery. However, due to the great variability of the cross-sectional area measurements in the open microdiscectomy patients, no adequate comparison could be performed between open and MIS patients.
In summary, the findings of the current study suggest primary 1-level MIS microdiscectomy results in minimal atrophy and fatty infiltration to the multifidus muscle at the index level on the ipsilateral side of the intervention. Atrophy, as measured by the lean CSA at the index level on the ipsilateral side, ranged from 2.9-18.6% with increasing atrophy demonstrated caudal to the index level. Fatty infiltration (best represented by the decrease in the lean-to-total CSA ratio) increased by 1.2% at the index level on the ipsilateral side. However, more profound fatty infiltration was demonstrated caudally toward the inferior disc level, which increased by 17.2% and 5.3% on the ipsilateral and contralateral sides, respectively.
Disclosures
The authors declare no relevant financial disclosures.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Qualitative Evaluation of Paraspinal Musculature After Minimally Invasive Lumbar Decompression: A Prospective Study
- Clinical utility and reproducibility of surface electromyography in individuals with chronic low back pain: a protocol for a systematic review and meta-analysis
- Magnetic Resonance Imaging Documentation of Approach Trauma With Lumbar Endoscopic Interlaminar, Translaminar, Compared to Open Microsurgical Discectomy
- Minimal Clinically Important Difference in Patient-Reported Outcome Measures with the Transforaminal Endoscopic Decompression for Lateral Recess and Foraminal Stenosis