


ABSTRACT
Background: Full-body stereographs for adult spinal deformity (ASD) have enhanced global deformity and lower-limb compensation associations. The advent of age-adjusted goals for classic ASD parameters (sagittal vertical axis, pelvic tilt, spino-pelvic mismatch [PI-LL]) has enabled individualized evaluation of successful versus failed realignment, though these remain to be radiographically assessed postoperatively. This study analyzes pre- and postoperative sagittal alignment to quantify patient-specific correction against age-adjusted goals, and presents differences in compensation in patients whose postoperative profile deviates from targets.
Methods: Single-center retrospective review of ASD patients ≥ 18 years with biplanar full-body stereographic x-rays. Inclusion: ≥ 4 levels fused, complete baseline and early (≤ 6-month) follow-up imaging. Correction groups generated at postoperative visit for actual alignment compared to age-adjusted ideal values for pelvic tilt, PI-LL, and sagittal vertical axis derived from clinically relevant formulas. Patients that matched exact ± 10-year threshold for age-adjusted targets were compared to unmatched cases (undercorrected or overcorrected). Comparison of spinal alignment and compensatory mechanisms (thoracic kyphosis, hip extension, knee flexion, ankle flexion, pelvic shift) across correction groups were performed with ANOVA and paired t tests.
Results: The sagittal vertical axis, pelvic tilt, and PI-LL of 122 patients improved at early postoperative visits (P < .001). Of lower-extremity parameters, knee flexion and pelvic shift improved (P < .001), but hip extension and ankle flexion were similar (P > .170); global sagittal angle decreased overall, reflecting global postoperative correction (8.3° versus 4.4°, P < .001). Rates of undercorrection to age-adjusted targets for each spino-pelvic parameter were 30.3% (sagittal vertical axis), 41.0% (pelvic tilt), and 43.6% (PI-LL). Compared to matched/overcorrections, undercorrections recruited increased posterior pelvic shift to compensate (P < .001); knee flexion was recruited in undercorrections for sagittal vertical axis and pelvic tilt; thoracic hypokyphosis was observed in PI-LL undercorrections. All undercorrected groups displayed consequentially larger global sagittal angle (P < .001).
Conclusions: Global alignment cohort improvements were observed, and when comparing actual to age-adjusted alignment, undercorrections recruited pelvic and lower-limb flexion to compensate.
Level of Evidence: 3
- adult spinal deformity
- age-adjusted alignment
- compensatory recruitment
- full-body radiographs
- global spinal alignment
INTRODUCTION
Correspondence between key radiographic parameters—sagittal vertical axis (SVA), pelvic tilt (PT), lumbo-pelvic mismatch (PI-LL)—and disability measures has resulted in advancements in complex adult spinal deformity (ASD) assessments; optimization of these parameters has consequently resulted in meaningful clinical improvements.1–6 These relationships have standardized clinical targets to guide surgical decision making, as prescribed by the Scoliosis Research Society–Schwab ASD classification.7 Recent studies, however, have demonstrated that pathophysiological factors of age, bone mineral density, and comorbidity status mitigate the generalized applicability of predetermined realignment targets to individual deformities. Instead of one surgical solution for all, a tailored approach specified to a single patient for ideal alignment may be more appropriate for successful correction.8
Execution of preoperative plans requires a thorough understanding of a patient's sagittal profile in conjunction with factors contributing to progressive malalignment. Lafage et al8 have emphasized age as a necessary metric to incorporate into planning to redefine alignment thresholds. Historically, ASD correction is associated with a high failure rate of around 22%, despite intraoperative imaging and surgical technique improvements.9,10 Root cause analysis highlights greater baseline spino-pelvic deformity and requirements for more aggressive procedures to match patients' sagittal profiles as driving radiological failures. Consequently, suboptimal alignment outcomes are commonly attributed to deficiencies in preoperative planning strategies; prospective implementation of novel age-adjusted targets for individualized realignment may remedy this.
Intolerance to sagittal plane under- or overcorrection may result in important radiographic and clinical deteriorations, but recruitment of lower extremity musculoskeletal mechanisms to counteract postoperative malalignment remains unexplored.11–13 Advances in ASD assessment through novel full-body imaging technology accentuate the need for head-to-toe radiographic evaluation of lower extremity compensatory mechanism visualization, including knee and ankle flexion, hip extension, and pelvic displacement. Preliminary analyses have unveiled important associations between lower limb recruitment, maintenance of standing posture, and demographic characteristics, including age; such findings may precipitate changes in operative planning and realignment goals.14–16
These reports, however, only present a baseline snapshot of a patient's global alignment, as no study to date has offered a full-body analysis following surgical sagittal deformity correction using new age-alignment goals as indicative of successful versus failed realignment. This study thus analyzes pre- and postoperative full-body alignment following spinal deformity correction to evaluate adoption of compensation in patients whose postoperative sagittal profile deviates from novel age-adjusted alignment targets.
METHODS
Data Source
This is a retrospective radiographic analysis without clinical correlation of patients visiting a single academic center for spine-related complaints from 2013 to 2015 following Institutional Review Board approval. Inclusion criteria were adults (≥ 18 years) undergoing ≥ 4 levels of fusion for sagittal spinal deformity (scoliosis, kyphosis) with biplanar full-body stereotactic radiographs (EOS imaging) at baseline visit and early follow-up (≤ 6 months).17 Exclusion criteria were patients with fractures, malignancies, infections, pseudarthrosis, hardware failure, or nonidiopathic or nondegenerative deformity etiologies. A subanalysis was performed on the portion of the included cohort with complete radiographic follow-up at 1 year postoperative.
Data Collection and Radiographic Evaluation
Demographic data comprised age, body mass index (BMI), and gender. Surgical variables included upper and lower instrumented vertebrae (UIV/LIV), and osteotomy use (Smith-Petersen osteotomy, 3-column osteotomy [3CO]).
Full-body images were measured for the 122 patients who met the inclusion criteria (Surgimap, Nemaris Inc, New York, New York).18,19 Spino-pelvic parameters included SVA, PT, pelvic incidence (PI), PI-LL, and thoracic kyphosis (TK) (Figure 1). Lower-limb parameters included knee flexion angle (KA: angle between the mechanical axes of the femur and tibia), ankle flexion angle (AA: angle between the mechanical axis of the tibia and the vertical), posterior pelvic shift (PS: offset between the posterosuperior aspect of the sacrum and the distal tibia anterior cortex), hip extension (SFA: angle formed by the line from the middle of S1 endplate to the midpoint of the 2 femoral heads and the line between the midpoint of the 2 femoral heads and the femoral axis), and global sagittal angle (GSA: angle subtended by a line from midpoint of C7 vertebra to midpoint of femoral condyles and a line from this point to the posterosuperior S1 corner).16,20,21
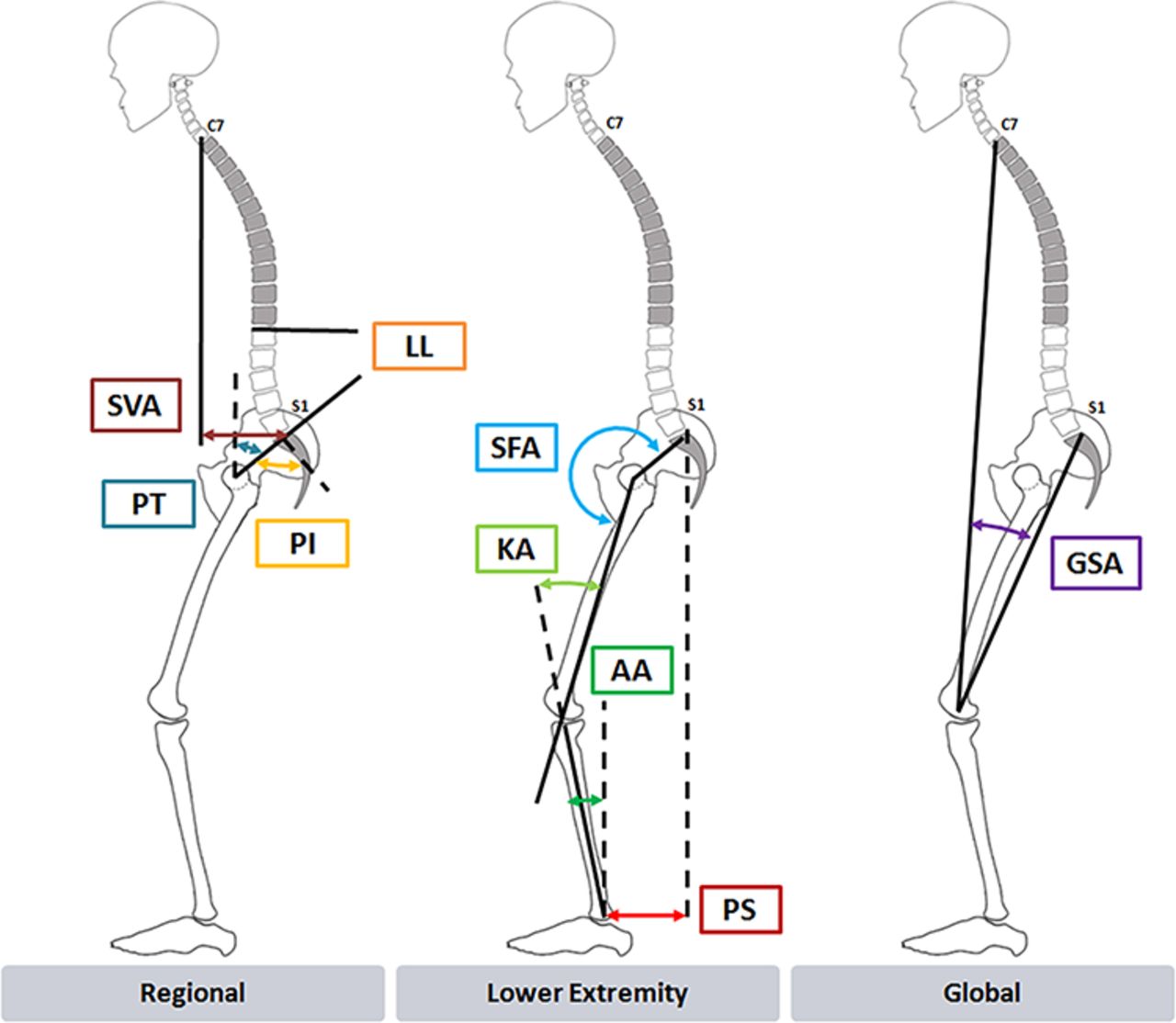
Measurements of regional (left), lower-limb (middle), and global (right) spinal radiographic parameters. Abbreviations: SVA, sagittal vertical axis; PT, pelvic tilt; PI, pelvic incidence; LL, lumbar lordosis; SFA, sacrofemoral angle; KA, knee angle; AA, ankle angle; PS, posterior pelvic shift; and GSA, global sagittal angle.
Patient Age-Alignment Grouping
Age-specific alignment values for SVA, PT, and PI-LL were generated for each individual patient according to previously published formulas:8


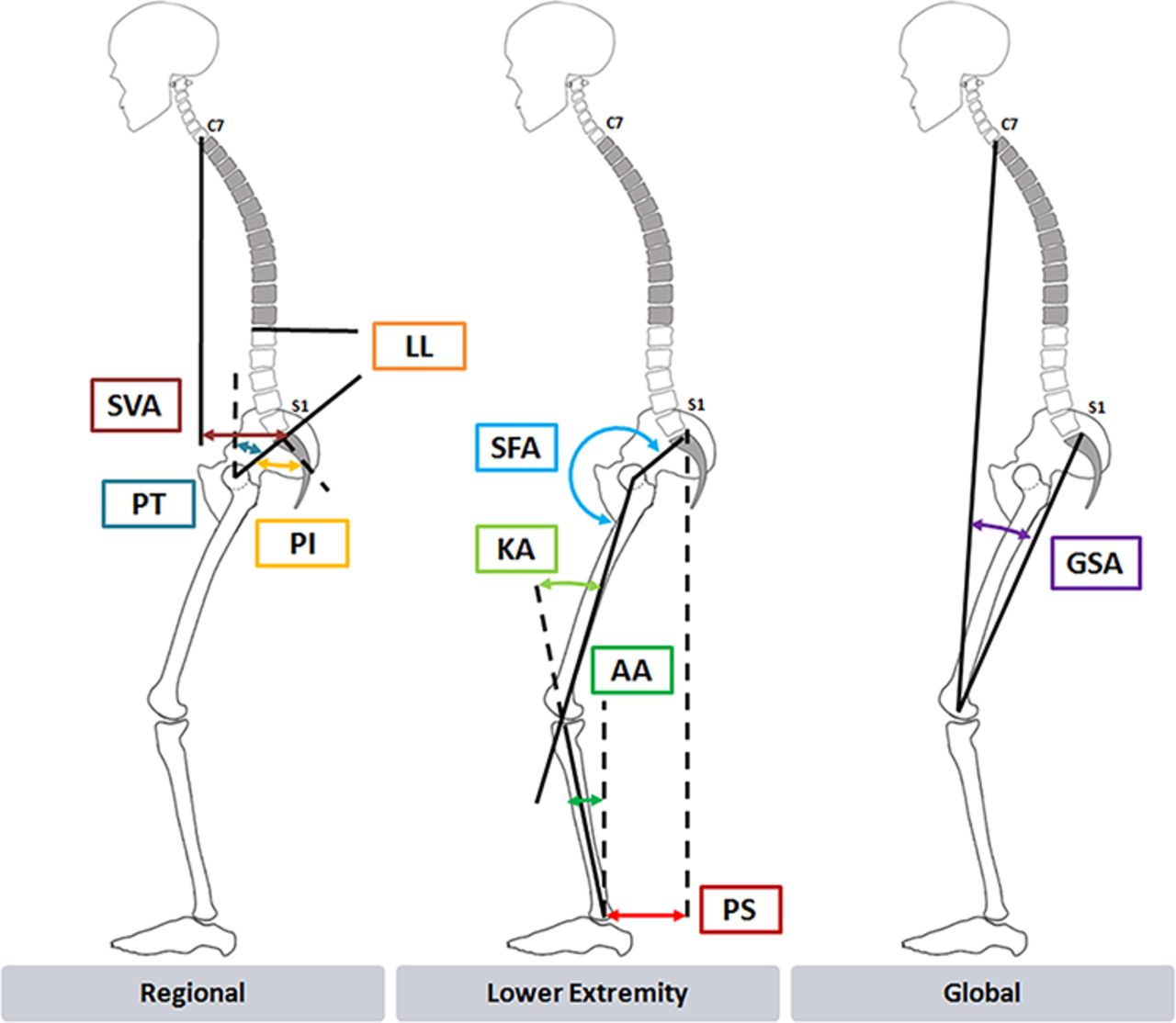
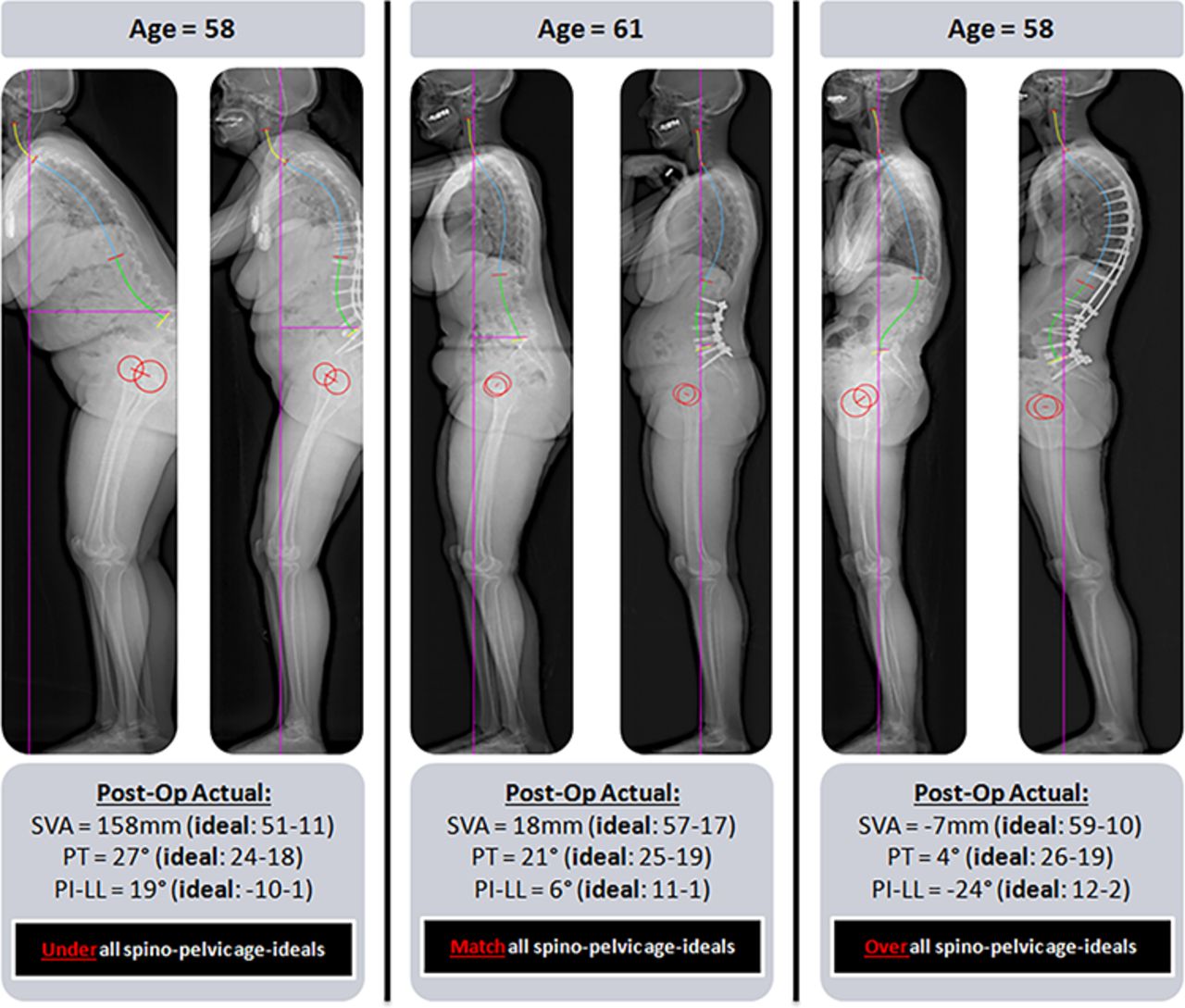
Correction groups were then generated according to the agreement between actual measured alignment recorded at the early postoperative visit and calculated age ideals: matched, undercorrected, and overcorrected. Matched patients' actual postoperative alignment reached a ± 10-year interval of age-adjusted values, based on a validated method of gauging under- versus overcorrection.8 Undercorrected and overcorrected patients were aligned to targets that were > 10 years or < 10 years of their age in each spino-pelvic category (Figure 2).

Case examples (baseline and early [≤ 6-month] postoperative) full-body stereoradiographs of 3 patients whose actual postoperative alignment was Under (undercorrected), Match (matched), or Over (overcorrected) compared to the age-adjusted ideal for sagittal spino-pelvic parameters. Postoperative age-adjusted ideal measurement ranges for each spino-pelvic parameter are provided for a ± 10-year threshold range for optimal alignment based on the individual patient's age. Abbreviations: SVA, sagittal vertical axis; PI-LL, mismatch between pelvic incidence and lumbar lordosis; and PT, pelvic tilt.
Statistical Analysis
Descriptive statistics were used to describe categorical and continuous variables. Comparisons between baseline and postoperative alignment for compensatory mechanisms (TK, SFA, KA, AA, PS) and spino-pelvic measures (SVA, PT, PI-LL) were made between 3 correction groups with ANOVA. Statistics were performed with SPSS software (version 21.0, Armonk, New York) with statistical significance set at P < .05.
RESULTS
Study Sample and Surgical Summary
A total of 122 patients met inclusion criteria (mean age: 61.7 ± 14.6 years; mean BMI: 26.9 ± 5.8 kg/m2; 64.8% female). A mean 10.0 levels were fused among all patients. The 3CO rate was 14.8%, and the Smith-Petersen osteotomy rate was 47.5%.
Radiographic Realignment Outcomes
The average preoperative spino-pelvic parameters for all patients revealed severe baseline sagittal malalignment: SVA = 73.1 ± 73.8 mm, PT = 27.1° ± 12.0°, PI-LL = 20.5° ± 21.8° (Table 1). The mean calculated age-ideal alignment values were: SVA = 38.3 ± 29.2 mm, PT = 22.2° ± 4.9°, PI-LL = 9.5° ± 17.7°. Compared to theoretical age-adjusted targets, actual postoperative values for all parameters were significantly larger (P < .001). However, all patients significantly improved in alignment at early follow-up: Δ SVA = −37.3 ± 59.0 mm, Δ PT = −3.1° ± 8.4°, Δ PI-LL = −11.0° ± 16.0° (P < .001 all). There was an overall reduction in pelvic shift (38.8 ± 47.8 mm to 16.7 ± 38.7 mm) and knee flexion (9.8° ± 9.2° to 6.8° ± 8.4°) accompanied by the surgical correction (P < .001 both cases); postoperative hip extension, however, remained unchanged (P = .577). The improvement in global standing alignment was reflected in a significant GSA decrease (8.3° ± 7.2° to 4.4° ± 5.0°, P < .001).
Mean baseline, age-adjusted, and actual postoperative sagittal alignment parameter values for the entire study cohort.
Postoperative Correction Groups
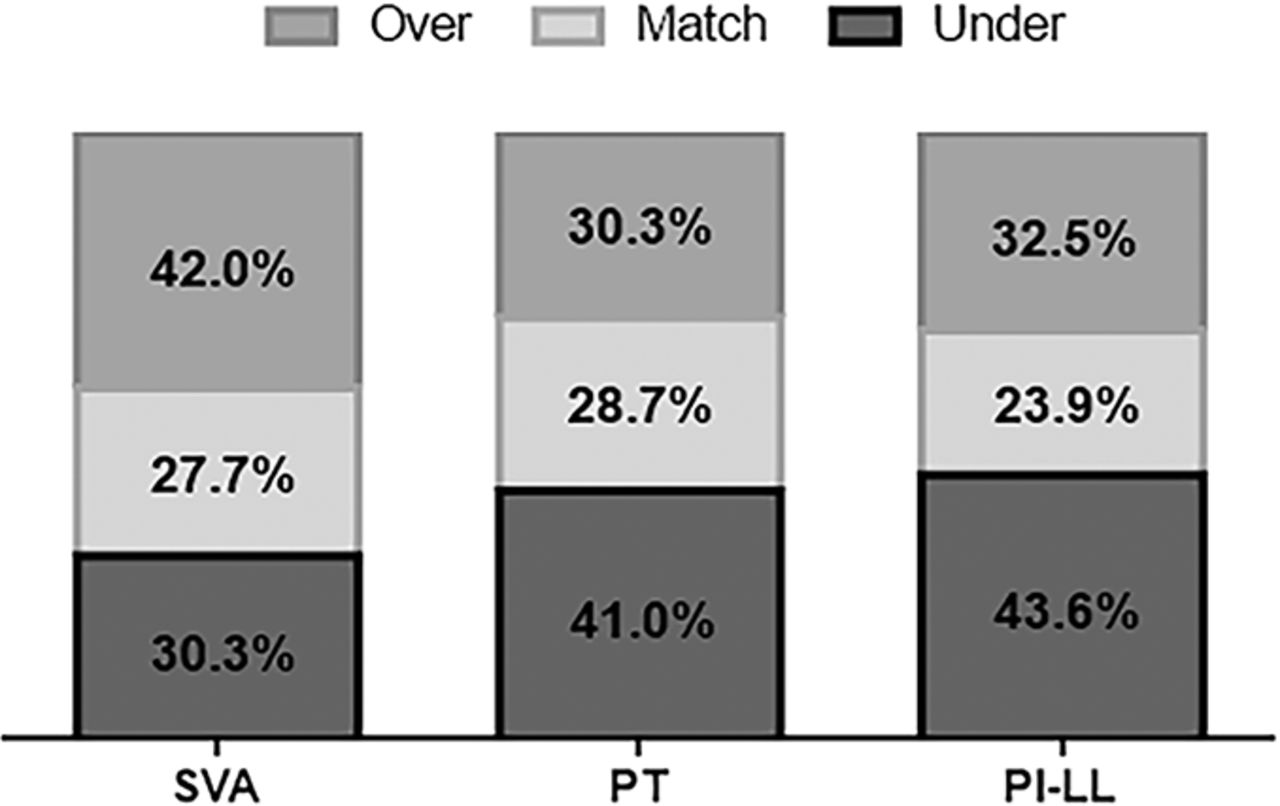
Following correction, there was low congruity of actual alignment with age-adjusted ideals, with 27.7%, 28.7%, and 23.9% of patients matching age targets in SVA, PT, and PI-LL, respectively (Figure 3). Patients were more frequently undercorrected, compared to age-adjusted targets, for PT (41.0%) and PI-LL (43.6%). However, in the SVA group, 42.0% of patients were overcorrected. Mean spino-pelvic values in each postoperative age-alignment correction group differed, with the most severe malalignment observed in undercorrections (Table 2). Use of 3CO did not significantly affect resultant correction group (P > .05).

Rates of patients in each early postoperative spino-pelvic alignment group (Match, Undercorrect, Overcorrect) according to age-adjusted targets. Abbreviations: SVA, sagittal vertical axis; PI-LL, mismatch between pelvic incidence and lumbar lordosis; and PT, pelvic tilt.
Actual measured spino-pelvic values for each age-adjusted alignment target group (Match, Undercorrect, Overcorrect) at baseline and early postoperative visit.
SVA Correction Analysis
Each SVA correction group was similar for BMI, UIV, LIV, and levels fused (range: 9.3-10.6) (P > 0.05 all). For SVA, undercorrected patients were younger than overcorrected patients (55.2 ± 19.0 vs. 68.6 ± 8.7 years, P < .001). Undercorrected cases had the greatest offset between age-adjusted and actual postoperative alignment (−61.6 ± 32.0 mm). These patients showed the greatest pre- and postoperative anterior malalignment, resulting from the smallest correction (Table 2). Undercorrected SVA patients compensated for persistent postoperative anterior alignment with reduced TK (40.9° ± 17.7°) and increased KA (9.0° ± 8.8°; P < .040 all; Table 3). They also recruited an increased posterior pelvic shift (50.5 ± 36.9 mm) compared with both matched and overcorrected cohorts (P < .001 all). Undercorrection impacted full-body standing axis, displaying significantly larger GSA (undercorrected: 9.1° ± 5.2°, matched: 5.0° ± 3.3°, overcorrected: 1.7° ± 3.3°, P < .001).
Adoption of compensatory mechanisms for SVA postoperative age-adjusted alignment groups (Match, Undercorrect, Overcorrect) at baseline and early follow-up.
PT Correction Analysis
The 3 pelvic tilt (PT) correction groups had similar age, UIV, LIV, and levels fused (range: 9.3-11.2 levels; P > .05 all). Age-undercorrected PT patients had a larger baseline BMI than overcorrections (27.7 ± 5.9 versus 24.3 ± 4.9 kg/m2, P = .015). Undercorrected cases were on average 11° ± 7.3° from age-adjusted goals. These patients displayed the largest baseline and postoperative PT, with the smallest degree of tilt change with surgery (Table 2). Undercorrections also reported a larger postoperative SVA than overcorrected cases (undercorrected: 88.7 ± 72.3 mm versus overcorrected: 50.2 ± 77.5 mm, P = .048). When patients were age-undercorrected for PT, they recruited more posterior pelvic shift (37.7 ± 32.7 mm), hip extension (212.4° ± 9.6°), knee flexion, and ankle dorsiflexion (P < .044) to compensate (Table 4); their GSA was consequently greater (undercorrected: 7.3° ± 4.9°, matched: 4.2° ± 4.6°, overcorrected: 1.8° ± 4.3°, P < .001).
Adoption of lower extremity compensatory mechanisms for PT postoperative age-adjusted alignment groups (Match, Undercorrect, Overcorrect) at baseline and early follow-up.
PI-LL Correction Analysis
The UIV, LIV, and BMI for PI-LL age-adjusted correction groups were similar (P > .05), though overcorrections underwent slightly longer fusions than matched cases (undercorrected: 9.9, matched: 8.5, overcorrected: 11.1, P = .047). Undercorrected patients were younger than both the matched and overcorrected groups (undercorrected: 59.0 ± 16.7 years, matched: 65.9 ± 11.1 years, overcorrected: 65.5 ± 10.4 years, P = .034). Patients undercorrected for PI-LL were on average 20.0° ± 13.2° from the age-adjusted targets. Undercorrected patients had a significantly greater PI-LL than all correction groups at baseline and early postoperative visit (Table 2). The degree of correction in the age-undercorrected PI-LL group versus matched cases was smallest. At early follow-up, PI-LL undercorrections were characterized by a larger SVA (54.5 ± 54.5 mm) and PT (27.7° ± 11.3°) compared to matched and overcorrections (P < .001 all). The undercorrected cohort demonstrated a significantly increased posterior pelvic shift (39.3 ± 34.1) with reduced TK (37.0 ± 16.1; P < .001 all; Table 5). This sagittal profile was reflected in an increased GSA (undercorrected: 7.3° ± 4.9°, matched: 4.3° ± 3.1°, overcorrected: 1.9° ± 4.6°, P < .001). PI-LL overcorrected patients also displayed a significantly greater SFA (208.6° ± 10.1°) and more anterior pelvic displacement (−6.6 ± 38.2 mm) compared to those undercorrected.
Adoption of lower extremity compensatory mechanisms for PI-LL postoperative age-adjusted alignment groups (Match, Undercorrect, Overcorrect) at baseline and early follow-up.
Effect of Lumbosacral Fusion or Pelvic Fixation on Lower Limb Compensation
There were 79 (65%) patients with fusion to lumbosacral region or pelvic fixation. Patients with lumbosacral fusions/sacrum/pelvic fixation experienced a larger decrease in KA from pre- to postoperatively than patients without lumbosacral fusions or pelvic fixation (with: −4.2°, without: −0.6°, P = .003). Pelvic shift significantly decreased postoperatively for patients with lumbosacral fusions or pelvic fixation and increased for patients without (with: −36.8mm, without: +10.7mm, P < .001). GSA also decreased for patients with lumbosacral fusions and/or pelvic fixation and increased for patients without (with: −5.4°, without: +0.48°, P < .001). Patients with lumbosacral fusion or pelvic fixation did not show different changes in SFA and AA pre- to postoperatively (both P > .05).
Relationship between Radiographic Correction and Clinical Outcomes
In looking at SVA alignment groups, we assessed clinical scores for the Oswestry Disability index (ODI), neck disability index (NDI), and visual analog scale (VAS) neck, arm, back, and leg pain scores for patients who were matched for SVA, undercorrected, and overcorrected. Patients who matched their target SVA trended toward improvement in VAS back pain scores (preop: 6.1 ± 3, postop: 4.1 ± 2.3, P = .056). Patients who were undercorrected with respect to SVA worsened in ODI (preop: 40 ± 26.2, postop: 53.8 ± 20.1, P = .038) and NDI (preop: 31.3 ± 23.4, postop: 48.5 ± 16.6, P = .0009) after surgery. Patients who were overcorrected with respect to SVA displayed improvements in VAS neck and leg pain scores.
Alignment Sustainability
A subanalysis of patients with 1-year postoperative radiographs (in addition to the 6-month follow-up for the entire cohort) was performed. The rates of patients reaching age-adjusted threshold ranges by 1 year postoperative were as follows:
SVA: undercorrected to matched = 0.0%; overcorrected to matched = 28.6%
PT: undercorrected to matched = 26.7%; overcorrected to matched = 31.2%
PI-LL: undercorrected to matched = 15.4%; overcorrected to matched = 14.3%
Matches in all spino-pelvic age-adjusted correction groups maintained optimal alignment (P > .05). Undercorrections showed significant changes in compensation from early to 1-year follow-up visits in this subset of patients (Table 6): undercorrection for SVA displayed a decrease in TK (Δ −7.8°, P = .032) with more anterior PS (Δ −13.2 mm, P = .039); undercorrection for PT decreased hip extension (Δ −3.7°, P = .004) and TK (Δ −4.7°, P = .036); undercorrection for PI-LL only resulted in significant increase in TK (Δ 6.3°, P = .009).
Changes in sagittal alignment from early (≤6M) to 1-year postoperative visit for each spino-pelvic age-adjusted correction group (Match, Undercorrect, Overcorrect).
DISCUSSION
Full-body imaging is a powerful tool for extensive visualization and analysis of sagittal alignment in treating complex spinal deformity. However, these principles remain untested in a postoperative setting, wherein compensation may be required to offset unfavorable realignment. There have been a number of articles previously published on sagittal balance of the mobile spine, but fewer on age-adjusted alignment targets in spine surgery.22,23 To our knowledge, the only studies describing full-body postoperative alignment are in hip and acetabular pathology, without characterization of lower extremity alignment changes.24,25 This study presents a pre- and postoperative investigation of variations in sagittal alignment and compensation based on deviations from age-adjusted deformity thresholds for optimal correction.
Expectedly, patients displayed significant improvements in spino-pelvic parameters at the early postoperative visit. Optimal global postoperative alignment assessment demands analysis of the lower extremities, as these mechanisms work to regulate standing posture.16,26,27 Consistent with the overall SVA decrease and lordosis restoration, the cohort's pelvic displacement shifted anteriorly (Δ −24.0 mm) coupled with reduction of knee flexion (Δ −3.3°). This lower-limb decompensation follows sequential compensatory mechanism recruitment and relaxation given improved spinal alignment to maintain erect posture.16 The cohort's decrease in GSA, accounting for simultaneous spino-pelvic deformity and lower-limb compensation, confirms this full-body change.20
Failure to realign deformity patients frequently results in hardware complications and poor long-term outcomes.9,28,29 Surgical plans built on age-adjusted targets, providing clinically relevant patient-specific thresholds, are essential to mitigate this risk.8 In the current study, by applying these age-adjusted ideals for classic spino-pelvic measures, we were able to determine rates of success and failure following deformity correction. Interestingly, rates of patients' postoperative sagittal profile matching a ± 10-year age range were lower than prior reports evaluating successful versus failed ASD procedures. Against PT and PI-LL age ideals, patients tended to display high rates of undercorrection; only for SVA did patients reach a higher success (match or overcorrection) rate (69.7%), which compares well to the 77% frequency proposed by Schwab et al.9 However, this study reveals that prior literature, basing alignment failures off of generalized thresholds instead of an individualized goal, may underestimate actual undercorrection occurrence, particularly when considering the magnitude of deformity at baseline.
All undercorrections showed consistently larger baseline sagittal malalignment for each respective spino-pelvic parameter. Comparably, Lafage et al10 presented a 22% failure rate following thoracic 3CO and noted that these patients also displayed greater preoperative SVA, PT, and LL malalignment. Our findings are similar to the failure analysis done by Schwab et al of 79 ASD patients following 3CO: failed patients at < 6-month postoperative follow-up had a significantly larger preoperative SVA, PT, and PI than successful realignments.9 Collectively, these results support the concept that optimal realignment requires a specific degree of correction that proportionally matches a single patient's baseline deformity, which may be prospectively achieved via age-adjusted correction formulas. For SVA and PI-LL, undercorrected patients were younger (SVA: undercorrected: 55.2 years versus overcorrected: 68.6 years; PI-LL: undercorrected: 59.0 years, matched: 65.9 years, overcorrected: 65.5 years) than successful realignments, suggesting that despite older ASD cases requiring less rigorous age-idealized thresholds, greater baseline deformity in undercorrections was the predominant driver of inferior radiographic outcomes.8 Effectively, despite undergoing comparable fusions, undercorrections displayed the smallest amount of regional correction per spino-pelvic parameter considered against all other groups.
SVA, PT, PI-LL mismatch present with variable severity for each patient, and may differentially hinder the ability to compensate throughout the spine or lower limbs. As seen in our analysis according to each parameter, deformities with different malalignment as measured by these characteristics triggered different methods for compensation.
At early postoperative visit, SVA undercorrection to age-adjusted ideals, marked by a mean offset of 62 mm, correlated with increasing posterior pelvic shift, flexed knees, and thoracic hypokyphosis, all well-documented mechanisms to compensate for an anterior displacement of C7.16,30 At 1-year follow-up, undercorrected SVA patients were unable to regain age-ideal alignment (0.0% undercorrection-to-match), despite apparent thoracic flattening and anterior pelvic displacement. Though the contribution of TK to counteracting excessive anterior malalignment has been described, it is possible that these patients did not retain the flexibility required; extension of fusion to cephalad levels may further reduce this possibility, though the UIV of SVA correction groups was similar.31,32
When PT was undercorrected, knee flexion and pelvic shift were adopted, consistent with prior reports theorizing the transfer of compensation to lower limbs when pelvis retroversion is exhausted.15,16,33 Patients at risk for PT undercorrection based on age-adjusted targets displayed the largest preoperative tilt and highest BMI, factors also implicated in ASD failures analyzed by Schwab et al.9 These same patients displayed PT normalization 1 year postoperation via a reduction in hip extension (SFA Δ −3.7°) and thoracic compensation (Δ −4.7°).
Patients undercorrected to age-adjusted PI-LL thresholds were distinct in smaller postoperative TK and greater pelvic shift to mitigate the residual spino-pelvic mismatch and anterior malalignment (SVA = 55mm, PT = 28°). This hypokyphotic thoracic posture with posterior pelvic displacement assumed for maximum compensation with positive SVA and inadequate LL has been described.15,34,35 Moreover, patients overcorrected in PI-LL displayed a comparable profile as previously described by Ferrero et al16: heightened hip extension and thoracic kyphosis, with anterior pelvic displacement acting as compensation, with overall neutral global alignment and low PT.16 Consistent with the smaller PI-LL correction (Δ −4.5°) in age-undercorrected patients, Jang et al noted a strong correlation between the lumbar correction angle and the spontaneous postoperative thoracic curve change.36 Subsequent rapid exhaustion of the hypokyphotic compensatory mechanisms was also noted by 1-year follow-up in undercorrected cases, with a significant increase in TK (Δ 6.3°). Prior series have similarly noted kyphotic instability and progression following insufficient LL correction: Lafage et al31 reported on 18 patients with unfavorable postoperative TK after pedicle subtraction osteotomy, which was theoretically driven by inadequate postoperative LL restoration. Interestingly though, no supplemental variations in lower extremity compensation were noted in age-undercorrected PI-LL patients at 1 year postoperation.
Limitations
A primary limitation of this study is the heterogeneous nature of spinal deformity, which was not controlled for beyond fusion extent. Further, local compensatory mechanisms of retrolisthesis and adjacent segment hyperextension were not evaluated. In addition, the EOS database is currently limited in the evaluation of intrinsic joint disease that might influence the position of the hips, knees, and ankles in compensatory mechanisms. This study is lacking coronal imbalance assessment that likely contributes to clinical symptoms that should be investigated further. As this was primarily a radiographic study, correlations between clinical outcome measures and observed compensatory mechanisms should be subsequently evaluated with extended postoperative follow-up.
Conclusion
This is the first study to analyze full-body alignment following spinal deformity correction using novel age-adjusted formulas for radiographic thresholds as a benchmark for surgical success. Undercorrection is underappreciated using traditional standardized thresholds. Differential compensation recruited in undercorrections according to spino-pelvic parameter highlights the dynamic relationship between spinal regions and certain musculoskeletal components in patient-specific deformity evaluation.
Footnotes
Disclosures and COI: The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this paper. Institutional Review broad approval was obtained prior to study.
- ©International Society for the Advancement of Spine Surgery
- Copyright © 2019 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Risk Factors for Recurrent Proximal Junctional Failure Following Adult Spinal Deformity Surgery: Analysis of 60 Patients Undergoing Fusion Extension Surgery for Proximal Junctional Failure
- Improved Surgical Correction Relative to Patient-Specific Ideal Spinopelvic Alignment Reduces Pelvic Nonresponse for Severely Malaligned Adult Spinal Deformity Patients