


ABSTRACT
Background: Expandable cages have gone through several iterations since they first appeared on the market in the early 2000s. Their development was prompted by some common problems associated with static interbody cages, including migration, expulsion, dural or neural traction injury, and pseudarthrosis.
Objective: To summarize current technological advances from earlier expandable lumbar interbody fusion devices to implants with vertical and medial-to-lateral expansion mechanisms.
Methods: The authors review the currently available expandable cage designs, the incremental technological advances, and how these devices impact minimally invasive surgery interbody procedures and clinical outcomes. The strategic concepts intended to improve the minimally invasive application of expandable interbody fusion implants are reviewed from a surgeon's perspective in a clinical context to discuss how their use may improve patient outcomes.
Conclusions: The geometrical configuration, effective stiffness of composite multi-material cage designs may impact the bone-implant contact area with the endplates. Hybridization strategies of expandable cage technology with modern minimally invasive and endoscopic spinal surgery techniques are presented by outlining their advantages and disadvantages.
Level of Evidence: 1
Clinical Relevance: Systematic review.
INTRODUCTION
This special issue of the International Journal of Spine Surgery is focused on demonstrating the clinical application of endoscopic and other minimally invasive spinal surgeries (MISSs) beyond the scope of simple decompression by adopting state-of-the-art technologies. Treatment of many common degenerative conditions requires the use of an implant to aid in the stabilization of the lumbar spine. The combination of endoscopy with interspinous process implants is an example of posterior column stabilization1 demonstrated in this special focus issue. Anterior column stabilization is integral to many modern reconstructive fusion procedures. Successful endoscopic implantation of interbody fusion cages through the transforaminal approach for anterior column stabilization has been described in several studies,2–5 some as standalone fusions5,6 and others as endoscopically assisted placement of interbody fusion cages with posterior supplemental fixation.2–4 In this editorial, the authors review contemporary design rationales and comparative biomechanical concepts for static and expandable lumbar interbody fusion cages and how they relate to clinical outcomes.
SIMPLIFIED SPINE CARE
Coupling modern interbody fusion cages with minimally invasive implantation techniques is attractive as it facilitates less invasive spinal fusion further and enables the evolution from traditional open surgery to other types of translaminar MISS or even transforaminal endoscopic techniques.6 Nowadays, there is an ongoing transition of appropriately selected spine surgeries from the hospital into an outpatient ambulatory surgery center setting.7,8 Hence, less traumatic, less complicated, and less painful surgeries with reliable outcome improvements are needed to facilitate this transition.9 Expandable interbody fusion cages have the potential to play a role in the outpatient ambulatory spinal decompression fusion surgery solution.5
WHY EXPANDABLE CAGE DESIGNS?
Historically, interbody fusion cages were introduced to improve fusion rates and to restore lumbar lordosis, as well as intervertebral and foraminal height.10–12 Additional advantages relate to better containment of bone graft.13 In recent years, the evolution of static interbody fusion cages has emphasized minimally invasive spinal surgery technique (MISST) applications with the primary goal to reduce approach morbidity by improving insertion mode and to control sagittal and coronal alignment better.14–19 Consequently, interbody fusion cages of different sizes and shapes were offered. Additional technological advancements included biomaterial components and cage manufacturing processes, such as 3-dimensional printing.20 Despite these advances in static cage design, subsidence-related problems due to endplate violation on insertion remained an issue linked to inferior clinical outcomes.10,21,22 These shortcomings stimulated a shift from static to expandable cage technology in an attempt to minimize undersizing of static cages used in posterior lumbar interbody fusion (PLIF), and transforaminal lumbar interbody fusion (TLIF). The first-generation expandable lumbar interbody fusion cages were primarily vertically expandable.23,24 Minimizing size during the insertion process was shown to facilitate the application of MISST during insertion while maximizing vertical height restoration.16–19,25 Second- and third-generation cage expansion technologies added horizontal expansion to provide a larger footprint and cover more of the endplate.16,26 Further advances focused on better controlling sagittal alignment and the ability to place more substantial amounts of bone graft either around the device or into an internal graft chamber.26
THE EVOLUTION OF EXPANDABLE INTERBODY CAGES
The development of expandable cages followed the surgical approaches ranging from lateral to oblique and direct posterior access. Consequently, medial-to-lateral, anterior-to-posterior, vertical, and translating expansion mechanisms have been employed. Early examples of vertical expansion were embodied in the StaXx.27 This first-generation expandable poly-ether-ether-ketone (PEEK) cage provides expansion by the sequential insertion of PEEK wafers in situ, creating a stack or column of vertical distraction in 1-mm increments caudad to cephalad. While the StaXx allows intervertebral implantation through a small entry portal, it cannot be retracted once implanted and fully expanded. Also, it does not have a bone graft chamber. Another example of an expandable cage device to be assembled in situ is the modular InFix device.28–30 In total, 84 unique configurations are possible with the 3 different footprints, 4 vertical side struts ranging from 8 to 14 mm, and 7 lordotic angles ranging from 0° to 18° degrees in 3° increments. This modular expandable cage design brought several advantages to the operating room. The in situ expansion was shown to reduce endplate trauma and subsequent propagation of subsidence. When fully assembled in situ, this titanium implant was intended to be a load-sharing device resting on the ring apophysis with a lower design-inherent strain limitation at the bone-cage interface. This design include a fenestrated bone graft chamber intended to promote interbody fusion. Moreover, the overall low modulus of elasticity of the InFix device (1099 MPa) was reported to be much closer to cancellous bone (≈220 MPa), than the material modulus of elasticity of PEEK (3600 MPa), cortical bone (12 000 MPa), titanium (113 800 MPa), or cobalt-chrome alloys (234 000 MPa).30 Another early example of vertically expandable is the Omega Lumbar Interbody Fusion Device.31 This all-titanium, bullet-nose design facilitated insertion and featured an infinitely adjustable, from 0 to 3 mm, self-locking expansion mechanism for minimal impaction. It also featured a cannulated option for the trans-Kambin triangle lumbar interbody fusion over a guidewire and in standard solid form for PLIF implantation.
Other examples of primarily vertically expanding interbody fusion cages include the Caliber, the Rise, and the Altera.23,24 These titanium implants are designed for posterior PLIF and TLIF approaches and intended to deal with reduced height during insertion to minimize impaction and preserve endplate integrity. The Altera (released in 2014) features an articulating expandable cage design to be steered into the anterior disc space during TLIF procedures. The VariLift is a threaded cylindrical interbody fusion device that can be used in pairs bilaterally through a PLIF approach or as a single device from a unilateral oblique TLIF approach.32,33 Most of these expandable interbody fusion spacers are approved by the US Food and Drug Administration (FDA) for single- or 2-level implantation and are to be used with posterior supplemental fixation systems.32,33
The FlareHawk expandable cage features a hybrid design with an outer PEEK shell and an inner titanium shim.34 The shell is inserted in a compressed form ideally suited for MISS applications because it can be inserted through a small annular window into the intervertebral disc space and expands bidirectionally when the inner titanium shim is inserted into the PEEK shell.
DRAWBACKS OF EXPANDABLES
Some disadvantages of expandable interbody fusion cages have been demonstrated in clinical follow-up. Damage to the endplate and the resultant subsidence and loss of intervertebral and neuroforaminal height with recurrence of symptoms can occur with overexpansion, especially in patients with osteopenia or osteoporosis. Stress-shielding and lack of sufficient area for bone grafting may contribute to pseudarthrosis. One of the biggest drawbacks of expandable interbody fusion cages may be related to the increased cost. Clinical research will have to show whether the higher implant cost on the front end of a clinical treatment cycle are justified by perioperative cost savings on the back end due to shorter operative time, fewer complications, and fewer reoperations.
SURGEON INPUT AND DESIGN FEATURES
Expandable cages have several design features that were prompted by surgeons' desires to solve the problems of prior designs. For example, smaller insertion height helps minimize nerve root retraction and reduces the impaction force require to place the cage in its optimal position. Another feature common to several commercially available expandable interbody fusion cages relates to continuous expansion. This feature is considered advantageous by most surgeons familiar with this technology as it allows optimal endplate-to-endplate fitting while minimizing overdistraction. The in situ distraction and expansion is another such surgeon-preferred feature because the best fit can be combined with optimal height restoration. The combination of PEEK with titanium or cobalt-chrome alloys facilitates radiographic fusion assessment at the bone-implant interface. Likewise, radiographic markers are helpful in ascertaining the exact implant position. Some surgeons prefer an automatic locking mechanism to eliminate an extra locking step and to maintain the desired implant height over time.
MEASURES OF CLIINICAL SUCCESS
Commonly used clinical and radiographic outcome parameters have been correlated in several clinical studies in an attempt to develop predictors of clinical success with the expandable cage technology. Increase in posterior disc and foraminal height, restoration of lumbar lordosis, the absence of cage subsidence or endplate injury, along with bony bridging on advanced cross-sectional imaging studies including computed tomography are commonly investigated variables. Several clinical studies1–4,6,16,22,23,25–27,35–49 and a meta-analysis10 on expandable lumbar interbody fusion cages have highlighted the use of these radiographic parameters and how they correlate to commonly used patient self-reported outcome measures.
Early studies were on simple cage designs such as the B-Twin.2–4,35 The studies demonstrated the problems with cage subsidence and in expandable devices, which have stress concentration at the bone-implant interface. Other stacked implant designs demonstrated the need for migration resistance. Posterior extrusion was a common complication noted with stacked PEEK designs.36 An early comparative prospective randomized controlled clinical and radiological study with enrolling patients in 2 groups, (1) with expandable cage (73 patients) or (2) static cage (72 patients), proved the concept of lower complications during PLIF surgery because of less tissue trauma and fewer problems from retraction of neural tissues.37 This clinical trial statistically confirmed a greater increase in anterior disc height ratio (P = .0057), posterior disc height (P = .016), and segmental lordosis (P = .00021) without loss of correction in follow-up. The authors reported similar radiologic fusion rate of 94.5% with the expandable and 87% with the static cage (P > .2). Long-term 5-year follow-up was published on 72 patients treated with expandable spacers. At final follow-up, the authors reported significant Oswestry Disability Index reductions (41.5 ± 3.5; P < .05). The focal lordosis restoration was maintained without significant difference (P = .453) with a 100% fusion rate and without adjacent segment degeneration.39 Later designs showed favorable clinical outcomes and maintained restoration of neuroforaminal height with expandable PEEK cages.27 At average follow-up of 19.3 months, the authors demonstrated a statistically significant increases in the average disk height from 6.49 to 8.18 mm (P = .037) and foraminal height from 15.6 to 18.53 mm (P = .0001), and a significant reduction in the anterolisthesis from 5.13 to 3.15 mm (P = .005), and a very low, statistically not significant, vertical subsidence numbers averaging 0.66 mm (7.4%; P = .35). Correlation with clinical outcomes showed statistically significant reductions in the visual analog scale (VAS) back from 6.42 to 3.11 (P < .001), in VAS buttock from 4.66 to 1.97 (P = .002), in VAS leg from 4.55 to 1.96 (P < .001), and in Oswestry Disability Index from 21.7 to 12.1 (P < .001). On the basis of these results, the authors concluded that expandable PEEK spacers can “…effectively and durably restore disk and foraminal height and improve the outcome without significant subsidence.” 27 Several MISS implantation studies utilizing multiple, different expandable interbody fusion cages in conjunction with percutaneous pedicle screw constructs were demonstrated soon thereafter.1,16,25,41
STATIC VERSUS EXPANDABLE
When looking at clinical outcomes in standard MISS TLIF with static versus expandable cages, several studies have failed to demonstrated superior outcomes with the expandable cage technology.23,25,42,43,49 Various geometrical cage configurations including “banana” cage design have been found to be less prone to subsidence and better maintenance of lordosis and sagittal alignment corrections than with straight cage designs. In one study, 33 patients were implanted with an expandable banana-shaped and another 28 with an expandable straight cage. The authors found statistically greater improvements (P = .03) of disc height in the banana group where disc height changed from 4.8 ± 2.5 mm to 10.4 ±2.4 mm versus the straight cage group, where posterior disc height changed from 6.2 ± 2.5 mm to 9.6 ± 1.7 mm. In addition, segmental lordosis angle correction was higher in the banana group with 5.8° ± 5.0° versus 3.7± 3.6°. The lumbar lordotic angle improved in the straight group with 5.2° ± 6.4° compared to 3.7° ± 5.8° in the banana group. The subsidence rate was 6.6% in patients who received the banana-shaped expandable cage and 14.8% in patients who received the static expandable group.46 This study clearly highlights the importance of cage geometry and geometrical stiffness on clinical and radiographic outcome parameters.
Another FDA-registered retrospective clinical trial34 reported favorable outcomes on 129 patients with a stent-like implant emphasizing the importance of geometrical configuration of the expandable interbody fusion cage. Follow-up to date indicates that 96.6% fusion rate based 56 of 58 patients with available postoperative radiographs. Among 45 evaluable subjects, 71% (32 patients) achieved clinically significant improvements in VAS leg pain, and 76% (34 patients) achieved clinically significant improvements in VAS back pain. In the absence of complications including subsidence, displacement, and nerve injury attesting to the importance of geometrical configuration of cages capable of both cephalad-caudad and lateral-medial expansion maximize vertebral body endplate coverage and fusion area while minimizing nerve root retraction.
CLINICAL AND BIOMECHANICAL RELEVANCE OF STIFFNESS
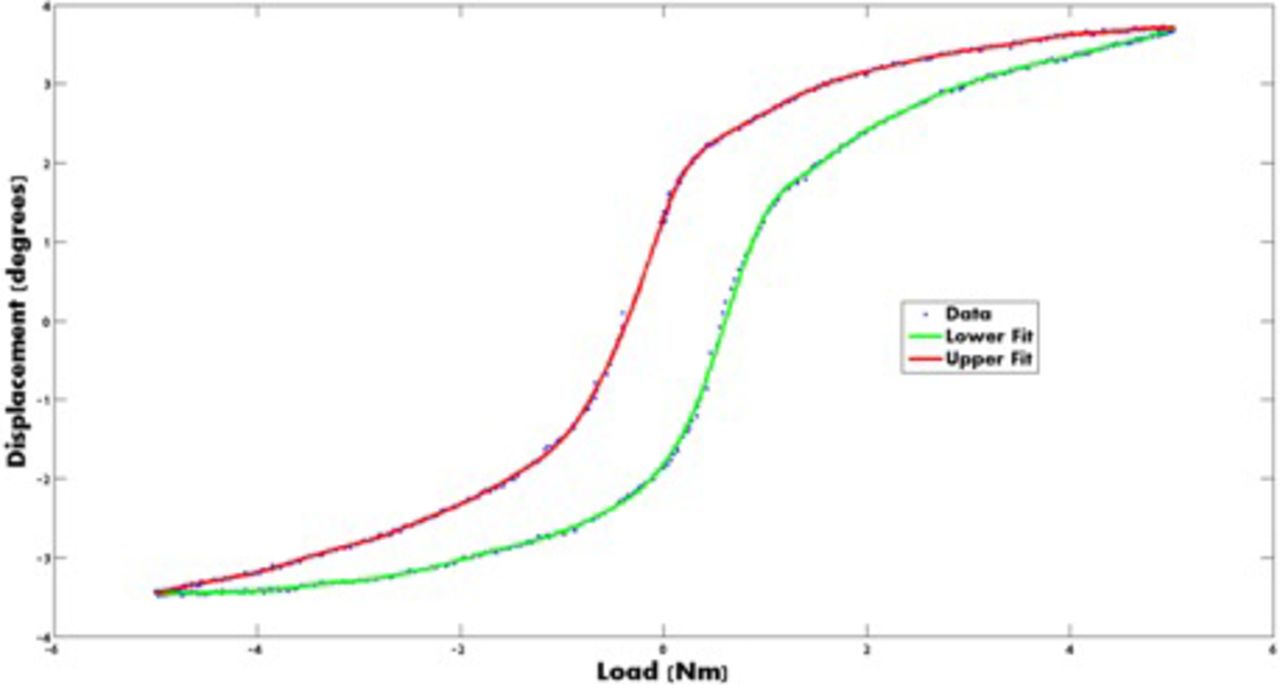
Many parameters have been suggested as clinically relevant indicators of spinal stability. Range of motion is the most commonly used metric with utility in both the clinical and biomechanical setting. For in vivo comparisons of stability (eg, between degenerative conditions and fused spines) range of motion may be readily determined but may not be sufficient in characterizing the efficacy of a given spinal device. A relevant example would be the different responses seen between the fixation device and the response of an functional spinal unit (FSU) when implanted with a motion-preservation device. Because of this, parameters such as stiffness, which incorporate displacement as a function of load, offer both physical relevance and a direct-controlled correlation to stability. A representative load-displacement curve for a functional spinal unit can be found in Figure 1.
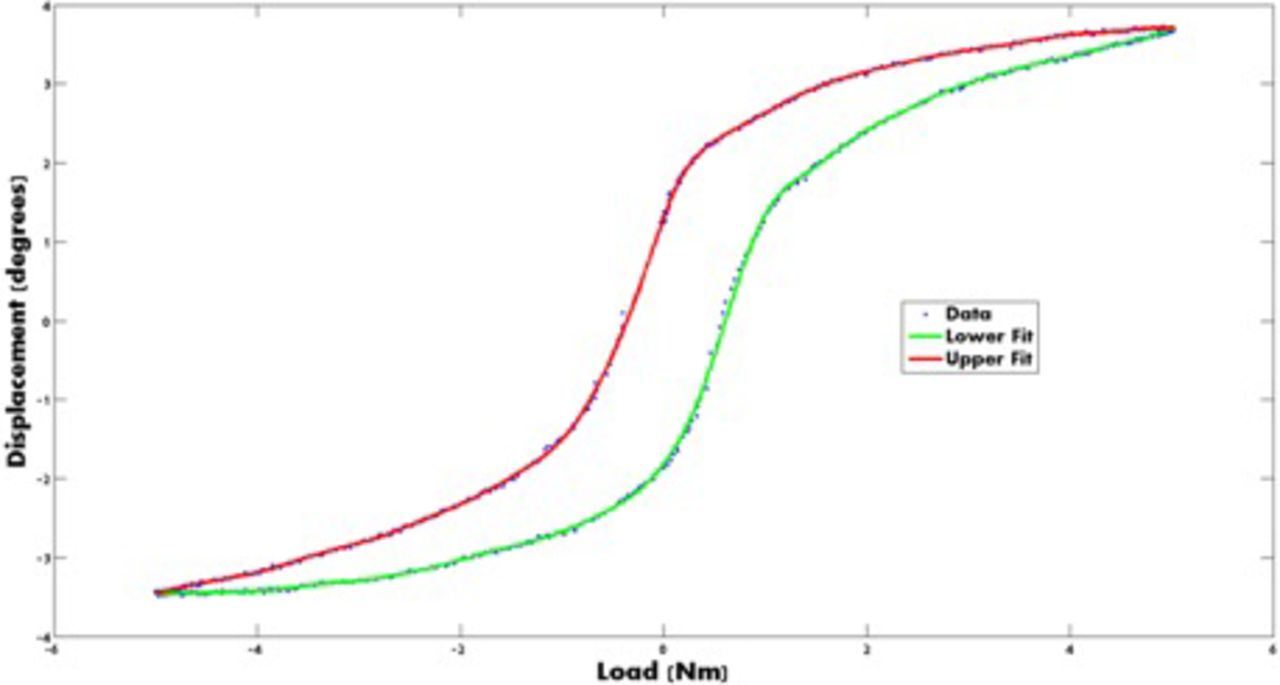
Representative load-displacement curve for a functional spinal unit.
EFFECTIVE STIFFNESS OF COMPOSITE DEVICES
Spinal interbody fusion devices have traditionally been designed and manufactured from homogenous materials. Examples include commercially pure titanium and titanium alloys. The device properties are dependent upon intrinsic material properties (eg, modulus of elasticity or stiffness), while the implant construct exhibits a design-dependent construct stiffness along with those material properties. In devices that incorporate different materials, an effective stiffness should be used in the modeling of the construct stiffness and, generally, can include a “springs-in-series” type of stiffness model for a single device with multiple layers of differing materials. Current titanium and PEEK polymer combination falls into multi-material device designs. In the case of numerous interbody devices (ie, 2 interbody cages) with various design materials, the appropriate, sufficient stiffness could be modeled as springs in parallel with each spring modeled in series. Combinations of devices and materials make for various spring models for an overall construct stiffness.
CONCLUSIONS
Ease of implantation in surgery and superior clinical outcomes are 2 of the many key requirements for surgeons to favor one implant over another. Spine surgeons are keenly aware that implant stiffness and spinal stability are the foundation of successful fusion. Common problems with both static and expandable interbody fusion cage implants include migration, expulsion, subsidence, and nonunion. Minimally invasive application through small access portals substantiates the need for expandable implants as they bridge the gap between the small size required during insertion, and the maximum size desired for optimum anterior column support. Important metrics relative to spinal stability include the stiffness of native materials along with the stiffness of an implant. Material stiffness is a fundamental material property with specific requirements. The stiffness of materials requires empirical derivation from homogenous isotropic test coupons. The same material configured in the form of a spinal implant has a different construct stiffness when compared to the native material, that is, a construct stiffness that is dependent upon the configuration of an implant and not the intrinsic native material property. Although both are commonly referred to as “stiffness,” a material's intrinsic property is different when configured as a medical device and loaded as is the overall FSU when implanted with the implant. All reflect a specific response given the same unit load. Surgeons must consider this relationship between effective stiffness of the implant in its final expanded position and the patient-inherent factors that dictate the final size and implant to endplate interactions that may impact clinical outcomes. Open architecture expandable cage designs that allow vertical and medial-to-lateral increase in size appear the most suitable for successful clinical application since the final construct stiffness is likely sufficient to provide immediate anterior column support while accommodating reduced sizes required for minimally invasive surgery applications.
Footnotes
Disclosures and COI: The views expressed in this article represent those of the authors and no other entity or organization. The authors have no conflict of interest in regards to this research. KUL and BC have nothing to disclose.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS
REFERENCES
In this issue




{kind=link}
Jump to section
- Article
- ABSTRACT
- INTRODUCTION
- SIMPLIFIED SPINE CARE
- WHY EXPANDABLE CAGE DESIGNS?
- THE EVOLUTION OF EXPANDABLE INTERBODY CAGES
- DRAWBACKS OF EXPANDABLES
- SURGEON INPUT AND DESIGN FEATURES
- MEASURES OF CLIINICAL SUCCESS
- STATIC VERSUS EXPANDABLE
- CLINICAL AND BIOMECHANICAL RELEVANCE OF STIFFNESS
- EFFECTIVE STIFFNESS OF COMPOSITE DEVICES
- CONCLUSIONS
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- Biplanar Expandable Cages for Transforaminal Lumbar Interbody Fusion Are Safe and Achieve Good 1-Year Clinical and Radiological Outcomes in an Asian Population
- Biplanar Expandable Cages for Transforaminal Lumbar Interbody Fusion Are Safe and Achieve Good 1-Year Clinical and Radiological Outcomes in an Asian Population
- Expandable vs Static Interbody Devices for Lateral Lumbar Interbody Fusion