


ABSTRACT
Background: The sacroiliac joint (SIJ) is responsible for 15%–30% of chronic low back pain and fusion is increasingly used to alleviate chronic SIJ pain in adults. However, questions remain as to the most effective implant patterns to stabilize the joint. The objective of this biomechanical study was to evaluate how different implant spacing, configuration and quantity effect range of motion (ROM) of a synthetic foam SIJ model.
Methods: Triangular SIJ fusion implants were tested in six patterns using three implants, and two patterns with two implants (n = 5/pattern). Linear, triangular, and angled (10° or 20°) implant patterns were used with spacing of 13 or 22 mm between implants. Implants were placed through a denser polyurethane foam block (0.32 g/cm3) representing the ilium and into a less dense block representing the sacrum (0.16 g/cm3) to a depth 30 mm with a 2-mm gap between blocks. Cyclic torsion and shear testing were conducted for 10,000 cycles and ROM was recorded. Pullout testing was conducted on non-cycled (n = 10) implants and individually on all implants after construct cycling.
Results: ROM was significantly lower for all 22-mm implant patterns compared to the 13 mm linear pattern after cyclic loading in both torsion and shear. The use of three implants provided 60% and 86% greater stability, respectively, than two implants with spacing of 22 and 13 mm. Pullout resistance followed similar trends with the lowest forces occurring in closely spaced patterns that used two implants.
Conclusions: This study demonstrated that the use of three implants and maximizing the spacing between implants might provide greater stability to the SIJ. If implants must be placed closely, then nonlinear patterns may improve construct stability.
- biomechanics
- fusion
- fixation
- range of motion
- cycling
- implant spacing
- sacroiliac joint stabilization
- minimally invasive surgery
INTRODUCTION
Recent studies have demonstrated that sacroiliac joint (SIJ) pain is a significant public health burden responsible for 15%−30% of chronic low back pain.1–4 Quality of life comparisons with common medical conditions have shown SIJ patients to be in the lowest 15%, indicating the potential for drastic improvements in patient satisfaction with appropriate interventions.5 It appears that SIJ dysfunction has been an overlooked disease with misdiagnosis resulting in unnecessary and detrimental surgical interventions in the neighboring lumbar spine and hip joints.
Low treatment rates may be due to lack of awareness of the SIJ as a primary source of pain, difficulties in definitive diagnosis of SIJ pain, and until recently, the lack of effective options for surgical intervention. The treatment of SIJ dysfunction is gaining in popularity due to the recent availability of surgical treatment options that focus on minimizing motion at the joint to provide pain relief. A lateral transiliac approach is most frequently used for SIJ fusions with screw-based systems available from multiple manufacturers, although a unique fixation system consisting of triangular titanium implants with an osteoconductive coating is also commonly used (Figure 1). There is a substantial amount of published literature supporting the use of the triangular implants including retrospective case series, reviews, pooled analyses, and 3 prospective clinical trials.6–23 The results from these studies are encouraging, as patients treated with SIJ fusion have demonstrated significant improvements in pain, disability, and quality of life when compared with patients that received nonsurgical treatment.

(Left) Lateral and (right) anterior-posterior radiograph demonstrating the placement of 3 triangular titanium implants.
Despite the effectiveness of surgical treatment of the SIJ, a loss of fixation in the sacrum is a concern among surgeons and has been reported as a common fixation failure mode.20,24 Sacral bone density has been shown to vary with the highest density in the S1 body and regions of decreased density in the lateral and central sacral ala.24,25 Effective stabilization of the SIJ has been previously demonstrated in biomechanical studies with triangular implants. Soriano-Baron et al26 compared implants placed in line to those with an angled transarticular placement toward an area of higher sacral bone density. Both techniques significantly reduced motion and, although not significant, the transarticular placement provided greater stability on average. The triangular implants have also recently been studied using a finite element model to quantify the effects of implant orientation, superior implant length, and implant number on SIJ range of motion (ROM).27 The model demonstrated that the use of 3 implants, with the superior implant extending to the sacral midline, provided the greatest SIJ stability.
While fixation of the SIJ has demonstrated clinical effectiveness, questions remain as to the most effective implant configurations to stabilize the joint. The purpose of this study was to biomechanically evaluate the stability of different implant placement patterns and quantities in a synthetic foam SIJ model. The SIJ constructs were subjected to 2 different cyclic loading modalities which simulated nutation, counternutation, and shear loading.
MATERIALS AND METHODS
SIJ Foam Model
The bone density of the ilium is 2 times greater than the sacrum in vivo. Cellular foam blocks with densities of 0.32 and 0.16 g/cm3 were therefore used to represent the ilium and sacrum, respectively (Sawbones, Vashon Island, WA, model #1522-12 and #1522-10).28 The foam was cut into blocks measuring 85.7 × 61.9 × 40 mm using a table saw to ensure consistent dimensions.
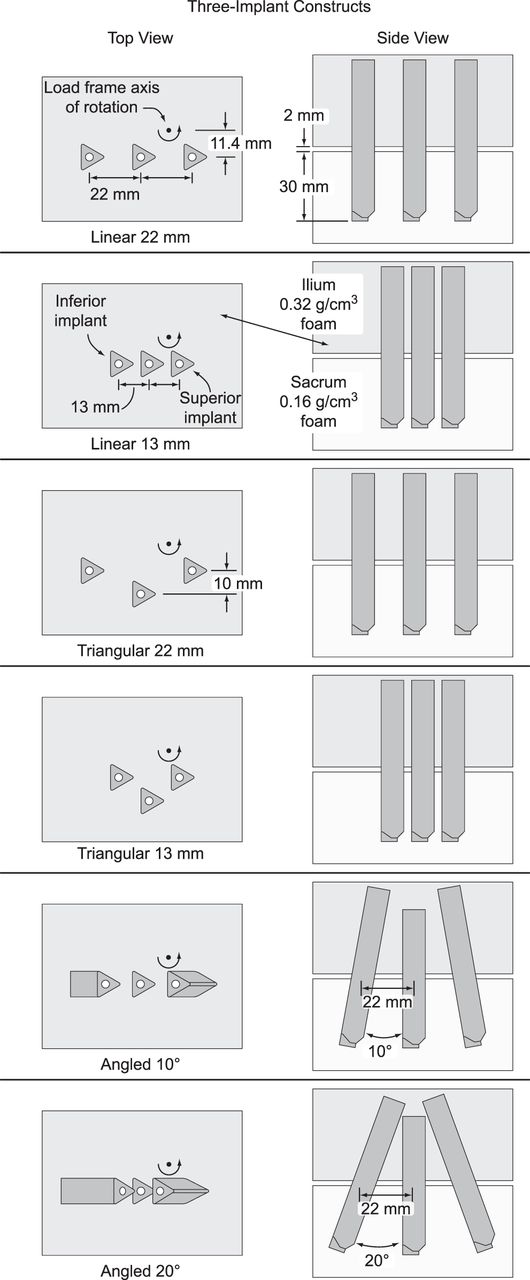
Implant configurations were chosen from those used clinically by the surgeon author (DWP) to evaluate different implant spacing, patterns, and quantities. Three-implant constructs were tested in 6 different patterns and 2-implant constructs were tested in 2 patterns. The 3-implant constructs consisted of linear and triangular patterns with 13- and 22-mm spacing between implants (Figure 2). The linear 22-mm pattern was also tested with the peripheral implants angled outwards at 10° and 20°. In the triangular patterns, the middle implant was offset 10 mm from the outer 2 implants. The linear 13- and 22-mm patterns were also tested using only 2 implants. All implants were placed to a depth of 30 mm into the sacral foam.

Configurations of constructs tested with 3 implants.
Pilot holes were drilled through the ilial foam blocks using a computer numerical control milling machine with a 7-mm drill bit. For the sacral blocks, holes were drilled several millimeters deeper than the final implant placement depth. Spacing of the implants was the same for both torsion and shear testing, although the shear constructs were angled 50° from horizontal to represent the slope of the sacrum during standing.29
The ilial and sacral blocks were aligned, clamped together, and a triangular broach was pounded through each pilot hole; residual foam particles were removed with a vacuum. A gap of 2 mm was maintained between the 2 blocks using aluminum spacers. Triangular titanium implants that were 70 mm in length (iFuse, SI-BONE, San Jose, CA) were pounded to a depth of 30 mm into the sacral foam. The 10° and 20° angled patterns used two 70-mm peripheral implants with a 60-mm implant in the middle position.
The 3-implant foam block constructs were tested with 6 patterns in torsion (n = 5/pattern) and with 4 patterns in shear (n = 5/pattern); the 10° and 20° angled patterns were not tested in shear (Table). The 2-implant constructs with 13- and 22-mm patterns were only tested in torsion (n = 5/pattern).
Sample sizes used for testing in each implant pattern and loading modality.
Cyclic Torsion Testing
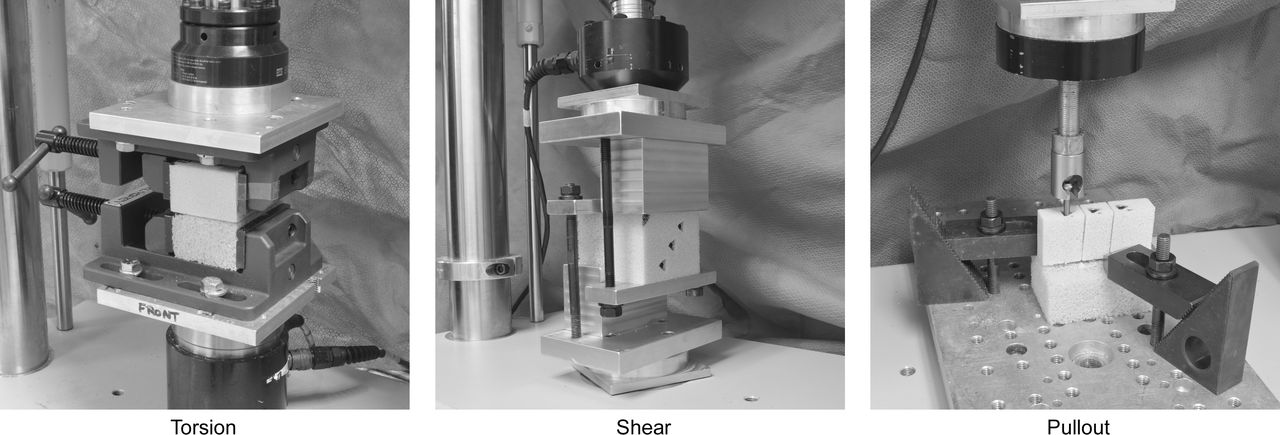
Vises were secured to a biaxial load frame (858 Mini Bionix, MTS, Eden Prairie, MN) using custom fixtures to position the axis of rotation approximately 11 mm posterior to the superior implant (Figure 3). Cyclic torsion testing was conducted using a sinusoidal waveform at ±7 Nm for 10 000 cycles at 1 Hz. ROM tests were conducted at a slower rate of 0.5 Nm/s to ±7 Nm following 10 cycles of initial preconditioning (0 cycles) and at 10 000 cycles; timed data were acquired at 50 Hz.
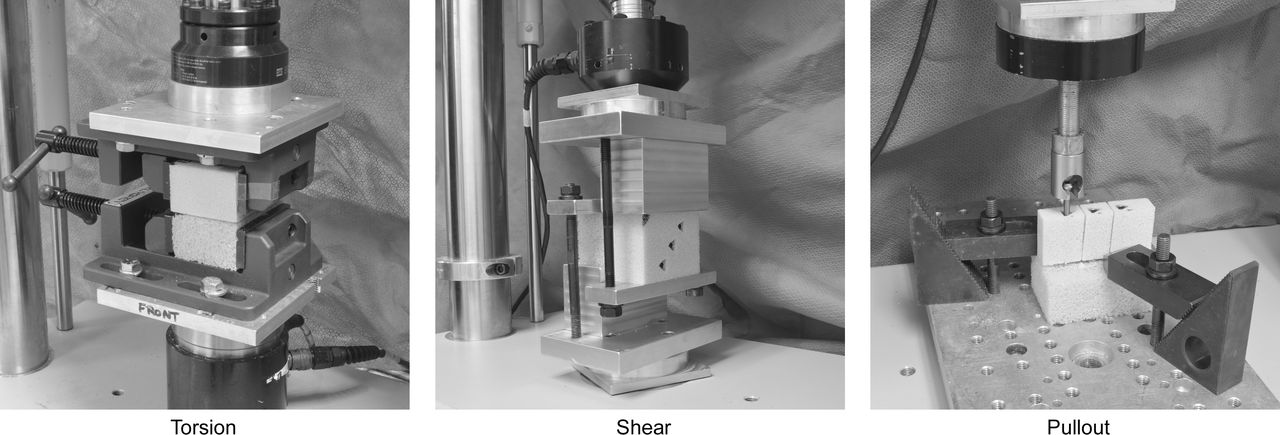
Test setups for cyclic torsion, cyclic shear, and implant pullout tests.
Cyclic Shear Testing
Shear testing was performed by positioning the long axis of the implants perpendicular to the actuator of the load frame with the test block construct angled 50° from horizontal to represent the slope of the sacrum during standing. The blocks were tightened with the load frame in load control to ensure that no unintended loads were induced. Cyclic shear testing was conducted using a sinusoidal waveform in compression from −300 ± 200 N for 10 000 cycles at 1 Hz. ROM tests were conducted for 1 cycle at a slower rate of 50 N/s from −300 ± 200 N after 10 cycles of initial preconditioning (0 cycles) and at 10 000 cycles; timed data were acquired at 50 Hz.
Pullout Testing
After the completion of cyclic testing, the ilial foam was cut using a band saw between each implant to allow for independent pullout tests on each implant (Figure 3). A machine screw was threaded into the open end of the implant, and the head of the screw was placed into a pullout fixture attached to the load frame actuator. The sacral block was secured with clamps to an aluminum plate. The angled constructs were clamped in a vise with the implant positioned vertically to allow for pullout in line with the primary axis of the implant. Pullout tests were also conducted on noncycled control implants (n = 10) placed 30 mm deep into a block of sacral foam. Pullout testing was conducted at 5 mm/min with data acquisition at 30 Hz.
Data Analysis
Custom computer code (Matlab, Mathworks, Natick, MA) was used to calculate ROM in torsion and shear at 0 and 10 000 cycles. Construct ROM was calculated as the difference between the maximum and minimum rotation (torsion) or displacement (shear). Peak pullout forces were also calculated.
Statistical Methods
Statistical differences in torsion and shear ROM were evaluated by performing a 2-way repeated measures analysis of variance (ANOVA; Prism 5, GraphPad, San Diego, CA). Torsion ROM data for the 2- versus 3-implant constructs were also analyzed using a 2-way repeated measures ANOVA. The pullout data between all configurations were evaluated using a standard ANOVA. Statistical significance was declared at P < .05.
RESULTS
Torsion—ROM
The ROM was significantly lower for the linear and triangular 22-mm patterns than both the linear and triangular 13-mm patterns at 0 and 10 000 cycles (P < .05, Figure 4). The pattern with 10° implant angles had significantly less ROM than the linear and triangular 13-mm patterns at both 0 and 10 000 cycles (P < .01). The pattern with 20° implant angles only experienced a significant reduction in ROM versus the linear 13-mm pattern at 10 000 cycles (P < .01). The initial ROMs for patterns with 22-mm implant spacing ranged from 2.0 ± 0.4° for the triangular pattern to 2.9 ± 0.6° for the pattern with 20° implant angles. ROM increases for the 22-mm implant spacing ranged from 0.9° (triangular) to 1.4° (angled 20°) after cyclic loading. The two 13-mm patterns had similar initial ROMs of ∼3.6°, which increased to 5.5 ± 0.5° for the 13-mm triangular and 6.0 ± 1.1° for the 13-mm linear patterns after cyclic loading. The linear 13-mm pattern allowed 81% more ROM than the 22-mm triangular pattern at 0 cycles and allowed 106% more ROM after 10 000 cycles.
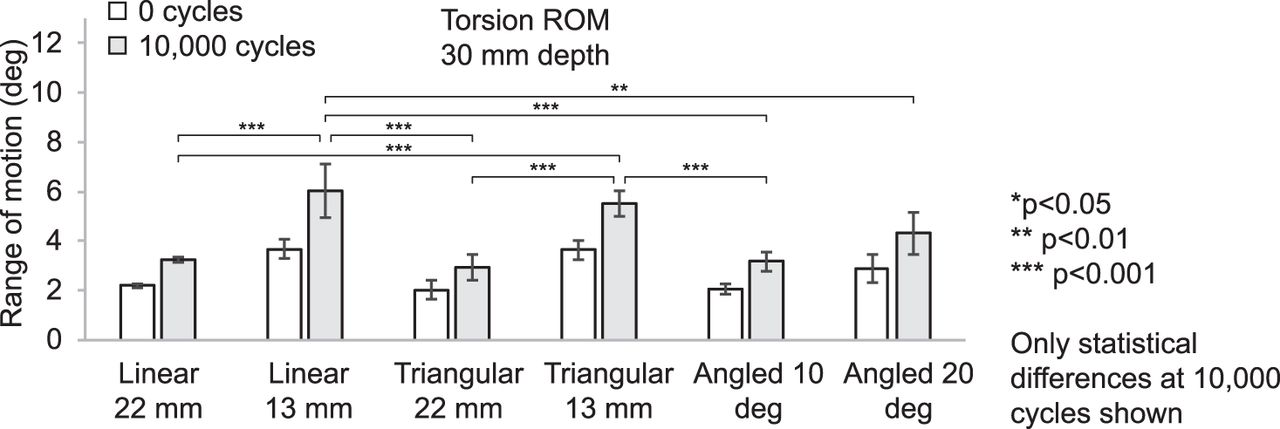
Construct range of motion (average ± SD) in torsion for all patterns. **P < .01, ***P < .001.
Torsion—ROM, 2 Versus 3 Implants
The 2-implant patterns exhibited greater ROM at both 0 and 10 000 cycles than the 3-implant patterns, although differences were only significant at 10 000 cycles (Figure 5). The 2-implant patterns had noticeably more toggle between the blocks than 3-implant patterns at the completion of cyclic loading, particularly in the 13-mm linear pattern. Gap formation and widening of the broached holes was observed in the sacral foam of the 2-implant linear 13-mm pattern after cyclic loading. After 10 000 cycles, the 3-implant linear 22-mm pattern had a ROM of 3.3 ± 0.1°, while the 2-implant pattern was 8.4 ± 2.2° (P < .05). The 2-implant 13-mm linear pattern had a large increase in ROM after 10 000 cycles to 43.8 ± 6.4°, while the 3-implant pattern was 6.0 ± 1.1° (P < .001).

Torsion range of motion (average ± SD) comparing configurations using 2 versus 3 implants at 0 and 10 000 cycles. *P < .05, ***P < .001.
Shear
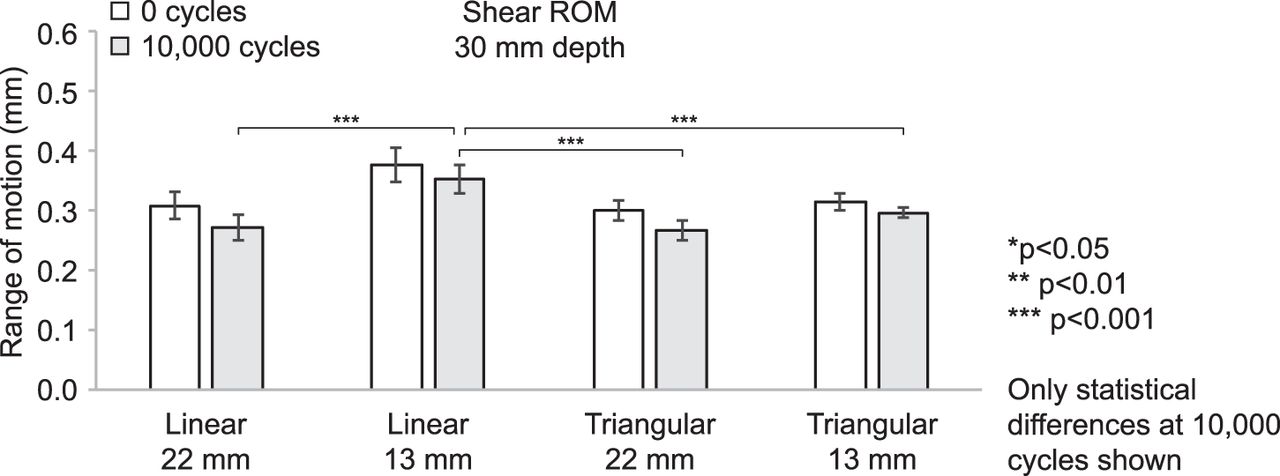
ROM was significantly greater for the linear 13-mm pattern than all other patterns at both 0 and 10 000 cycles (P < .001, Figure 6). ROM for the 13-mm linear pattern at 10 000 cycles was 0.35 ± 0.02 mm compared with 0.27 ± 0.02 mm for the linear 22 mm, 0.30 ± 0.01 mm for the triangular 13 mm, and 0.27 ± 0.02 mm for the triangular 22 mm, respectively.

Construct range of motion (average ± SD) in shear for linear and triangular patterns. ***P < .001.
Pullout
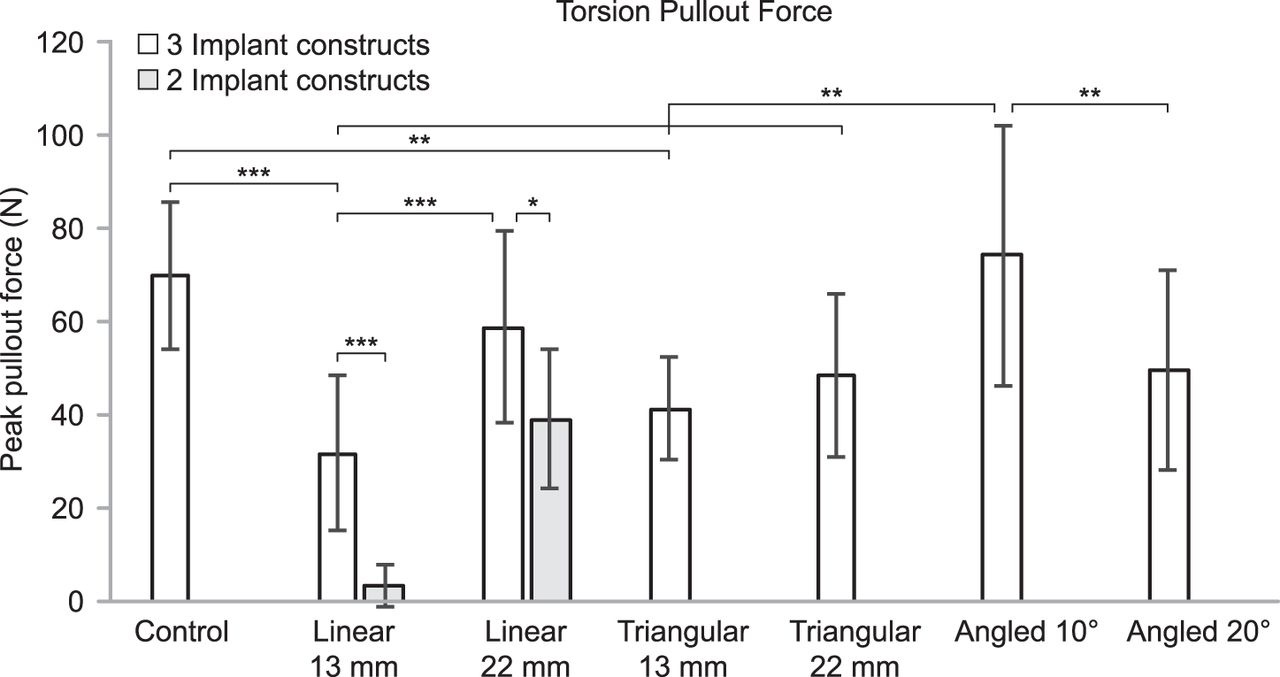
The noncycled control implants had an average pullout force of 70 ± 16 N (Figures 7 and 8). The lowest pullout forces for 3-implant constructs occurred in the linear 13-mm pattern at 32 ± 17 N, while the greatest force was in the angled 10° pattern at 74 ± 28 N. The linear and triangular 22-mm patterns had pullout forces of 59 ± 21 and 49 ± 18 N, respectively. Pullout forces in the 2-implant patterns were 4 ± 5 and 39 ± 15 N for the 13- and 22-mm spacing, respectively

Peak pullout force (average ± SD) on noncycled control implants (n = 10) and after cyclic torsion testing (n = 15 for each pattern). *P < .05, **P < .01, ***P < .001.

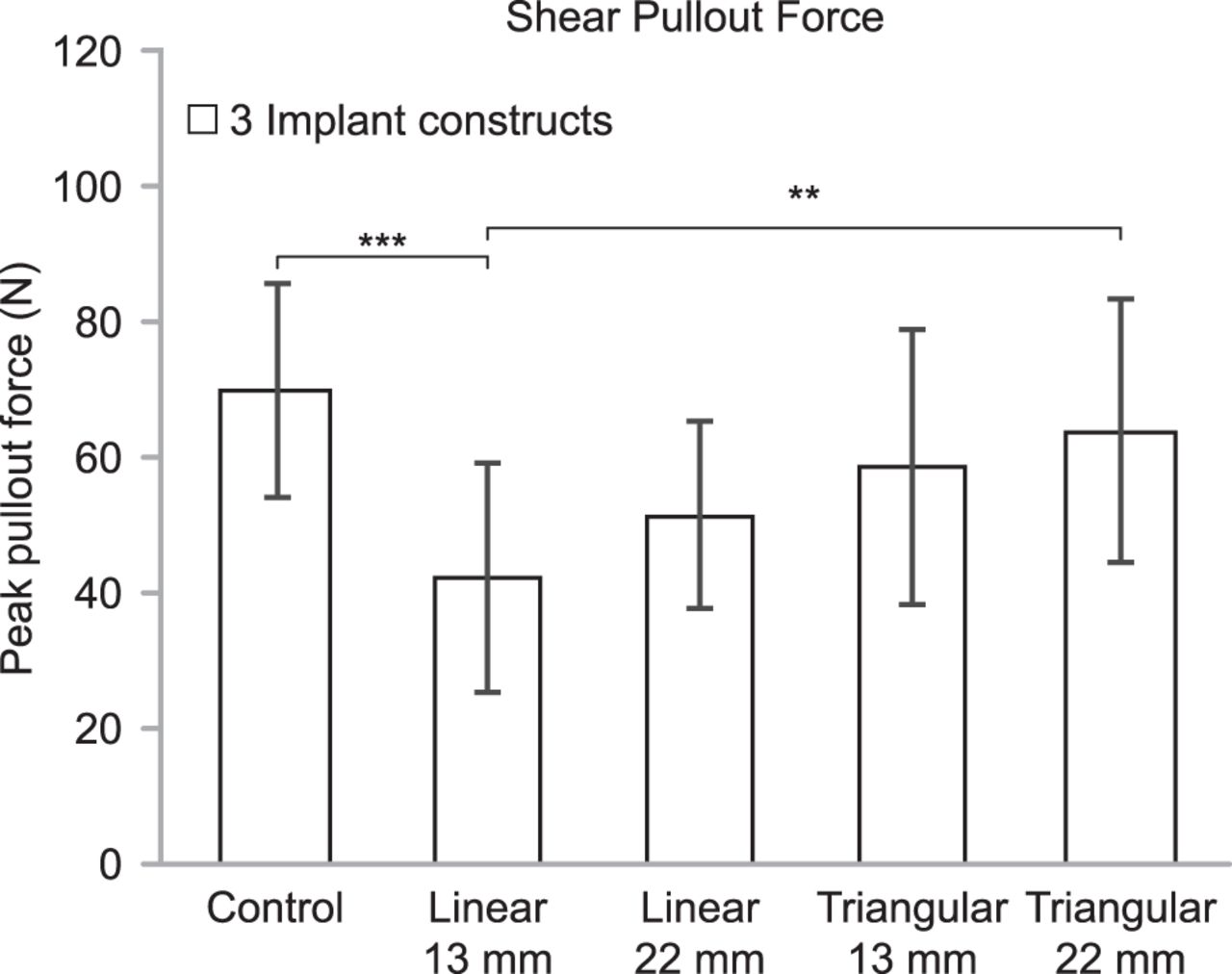
Peak pullout force (average ± SD) on noncycled control implants (n = 10) and after cyclic shear testing (n = 15 for each pattern).
DISCUSSION
The results of this study suggest that there are several implant placement strategies that may be beneficial to enhance the stability of SIJ fusions. The spacing between implants (13 or 22 mm) had a larger effect on the biomechanical performance than the implant pattern (linear versus triangular) in both torsion and shear testing. The test configurations with 22-mm spacing between implants had significantly less ROM and greater pullout loads than configurations with 13-mm spacing. There were no statistical differences in the torsion and shear outcome data between the linear and triangular patterns with 22-mm spacing. At the 13-mm spacing, the triangular pattern tended to perform better than the linear pattern, and there were several significant differences in ROM and pullout data for both torsion and shear. These data indicate that greater stability can be expected when spacing between implants is increased.
Although 3 implants are recommended to provide improved SIJ stability, there are certain cases where this may not be feasible and only 2 implants can be placed. In a recently completed randomized controlled trial using the implant evaluated in the present study, 5% of patients received 2, 91% received 3, and 4% received 4 implants.20 To determine how the number of implants may affect SIJ stability, the present study tested 2-implant constructs cyclically in torsion with 13- and 22-mm spacing between implants. The 2-implant constructs had greater motion and reduced pullout strength than the 3-implant constructs with significant differences after 10 000 cycles. At the completion of cyclic loading, the 22- and 13-mm 2-implant constructs allowed 2.5 to 7.3 times more ROM, respectively, than the 3-implant constructs. The 2-implant constructs with 13-mm spacing were extremely loose with a 44° ROM and almost no resistance to pullout forces (4 N). Based on these data, the use of 3 implants is advised, but if only 2 implants can be used, they should be spaced as far apart as possible to provide greater SIJ stability.
The ROM values in the present study for both torsion and shear were consistent with previously published cadaveric biomechanical studies.26,30–32 In a cadaveric study, Lindsey et al30 reported flexion-extension ROM ranging from 1.6° to 6.4° for specimens implanted with 3 triangular titanium implants, which compares favorably to the 2.0°–6.9° ROMs for the noncycled 2- and 3-implant constructs in the present study. The vertical displacement of the SIJ was measured in a cadaveric study by Dujardin et al32 to be 0.22 to 0.35 mm under an applied load of 310 N. Although a higher shear load was used in the current study (500 N), the displacement of our SIJ construct was similar with a range of 0.30 to 0.38 mm. The 7 Nm moment applied during torsion testing was similar in magnitude to other cadaveric biomechanical studies where specimens were cyclically loaded using moments from 3.75 to 7.5 Nm or tested for flexibility (no cycling) at 7.5 Nm.26,30,31
Authors of a finite element analysis (FEA) of the SIJ evaluated in line and transarticular placement of triangular titanium implants with a varying number of implants (1, 2, or 3) and superior implant lengths.27 Authors of this FEA study found a reduction in SIJ ROM using a transarticular implant placement, longer superior implants, and a greater number of implants. Compared with in-line placement, the transarticular technique only affects the middle implant in that the starting point is ventral to the anterior sacral body and aimed posteriorly across the cartilaginous area of the SIJ. The triangular configurations in the present study are like a transarticular placement but maintain parallel positioning of all implants. The data from the current study support the findings of the FEA study in that SIJ stability was improved with a greater number of implants, increased spacing between implants, and nonlinear implant configurations.
As with all biomechanical studies, there are several limitations that must be considered. A foam model was chosen to provide a simplified simulation of the SIJ so that variability could be minimized between test constructs. The implant spacing (13 and 22 mm), angulation (parallel, 10°, or 20°), and offset (10 mm) were based on the clinical experience from more than 200 primary SIJ fusion cases performed by the surgeon author. The implant configurations were chosen to represent a range of options that are suitable for differing patient anatomy. The use of cadaveric specimens would have introduced significant variations in bone quality, anatomy, and native ROM that would have made consistent implant placement difficult and increased the variability in the data, which may have masked differences between test groups. The loading used in this study was not intended to replicate the complex in vivo motion of the SIJ but to simulate the worst-case loading of implants. Nutation and counternutation (torsional loading) is the largest motion in the SIJ and has been suggested as being responsible for implant loosening; therefore, more tests were conducted in this loading mode.33 This model is also not capable of characterizing any biological responses, such as bone ingrowth, that occur in vivo. Although the quantitative results from this study may differ from clinical values, the qualitative differences between constructs are expected to behave similarly in the human SIJ.
This biomechanical study has demonstrated that the stability of SIJ fusions may be improved by considering how implants are configured. The number of implants had the largest effect on construct stability, and the use of 3 implants instead of 2 is preferable for both short- and long-term stability. Increasing the spacing between implants reduced ROM, particularly when only 2 implants were used. The use of nonlinear implant configurations may provide additional stability. Placement of implants in nonlinear and angled configurations may require the use of advanced imaging and robotic navigation systems. The application of these results to clinical use should be further evaluated in future studies.
Footnotes
Disclosures and COI: The authors acknowledge SI Bone for donation of the implants and financial support.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.