


Abstract
Background Following total sacrectomy, the continuity between the spine and pelvis is necessary for ambulation and to enable patients to resume daily living activities sooner during rehabilitation. Reconstructing spinopelvic stability after a total sacrectomy is a challenge that has not yet been overcome. Thus, the objectives of the present study are as follows:
Establish a new system of reconstructing the spinopelvic region after a total sacrectomy using a rapid prototyping technique to design the sacral replacement pieces.
Evaluate the biomechanical properties of this system.
Study a new reconstruction system for the spinopelvic joint that reduces reconstruction failures after total sacrectomy, reducing postoperative complications and allowing early sitting and standing of these patients.
Methods A sacral replacement implant was designed according to an authentic clinical case of a patient who had undergone a total sacrectomy. Using the finite element method, a biomechanical study was carried of 2 reconstructions that had been performed using the new prosthetic. The results of the study were compared with 4 other reconstruction models.
Results A maximum von Mises stress of 112 MPa and a vertical displacement of −0.13 mm in L5 were observed in the models of the sacral implant that had been generated. A maximum rigidity of 861.5 Nm/mm was observed in the models when assuming a reduction in rigidity of more than 85% with respect to the other models assessed. In all models, maximum tension was concentrated in the rods joining L5 with the screws anchored to the pelvis.
Conclusions The sacral prosthesis substitution after a total sacrectomy produced a profound reduction in stress in the instrumentation and the bone structure as well as smaller vertical displacement, the lowest values ever reported. These results indicated that the assembly was rigid and stable and would prevent the collapse of the spine in the pelvis. According to stress values, the replacement piece was not likely to rupture as a consequence of static load or implant fatigue.
Level of Evidence 5.
- total sacrectomy
- biomechanics
- finite element analysis
- spinopelvic reconstruction
- spinopelvic stabilization
- tumors of the sacrum
Introduction
Reconstructing spinopelvic stability after a total sacrectomy is a challenge that has not yet been overcome. The aims of the present study were to:
Design a new system for reconstructing spinopelvic stability after a total sacrectomy.
Analyze the biomechanical properties of this new system and compare them with properties of systems already reported.
Study a new reconstruction system for the spinopelvic joint that reduces reconstruction failures after total sacrectomy, reducing postoperative complications and allowing early sitting and standing of these patients.
This novel system consisted of using a rapid prototyping technique to fabricate a sacral replacement piece from solid and porous titanium.
Materials and Methods
The experimental biomechanical study consisted of designing a sacral prosthetic implant and comparing it with other systems of spinopelvic stabilization using the finite element method (FEM). This study was supported through a fellowship from the Society for the Study of Spinal Diseases (GEER) and was approved by the hospital’s ethical committee.
Designing and Fabricating the Assembly
The sacral replacement piece was designed using a 3-dimensional (3D) model of the spine, pelvis, and upper segments of the sacrum. This model was constructed using the preoperative computed tomography (CT) image of a 50-year-old man undergoing total sacrectomy and instrumented spinopelvic reconstruction (Figure 1). We used the preoperative CT to segment the 3D STL file by MIMICS 17, then converted the mesh back to computer-aided design, making the design modification of sacral prosthesis by 3-MATIC 9.0. The slice thickness of the preoperative CT was 1 mm.

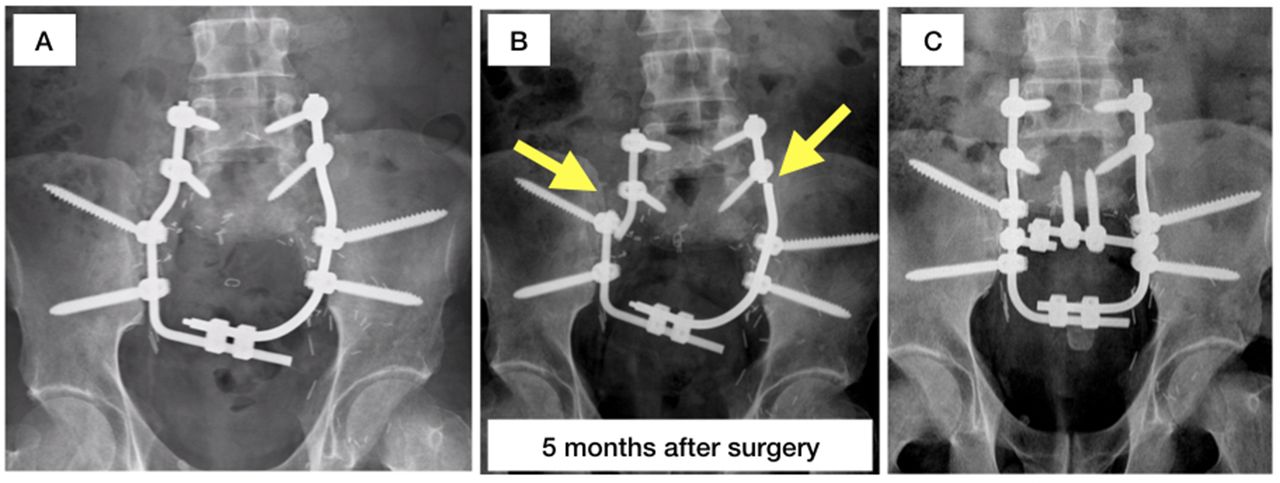
Clinical case. During the initial surgery, reconstruction was performed according to model 2 (A). After 5 mo, the rods broke at the fusion site of the L5 pedicle screws and the proximal iliacs (B). A second reconstruction was subsequently performed on the basis of model 4 (C).
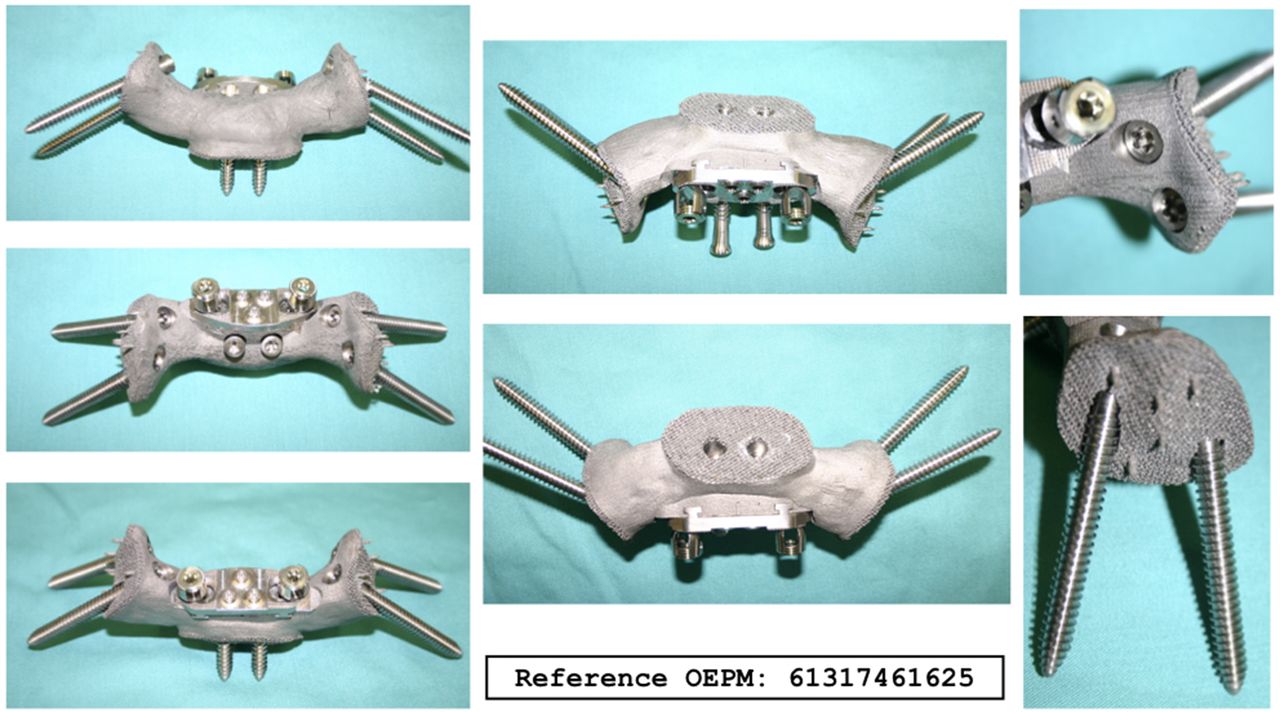
The replacement piece simulated the morphology of the S1 vertebra. It had holes fitting 2 screws used for fixing the lower plate of L5 vertebra and both ends of the iliac bone. In addition, it had a flat posterior surface where 2 vertical rods were fixed to the pedicle screws at the L4 and L5 vertebrae (Figure 2).
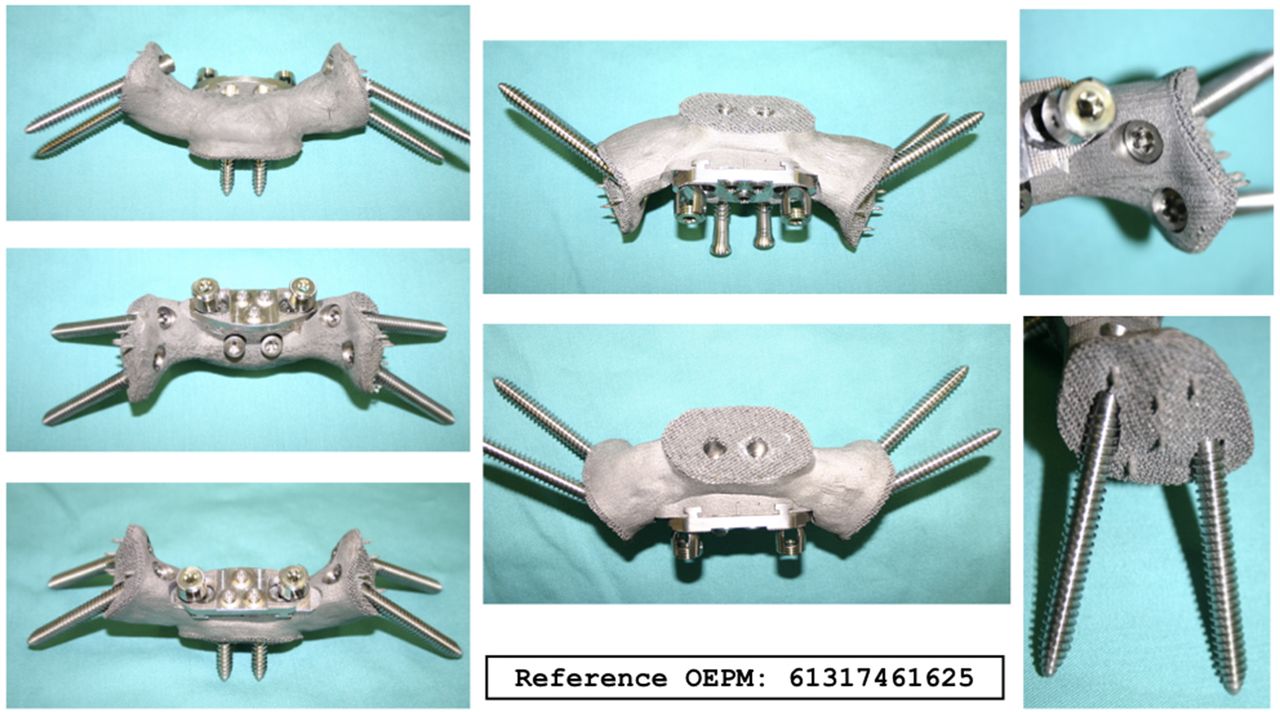
Sacral prosthesis substitution.
The piece consisted of a core of solid titanium surrounded by porous titanium. The porous layer made contact with the pelvis and the vertebral column. The implant was manufactured from Ti6Al4V titanium alloy, using the model of the patient’s pelvis as guide and the 3D-matic software (Materialize). The implant was fabricated by rapid manufacturing technology with 3D metal printer. The pore sizes of the porous titanium was between 400 and 700 μm.
Studies Using the Finite Element Model
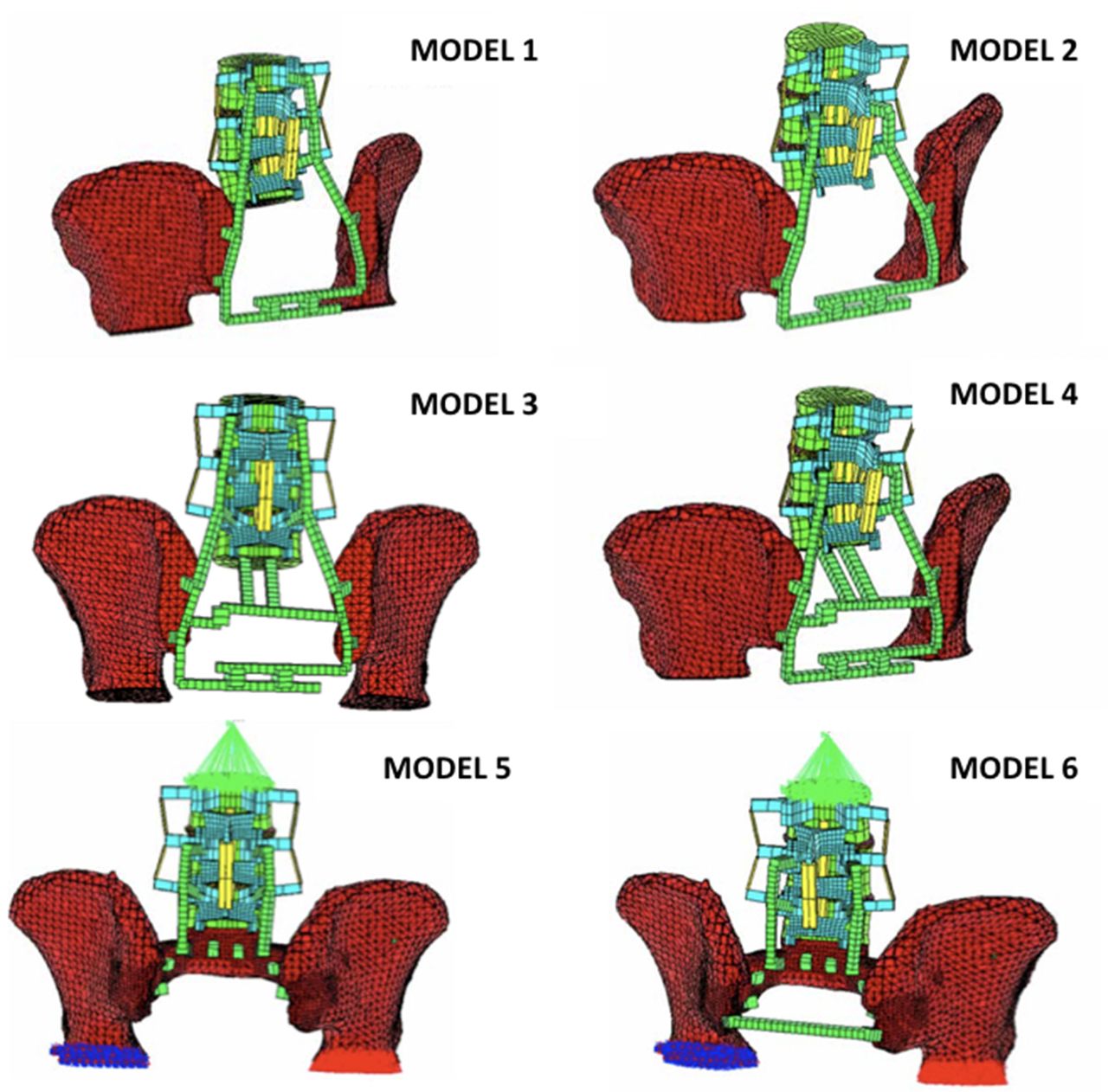
A total of 6 models of the reconstruction were analyzed. The models were based on the aforementioned clinical case (Figure 3).

Finite element models.
Model 1: Reconstruction with 2 L-shaped rods joined together in the shape of a fork with 2 connectors, 2 pedicle screws in L3, L4, and L5 vertebrae, and 2 bilateral iliac screws.
Model 2: Same as in model 1 but without the pedicle screws in the L3 vertebra.
Model 3: Reconstruction with 2 L-shaped rods joined together in the shape of a fork with 2 connectors, a proximal connecting rod between the rods with 2 screws to the body of L5, and 2 pedicle fixation screws in the L3, L4, and L5 vertebrae.
Model 4: Same as in model 3 but without the pedicle screws in the L3 vertebra.
Model 5: The sacral replacement piece was fixed to the spinal column with pedicle screws in the L4 and L5 vertebrae, 2 bilateral iliac screws, 2 pedicle fixation screws in the L5 vertebra, and 2 vertical rods joining the pedicle screws to the piece.
Model 6: Same as model 5 but with a transiliac rod.
Modeling Anatomical Structures and the Implants
The finite element software ANSYS 12.1 was used to model anatomical structures. A model was generated of the lumbar spine along with the L2-L5 vertebrae. The FEM modeling was validated by the Biomechanics Institute of Valencia.1
Using rod elements, ligaments were meshed with I-DEAS program. The mesh was subsequently exported to the ANSYS 5.5 program. The behavior of the mesh was simulated using LINK10 cable elements. The cortical bone of the pelvis was meshed using shell elements.2
The implant modeling was carried out using 2-node unidimensional rod-like elements (BEAM4). Fastener and material properties are laid out in Tables 1 and 2, respectively.
Properties of attaching elements: diameter of element and type of material.
Properties of the materials cobalt-chrome, titanium, and porous titanium, as determined by the Biomechanics Institute of Valencia.
The screws and connectors were manufactured out of Ti6Al4V titanium alloy. The rods were made of CoCr.
The TARGE170 target segment and CONTA173 element were used to model the point of contact between the titanium sacrum and the pelvis.
Applying Loads
An average vertical compressive load of 500 N was applied to the lumbar spine in standing position, at the center of the upper surface of the vertebral body of L2.3–5
Parameters Taken Into Account in the Analysis
The vertical descent of L3, L4, and L5 was determined according to the vertical displacement, in mm, of the upper plates of L3, L4, and L5 with respect to the position of the column before the loads were applied.
The stresses that supported the implants were expressed in von Mises stress values (in Nm).
The rigidity of the systems was calculated from the maximum von Mises stress value and the vertical displacement of L5. This was measured in Nm/mm.
The distribution of tension in the instrumentation and bone structures was taken into account.
The modified pelvic incidence (mPI) of the patient was determined prior to undergoing total sacrectomy, after undergoing sacrectomy, as well as the mPI in models 2 and 4 that were derived from the CT. The mPI was measured according to the intersection between the line running from the center of the femoral heads to the midpoint of the lower saucer of L5 and a line running perpendicular to the center of the inferior lower endplate of L5.6
The theoretical mPIs in models 5 and 6.
Results
The smallest displacements were observed with models 5 and 6 (Table 3).
Vertical displacement according to each model.
The highest value observed for the maximum von Mises stress in the implants was for models 1 and 2 (Table 4).
Maximum von Mises stress values in the implants, according to each model.
The lowest maximum von Mises stress was observed in models 5 and 6 (Table 4). In these models, using the sacral substitution piece led to a 91% reduction in tension compared to models 1 and 2 and an 86% reduction compared to models 3 and 4. The most pronounced rigidity was observed in models 5 and 6 (Table 5).
Rigidity values according to each model.
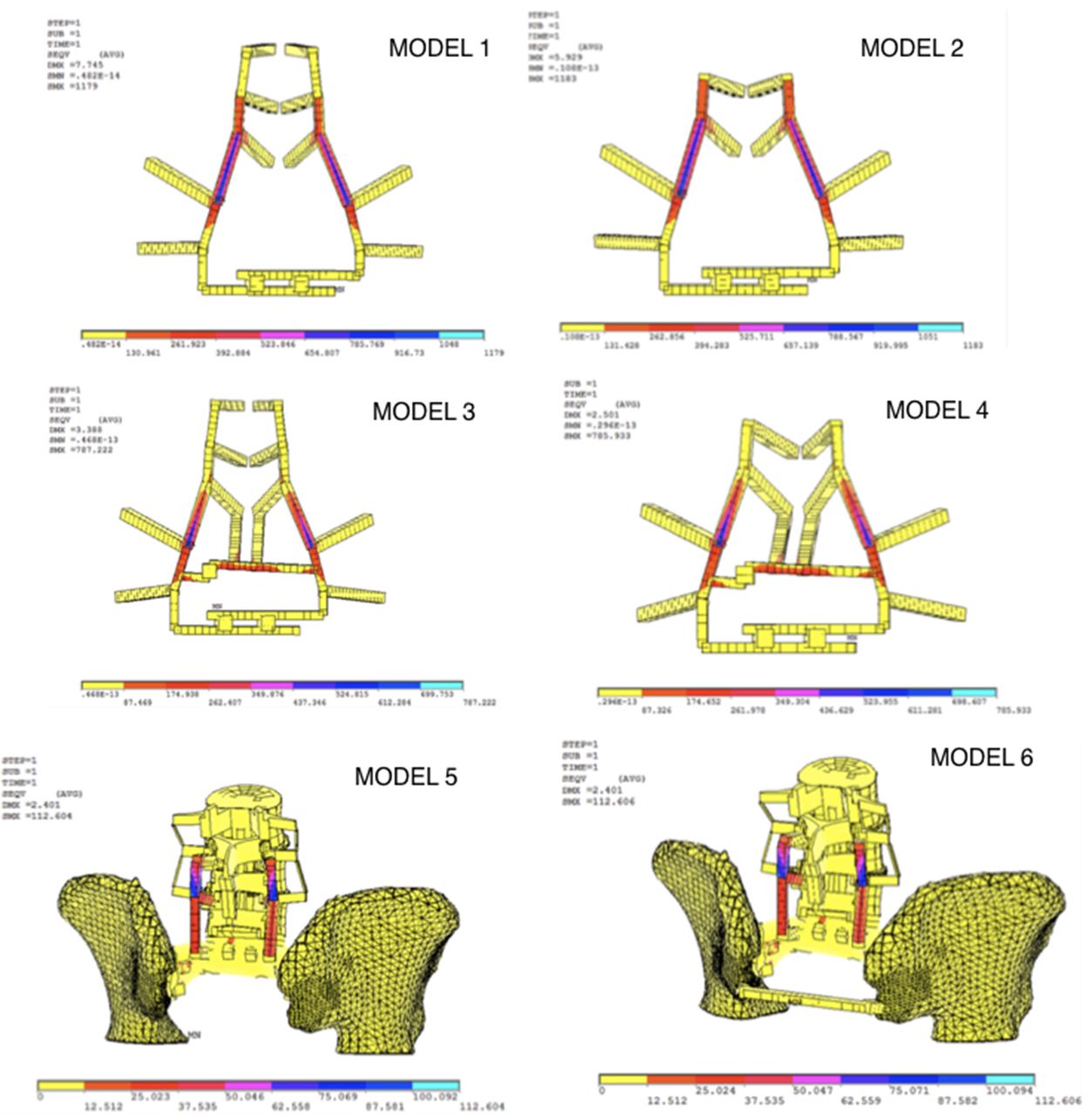
The distribution of the maximum stress values is shown in Figure 4. In models 1, 2, 3, and 4, the highest values for maximum concentrated tension were observed in the rods connecting L5 with the screws anchored to the pelvis.

Stress distributions resulting from application of loads in the finite element models.
In models 5 and 6, the patient’s preoperative mPI was found to be preserved (Table 6).
Modified pelvic incidence values for each reconstruction.
Discussion
Models 5 and 6 of the sacral substitute showed the piece’s smallest vertical L5 displacement and the highest rigidity values ever described for FEM biomechanical studies (Table 7).
Literature review of finite element model studies of spinopelvic reconstructions following total sacrectomies and a comparison with the results of the present study.
The largest displacement values were observed with models 1 and 2: 5.08 and 5.15 mm, respectively. Smaller values were observed with models 3 and 4: 1.69 and 1.7 mm, respectively. Models 3 and 4 had an anterior column and 2 screws driven into the body of L5. Meanwhile, in models 5 and 6, displacement values of only 0.13 mm were observed. In the latter models, a sacral replacement piece was included. These results reaffirm the importance of having anterior support of the spine when reconstructing lumbopelvic stability, which was examined in previous studies.3,10,11
The system that is the least rigid is the four-rod reconstruction (FRR), which is a spinopelvic fixation system that does not include anterior support of the column nor fixation of the iliac bones (Table 7).5 Triangular frame reconstruction (TFR) and modified Galveston reconstruction (MGR) are systems that do not include anterior support. However, we cannot make a comparison with TFR and MGR because no data are available. In our study, models 1 and 2 have displacement values close to, but not as high as, those observed with FRR: 7.2 mm.5 The reduction in vertical displacement is likely due to the joining of the 2 rods, which would distribute the tension in the posterior part.
Morphologically, models 3 and 4 only differ from 1 and 2 in the anterior support provided by the screws fixed to the body of L5. This technique was initially described by Kawahara et al9 as part of the sacral rod reconstruction system (SRR). In the SRR, the L5 body screws are joined to a transiliac rod. Subsequently, this element was conserved in the improved compound reconstruction (ICR) system.3,5 The ICR includes 2 fibula support grafts connecting the L5 to pelvis dish. According to Cheng et al,3 the ICR system provides more stability than bilateral fibular flap reconstruction (BFFR), a similar model that lacks the transiliac rod and the L5 body screws.
The models that provide the highest stability are ICR followed by BFFR.3,5 However, both systems require long surgical times, are technically complex, and are associated with a high incidence of pelvic organ injury.3,5 The sacral replacement piece in our model should be much simpler to use, since it is customizable to the patient. In addition, all the holes for iliac bone and L5 body screws are made in a mechanized fashion, decreasing the technical complexity, surgical times, number of instruments required, and the frequency of associated complications, including pelvic organ injury, among others.
Models 3 and 4 showed double the rigidity that was seen with models 1 and 2, while models 5 and 6 had triple the rigidity. Reported ICR rigidity values are close to that seen with models 1 and 2, as well as the other models we studied.
The models that included replacement parts showed much higher rigidity values than ever described in the literature. Too much rigidity can be a problem, however. Micromotions are blocked, preventing the stimulation of fusion. However, microporosis of the sacral implant piece could promote osteoinduction, osteoconduction, and osseointegration.
Having a high level of stress applied to the implants or the bone structure increases the risk of rupture and/or loosening of the implants. The highest maximum von Mises stress value was observed in models 1 and 2: 1179 and 1182 MPa, respectively. These stress values were comparable with the 1042 MPa observed with the MGR system8,9. Likewise, in both systems, the zone of maximum tension was observed in the same areas in the instrumentation: around the column rod and between the L5 screw and iliac screw of the column.8
Models 3 and 4 had lower maximum stress values than seen with MGR; however, the values seen with 3 and 4 were greater than the values that observed with BFFR, ICR, TFR, FRR, and SRR. The lower values were likely a consequence of the tension being distributed in lumbar column via the L5 body screws that were connected to the transverse connectors.
Models 5 and 6 contained the sacral replacement piece. The maximum stress values from both these models equaled 112 MPa. This is below the breaking stress of the Co28Cr6Mo and Ti6Al4V materials (Table 2). This low value reflects a reduced risk of implant breakage and fatigue that results from the application of static loads. This result contrasts with the high stress values of reported systems. The reported systems fail soon after implantation and the commencement of physical activity. The maximum stress of the sacral substitute piece was 112 MPa. This value is comparable with the lowest finite elements value reported to date: 108 MPa for ICR.5 This result was surely due to a change in the load distribution. The axial loads exerted on the lumbar spine are distributed widely and harmoniously over the section replacing the S1 vertebra. The pressure to the iliac and sacroiliac joint is thus partially recreated. From there, the pressure is transmitted to the hip joint. Thus, the load transmission in models 5 and 6 is more anatomical than other reconstructions. Importantly, the area of union between L5 and pelvis is found to be a zone of weakness both in the published models and our own.
One of the advantages of using a sacral substitution piece in models 5 and 6 is its theoretical capacity to maintain the mPI. The pelvic incidence (PI) is a fixed measure of the relationship between the pelvis and the sacrum. The PI is unique in each individual and remains constant postadolescence.7,12,13 Changes in the PI lead to changes in spinopelvic stability.6
The limitations of the study are as follows:
The model represents only the size and weight of an average European man.
In order to perform the modeling, the regions and the reconstructions had to be simplified. The finite element analysis models not include simulation of all ligaments and muscle forces of the lumbosacral spine.
The connection between the screws, the rods, and bones was assumed to be rigid, which is not really true.
Since 1D beam interpretation was used and the screws and bone were analyzed as one rigid unit, the models don’t account for stress failure of any connecting parts, which are usually crucial points of failure clinically.
The material properties are more profound than the assumptions that have been made.
Only axial loads were studied. Flexion, extension, and rotation moments were not taken into account.
In order to investigate the risk of implant loosening, we assumed it to be associated with the force along the main axis of the implant at the implant-bone interface but it was not validated in clinical setting. The interpretation of risk of loosening should be considered only in qualitative terms.
The results of the study are valid for the average patient but may differ between specific individuals.
It should be noted that these technologies (finite element analysis, 3D printing, computer-aided design, and surface meshing) are time-consuming and complex to design, create, and validate for specific patients. Although there are upcoming automations that will facilitate this process, they are still under study and are not affordable now. Hence, the appropriate case selection for these technologies is the complex, difficult, high risk, and high skill demand cases, such as a sacrectomy.
The sacral prosthesis could present a good behavior once implanted, reconstructing the anterior column, avoiding overloads in the spine or pelvis, increasing fusion rates, being able to reduce the number of revision surgeries due to instrument failure and allowing an early mobilization of the patient.
Compared to the systems published, the sacral prosthesis is easier to implant, and less instrumentation, which would lead to a reduction in surgical time and postoperative complications (infection, bleeding, visceral injury, etc). Clinical studies are necessary to assess the effects of the implantation of the sacral prosthesis.
Conclusions
In this finite elements study, the sacral replacement piece was shown to cause an important reduction in stress in the instrumentation and bone structure. In fact, these stress values are the lowest ever reported. These results demonstrate the high rigidity and stability of the replacement piece and the theoretical capacity of the piece to prevent the collapse of the spine in the pelvis. The lowest maximum von Mises stress seen with the replacement piece is indicative of a low risk of rupture due to static loads or implant fatigue.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}