


Abstract
Background Discectomy is the surgical treatment of choice for disc herniation. However, discectomy can lead to disc degeneration and vertebral instability over time. Interspinous devices (ISDs), added to conventional surgery, constitute a low-invasive alternative that attempts to prevent these complications. The aim of this study is to compare the long-term clinical and functional outcomes of patients undergoing conventional discectomy with those who had an ISD added during surgery.
Methods This analytical-descriptive, retrospective, and transversal studyinvestigated outcomes of 114 patients who underwent surgery for a lumbar disc herniation between 2008 and 2011. The results were evaluated with a minimum follow-up of 8 years (mean, 10 years) by means of different questionnaires: visual analog scale (VAS), Oswestry Disability Index (ODI), consumption of analgesic medication, work status, degree of satisfaction, and complications and reinterventions during the follow-up period.
Results At the end of the follow-up, an overall improvement of VAS of 5 points (71%) and ODI of 36 points (77%) was observed, with a degree of satisfaction of 76% with disc surgery. The analysis between both groups showed a better behavior in VAS and ODI in the implant group, with a pre- and postsurgery difference of 73% and 79% compared to 66% and 77% in the control group, respectively, though this finding was not statistically significant. The current analgesic consumption and the degree of satisfaction were also better in the group with an implant. Compared with the non-implant group, the number of reinterventions at the end of the follow-up was lower (7% vs 15.5%) and the time until the second intervention was higher (81.5 vs 41 months) in the group with an implant, but the differences were not statistically significant.
Conclusions Lumbar discectomy proved to be a safe technique for the treatment of disc herniation, and results are maintained over time. The additional gesture of adding an ISD to conventional discectomy improves clinical outcomes overall, but not in a statistically significant way. The lower number of reinterventions and the longer period without surgery being required may mean a certain protective effect of the ISD on the intervertebral disc being operated on.
Introduction
The annual incidence of sciatica is around 2% of the population.1 Persistent sciatica is the primary surgical indication in most cases of lumbar disc herniation. Discectomy enables decompression of the neural elements but not repair or regeneration of the ruptured intervertebral disc. The short-term clinical results of this intervention show that it is very effective for the resolution of sciatica. However, in the long term, recurrent symptoms may appear in the form of severe lumbar pain and sciatica.2 Late complications of disc surgery include herniated recurrence in 7% to 9% of patients and associated scarce discectomy,3 periradicular fibrosis in 6% of cases,4 segmental instability as a consequence of an average disc height loss of 25% at 2 years after surgery and associated wide discectomy, and degeneration of the intervertebral disc itself.5 Thus, 27% of patients who undergo discectomy will suffer the so-called postdiscectomy syndrome or failed back surgery syndrome, requiring a second surgery within 10 years after the first intervention.6
A possible solution to avoid postdiscectomy syndrome is to perform a lumbar fusion instrumented with pedicle screws during the surgical discectomy. However, instrumented spinal fusion has important disadvantages such as the morbidity associated with the surgical technique itself, the potential complications such as implant failure or the effect on adjacent segments, and the uncertainty of the final result. Therefore, there is a growing interest in less invasive therapeutic solutions as an alternative to lumbar fusion. Other types of implants of less local aggressiveness, such as interspinous stabilization devices (ISDs), are included in this context.
ISDs are implanted in the interspinous space through the ligament and between the 2 spinous processes. These devices could have possible “theoretical” effects, such as reducing the narrowing of the foramen, unloading the articular facets by absorbing part of the axial load that they support, and providing stability to the vertebral segment by neutralizing hypermobility generated by the removal of disc material.
Experimental and anatomical studies support the use of ISD to reduce postdiscectomy instability. Most of the biomechanical studies have been carried out in the laboratory on cadaver spine. The X-STOP implant has been studied following this experimental model by several authors,7–11 reaching the conclusion that the presence of an interspinous implant impaired the intradiscal pressure at the back of the ring and the flexo extension movement in the stabilized segment, but it did not affect the lateral inclination and vertebral rotations. A recent study, using finite element analysis and comparing these implants, agreed that the consequence of the implantation of these devices mainly produces a limitation of the lumbar flexo extension range without affecting the torsion and lateral inclination of the spine.12
Conventional radiological studies carried out after the implantation of an ISD, 2 years after the surgery, have determined that the intersegmental mobility was limited by 4° with respect to the control group.13 Crawford et al14 have determined that an ISD does not change the parameters of preoperative lumbar lordosis or segmental kyphosis in the supradjacent disc. Magnetic resonance studies carried out on patients have shown that the implantation of an X-Stop elicited an increase of the medullary canal between 18% and 22% in extension and of the foraminal canal between 25% and 37% in extension, but it did not alter the disc height, with an average recovery of only 1–1.75 mm.15
Therefore, the aim of this study was to analyze and compare in long-term (more than 8 years) clinical and functional results, complications, and reinterventions of patients who had undergone surgery for a herniated disc, with or without an ISD Device for Intervertebral Assisted Motion (DIAM) type (Medtronic) implanted during surgery.
Methods
Study Design
The present study was a retrospective, analytical-descriptive, observational, and transversal study that evaluates the postoperative results in patients who have undergone lumbar disc herniation surgery, by means of lumbar discectomy, with and without the placement of an ISD added to conventional surgery, with a minimum follow-up of 8 years.
Patients
A total of 171 patients, aged 18 to 65 years, who underwent surgery for symptomatic lumbar disc herniation between January 2008 and December 2011 were included in the study groups (95% CI with 5% margin of error). Inclusion criteria were patients with a lumbar disc herniation among L4-L5-S1 causing permanent sciatica, without improvement with medical treatment for at least 2 months, confirmed by magnetic resonance imaging and surgically submitted to a conventional discectomy, and with a minimum follow-up after surgery of 8 years.
Exclusion criteria were as follows:
Patients who suffered an objective neurological deficit during the clinical evaluation.
Patients who showed, in the imaging studies (x-ray and magnetic resonance imaging), another associated pathology such as spondylosis, canal stenosis, vertebral instability, or degenerative discopathy.
Patients who had undergone previous surgery on the lumbar spine.
Patients who required some type of psychiatric treatment or consultation during their evolution since surgery.
After excluding all patients who did not meet the inclusion criteria or who were not located or not willing to participate in the study, a total of 55 patients who underwent discectomy with placement of the interspinous implant and 59 patients who underwent lumbar discectomy exclusively were included.
Surgical Technique
The surgery was performed by the same team of orthopedic surgeons with the patient under general or spinal anesthesia depending on the preference of the attending anesthetist. Patients were placed in a genu chest position. The correct intervertebral space was located with the image intensifier. An incision was made in the midline of the lower lumbar spine of between 5 and 8 cm, and the paravertebral muscles were retracted bilaterally to the lamina. After opening the flavum ligament, partial laminectomy and discectomy of free disc fragments and nerve root decompression were performed. The wound was closed, and a suction drainage was placed.
For the placement of the ISD, the interspinous ligament was partially removed, while the supraspinatus ligament was kept in place with a minimum width of 0.5 cm. After appropriate measurement of the interspinous space without overdistraction, the DIAM implant was placed in this space, below the supraspinatus ligament, and positioned as anteriorly as possible. The implant was secured by passing the straps around the upper and lower spinous process. Patients started walking the day after surgery with a semirigid lumbar support, and they were discharged from the hospital 48 hours after surgery.
Performance Measurement
The variables analyzed in this study can be grouped into 4 sections. The first is the sociodemographic variables collected from the medical history, which included age, gender, duration of sciatica symptoms before the operation in months, location of the herniated disc, and type of surgery, with or without an associated implant. The second section included other variables also collected from the patient’s medical history, such as follow-up time in months since surgery, description of immediate surgical complications if any, and description of reintervention, if any, together with the time elapsed since the first surgery and probable cause of reintervention.
The third section included qualitative variables of a subjective nature that the patient manifested at the time of the face-to-face review, such as the consumption of analgesic medication, current work status, and degree of satisfaction with the surgery performed. The fourth section referred to the quantitative variables that aim to evaluate the final clinical result of the intervention by means of standardized questionnaires commonly used in spinal surgery. The questionnaires used were as follows: visual analog scale (VAS) to measure pain intensity and Oswestry Disability Index (ODI) to calculate the level of disability presented by the patient. The VAS was established between 0 (no pain) and 10 (very severe pain), which was determined with a millimeter rule. The ODI was established as a percentage between 0 and 100, calculated with the standardized quotient. Both questionnaires were used both in the preoperative phase (it is recorded in the medical history as it is provided to all patients before surgery) and in the current review to establish the existing differences.
Statistical Methods
The tool used for statistical analysis was the PSPP software package. The descriptive analysis was performed on the whole study sample with a 95% CI for both means and proportions, considering the existence of statistical significance when P < 0.05. The Kolmogorov-Smirnov test was used to check the normality in the quantitative variables. To analyze the statistically significant differences between the 2 study groups, the Student t test for independent samples or the Mann Whitney U test for quantitative variables was employed according to the results obtained in the normality test; χ 2 was used for the qualitative variables by study groups based on the types of surgery performed (LAM group: laminectomy/discectomy; ISD group: LAM plus implant).
A Kaplan-Meier survival curve was made with the collected data on reoperation, and the time elapsed until reoperation was performed. The log-rank test was used to evaluate the effect of the implant.
Results
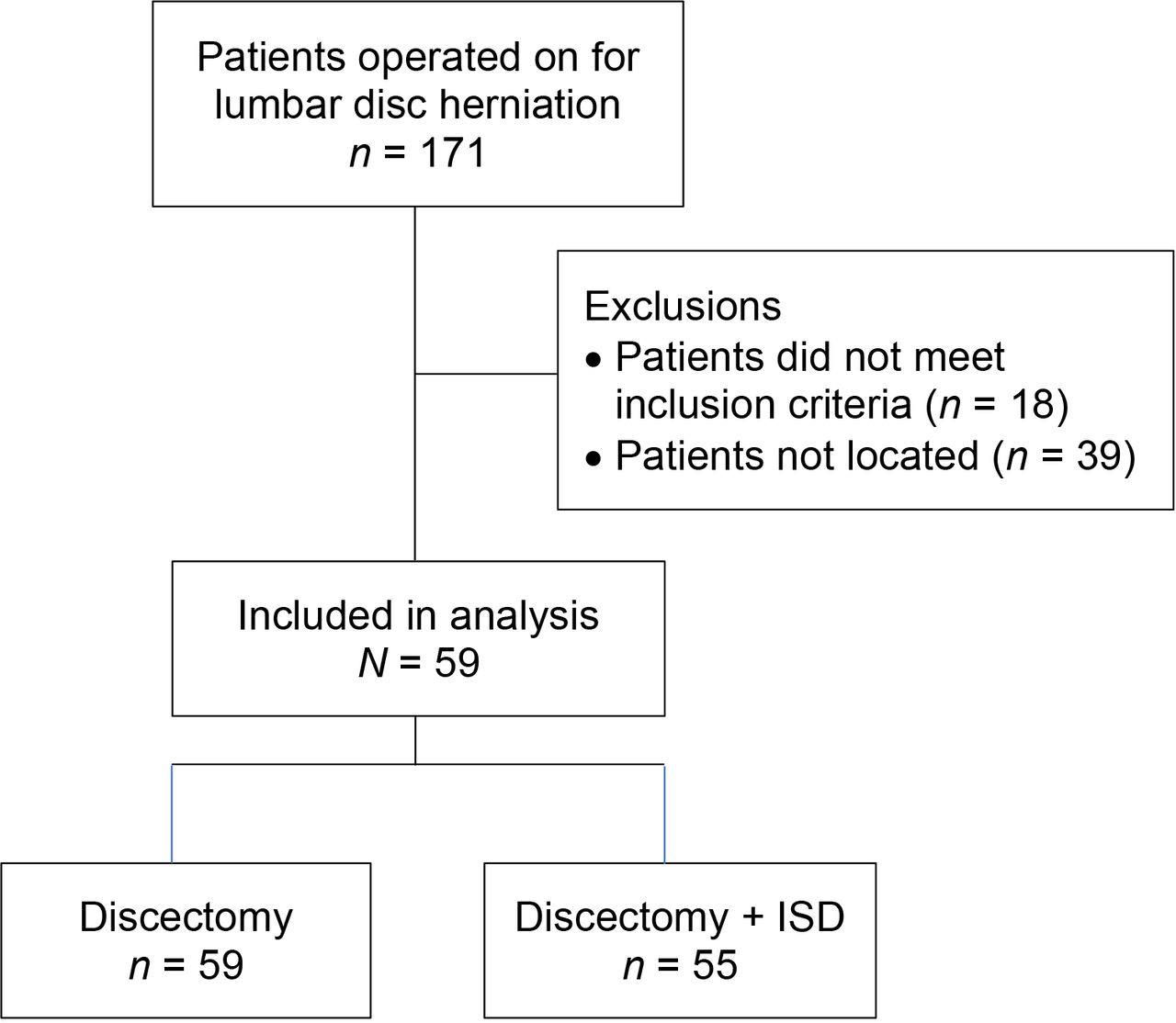
A total of 171 patients with lumbar disc herniation were operated on at the Hospital Príncipe de Asturias in Alcalá de Henares in Madrid, Spain. Our institution is a general hospital that attends to individuals living in the Eastern area of Madrid and properly represents the average patient with lumbar herniation in the community. Therefore, the bias of a highly specialized center attending particular groups of patients did not exist. A total of 57 cases were not included in the study: 18 patients were excluded because they did not meet the inclusion criteria, mainly because of the existence of some permanent neurological deficit or associated psychiatric disorder, and 39 patients were not included because it was not possible to locate them or because they refused to participate in the face-to-face survey. In this study, 18 of 39 patients not located were distributed to the discectomy group while the remaining 21 were in the DIAM group. There was no statistically significant difference in the distribution of patients to discectomy with or without device among the 114 patients included in the final study and the 39 patients not located (χ 2 test, P = 0.67572). Thus, the study was carried out on a total of 114 patients who underwent surgery. The minimum follow-up time since surgery was 8 years, excluding patients with reintervention. Follow-up ranged from 98 to 144 months, with an average follow-up of 118.8 months (Figure 1).

Flowchart of inclusion and exclusion of patients from the study. ISD, interspinous stabilization device.
The mean age of patients was 41.4 years(range, 18–62 years). Of the included patients, 63 (55.25%) were men and 51 (44.75%) were women. Disc herniation was located in L4-L5 in 53 cases (46.5%) and in L5-S1 in 61 cases (53.5%). The predominant symptom was lumbosciatica, and the duration of symptoms ranged from 2 to 24 months with a mean duration of 5.5 months (Table 1).
Sociodemographic analysis of the population studied.
The group who underwent discectomy with the addition of an interspinous stabilizing device included 55 patients (48.25%). The mean age of this group was 42.1 years, and 31 (56.1%) of the patients were men. The predominant location was in L4-L5 in 37 cases (67.3%), and the average duration of symptoms was 5 months (Table 1).
The group who underwent an isolated discectomy consisted of 59 patients (51.75%). This group was similar in terms of age and sex of the patients, with an average age of 40.7 years and a slightly higher incidence of 54% in men (32 cases) with respect to women. In this group, the predominant location was L5-S1 with 43 cases (72.9%). The average duration of symptoms before the intervention in this group was 6.1 months (Table 1).
Discectomy as a conventional technique for the treatment of lumbar disc herniation has proven to be effective and maintained over time. Mean VAS was reduced by 4.6 points (70.6%), from 7.8 before surgery to 3.1 at present. The mean ODI decreased from 50.1% before surgery to 11.3% after surgery (a diminution of 78.5%). No patient had a score higher than 20%, indicating that there was no disability among patients after discectomy. The total percentage of immediate postoperative complications was 5.25% (6 cases), and the percentage of long-term surgical reinterventions to resolve pathological findings related to a postdiscectomy syndrome was 11.4% (13 patients) (Table 2).
Result of surgery according to pain, disability, complications, and reinterventions.
The subjective results of the surgery have shown that 81.2% of the patients at the present time are not taking medication or very occasionally nonsteroidal anti-inflammatory drugs. Likewise, 75% of the patients have returned to their usual jobs or have changed their type of work, but without reducing their working hours. A total of 88 patients (78.6%) stated that they were very satisfied or satisfied with the operation, while 24 patients (21.4%) were not satisfied or clearly dissatisfied (Table 3).
Subjective results of surgery for each study group.
Comparative Result of Both Techniques
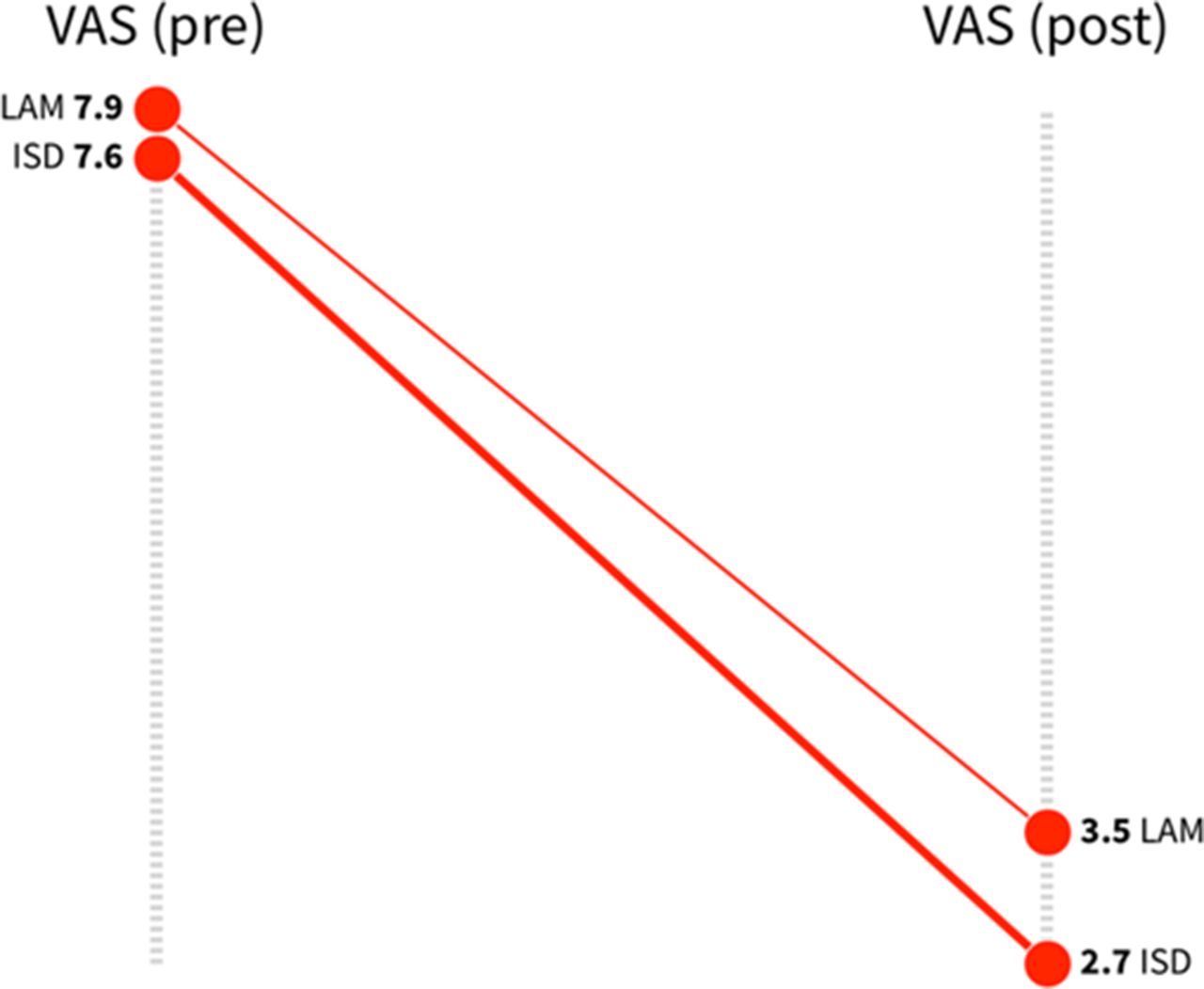
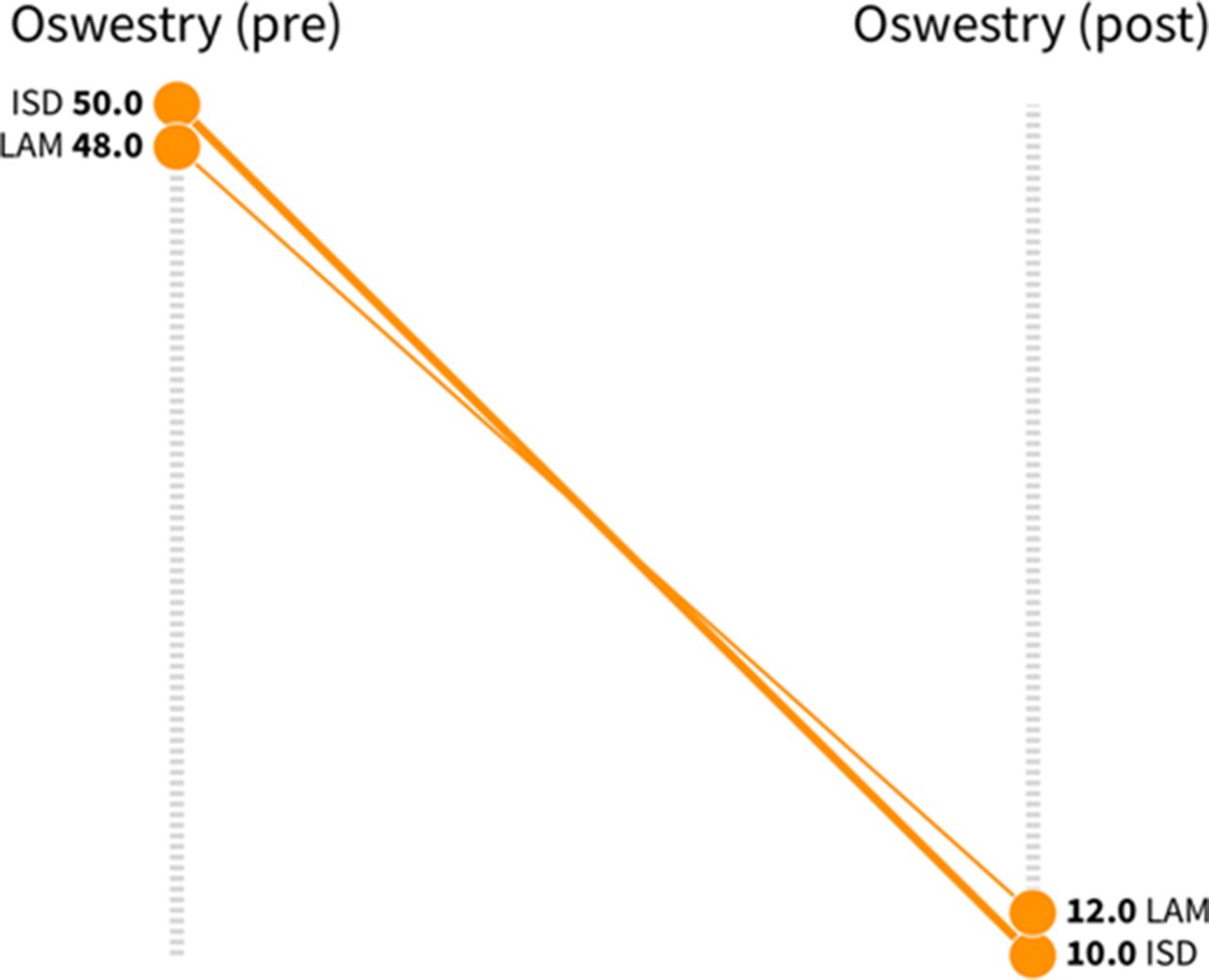
Prior to surgery, no statistically significant differences were found between ISD associated and isolated discectomy, in terms of VAS and ODI, demonstrating that both groups were uniform. The final result after surgery was slightly higher in those patients who received the interspinous implant. Postsurgical VAS in the latter group was 27 compared to 35 for isolated discectomy, and postsurgical ODI was 10% compared to 12% for patients without implants. However, these differences were not statistically significant (Table 2; Figures 2 and 3).

Preoperative and postoperative visual analog scale (VAS) with both techniques (0–10). LAM (laminectomy/discectomy); interspinous stabilization device (ISD) (LAM plus implant).
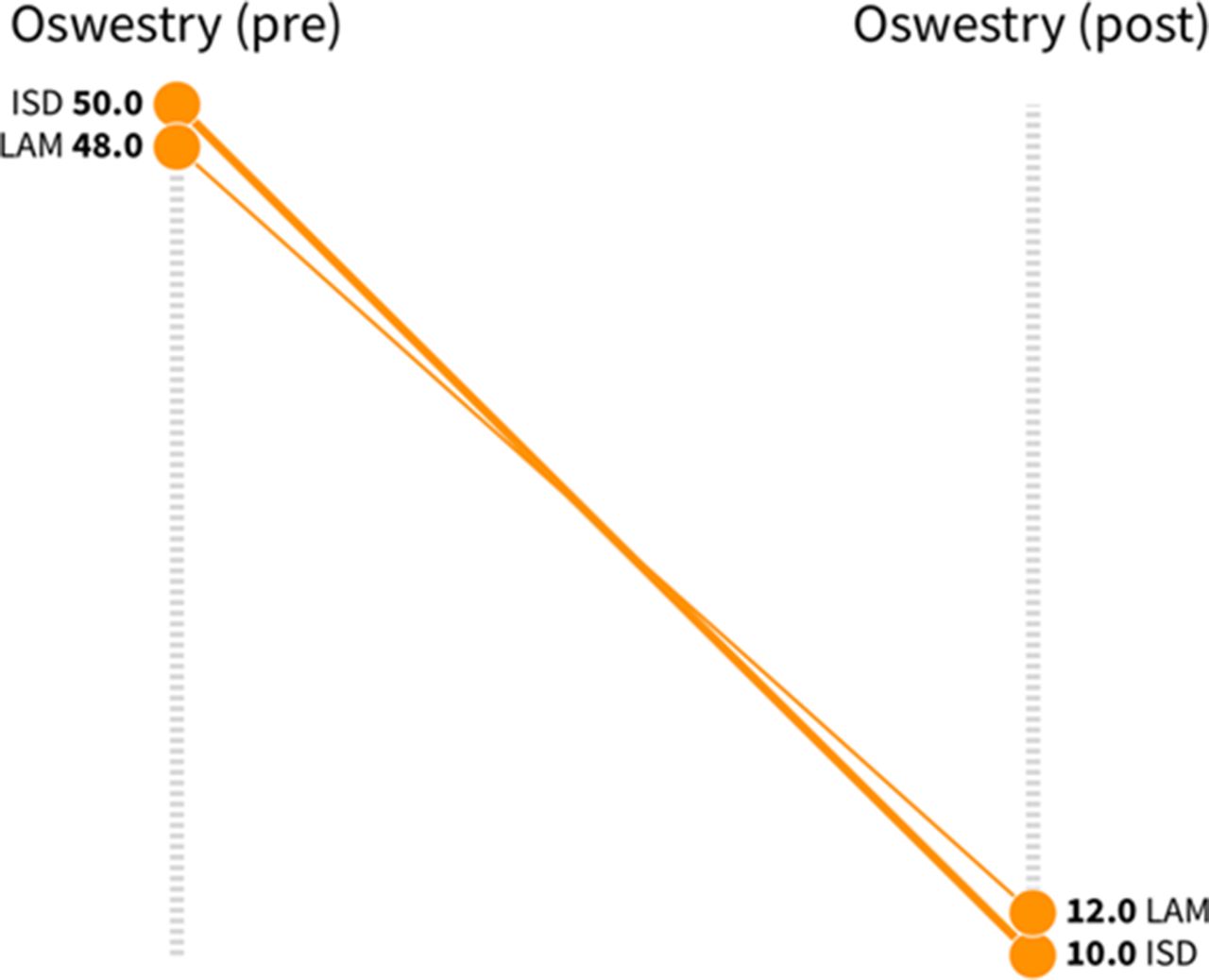
Preoperative and postoperative Oswestry Disability Index with both techniques (%). LAM, laminectomy/discectomy; ISD, interspinous stabilization device (LAM plus implant).
The percentage of immediate complications after surgery was higher in patients who underwent ISD. In this group, a total of 4 complications were found (7.3%), an opening of the dura mater, a fracture of the spinous process without consequences for the stability of the implant, and 2 superficial infections that forced surgical cleaning and early removal of the implant. However, in the isolated discectomy group there were only 2 complications (3.4%). These were 2 openings in the dura mater, which were repaired during the surgical act without any future repercussions for the patient. The difference between the 2 groups did not prove to be statistically significant (Table 2).
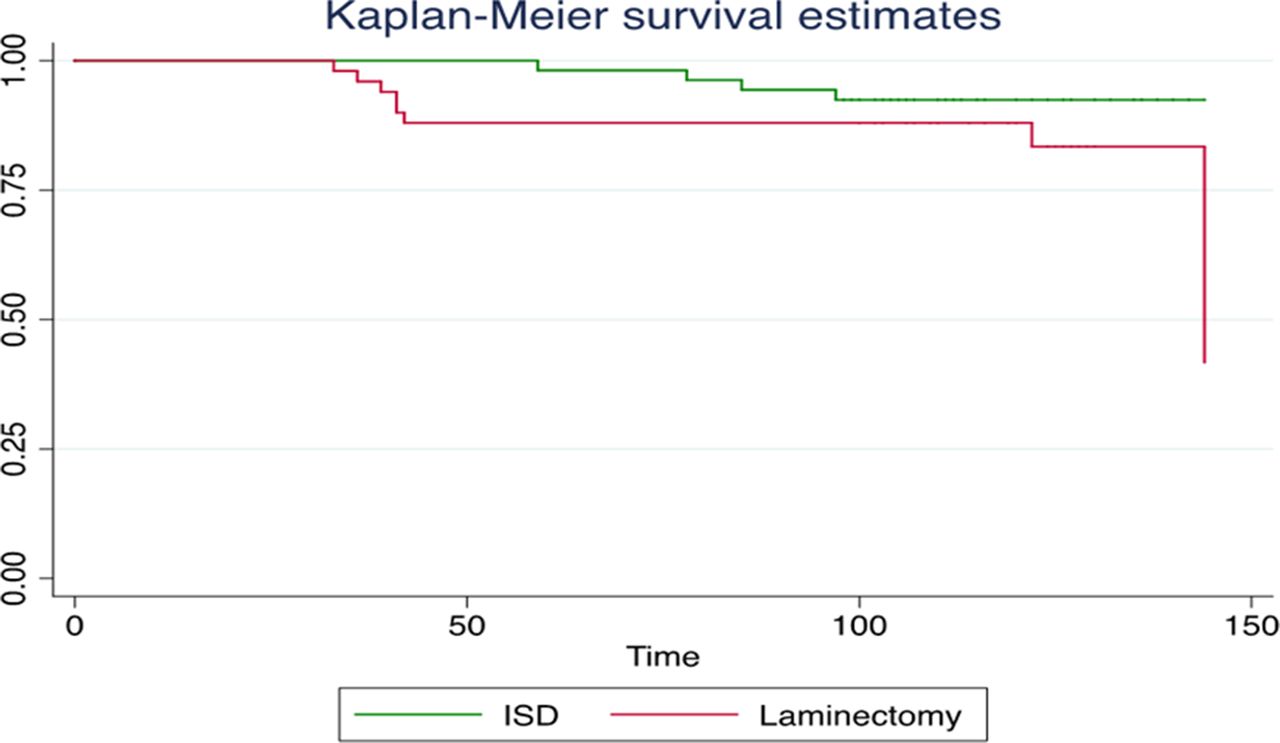
An inverse relationship has been observed in the section on long-term reinterventions after surgery. Thus, 4 patients (7.27%) were reintervened in the group with ISD as a result of degenerative disc disease. All of them underwent an instrumented lumbar arthrodesis. The average time between both surgeries was 81.5 months. However, in the isolated discectomy group, the number of reinterventions during the follow-up time was 9 cases (15.25%). The 9 reinterventions were for degenerative discopathy in 5 cases, periradicular fibrosis in 2, and for recurrence of disc herniation in the other 2. The reinterventions consisted of instrumented lumbar arthrodesis in 7 patients and new discectomy in 2 cases (Table 2). The average time from the first surgery to the second reintervention was 41 months, a difference not statistically significant, but with an estimated slightly higher time to reoperation in patients with implants according to the Kaplan-Meier curve (Figure 4), although with a log-rank analysis P = 0.13.

Kaplan-Meier survival estimates. ISD, interspinous stabilization device.
The subjective results of both groups also showed a slight benefit in patients with ISD (Table 3). Two patients were excluded in this analysis because the questionnaire was not properly filled out. In the group with ISD, 85% of patients did not take medication or did so occasionally, compared to 78% with isolated discectomy. Return to work did not occur in 11 cases of discectomy with ISD (20.75%), while this took place in 17 cases (28.8%) in the isolated discectomy group. Finally, the percentage of patients who were very satisfied or satisfied with a discectomy plus ISD was 81.1% compared to 76.3% of patients with isolated discectomy. The differences were not statistically significant (Table 3).
Discussion
Disc herniation surgery by means of conventional discectomy was a reliable and reproducible technique with results that are maintained over time. The review of 114 cases of disc herniation with a minimum follow-up after surgery of 8 years shows a clear improvement in VAS and ODI and how this improvement is maintained over time. VAS has been reduced by 46 points, which is equivalent to a difference between current preoperative and postoperative VAS of 70.6%. Similarly, ODI has been reduced by almost 32 points, which is an improvement of 63.5% compared to the situation before the intervention.
However, no statistically significant differences could be demonstrated when an ISD was added to conventional surgery. The 2 groups of patients with symptomatic disc herniation were uniform in terms of age, gender, and duration of symptoms before the intervention. However, the results are slightly better in the implant group in terms of ODI because the presurgical and postsurgical difference resulted in an average reduction of 38 points (79%) compared to 34 points (77%) in conventional surgery. Other data from the study also show that the implant group had improved VAS by 73% compared to 66% for conventional discectomy. Likewise, this group needed a lower consumption of analgesics compared to patients without implants, a higher return to normal work and level of satisfaction with the surgery, although there were few differences between them.
Most of the randomized studies analyzed short-term clinical outcomes and focused on patients with a basic pathology of lumbar canal stenosis. Some of these studies have compared the conventional decompressive surgery of laminectomy vs the implantation of the ISD “in situ” without associated neurosurgical decompressive gesture. The results of those studies, however, did not show statistically significant differences between both groups, though a high number of reinterventions (25% of the cases) were noted in the group with implant.16,17 Other works,18,19 on the contrary, have analyzed the behavior of ISD, not as an isolated technique capable of solving the pathology by itself, but as a coadjuvant technique associated to a decompressive surgery. The result of comparing both groups, with and without implant, shows the absence of statistically significant differences, but a better clinical-functional behavior at the end of the follow-up in cases with implant.
Clinical studies involving ISD focused exclusively on disc pathology are scarce. Two comparative analyses in patients with disc herniation in which a Wallis was added with follow-up between 3 and 4 years should be highlighted.20,21 These studies coincide in their conclusions, finding no statistically significant differences in the final result between the 2 groups. In degenerative discopathy as a pathological entity, Buric et al22 implanted a DIAM in a total of 52 patients, reporting improvement in VAS in 67% and in functionality in 79% after a 4-year follow-up. Other authors23 have also been able to verify absence of symptoms in 91% of cases with moderate lumbar degenerative discopathy 3 years after surgery when a DIAM was implanted. These data, which can be superimposed on those obtained in this study, may indicate a certain “protective” effect of this type of device. The distraction of the interspinous space may reposition the facet joints eliminating possible sources of postsurgical lumbar pain.
The total complications attributable to the surgical act of discectomy itself correspond to 2 cases of durotomy, which would indicate an incidence of 3%. These data are considered similar to the incidence reported in the medical literature of dural injury during discectomy, around 3%.24 The rate of complications in the ISD group, including the case of durotomy, stood at 7%. The complications were 2 cases of surgical wound infection that were treated with debridement, cleaning, and early implant removal, and another one of spinous process fracture during implant insertion that did not affect implant stability. The data on immediate postoperative complications contrast sharply with some published works. Barbagallo et al,25 out of a total of 69 patients, found an 10% incidence of complications with X-Stop. The overall incidence of immediate postoperative complications with the use of an ISD has been estimated at around 4%.26 The complications described were similar to those of the study: fracture of the spinous process, implant migration, and surgical wound infection. It seems that these types of complications are mild and bearable as long as the implant is considered to be beneficial.
In the chapter on reinterventions, the overall incidence of our study, after an average follow-up of 9 years, was 11%. This incidence is in line with that published in the medical literature, with an incidence of reinterventions of 11% to 15% between 8 and 10 years after surgery.26–28 The most important causes of reintervention were degenerative disc disease of the operated disc, periradicular fibrosis, and recurrence of disc herniation. However, separate analysis between the 2 groups shows a notable, although not statistically significant difference, with the rate of reinterventions in the isolated discectomy group being 15% compared to 7% of cases with ISD. Furthermore, the average time for reoperation in patients with discectomy was 41 months, while in the group with ISD was 81.5 months. A possible explanation for this difference is the effect of the implant on the abnormal mobility of the vertebral segment after a wide discectomy. Stabilization of the posterior intervertebral space tightens the fibrous ring of the intervertebral disc and the posterior common spinal ligament which can improve the ability to withstand loads. Also, this type of implant may be able to neutralize some of the abnormal movement of the vertebral segment after discectomy, enough to reduce the formation of periradicular fibrosis.
Survival studies estimate the rate of reinterventions with ISD for disc pathology in implants such as the DIAM or the Wallis in 8% and 10% of cases, respectively, with follow-ups between 4 and 5 years.29,30 These data are similar to this study, with a percentage of reinterventions of 7% in the group with ISD but with a greater follow-up in the time of 9 years. Also, several meta-analyses refer to ISDs in lumbar pathology.31–34 All of them focus on lumbar canal stenosis, but their observations can be extrapolated to disc pathology. There is some agreement in their conclusions that ISD slightly improves clinical and functional outcomes in the medium term with respect to laminectomy, low rate of complications of ISD, but high incidence of reoperations when used in isolation. However, no differences are observed in the percentage of reoperations when the ISD is associated with decompression at around 8%.
Nevertheless, all these studies mention 3 important aspects of the ISD technique that can have evident repercussions when it is also used in disc pathology. A possible disadvantage of this type of implant would be the possibility of increasing kyphosis by distracting the posterior part of the vertebral segment and which could lead to an alteration in the sagittal balance, which is harmful to the patient in the long term. However, radiographic studies14,35 have not found significant differences in the sagittal balance in patients with an ISD. Another aspect that stands out is the simplicity of the technique of implantation of the ISD with no blood loss, minimal damage to anatomical structures during placement, and a short surgical time consumed. Furthermore, if necessary, the extraction of the implant and the conversion into fusion are simple, with minimum soft tissue damage and low surgical risk. All these aspects are considered to be advantages of ISD.
On the contrary, some authors have questioned the cost-utility ratio of ISD in the long term due to the demonstrated high rate of reinterventions.26 Therefore, future studies assessing the cost-effectiveness of implants are essential. In the meantime, and accepting a possible protective effect of ISD, our recommendation is their implantation after an adequate selection of patients. We think that their main indication would be in those cases that, in addition to disc herniation, already show an incipient established disc degeneration. Also, in cases of herniation with significant loss of disc material (extruded and migrated herniations) in order to limit early disc degeneration.
Limitations
The study has certain limitations such as the restricted number of patients which could condition a different clinical and functional impact in the long term. It is also necessary to consider the significant number of patients lost in this study, mainly attributable to the time elapsed since the surgery. Although all patients were operated on by 2 surgeons of the same team, the performance of different additional surgical gestures such as extended laminectomy or additional foraminotomy could equally influence the final clinical outcome of the patients, making it different. Furthermore, the size of the hernia or its morphology, which could condition a future disc degeneration, was not considered.
To avoid selection bias that could influence the final result, all patients presenting some type of objective neurological deficit at the time of surgery were eliminated, as well as those showing some associated degenerative lumbar pathology. In addition, a quality-of-life index was not evaluated, so the influence of associated psychosocial factors that could affect the final clinical outcome of the study cannot be ruled out.
Conclusions
Conventional lumbar discectomy has proven to be a safe and reproducible technique for the treatment of symptomatic lumbar disc herniation with adequate results maintained over time. The additional surgical gesture of adding an ISD to conventional discectomy has improved overall long-term clinical-functional outcomes, but not in a statistically significant way.
The rate of postsurgical complications was small with both techniques and without repercussions on the final results. Most of the reinterventions are secondary to the degenerative changes that appeared in the vertebral disc over time. Patients without implants had a higher rate of reinterventions and a shorter time until the second intervention. This may indicate a certain stabilizing effect of the ISD on the vertebral segment that prevents its hypermobility in the long term. Further studies, mainly cost-benefit analyses, are needed to support the use of ISD as a gesture to help traditional decompression surgery in patients with a lumbar disc herniation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was reported to the Ethics Committee for research work at the Hospital Universitario Príncipe de Asturias (CEIM) and was approved. All patients were given informed consent. As personal data was collected, a pseudonymization of the data was carried out, assigning a case code to each patient to perform the statistical analysis of the study.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.