


Abstract
Background Castellvi type III and IV lumbosacral transitional vertebrae (LSTVs) are fused to the sacrum. In these cases, the pelvic incidence (PI) and pelvic tilt (PT) may vary according to the selected “S1.” This study aimed to determine the optimum vertebral level of these LSTVs when measuring PI and PT.
Methods PI and PT were measured twice in 56 patients with type III and IV LSTVs with a balanced spine, with LSTV considered as the lowest lumbar vertebra (LLV) or S1. PI and PT measured with LSTV as LLV were denoted as LLV_PI and LLV_PT, and those measured as S1 were denoted as S_PI and S_PT. Reference ranges (mean −2 SD to +2 SD) of PI and PT were derived from 183 non-LSTV patients with a balanced spine as 35.5° to 68.8° (PI) and 2.5° to 29.6° (PT). If S_PI, S_PT, or both were below the reference range, the LSTV was interpreted as LLV. If LLV_PI, LLV_PT, or both were above the reference range, it was interpreted as S1. If all parameters were within the respective reference range, it was interpreted as an intermediate type.
Results The optimum vertebral level of LSTV was S1 (n = 29, 51.8%), most frequently due to high LLV_PT (35.4°±4.7), followed by LLV (n = 14, 25%) due to low S_PI (31.5°±5.2) and intermediate type (n = 13, 23.2%).
Conclusions If PI is too small or PT is too large to represent the actual sagittal alignment in patients with Castellvi type III and IV LSTVs, the selected S1 should be reconsidered.
Clinical Relevance PI and PT measurements can be used to determine whether the optimum vertebral level of Castellvi type III and IV LSTV should be considered LLV or S1.
Level of Evidence 3.
- adult spinal deformity
- Castellvi
- lumbar degenerative disease
- lumbosacral transitional vertebra
- spinopelvic parameters
- thoracolumbar transitional vertebra
Introduction
Spinopelvic parameters such as pelvic incidence (PI), pelvic tilt (PT), and lumbar lordosis (LL) are essential parameters when planning corrective spinal surgery for adult spinal deformity, including spinal degenerative disease. Schwab et al1 considered PI-LL ≤10 and PT <22 as ideal based on the health-related quality of life scores in patients with adult spinal deformity, and several authors2–4 created a formula to calculate the ideal LL angle based on the PI value using healthy volunteer data. However, care should be taken when applying the PI measured in patients with a lumbosacral transitional vertebra (LSTV) to those formulas. According to Khalsa et al, the interobserver reliability of the PI measurement in patients with LSTV was poor because of differences in the choice of S1.5
LSTV is a type of congenital spinal anomaly, classified by Castellvi et al, as types I to IV (Figure 1).6 Type I and II LSTVs are most likely to be recognized as the lowest lumbar vertebrae (LLVs); however, type III and IV LSTVs, in which the LSTVs and the sacrum are partially or fully fused, may be interpreted as either LLV or S1. In addition, LSTV frequently coexists with a thoracolumbar transitional vertebra and is often associated with variation in the number of vertebrae.7–10 Therefore, clinicians need to carefully consider whether the measured PI, PT, and calculated target LL are clinically applicable, especially in patients with type III and IV LSTVs.

Schematic diagrams of the Castellvi classification of LSTVs. Type I, including unilateral or bilateral dysplastic transverse process(es) >19 mm, was excluded because it is difficult to distinguish it from a non-LSTV. Normally, there are 4 sacral foramina bilaterally. Still, in types III and IV, the transverse process(es) of the lowest lumbar vertebra and the sacrum are fused, giving the appearance of 5 sacral foramina. LSTV, lumbosacral transitional vertebra.
In the preliminary study, non-LSTV patients with a balanced spine were selected, and the reference ranges of PI and PT were calculated. Then, in patients with type III and IV LSTVs, PI and PT were measured twice, first with LSTV as LLV and then as S1. Based on the reference ranges of PI and PT calculated in the preliminary study, we investigated under what conditions it would be appropriate to consider LSTV as LLV or S1 on a case-by-case basis.
Methods
This cross-sectional observational study was conducted in accordance with the ethical principles specified in the 1964 Declaration of Helsinki and its later amendments, and ethical approval from the Institutional Review Board of Yokohama Minami Kyosai Hospital was obtained for this study (approval number: 2-19-11-6). Regarding the acquisition of patients’ informed consent for study participation, this observational study only used clinical information; however, we explained in advance to each patient that these data might be used for research and disclosed the outline of our research content on the home page of our hospital’s website, providing the participants with an opt-out option.
This study included patients with lumbar degenerative disease who underwent lumbar fusion between July 2014 and September 2020 at our institution’s spine center. All patients underwent whole-spine radiography, computed tomography (CT), and magnetic resonance imaging preoperatively. Medical records of 902 consecutive eligible patients were retrospectively reviewed, and imaging data of these patients were examined for Castellvi type III and IV LSTVs. These LSTVs were accurately identified using 3-dimensional CT images according to Tatara’s method.10 This method focused on the position of the promontory on the arcuate line of the ilium on 3-dimensional CT images and identified LSTV as LLV after confirming that they were positioned above the arcuate line. Sagittal imbalance was set as an exclusion criterion because it made the interpretation of spinopelvic parameters difficult.
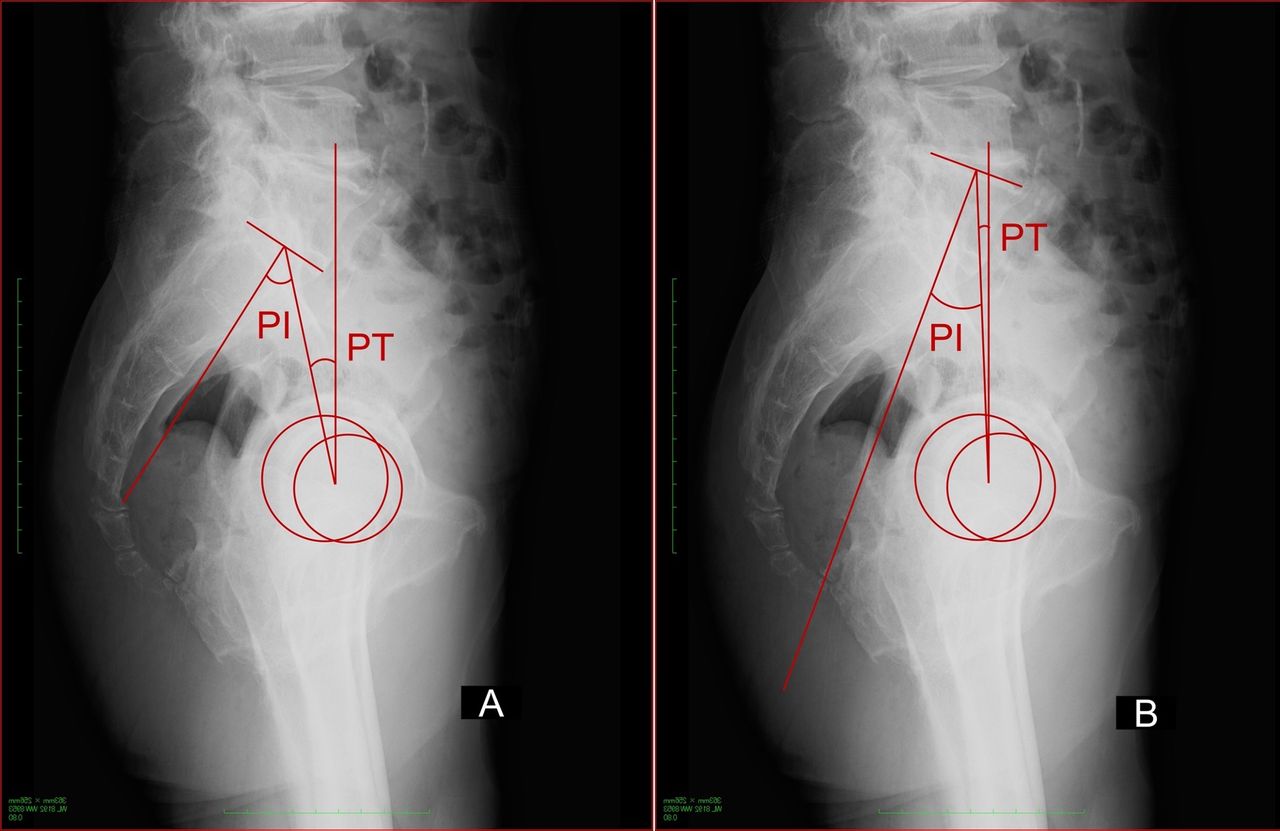
In patients with type III and IV LSTVs, PI and PT were measured twice using preoperative radiographs, with LSTV interpreted as LLV or S1 each time. When PI and PT were measured with LSTV as LLV, they were denoted as LLV_PI and LLV_PT, respectively. Conversely, when PI and PT were measured with LSTV as S1, they were denoted as S_PI and S_PT, respectively. Normally, LLV_PI and LLV_PT are larger than S_PI and S_PT, respectively (Figure 2). These parameters were measured by digital analysis using Ortho Planner Pro version 3.7.3 (TOYO, Tokyo, Japan). Descriptive statistics were expressed as mean and SD. All statistical analyses were performed using IBM SPSS Statistics for Windows version 24 (IBM Corp, Armonk, NY, USA).

Both x-rays (A and B) show the same Castellvi type IIIb case. PI and PT are measured in 2 ways, considering lumbosacral transitional vertebra as the lowest lumbar vertebra (A) or S1 (B).PI, pelvic incidence; PT, pelvic tilt.
Reference Ranges of PI and PT
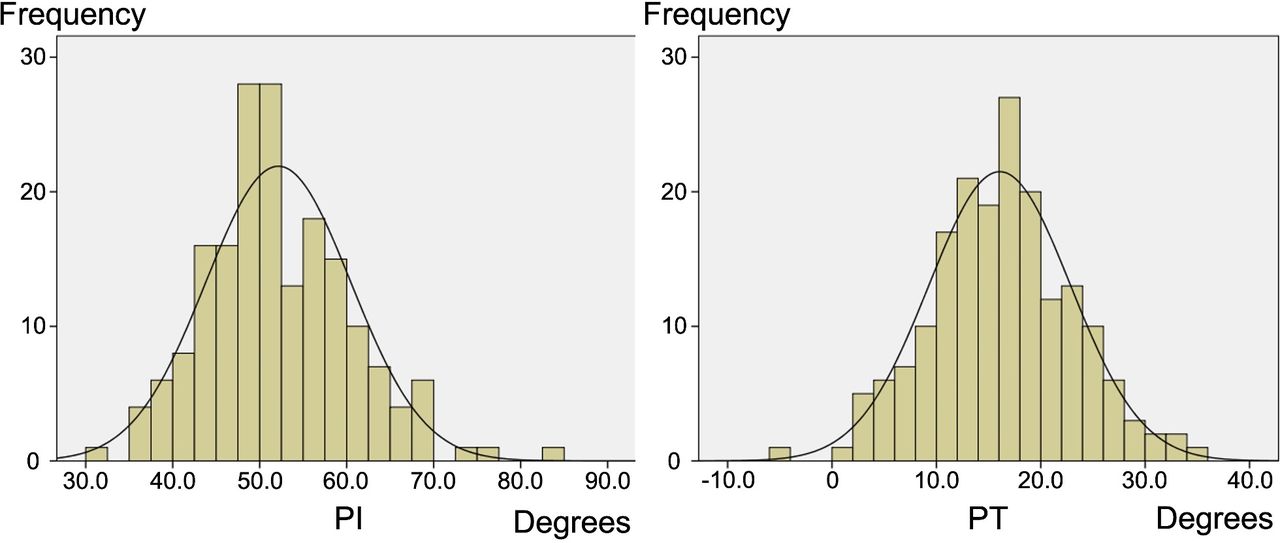
Of the 902 patients reviewed, 183 non-LSTV patients (mean age, 66.2 ± 12.1 years; woman:man ratio, 93:90) with normal sagittal alignment and coronal balance were selected, and the reference ranges of PI and PT (mean ± 2 SD) were determined using preoperative radiographs. The mean PI was 52.14° (SD 8.33), and its reference range (mean −2 SD to mean +2 SD) was 35.5° to 68.8°. The mean PT was 16.06° (SD 6.79), and its reference range (mean −2 SD to mean +2 SD) was 2.5° to 29.6° (Figure 3).
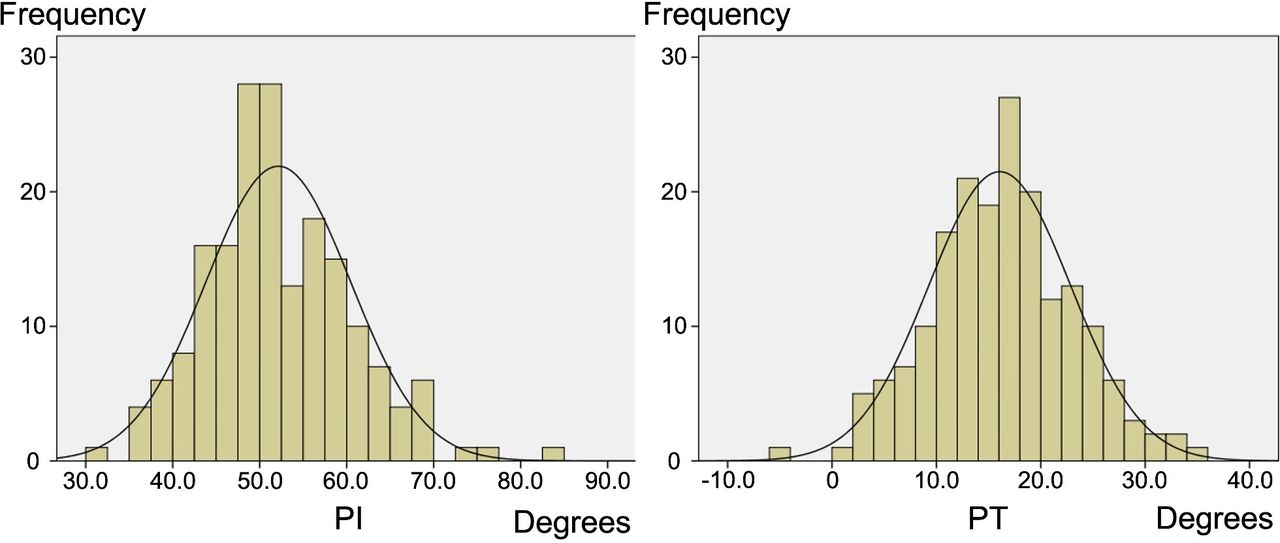
Histograms and normal distribution curves of PI and PT in patients with normal sagittal alignment and coronal balance, excluding patients with lumbosacral transitional vertebra. PI, pelvic incidence; PT, pelvic tilt.
Determining the Optimum Vertebral Level of LSTV
If either S_PI, S_PT, or both were below each reference range, the LSTV was interpreted as LLV. If either LLV_PI, LLV_PT, or both exceeded each reference range, the LSTV was interpreted as S1. If S_PI, S_PT, LLV_PI, and LLV_PT were all within each reference range, the LSTV was determined to be an intermediate type between LLV and S1.
Results
Fifty-six patients with Castellvi type IIIa, IIIb, or IV LSTV were eligible for this study. Their mean age was 70.1 (SD 12.2) years, with Castellvi type IIIb LSTV being the most frequent (n = 44, 78.6%). Table 1 shows the frequency distribution summarizing the optimum vertebral level of LSTV by LSTV type based on the reference ranges of PI and PT. The most frequent vertebral level of LSTV was S1 (n = 29, 51.8%), followed by LLV (n = 14, 25.0%) and intermediate type (n = 13, 23.2%).
Optimum vertebral level of LSTV by LSTV type based on the reference ranges of pelvic incidence and pelvic tilt.
Table 2 shows the results of PI and PT measured in 2 ways, with LSTV as LLV or S1. When the LSTV was LLV, S_PI was below the reference range, whereas LLV_PI and LLV_PT were within each reference range. Conversely, when the LSTV was S1, LLV_PT was above the reference range, whereas S_PI and S_PT were within each reference range. For patients with intermediate-type LSTV, other sagittal parameters such as LL, thoracic kyphosis, and C7 plumb line could have helped make a final decision, but such parameters were not pursued further in this study.
Measurement of PI and PT with LSTV as LLV or S1.
We give examples of 3 cases in which the vertebral level of LSTV was determined based on the reference ranges of PI and PT:
LSTV as LLV
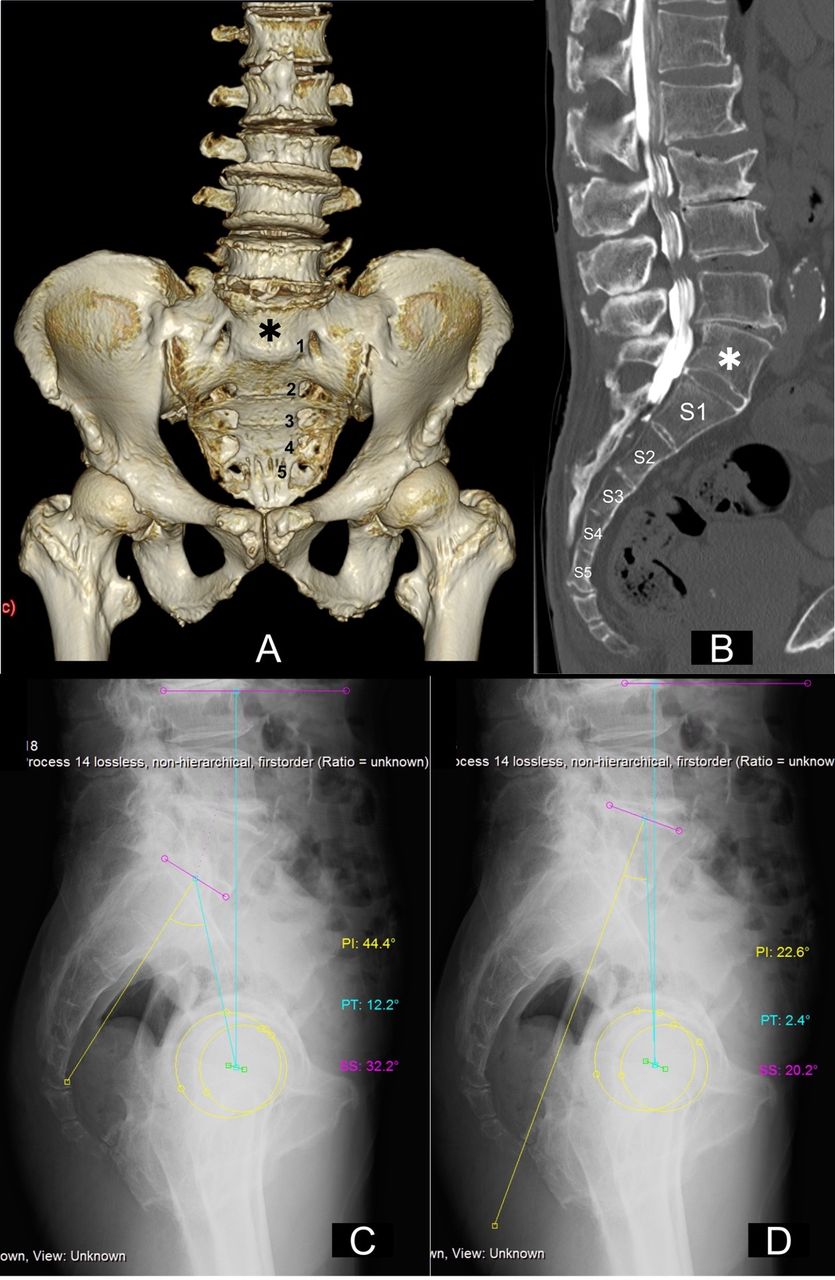
Figure 4 demonstrates a case where it is more appropriate to consider LSTV as LLV. PI (22.6°) and PT (2.4°) in Figure 4d are smaller than each reference range, whereas PI (44.4°) and PT (12.2°) in Figure 4c are within each reference range.
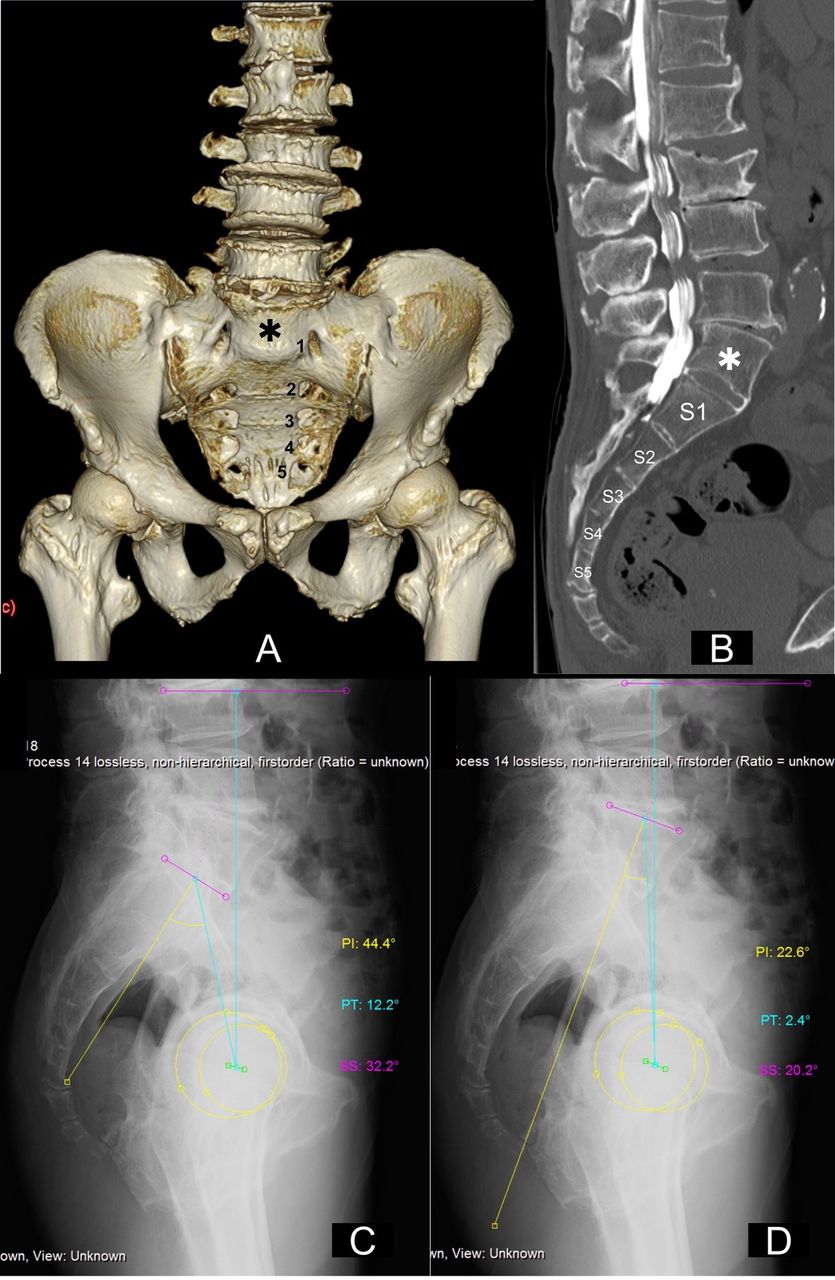
A 75-year-old man with Castellvi type IIIb. The asterisks in images A (a 3-dimensional CT image) and B (a sagittal reconstruction image of CT myelography) represent LSTV. PI and PT are measured with LSTV as the lowest lumbar vertebra (C) or S1 (D). CT, computed tomography; LSTV, lumbosacral transitional vertebra; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope.
LSTV as S1
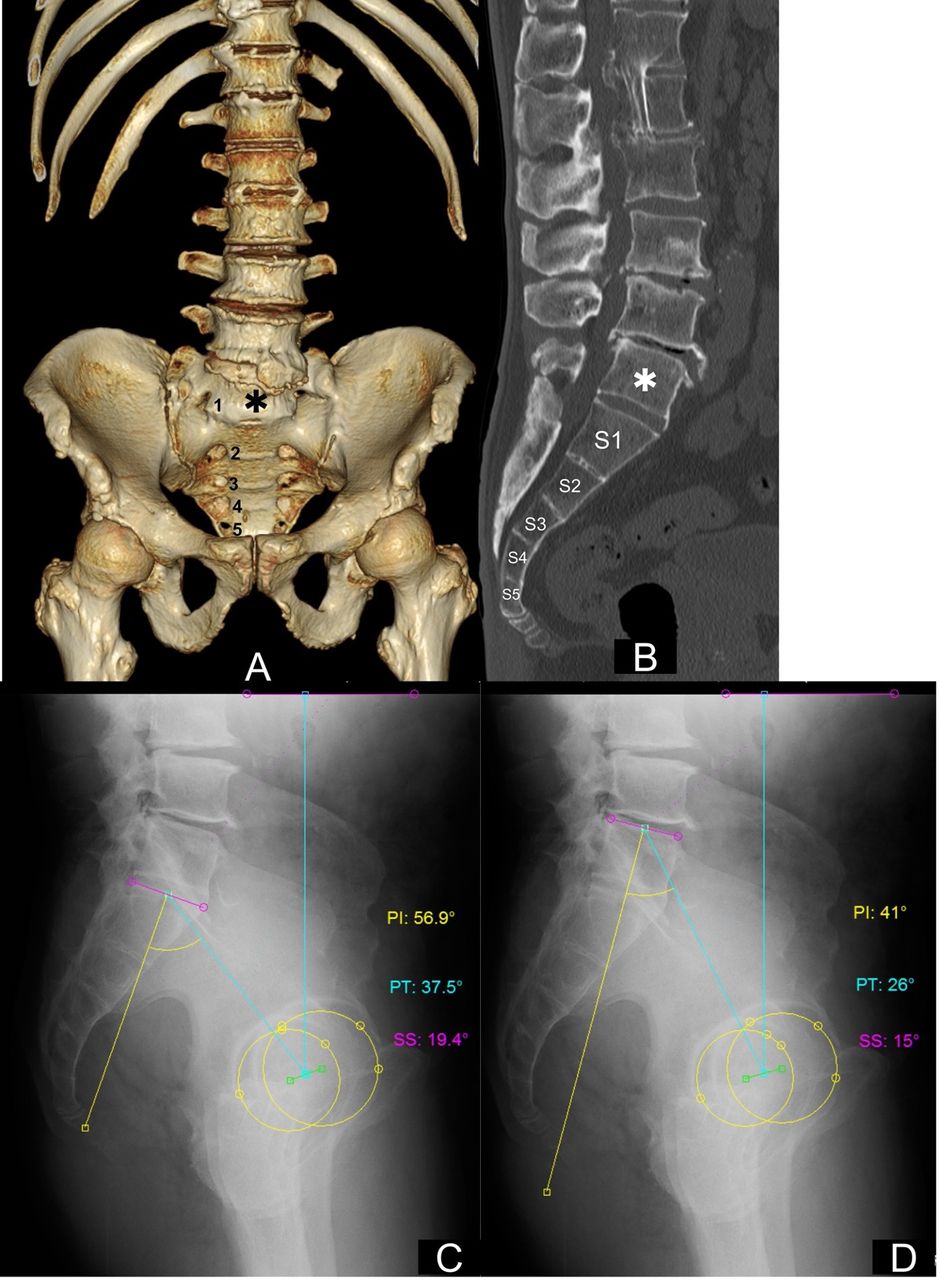
Figure 5 illustrates a case where it is more appropriate to consider LSTV as S1. PI (56.9°) in Figure 5c is within the reference range, but PT (37.5°) in Figure 5c is larger than the reference range. PI (41°) and PT (26°) in Figure 5d are within the reference range.
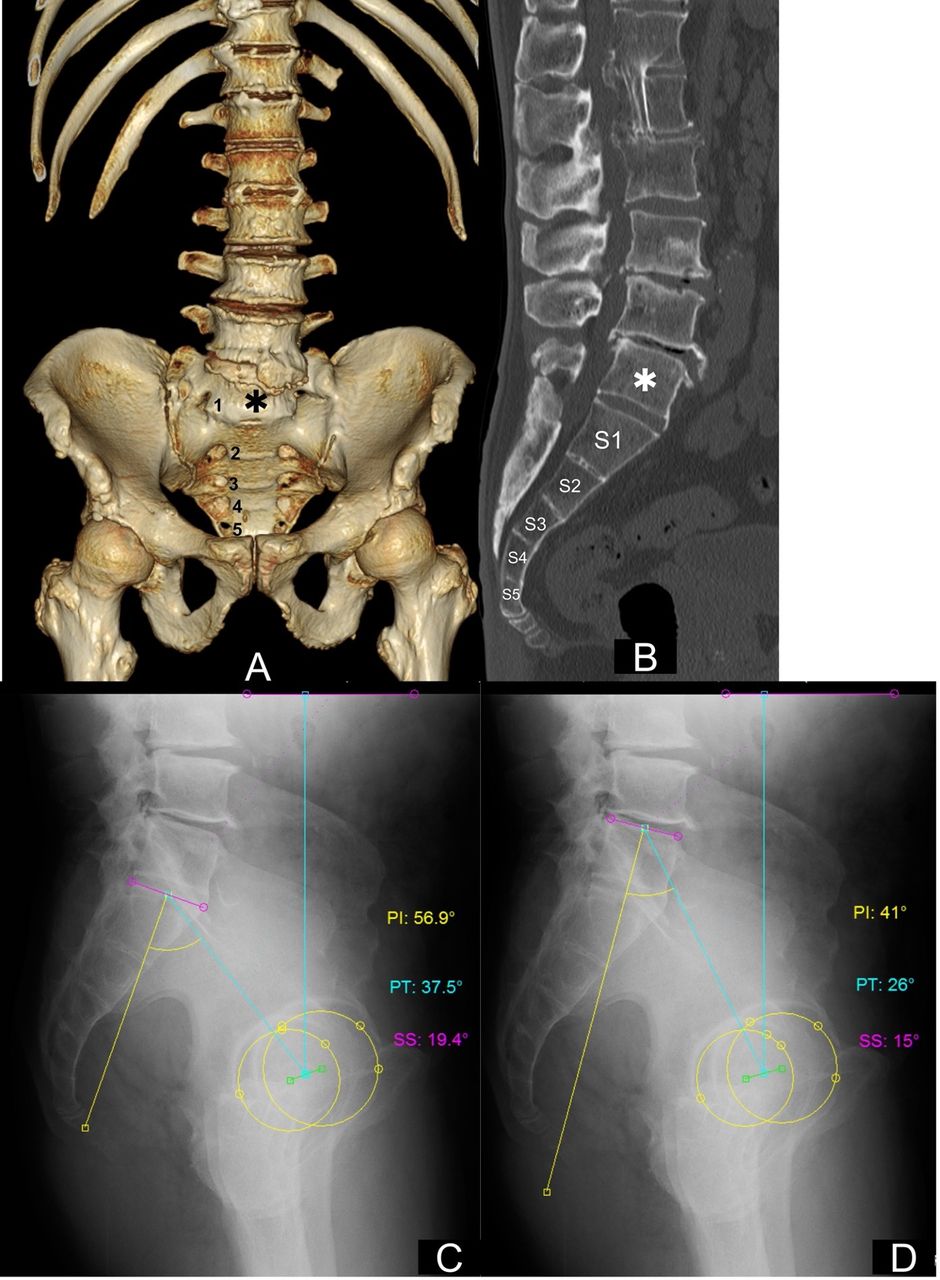
A 60-year-old man with Castellvi type IIIb. The asterisks in images A (a 3-dimensional CT image) and B (a sagittal reconstruction image of CT) represent LSTV. PI and PT are measured with LSTV as the lowest lumbar vertebra (C) or S1 (D). CT, computed tomography; LSTV, lumbosacral transitional vertebra; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope.
LSTV as Intermediate Type
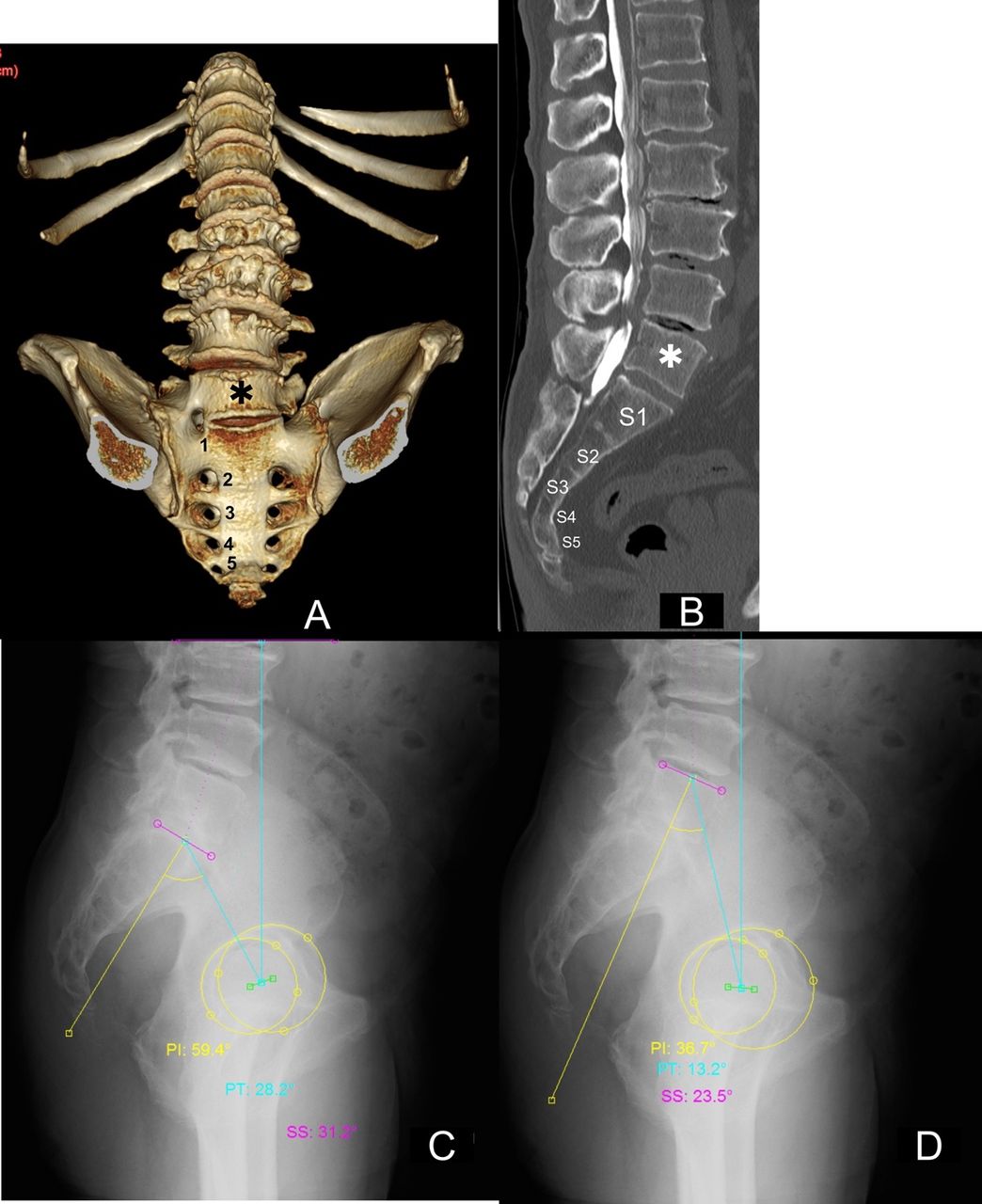
Figure 6 represents a case in which the vertebral level of LSTV was an intermediate type between LLV and S1. PI and PT in Figure 6c (59.4° and 28.2°) and Figure 6d (36.7° and 13.2°) are within the reference ranges.

A 72-year-old man with Castellvi type IIIa. The asterisks in images A (a 3-dimensional CT image) and B (a sagittal reconstruction image of CT myelography) represent LSTV. PI and PT are measured with LSTV as the lowest lumbar vertebra (C) or S1 (D). CT, computed tomography; LSTV, lumbosacral transitional vertebra; PI, pelvic incidence; PT, pelvic tilt; SS. sacral slope.
Discussion
There is a movable intervertebral disc between the LSTV and sacrum in Castellvi types I and II, but the LSTV and sacrum in Castellvi types III and IV are fused, which may explain why clinicians have different recognition sites of the S1 endplate. In this study, PI and PT were measured twice in patients with type III and IV LSTVs when LSTV was considered as LLV or S1. Based on the results, the optimal vertebral level of LSTV was determined for each case. In summary, type III and IV LSTVs were classified into 3 types: in cases where it was more appropriate to consider LSTV as LLV, S_PI was below the reference range. Conversely, in cases where it was more appropriate to consider LSTV as S1, LLV_PT was above the reference range. When S_PI, S_PT, LLV_PI, and LLV_PT were all within each reference range, LSTV was arbitrarily considered intermediate between LLV and S1.
Since LSTVs have both LLV and S1 elements, it is not surprising that some LSTVs have a strong LLV component, some have a strong S1 component, and some are in between. In this study, type III and IV LSTVs were divided into 3 types based on the PI and PT measurements, which represent the characteristics of the LSTV. Therefore, depending on the selected S1, the measured values of PI and PT may be outliers from either or both reference ranges, and it may be necessary to reconsider the selected S1 and choose one that is more compatible with other sagittal parameters. Price et al showed the PI and PT measurements of 11 LSTV patients but did not provide details of the Castellvi classification.11 In type II LSTV, there is a movable disc between the LSTV and sacrum; thus, we have no choice but to accept the PI and PT measurements as they are, whereas the condition is different for type III and IV LSTVs. Tables 1 and 2 clearly show the problem by measuring the PI and PT in 2 ways. In cases where it is more appropriate to consider LSTV as LLV, S_PI will be below the reference range. This means that the target LL is likely to be underestimated if S_PI is adopted. Conversely, in cases where it is more appropriate to consider LSTV as S1, LLV_PT will exceed the reference range, and LLV_PI will also become larger. When PI and PT are large, surgeons generally believe that the target LL is also large. Therefore, surgeons need to be cautious, especially when planning corrective spinal surgery for patients with LSTV. Notably, the case report by Crawford et al was probably a type III or higher LSTV case.12 They noted that considering LSTV as LLV made PI as well as the target LL larger, and that by treating LSTV as S1, PI and the target LL could be reduced and excellent postoperative sagittal alignment could be achieved.
The ranges of PI and PT values using healthy volunteers were reported by several authors and ranged from 26.9° to 85.0° for PI and −6.4° to 36.2° for PT.2,4,11,13,14 The mean age of volunteers surveyed in these studies ranged from the 20s to 40s, excluding the study by Yamato et al with a mean age of 64 years.4 These studies were unclear regarding whether they included patients with LSTV, and even if they excluded them, details regarding the Castellvi classification were not available. Although our participants were patients scheduled for surgery with a mean age of 66 years, their PI and PT values (mean ± 2 SD) ranged from 35.5° to 68.8° and 2.5° to 29.6°, respectively, which were comparable with those in previous studies.2,4,11,13,14 Furthermore, these data were found to approximate a normal distribution curve from the histograms in Figure 3. To increase the accuracy of our data, patients with LSTV were rigorously identified with 3-dimensional CT images using Tatara’s method and excluded.
This study has some limitations that need to be acknowledged. First, it excluded patients with sagittal imbalance; therefore, caution should be exercised in patients with type III and IV LSTVs when PT is large as a result of pelvic retroversion to compensate for the sagittal imbalance. However, PI is not affected by posture; therefore, if the measured PI is above the reference range, there is room to reconsider the selected S1. The next question is how to deal with the intermediate type, in which both PI and PT measured by the 2 methods are within the reference range. Currently, in such conditions, we have no choice but to determine the vertebral level of LSTV so that the PI-LL mismatch does not become too large. However, care should be taken even when LL is used as a determinant because it is highly associated with thoracolumbar transitional vertebrae, and the presence of these transitional vertebrae may cause variation in the number of vertebrae in the thoracic and lumbar spine.
Conclusion
Castellvi type III and IV LSTVs were divided into 3 types based on the PI and PT measurements, which represent the characteristics of these LSTVs; that is, the degree of involvement of S1 elements is reflected in the PI and PT measurements. Therefore, it is more clinically realistic to consider LSTV as LLV or S1, depending on the PI and PT measurements. If the measured PI is less than the reference range, it is likely that PI was measured with LSTV as S1; thus, it would be better to re-measure PI with LSTV as LLV. Conversely, if the measured PT is larger than the reference range despite a high PI and no sagittal imbalance, it is likely that PT was measured with LSTV as LLV. Similarly, it is recommended to change the selected S1 and re-measure PT with LSTV as S1.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval Ethical approval for this study was obtained from the Institutional Review Board of Yokohama Minami Kyosai Hospital (approval number: 2-19-11-6).
Data Availability Statement The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.