


Abstract
Background Iatrogenic cervical nerve root injury may occur during cervical spine surgeries, which leads to upper limb palsy. The question of how a permanent iatrogenic upper limb palsy would be managed remains unclear. Recent developments of nerve transfer have led to a considerable interest in its applications. This study outlines a new reconstructive approach forupper limb palsy following cervical spine surgery using nerve transfer.
Methods In an attempt to reconstruct iatrogenic upper limb palsy, we performed nerve transfer in 4 patients with permanently lost functions. Medical Research Council Scale for Muscle Strength was used to assess muscle strength. Electromyography was performed to assess the reinnervation of the target muscles.
Results All patients underwent surgery between 7 and 12 months after primary injury. Spinal accessory nerve to suprascapular nerve transfer with or without transferring the long head of triceps branch of the radial nerve to anterior branch of the axillary nerve was used to reconstruct shoulder abduction in 2 patients. Double fascicular nerve transfer (a fascicle of the ulnar nerve to biceps branch and a fascicle of the median nerve to brachialis branch of the musculocutaneous nerve) was used to reconstruct elbow flexion in 3 patients. One patient had lost both his elbow flexion and shoulder abduction. After a mean of 10 months of follow-up, all patients improved to a muscle strength of M4 without donor deficit.
Conclusion In our view, these results represent an excellent initial step toward the treatment of iatrogenic nerve root injury after spine surgery.
Level of Evidence 4.
Introduction
Although generally successful, both anterior and posterior cervical spine surgery may also lead to life-changing neurological complications. Evidence suggests that more than 38.8% of neurological complications arising from the C5 segment, and after that, C8, C7, C6, or multisegment involvement may occur, respectively.1
C5 root is at higher risk of iatrogenic injury due to its direct and short course as it exits the spinal cord.2 Deterioration in muscle power of the deltoid with or without the involvement of the biceps muscle is a dominant sign but may also have sensory changes and radicular pain.3 Of note, due to the close proximity between C5 and C6 roots (upper trunk), iatrogenic injuries are sometimes simultaneous. C6 root injury may result in weakness of elbow flexion, forearm supination, and wrist extension.4,5
Injury to C7-T1 or C8 and T1 roots is a rare entity in spine surgery in which shoulder and elbow motions are normal. However, marked weakness of the hand may occur.6
The literature emphasizes that such weaknesses are usually transient, and most patients will achieve a full recovery within 2 years. Nevertheless, the question regarding management of a permanent iatrogenic upper limb palsy remains debated.7
In permanent neurological deficits or progressive muscle atrophy, reconstructive surgery by nerve transfer would be considered based on the neurological examination.8,9 In the setting of the iatrogenic cervical nerve root injuries, restoration of the elbow flexion and the shoulder function has higher priority to control antigravity movements.9
In this study, we report the use of nerve transfers to restore lost functions in 4 cases with different nerve root injuries. In addition, we have addressed the question of how nerve transfer can help patients with iatrogenic cervical root palsy. In this regard, a variety of nerve transfers based on the pattern of paralysis are introduced (Figure 1).

The most common nerve transfers that can be performed to treat patients with permanent upper limb palsy after cervical spine surgery. SAN, spinal accessory nerve; SSN, suprascapular nerve; ICN, intercostal nerve; MCN, musculocutaneous nerve; ECRB, extensor carpi radialis brevis branch of radial nerve; AIN, anterior interosseous nerve; FCR, flexor carpi radialis branch of median nerve; PIN, posterior interosseous nerve. Supinator, supinator branch of radial nerve. Brachialis nerve, a branch of the musculocutaneous nerve that innervates brachialis muscle.
Methods
Four patients with upper limb palsy after cervical spine surgery were referred to our center. All patients underwent clinical assessment for muscle strength of the upper limb according to Medical Research Council (MRC) Scale for Muscle Strengthto recognize the extent and degree of injury. Preoperative physical examination revealed no muscle function in the territory of the injured nerve roots, and electromyography findings showed no muscle reinnervation.
Surgery was recommended for patients who had no signs of clinical recovery or poor reinnervation on electromyography despite at least 7 months of physiotherapy. Distal nerve transfer was performed to regain lost functions based on motor deficits in the upper extremity. Subsequently, physiotherapy continued for the patient 1 month after surgery.
Results
A total of 5 nerve transfers were performed in 4 patients. Of the 4 patients, 3 were men and 1 was a woman, ranging between 28 and 42 years of age (mean, 36.5). The causes of injury were posterior laminectomy in 3 cases and anterior decompression in 1 case.
The indications for primary surgery were cervical spinal instability due to traumatic injuries in 2 patients and cervical canal stenosis in 1 patient who underwent posterior laminectomy and in 1 patient whom underwent anterior discectomy for disc herniation. All patients had intact upper limb function before the surgery, so we considered the deficits to be complications of the surgery.
One patient had lost his shoulder abduction above 30°, suggestive of intact suprascapular nerve (SSN) (case 1). Two patients (cases 2 and 3) were referred with loss of elbow flexion as a complication of posterior laminectomy. The fourth patient suffered from loss of both shoulder abduction and elbow flexion after posterior laminectomy (case 4). The Table demonstrates demographics, surgical information, and outcome data for the patients.
Clinical findings and nerve transfers of the patients with iatrogenic cervical spine surgery.
Restoration of shoulder abduction was achieved by nerve transfer. In this regard, 1 patient underwent long head of triceps branch of the radial nerve transfer to the anterior branch of the axillary nerve (case 1), and 1 patient underwent both long head of triceps branch of the radial nerve transfer to the anterior branch of the axillary nerve and spinal accessory nerve (SAN) transfer to the SSN (case 4) (Figure 2).

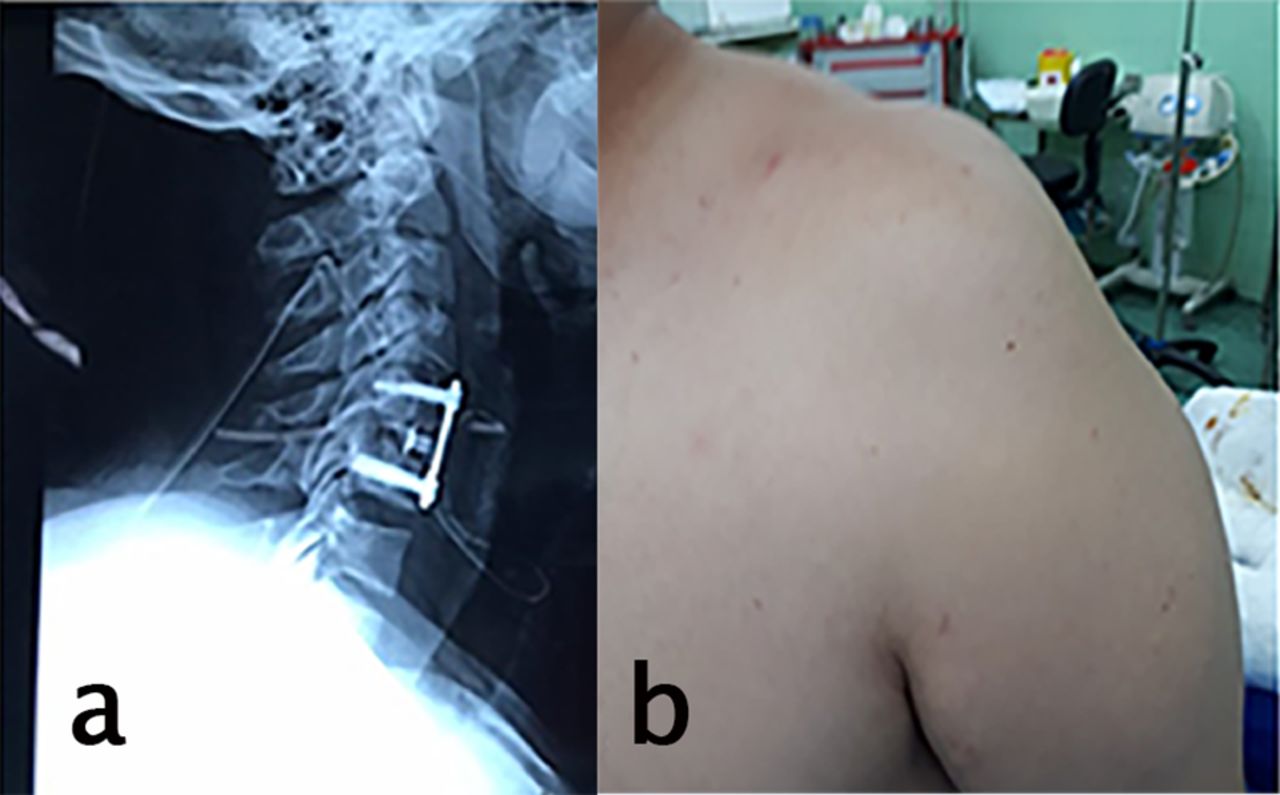
(a) Lateral neck x-ray images after anterior decompression for cervical disc herniation; (b) deltoid muscle atrophy after surgery.
In case of lost elbow flexion, double fascicular nerve transfer (a fascicle of ulnar nerve transfer to biceps branch and a fascicle of median nerve transfer to brachialis branch of the musculocutaneous nerve) was done (cases 2, 3, and 4). After a mean of 10 months follow-up, the patients who underwent an operation for lost shoulder abduction (cases 1 and 4) both achieved MRC grade 4/5 for shoulder abduction. Moreover, all the patients who underwent reconstructive surgery for lost elbow flexion (cases 2, 3, and 4) regained biceps and brachialis muscle strength MRC grade 4/5 (Figure 3).

(a), (b) Preoperative examination showed loss of right elbow flexion after posterior laminectomy for the cervical spinal canal stenosis, (c) postoperative examination after double fascicular nerve transfer.
Discussion
In cases of iatrogenic cervical nerve root injury, nerve grafting is impossible. In such cases, nerve transfer can provide a solution to have an active shoulder abduction and elbow flexion.10 The originality of this study is to explore the availability of nerve transfer in iatrogenic cervical nerve root injuries. Our results offer compelling evidence for the application of nerve transfer in iatrogenic nerve root palsies. Considering most of the iatrogenic nerve root injuries occur in midcervical roots, including C5 and C6, reconstruction of shoulder abduction and elbow flexion has higher priority in the setting of iatrogenic nerve root palsy.
Reconstruction of Shoulder Abduction
Shoulder abduction is initiated by supraspinatus. After 15°, the supraspinatus muscle helps the deltoid with the abduction of the arm up to 90°.11 For restoration of shoulder function, donor nerves that have been used include the SAN, intercostal nerves and triceps branches, thoracodorsal nerve, phrenic nerve, and medial pectoral nerve.9,12,13 The 2 most commonly used nerve transfers to restore the shoulder abduction are SAN transfer to the SSN and the long head of the triceps branch transfer to the axillary nerve.
To the best of our knowledge, Afshari et al reported the only case regarding the use of nerve transfer in iatrogenic nerve root injuries.8 Their case was a 46-year-old man who underwent C3-C4 and C4-C5 right-sided foraminotomies due to the right foraminal stenosis. Postoperatively, the patient developed severe weakness in the right arm and shoulder and altered sensation in the shoulder area. Nerve transfer was considered 6 months after spinal surgery because of permanent neurological deficits. The medial head of the triceps nerve branch of the radial nerve was transferred to the axillary nerve to reinnervate deltoid and teres minor. At 5-month follow-up, full forward flexion and lateral elevation of the shoulder were reported. The results of this article strengthened our confidence in applying for nerve transfer in patients with iatrogenic cervical nerve root injuries. The SAN is a vital donor, which can be used for transferring to SSN. Moreover, it can be transferred with an interpositional nerve graft to the musculocutaneous or the axillary nerve.
Leechavengvongs et al published results of nerve transfer to deltoid muscle using the nerve to the long head of the triceps in 7 patients with brachial plexus injuries. Recovery in all of their patients (deltoid muscle MRC grade 4) showed that the aforementioned technique is a promising option to restore shoulder function.13 Considering that the triceps action is synergistic with shoulder abduction, using 1 branch of triceps muscle (long head or medial head) is an excellent choice as a donor nerve. Among the 3 heads of the triceps muscle, the branch to the long head of the triceps has the largest diameter and highest number of motor axons. On the other hand, this branch has the least importance for elbow extension.14 We used double nerve transfers for shoulder function (SAN to SSN and radial to axillary nerve) in 1 case because of loss of function in both supraspinatus and deltoid. Concomitant reconstruction of both the axillary nerve and SSN improves the shoulder function.
Reconstruction of Elbow Flexion
In the absence of elbow flexion after cervical spine surgery, the donor nerves that can be transferred include the intercostal nerve, ulnar nerve (Oberlin procedure), SAN, and medial pectoral nerve.15–18 We performed a double fascicular nerve transfer (a fascicle of the ulnar nerve to the biceps branch and a fascicle of the median nerve to the brachialis branch of the musculocutaneous nerve) to restore elbow flexion in 3 patients with iatrogenic cervical nerve root injury.
Comparing the results of published literature using the abovementioned potential donor nerves demonstrates that using the ulnar nerve (Oberlin procedure) is associated with better outcomes.19 Satisfactory outcomes of the Oberlin procedure in patients with acute flaccid myelitis20 and transverse myelitis21 support the idea that this procedure can also be helpful in iatrogenic cervical nerve root injuries.
Advantages of using the ulnar nerve as a donor include a better and quicker recovery of elbow flexion and less invasive surgery, which make it the donor of choice for biceps reinnervation comparing other nerve transfers.5,22 However, Martins et al showed that using an ulnar transfer alone (Oberlin procedure) provides outcomes equivalent to double fascicular nerve transfer, we considered double fascicular nerve transfer for our patient.23 Our results demonstrated the effectiveness of double fascicular nerve transfer in reconstructing upper limb palsy. More studies are necessary to compare double fascicular nerve transfer and Oberlin procedure in the setting of iatrogenic nerve root palsy.
Reconstruction of Elbow Extension
Loss of elbow extension is rarely seen as a consequence of spine surgery. Elbow extension has been given a lower priority comparing shoulder abduction and elbow flexion because the passive elbow extension is achieved by gravity. To restore elbow extension, the potential donor nerves include the intercostal nerves, posterior branch of the axillary nerve, and ulnar nerve fascicle.24,25 We recommend transferring a fascicle of the ulnar nerve to the long head of triceps branches of the radial nerve to restore elbow extension.
Reconstruction of Hand Function
Hand function may be impaired in C7-T1 nerve root injuries but is rarely seen as a complication of cervical spine surgery; if so, this condition can also be restored by nerve transfer (Figure 1). In our study, an improvement in the lost functions of the upper extremity due to spine surgery supports the efficacy of nerve transfer for the treatment of iatrogenic nerve root injuries. Despite the effectiveness, the timing of the nerve transfer reconstruction is still challenging. Generally, a significant motor deficit with repeated clinical examinations and no recovery in neurophysiological studies indicates that surgical intervention should be considered. In cases without useful muscle function, motor nerve transfer is recommended 6 to 12 months after the injury to promote muscle function.8,9
Conclusion
This study shows preliminary success of nerve transfer as a possible solution for patients with postoperative root injury after cervical operations. Further studies are needed to establish the long-term outcomes of different potential nerve transfers in this field.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval The study was approved by the institutional review board of the Guilan University of Medical Sciences Department of Neurosurgery.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.