


Abstract
Background Over the years, lumbar laminectomy has been widely employed by spinal surgeons for many purposes throughout the spinal canal. The Misonix BoneScalpel relies on ultrasonic energy and allows the surgeon to make precise osteotomies while protecting collateral or adjacent soft tissue structures. Amplification of electric impulses allows the blade in the BoneScalpel to oscillate at very high frequencies, which thus allow it to cut bone with immense amounts of heat, which are then tempered with copious irrigation to prevent overheating. The purpose of this study is to outline and detail an innovative technique while providing insight into the technique’s clinical application in a variety of spine surgeries.
Methods Data were retrospectively collected from medical charts and surgical reports from February 2018 to July 2021 for each surgery in which the ultrasonic scalpel was used to perform the H laminectomy. Baseline demographic information was recorded, including age, gender, laminectomy indication, and the number of levels of laminectomy.
Results A total of 85 patients (64 women, 21 men) were included in this study. The mean age of the patients was 63.7 years. Of those patients, 42.4% underwent H laminectomy for degenerative stenosis without instrumentation, 31.8% for degenerative stenosis with instrumentation, 9.4% for traumatic injuries, and 7.1% for revision surgery with instrumentation. Approximately 55% of patients underwent laminectomy of 2 or more levels, while the rest underwent single-level laminectomy. No patients had a dural tear or cerebrospinal fluid (CSF) leak as a result of the BoneScalpel.
Conclusions The H laminectomy is another safe and effective way to perform a lumbar laminectomy. The technique has not been previously reported in the literature. No patients experienced a dural tear or CSF leak from the BoneScalpel using the H laminectomy technique. This technique affords the surgeon enhanced control of the dura-ligamentum interface. Even if the surgeon is not very experienced with the BoneScalpel, this technique provides an inherent safety mechanism with constant visualization/tactile feedback of the tip of the instrument and osteotome.
Level of Evidence 3.
Introduction
The first laminectomy was performed in 1814, but the first successful laminectomy was not recorded until 1838.1 Over the years, lumbar laminectomy has been widely employed by spinal surgeons for many purposes throughout the spinal canal. Some examples include in addition to osteotomies in deformity correction,2 en bloc spondylectomy for tumors,3 and laminoplasty4–6 in myelopathy. The Misonix BoneScalpel (introduced in 2012; Figure 1) relies on ultrasonic energy (Piezosurgery, introduced in 2000, and Sonopet, introduced in 2013) and allows the surgeon to make precise osteotomies while protecting collateral or adjacent soft tissue structures.7–9 Amplification of electric impulses allows the blade in the BoneScalpel to oscillate at very high frequencies (over 22,500 cycles/s), which thus allows it to cut bone with immense amounts of heat, which are then tempered with copious irrigation to prevent overheating (Figure 2). The pulsations pulverize noncompliant crystalline structures resulting in a precise cut. The more compliant adjacent soft tissue is not affected by the ultrasonic oscillation.10 A variety of pathologies such as degenerative disease with stenosis, trauma, infections, and revisions with stenosis are commonly encountered. With many different conditions warranting decompression of the spinal canal, this technique may afford one with an increased ability to limit inadvertent bony removal, reduce bleeding (particularly from the bone), and obtain greater control of the ligamentum-dura interface. A novel and yet innovative technique is now introduced to the literature with the initial clinical experience using the BoneScalpel.11 Using an ultrasonic osteotome or BoneScalpel has previously been described in the literature. Our literature search, however, has not discovered the purposeful or deliberate use of a transverse cut through the lamina for simple routine performance of a lumbar laminectomy.

The BoneScalpel (Misonix) with 25-mm blade (to make laminectomy troughs).
The BoneScalpel (Misonix) with hook shaver (widen laminectomy if needed).
The purpose of this study, therefore, is to outline and describe an innovative technique in detail while providing insight into its clinical application. The result of this study may represent a possible paradigm shift in the future of this procedure as it is becoming widely accepted as a safe alternative for this procedure.
Surgical Technique
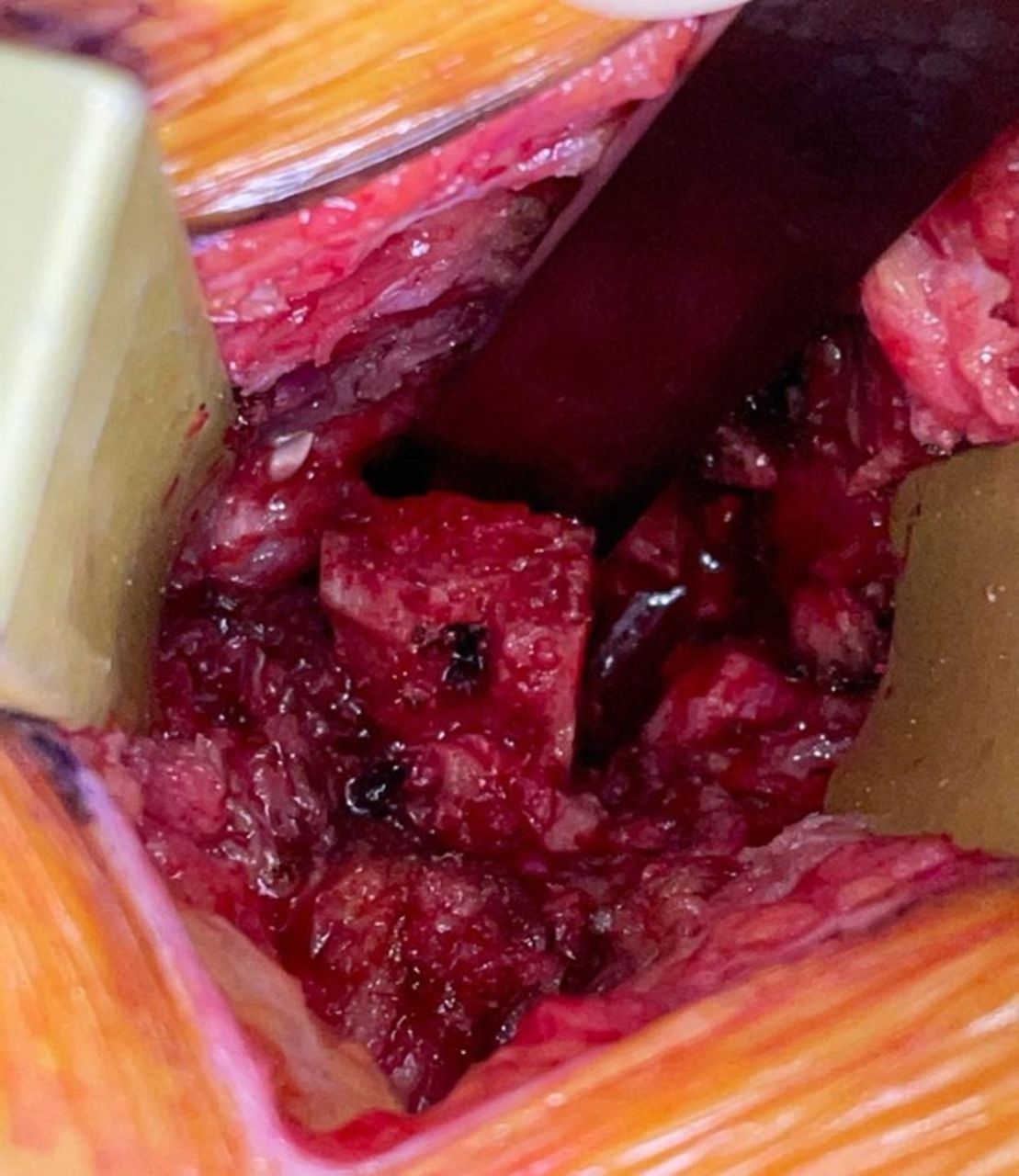
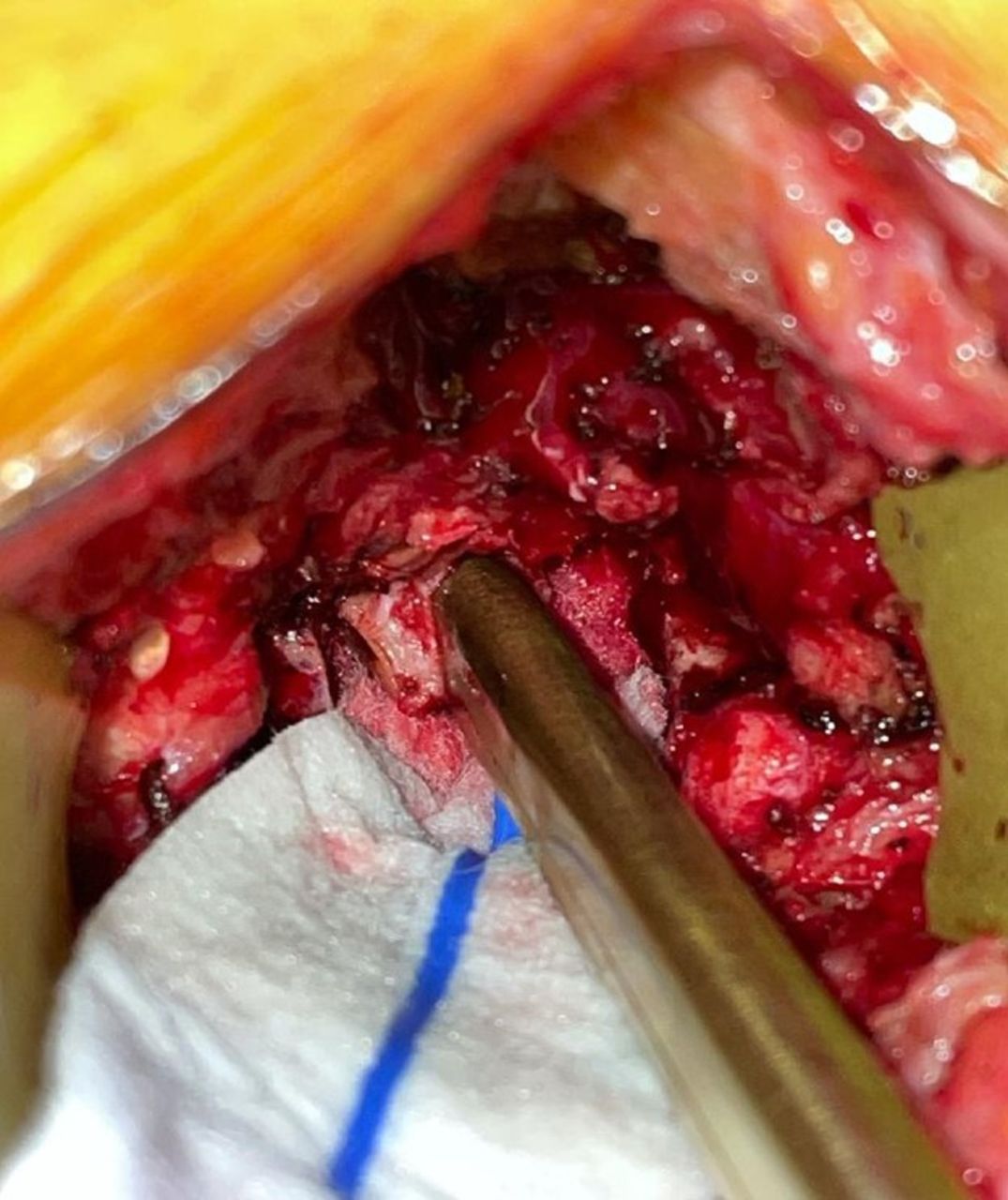
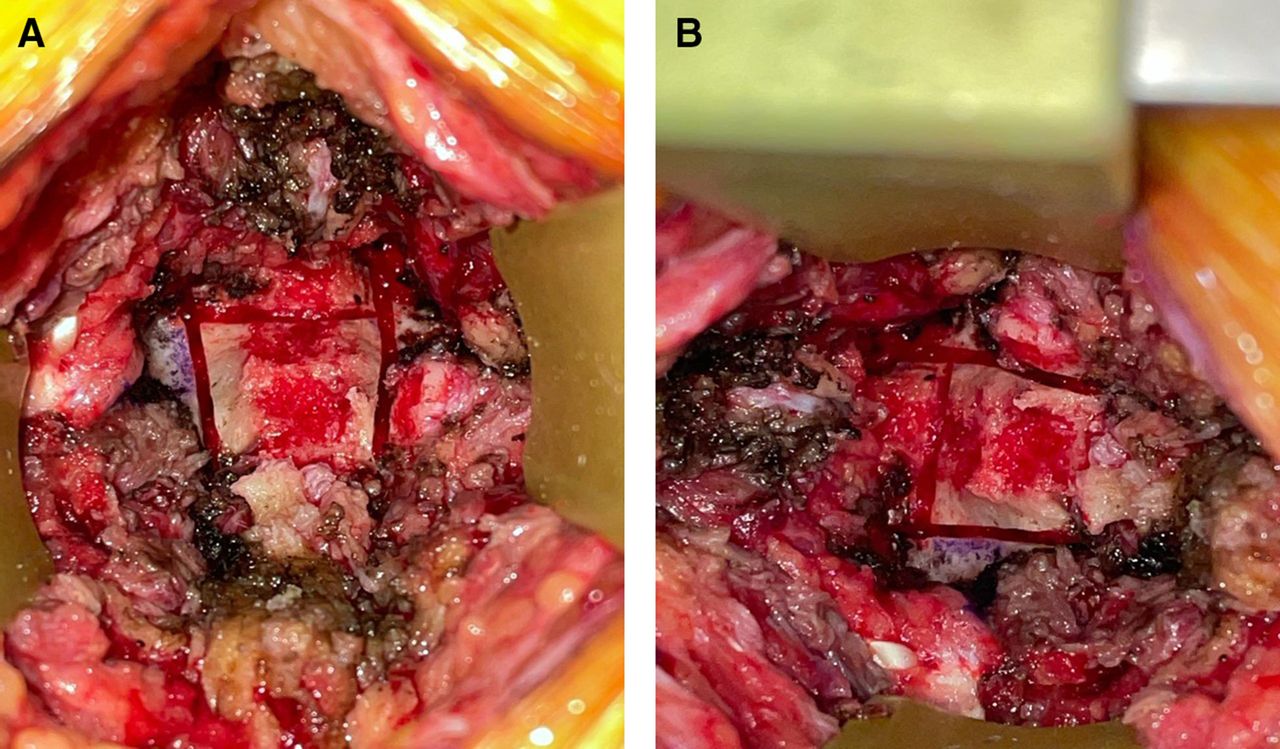
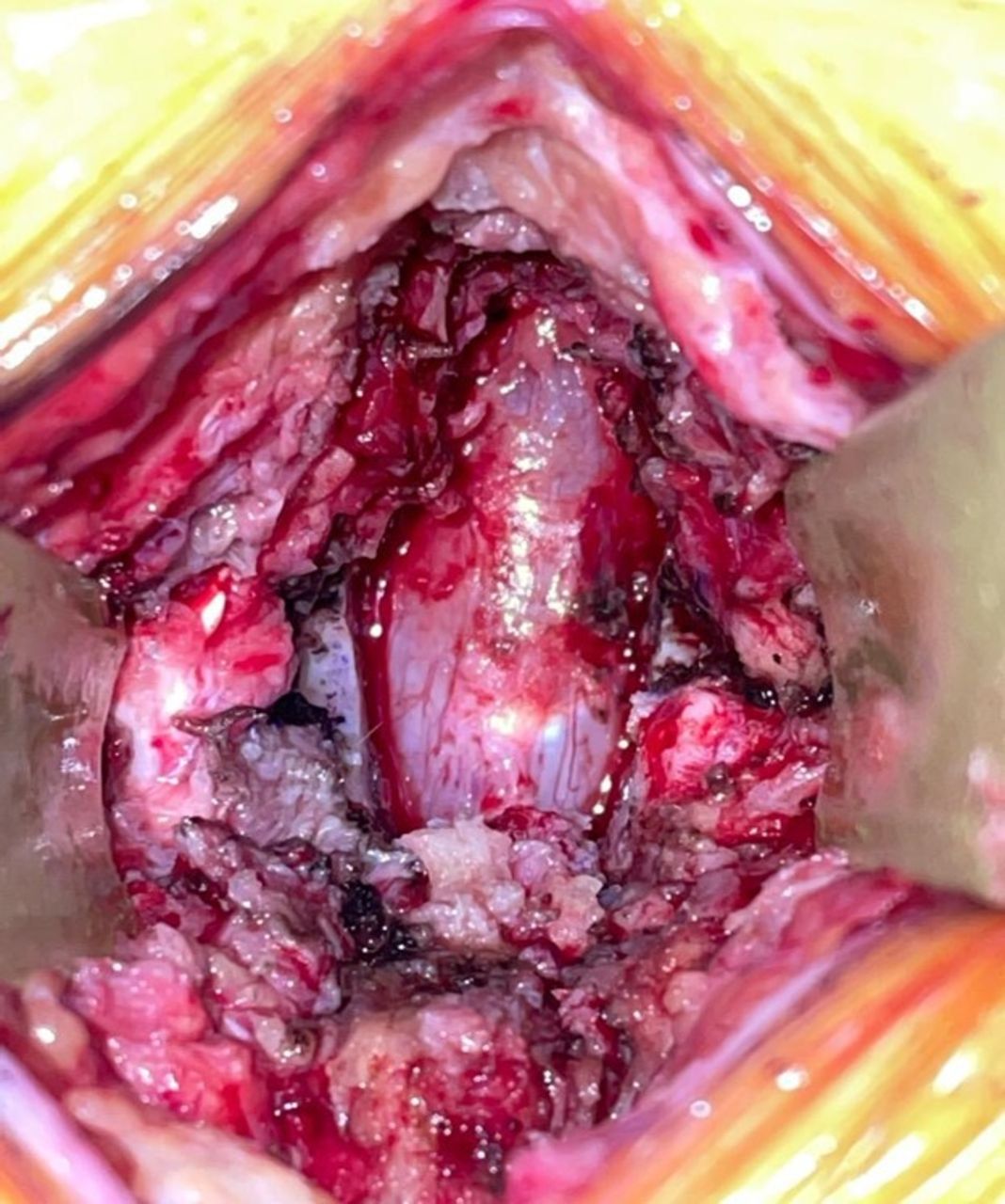
After a standard subperiosteal dissection through an open or mini-open incision, the interspinous ligament should be divided with cautery or sharply (Figure 3), with the purpose of isolating the level(s) of interest. Rongeurs can be now used to bite the spinous process down to the level of the lamina until the ligamentum flavum can be plainly identified in relation to the lamina (Figure 4). The pars interarticularis should now be identified bilaterally. After marking a line or point that is at 5 mm from the pars’ lateral extent, longitudinal troughs are cut from the top to the bottom of the lamina(e) of interest. At this point, the lamina does not need to be completely floating and freely detached. Next, a transverse trough (Figure 5A) is cut through the superior third of the respective lamina connecting the longitudinal troughs like the letter “H” (Figure 5B). A mallet and curved osteotome are now used to access, loosen, and mobilize the inferior laminar segment caudally (Figure 6). Once elevated away from the spinal canal, it is removed with rongeurs. Cottonoids are now placed onto the dura or remaining ligamentum flavum. Kerrison rongeurs are now used to remove the remaining superior third of the lamina (Figure 7). Immediate and direct visualization is afforded at all times so that cottonoids can again be used to protect the neural elements during the final stages of decompression (Figures 7 and 8).

Division of the proximal and distal interspinous ligament with the Bovie.

Removal of spinous process/superficial lamina.

(A) Initial “H laminectomy” troughs. (B) Initial “H laminectomy” troughs seen in transverse orientation.
Elevation of the inferior (caudal) laminar with a curved osteotome.
Removal of the superior portions of the remaining lamina.
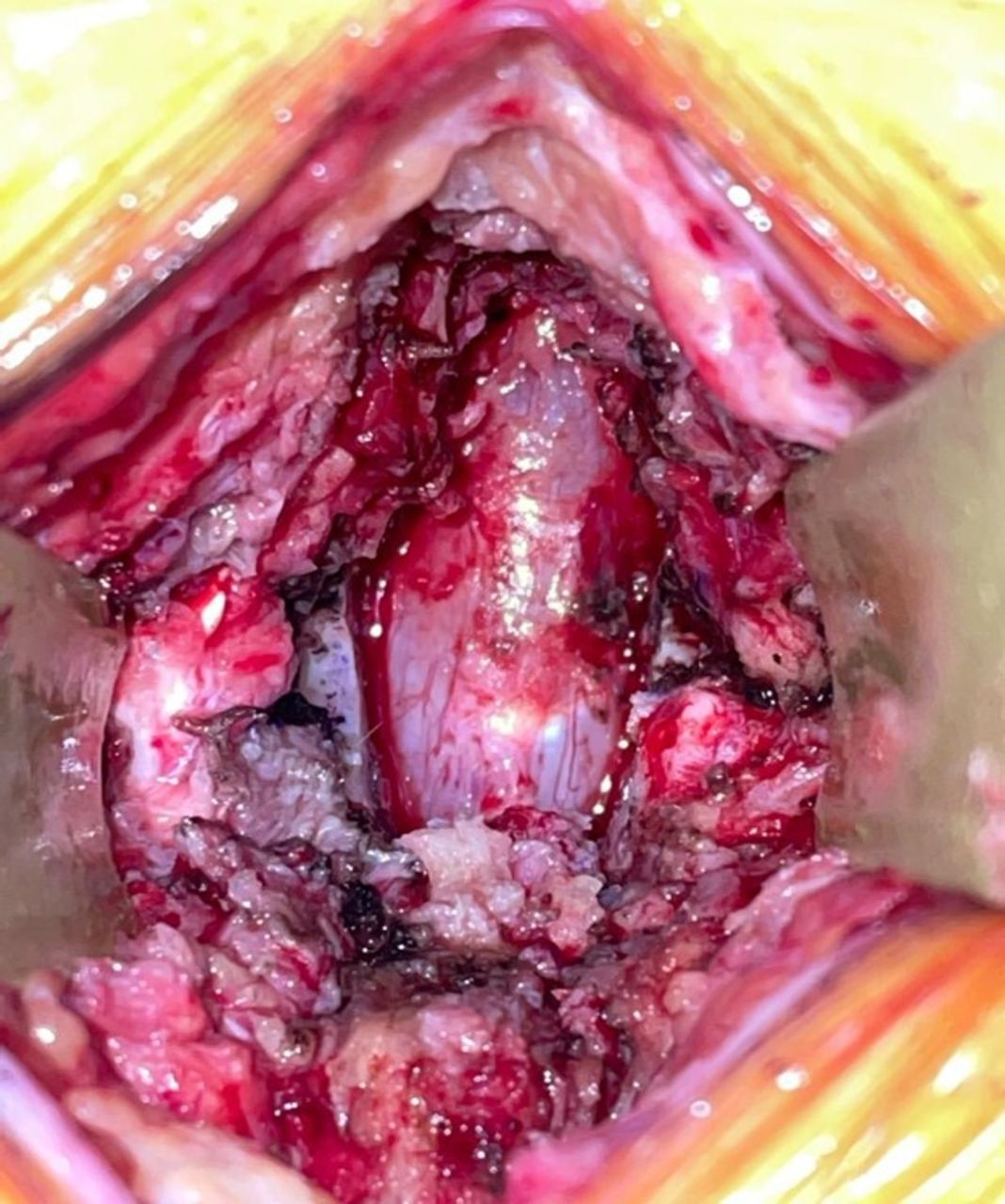
Completion of laminectomy.
Methods
A single surgeon began performing the H laminectomy in October 2017; however, it was routinely or exclusively performed starting in February 2018. A retrospective analysis was then performed on all laminectomies in the surgeon’s practice from February 2018 to July 2021 to select the eventual cohort of interest. Any patient who required a lumbar laminectomy in the study period was included if the levels of interest had not yet been laminectomized (even partially). An entire or full and intact lamina is required for this technique. Contraindications included cervical or thoracic laminectomies as well as revision lumbar laminectomies (segments that already had full or partial laminectomy).
Baseline demographic information was recorded, including age, gender, laminectomy indication, and number of levels of laminectomy, followed by clinical outcomes. All patients were followed for a minimum of 12 months.
Results
Of 245 laminectomies recorded in the review period, 66 were cervical, 44 were thoracic, and 135 were lumbar. Within the lumbar laminectomies, 58 were for degenerative conditions including no instrumentation without prior surgery, 31 were for degenerative conditions including instrumentation without prior surgery, 18 were performed in revision surgeries including instrumentation, 10 were performed in trauma, 5 were performed for emergent cauda equina cases, 5 were performed for metastatic tumors with epidural compression, 4 were performed for other reasons, 3 were performed for epidural abscesses, and 1 was performed for a sacral spinal cord untethering; these patients were excluded.
A total of 85 patients had the “H laminectomy” performed and thus comprised the cohort of interest. Of these patients, 75% (n = 64) were men, and the rest were women (n = 21). Among the patients who underwent the H laminectomy, 42.4% of procedures were for degenerative stenosis without instrumentation, 31.8% were for degenerative stenosis with instrumentation, 9.4% were performed for traumatic injuries, 7.1% were for revision surgery with instrumentation, 4.7% were for metastatic tumors with epidural compression, 2.4% were for epidural abscesses, 1.2% were for revision of prior surgery without instrumentation, and 1.2% were for spinal cord untethering (Table). The average age of H laminectomy patients in the cohort was 63.7 years (range 21–91 years). Forty-seven patients underwent laminectomy of 2 or more levels and 38 patients underwent single-level laminectomy.
No H laminectomies were aborted or converted to another technique. No patients had a dural tear or cerebrospinal fluid (CSF) leak as a result of the BoneScalpel. In this series, a total of 3 dural tears (3.5%) were encountered. None of the injuries was directly associated with the use of the ultrasonic scalpel. One patient had a dural tear during a single-level laminectomy simply from placing traction on a pinhole-sized dorsal dural ligament. Two patients had dural tears during multilevel laminectomies with instrumentation/arthrodesis while performing the lateral recess decompression with Kerrison rongeurs. No patients in the cohort developed clinical/radiographic instability that warranted fusion.
The primary diagnosis of study patients for indications for H laminectomy (N = 85).
Discussion
The purpose of this study was to describe an innovative technique when performing a lumbar laminectomy using a Misonix BoneScalpel. Based on this study’s results, the H-laminectomy technique provides spinal surgeons with yet another way of performing a lumbar laminectomy. Traditionally, different burrs are used with a high-speed drill, or rongeurs are used entirely. With the advent of the “ultrasonic osteotome,” 1 notable advantage is that the bony removal is more precise without the need to continually redefine the edges or extent of the intended laminectomy. As with a diamond or acorn burr, there is essentially no bony bleeding; however, the precision of the desired cut is vastly improved in theoretically less time, with no need to continually redefine the extent of laminectomy while getting down to the level of the ligamentum flavum. In patients with severe lumbar stenosis, there is an inherent risk of a spinal fluid leak during a laminectomy. No patients in the cohort experienced a dural tear during the initial bony removal or flavectomy. One patient had a dural tear during a single-level decompressive laminectomy with the removal of a dorsal dural ligament. Another 2 patients experienced CSF leak without an obvious tear during lateral recess decompression. None of the patients experienced any untoward neurologic or clinical events and was managed with recumbency for 24 hours. In comparison, none of the patients in this cohort experienced a dural tear as a direct result of the BoneScalpel.12
The extent to which one desires to decompress the lateral recesses may impact how likely one is to experience a dural tear. The ultrasonic BoneScalpel has been safely employed widely, even for en bloc spondylectomy, laminoplasty, and atypical decompressions in achondroplastic patients.4–6 Decompressions for central stenosis and claudication may experience a very low or even negligible rate of a dural tear with the H laminectomy. The initial bony removal and flavectomy can be limited to the bony cuts, and the need to use Kerrison rongeurs, curettes, and dural mobilization/retraction can be minimized. No patients in the cohort had a neurologic injury or dural tear directly from the BoneScalpel penetrating the dura. It is postulated by some that there is possibly less trauma, which can lead to improved outcomes with the use of ultrasonic osteotomes.12,13 Krishnan et al noted a statistically significant reduction in neurologic injuries/deficits comparing patients undergoing laminectomy in the thoracic region with a burr vs the ultrasonic BoneScalpel.12 Additionally, they noted statistically significant decreases in operative time, blood loss, and length of stay in patients treated with the ultrasonic osteotome vs the burr and suggested that thermal injury may have played a role in their “Discussion” section.12 In the present study, there were no reports of thermal injuries either. The BoneScalpel must repeatedly be moved in and out of the osteotomy because it has been shown that it may reach temperatures that can cause thermal injury.14 Cauda equina injuries during the access of the spinal canal can be further mitigated with the H laminectomy technique at this time. The key of the technique is that there is direct surface visualization of the osteotome with the inferior portion of the lamina while elevating it. There is also direct visualization of the ronguers and curettes used above while elevating the initial inferior laminar segment. Lastly, direct visualization of the Kerrison ronguers during the completion of the superior third of the lamina is afforded. Cottonoids are used to protect the dura while mobilizing it inferiorly away from the remaining lamina/ligamentum.
In the “H laminectomy,” although a transverse trough is made in the superior third of the lamina, this is the caudal extent rather than the cranial extent of the remaining superior lamina. The ligamentum flavum should still be present in this portion and protecting the dura. The BoneScalpel should not penetrate soft tissue and will generally stop working if excessive force is applied or if there is a change in the pitch of oscillations, indicating a change in the substrate being cut. We previously employed a different technique using the Misonix BoneScalpel as well as high-speed drills for laminectomy in the lumbar spine. The fear of “plunging” with a BoneScalpel keeps some surgeons from using the ultrasonic BoneScalpel. The lumbar laminae are the thickest compared with the cervical and thoracic laminae, so more force and deeper cuts are needed to traverse them. In this technique, the cuts can be made always visualizing the tip of the ultrasonic scalpel with frequent pauses. Furthermore, releasing the caudal lamina with the curved osteotome can be performed by cracking it instead of recessing the osteotome and not being able to see the depth of the instrument. At no point in this technique should the surgeon lose the ability to directly visualize their instrument tips; doing so is commonly performed but is generally reserved for those with vast experience using this instrument. Without the need to drill down repeatedly to the level of the ligamentum flavum, the H laminectomy mitigates the risk of dural injury during bony removal and flavectomy. The bone edges in the laminectomy are smooth in this technique. This, in theory, also decreases the risk for a delayed CSF leak second to sharp bony edges. With a defined technique, duration for lumbar laminectomy should be more uniform. Other factors (patient body habitus, exposure time, and closure time) are likely to affect actual operative times as well.
In spinal surgery, any tool can be dangerous if not used with care. While using the curved osteotome to elevate the caudal lamina, direct visualization of the edges of the osteotome should never be lost. This could result in a catastrophe. While in the transverse cut of the lamina with the curve facing upward, very gentle downward pressure on the osteotome should elevate the fragment upward and free it. This can also be performed laterally in longitudinal cuts, if needed. The surgeon may opt to deepen any of the cuts with the BoneScalpel or frequently pause while using the osteotome and mallet to assess the mobility of the laminar segment.
Cost must be taken into account when choosing an instrument as part of any spinal surgeon’s armamentarium. Generally, the generator with foot pedal and handpieces for the Misonix BoneScalpel costs roughly $130,000 plus about $500 per blade. One blade is typically sufficient per case but can vary with very dense/sclerotic bone or when addressing several levels. However, this pricing is heavily dependent on a hospital or hospital system’s group purchasing organization. Compare this with the Medtronic Midas Rex (generally in the region of $50,000 for a complete pneumatic set or $70,000 for a complete electric set with drill bit replacements in the range of $100) or Stryker Sumex (roughly $50,000 for a complete set and $100 for drill bit replacements).
The learning curve with the Misonix BoneScalpel is variable. Tactile feedback while using this tool is extremely important. Perhaps those who frequently use osteotomes may feel more comfortable with this tool much earlier than those who do not. The surgeon in this particular study noted proficiency within 3 weeks. He also noted that with time, his level of proficiency has continued to grow as expected with the repeated use of a specialized instrument.
This technique, although safe, will need a larger number of patients before a broader recommendation is made for its use. An additional limitation of the study involves the selection bias inherently involved when only 1 surgeon’s experience is reported. A successful procedure with the BoneScalpel is also nuanced, in that the surgeon must have a significant level of comfort with it before ensuring safety, no matter the technique. Also, excluding exposure and closure times, the actual duration of laminectomies was not recorded. Therefore, overall case lengths do not adequately highlight the isolated laminectomy times.
Conclusion
The H laminectomy is another safe and effective way to perform a lumbar laminectomy. The technique has not been reported in the literature. No patients experienced a dural tear or CSF leak from the BoneScalpel using the H laminectomy technique. This technique affords the surgeon enhanced control of the dura-ligamentum interface. Even if the surgeon is not very experienced with the BoneScalpel, this technique provides an inherent safety mechanism with constant visualization/tactile feedback of the tip of the instrument and osteotome. Further decompression into the lateral recesses poses an unchanged risk of CSF leak.
As with all tools and instruments, experience and familiarity are extremely important. Nuances regarding the practical use of the BoneScalpel are an ever-present factor regarding its safety. This current study reflects the work of a single surgeon; however, further evaluation of this technique with surgeons of different levels of experience (with the BoneScalpel) was not performed and will be needed to evaluate in future research studies. It is, however, hypothesized that the “H laminectomy” technique should allow for direct visualization of the BoneScalpel osteotomes. In theory, this should be safer than any techniques where the instrument tips cannot be seen at all deep to the laminar surfaces.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Ram Haddas reports grants or contracts from Medtronic, SI-Bone, and the Cervical Spine Research Society (all paid to the institution) and consulting fees from Medtronic. Akwasi Boah has nothing to disclose.
IRB Approval The study was approved by the Western Institutional Review Board for the Protection of Human Subjects (IRB#: 20153981).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.