


Abstract
Background The sacroiliac joint (SIJ) transfers the load of the upper body to the lower extremities while allowing a variable physiological movement among individuals. The axis of rotation (AoR) and center of rotation (CoR) of the SIJ can be evaluated to analyze the stability of the SIJ, including when the sacrum is fixed. The purpose of this study was to determine how load intensity affects the SIJ for the intact model and to characterize how sacropelvic fixation performed with different techniques affects this joint.
Methods Five T10-pelvis models were used: (1) intact model; (2) pedicle screws and rods in T10-S1; (3)pedicle screws and rods in T10-S1, and bilateral S2 alar-iliac screws (S2AI); (4) pedicle screws and rods in T10-S1, bilateral S2AI screws, and triangular implants inserted bilaterally in a sacral alar-iliac trajectory ; and (5) pedicle screws and rods in T10-S1, bilateral S2AI screws, and 2 bilateral triangular implants inserted in a lateral trajectory. Outputs of these models under flexion-extension were compared: AoR and CoR of the SIJ at incremental steps from 0 to 7.5 Nm for the intact model and AoR and CoR of the SIJ for the instrumented models at 7.5 Nm.
Results The intact model was validated against an in vivo study by comparing range of motion and displacement of the sacrum. Increasing the load intensity for the intact model led to an increase of the rotation of the sacrum but did not change the CoR. Comparison among the instrumented models showed that sacropelvic fixation techniques reduced the rotation of the sacrum and stabilized the SIJ, in particular with triangular implants.
Conclusion The study outcomes suggest that increasing load intensity increases the rotation of the sacrum but does not influence the CoR, and use of sacropelvic fixation increases the stability of the SIJ, especially when triangular implants are employed.
Clinical Relevance The choice of the instrumentation strategy for sacropelvic fixation affects the stability of the construct in terms of both range of motion and axes of rotation, with direct consequences on the risk of failure and mobilization. Clinical studies should be performed to confirm these biomechanical findings.
Introduction
The sacroiliac joint (SIJ) is the anatomical structure connecting the ilium and sacrum; its principal function is to transfer the load of the upper body to the lower extremities while allowing a certain degree of motion. The anatomical structure of this joint is variable among individuals.1–3 Several in vivo studies found that its physiological movement varies from about 15° (antagonistic mobility of the 2 ilia) to less than 3°, possibly influenced by degenerative disorders of the joint, which were typically present in the joints investigated in these studies.4,5 Many in vitro studies showed a range of nutation movement up to only 3° that might also be expected under normal physiological conditions in which the ligaments guide and restrict the joint motion.6,7
Despite this relatively low motion, many researchers have studied the movement of the SIJ because it is considered a possible cause of low back pain and posterior pelvic girdle pain.8–14 Such studies typically investigated rotational angles and translation of the SIJ in the anatomical planes,1 focusing on the “quantity” of the motion. To describe “quality” of motion, other parameters such as axis of rotation (AoR) and center of rotation (CoR) of the SIJ can be evaluated with respect to several individuals, load intensities, or loading planes in order to further analyze the motion and the stability of the SIJ.7
The study of the SIJ is very relevant when long thoracolumbar fixation and fusion procedures are performed to treat spinal disorders such as adult scoliosis, fixed sagittal imbalance, and high-grade spondylolisthesis. When the fixation involves the sacrum, symptomatic early degeneration of the SIJ due to increased stress and motion is a common finding, occurring in up to 75% of cases.15 Additional implants allowing for sacropelvic fixation are necessary in long spinal fusion to the sacrum to treat these disorders.16–18 Iliac screws and alar-iliac screws are the 2 implant types most commonly used when a sacropelvic fixation is performed. While such implants have been used for decades,19,20 they undergo instrumentation failure in a relatively high number of cases.20–23 In 1 clinical study, iliac screws resulted in an overall failure rate of 34.3%,24 while another clinical study resulted in a revision rate of 27.9% due to mechanical failure or wound complications.25 A third study reporting on acute S2 alar-iliac screw (S2AI) failures that occurred 6 weeks postoperatively demonstrated a failure rate of 5%.26 As such, these fixation methods are still a subject of investigation.
Supplementing iliac and S2AI screws with triangular titanium implants (iFuse Implant System, SI-BONE, Inc., Santa Clara, CA, USA) inserted with a minimally invasive technique can be an option to further stabilize the SIJ. In a previous study, we investigated the use of these triangular implants in addition to S2AI screws as compared with S2AI screws alone by means of a finite element model of T10-pelvis. This study revealed that the use of triangular implants in the innovative configurations has the potential to become clinically relevant in subjects needing a particularly solid fixation, such as in the case of osteoporosis.27 However, such configurations were not investigated in terms of AoR and CoR of the instrumented SIJ; extending the study to these aspects may further clarify the effects of these triangular implants, as well as of other sacropelvic fixation techniques, on the SIJ.
The first aim of this study was to determine whether load intensity affects the direction of the AoR and the position of the CoR of the intact SIJ in extension and flexion. The second aim of this study was to characterize how sacropelvic fixation performed with different techniques and implant configurations affect the AoR and CoR of the SIJ in extension and flexion.
Methods
Finite Element Model
A finite element model of T10-pelvis developed in another study,27 which details the meshes, element types, as well as validation of the intact model, was used as a baseline. The material properties of the ligaments are reported in Tables 1 and 2.28–31 Ligaments were kept intact for all configurations described in this study.
Finite element modeling of the ligaments of the sacroiliac joint.
Finite element modeling of the ligaments of the thoracolumbar spine (from calibration against Cook et al31).
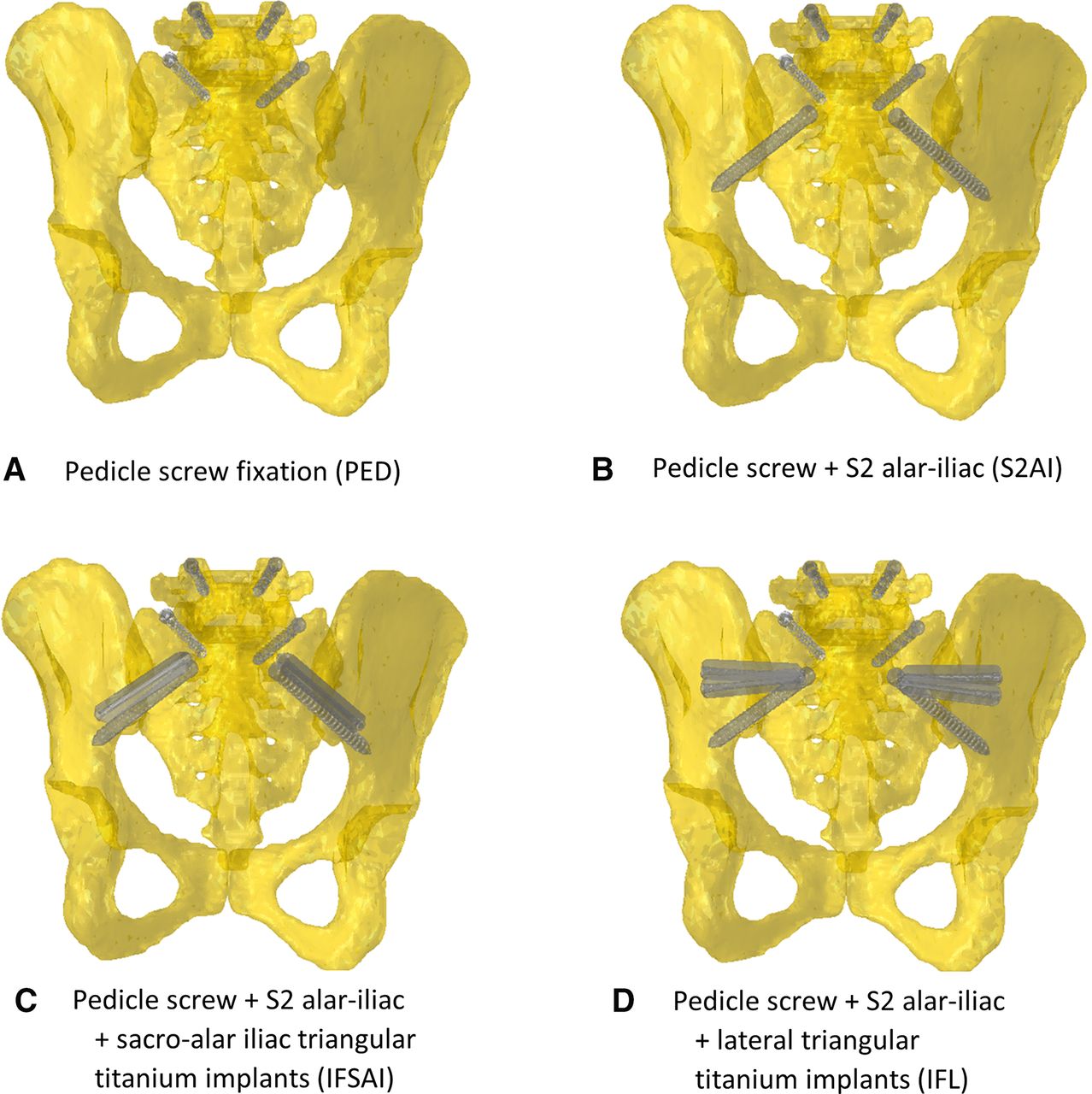
In addition, 4 instrumented models derived from the intact model and developed in a previous study27 were considered: (1) posterior rods and pedicle screws in the thoracolumbar spine and S1 (PED); (2) posterior rods and pedicle screws in the thoracolumbar spine and S1, and bilateral S2AI; (3) posterior rods and pedicle screws in the thoracolumbar spine and S1, and bilateral S2AI and triangular implants inserted bilaterally in a sacral alar-iliac trajectory (IFSAI); and (4) posterior rods and pedicle screws in the thoracolumbar spine and S1, and bilateral S2AI and 2 bilateral triangular implants inserted in a lateral trajectory (IFL) (Figure 1).

The 4 configurations of the instrumentation in the sacropelvic region: (A) pedicle screw fixation (PED); (B) posterior fixation and S2 alar-iliac fixation (S2AI); (C) same as (B) bilaterally supplemented by a triangular titanium implant placed in a sacro-alar-iliac trajectory (IFSAI); (D) same as (B) supplemented by 2 bilateral laterally placed triangular titanium implants (IFL). Rods not shown.
In all models, the triangular titanium implants were not connected to the posterior rods and had a length of 50–70 mm and an inscribed circular diameter of 7 mm; the posterior rods were modeled as beam elements with circular section and had a diameter of 5.5 mm; pedicle screws had a length of 40 mm and a diameter of 6.5 mm; S2AI screws had a length of 85 mm and diameter of 8.0 mm. All implants were modeled as having the material properties of titanium (elastic modulus of 110 GPa and Poisson’s ratio of 0.3).
Boundary Conditions and Interactions
The interaction between pedicle screws (T10-S1) and thoracolumbar vertebrae or sacrum, between S2AI and sacrum or ilium, and between triangular implants and sacrum or ilium was the same as described in a previous study.27 In brief, the interactions in the thoracolumbar region were modeled by means of embedded elements in order to impose 0 relative displacements between pedicle screws (T10-L5) and bone. In the sacrum and ilium, spring elements with stiffness calibrated from experimental measurements were used to define the interaction between implants and bone in order to simulate the micromovements of these implants under the effect of loading.
A pure moment of 7.5 Nm in flexion and extension without any additional compressive load (ie, follower load) was applied to the upper endplate of the T10 vertebra using a set of rigid beam elements in the sagittal plane in both directions. Double leg stance was replicated by constraining all nodes belonging to the bilateral acetabula of the finite element models.
Validation and Model Metrics
Validation of the intact model was supported by comparing the rotation and the displacement of the sacrum in extension and flexion against values found in literature.7 A qualitative comparison of (1) AoR and (2) CoR of the SIJ at incremental steps from 0 to 7.5 Nm was performed for the intact model. Following evaluation of the intact model, the AoR and CoR of the SIJ were identified for the instrumented models. Finally, a qualitative comparison among the 5 models (intact and instrumented models) at 7.5 Nm in flexion/extension was performed.
AoR and CoR were defined with respect to the pelvis, that is, considering the iliac side of the SIJ as not moving; the displacements of the sacrum with respect to the pelvis were then used to calculate the orientation of these axes. The global anatomical axes were considered as reference in all calculations. The AoR was defined as a line drawn in the frontal plane of the sacrum that connected the 2 most distal points on the left and right sides at which the minimum displacements were found, while the CoR was defined as a point in the sagittal plane of the sacrum at which the minimum displacement was detected.
Results
Validation
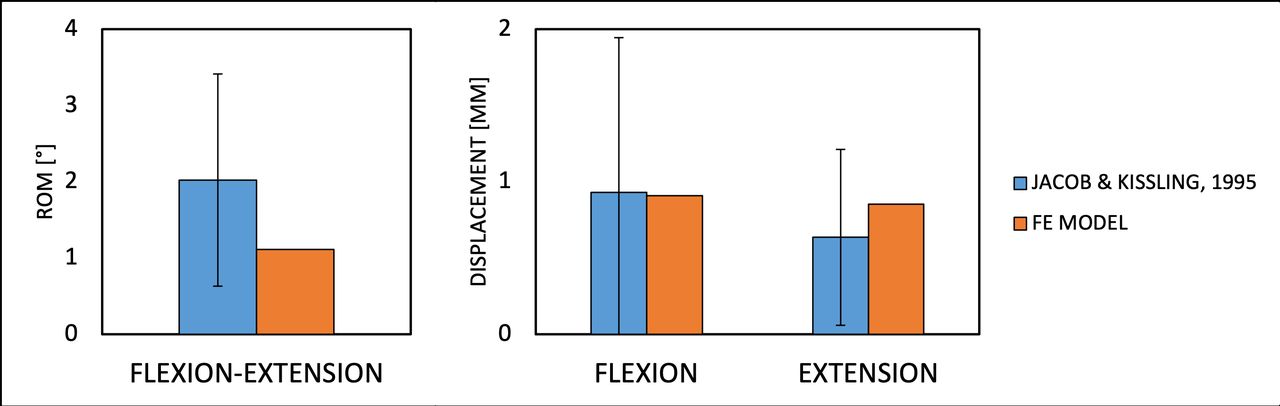
The ranges of motion calculated for the intact model in the 3 loading conditions were inside the ranges of experimental measurements conducted on cadaver specimens (Table 3).31,32 The range of motion of the SIJ in flexion-extension was within the SDs of the values found in an in vivo study7 (Figure 2). Moreover, the maximum displacements of the sacrum in both extension (0.8°) and flexion (0.9°) were very similar to the values reported in the same article (0.6° for extension and 0.9° for flexion).7 According to these comparisons, the validation of this model is supported by this in vivo study (Figure 2).
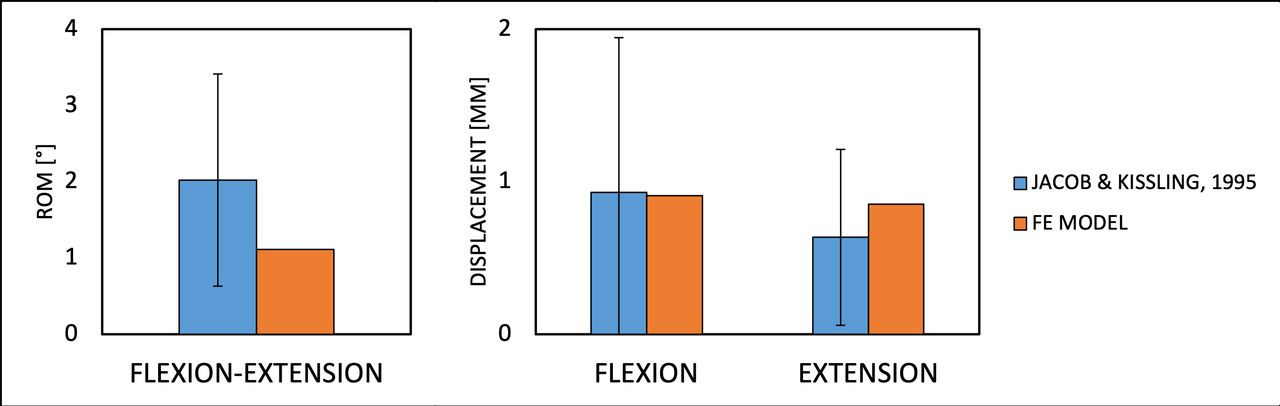
Predicted ranges of motion (ROM) of the sacroiliac joint of the intact model in flexion-extension (left) and displacements of the sacrum in flexion and extension (right), as compared with data from in vitro experiments.7
Ranges of motion (in °) of the intact model, compared with data from experimental studies available in the literature and obtained under the same loading conditions. SDs of the literature data are reported in parentheses.
AoR and CoR of the Intact Model
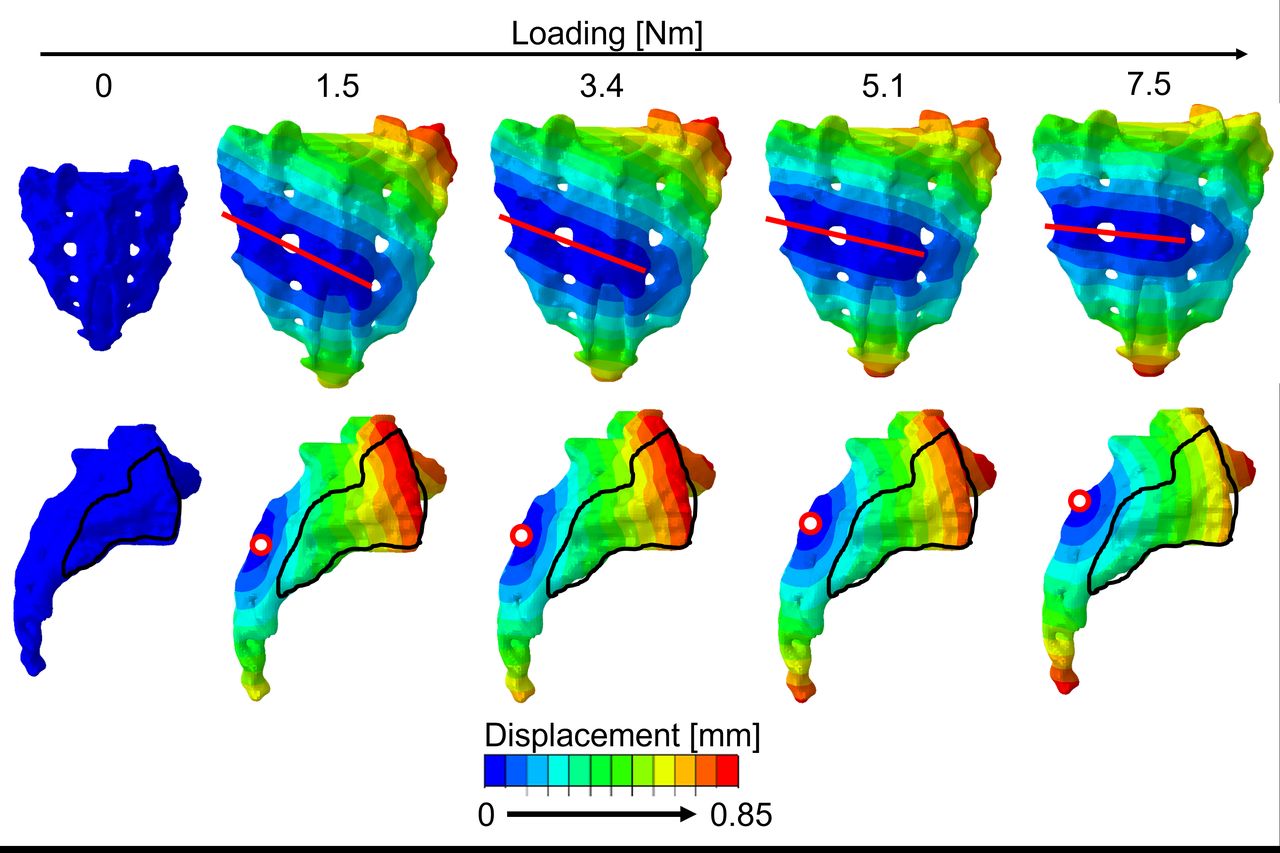
Following the application of a 1.5-Nm moment in extension, the AoR showed that the main rotation of the sacrum with respect to the pelvis was in flexion-extension. Nevertheless, small rotations in lateral bending and axial rotations were also observed. The CoR showed that the sacrum rotated around a point away from the SIJ (Figure 3), approximately in the middle of the sacral crest. At the next step (3.4 Nm), the AoR and the CoR showed minor differences with respect to the previous step. By increasing the moment applied to the model, the movement of the AoR showed that the coupled rotation of the sacrum in lateral bending and axial rotation decreased while the primary rotation in flexion-extension increased as expected. The CoR moved slightly following the increase from 1.5 to 3.4 Nm.
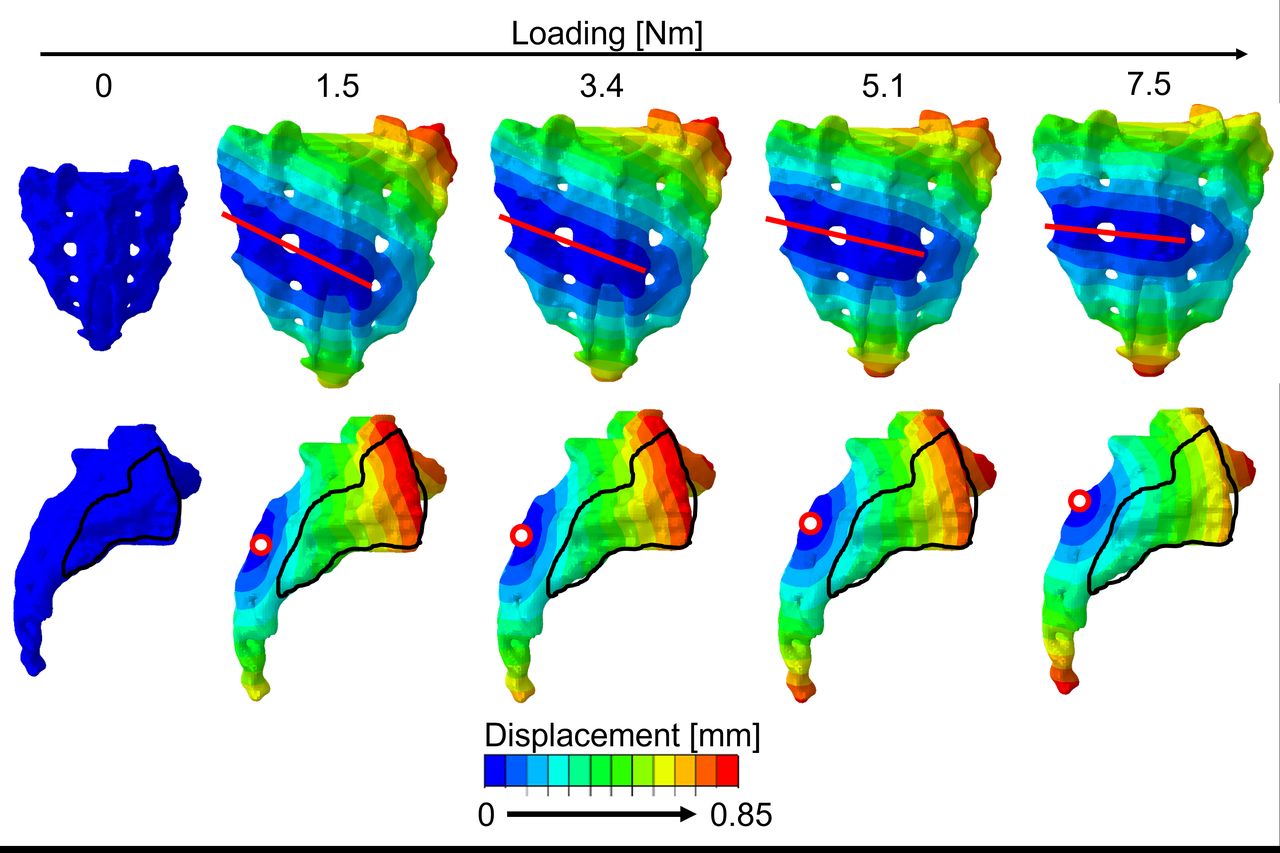
Qualitative axis of rotation (line drawn) in the frontal plane of the sacrum and center of rotation (point) in the sagittal plane of the sacrum for 5 loading values (0, 1.5, 3.4, 5.1, 7.5 Nm) in extension for the intact model.
After the application of a 1.5-Nm moment in flexion, the position of the AoR showed that the primary rotation of the sacrum was again in flexion-extension and the CoR, like in the extension case, was located outside of the SIJ (Figure 4). With a moment of 3.4 Nm, the AoR and the CoR maintained the same direction and position with respect to the previous step. Increasing the moment in the model affected neither the AoR nor the CoR.
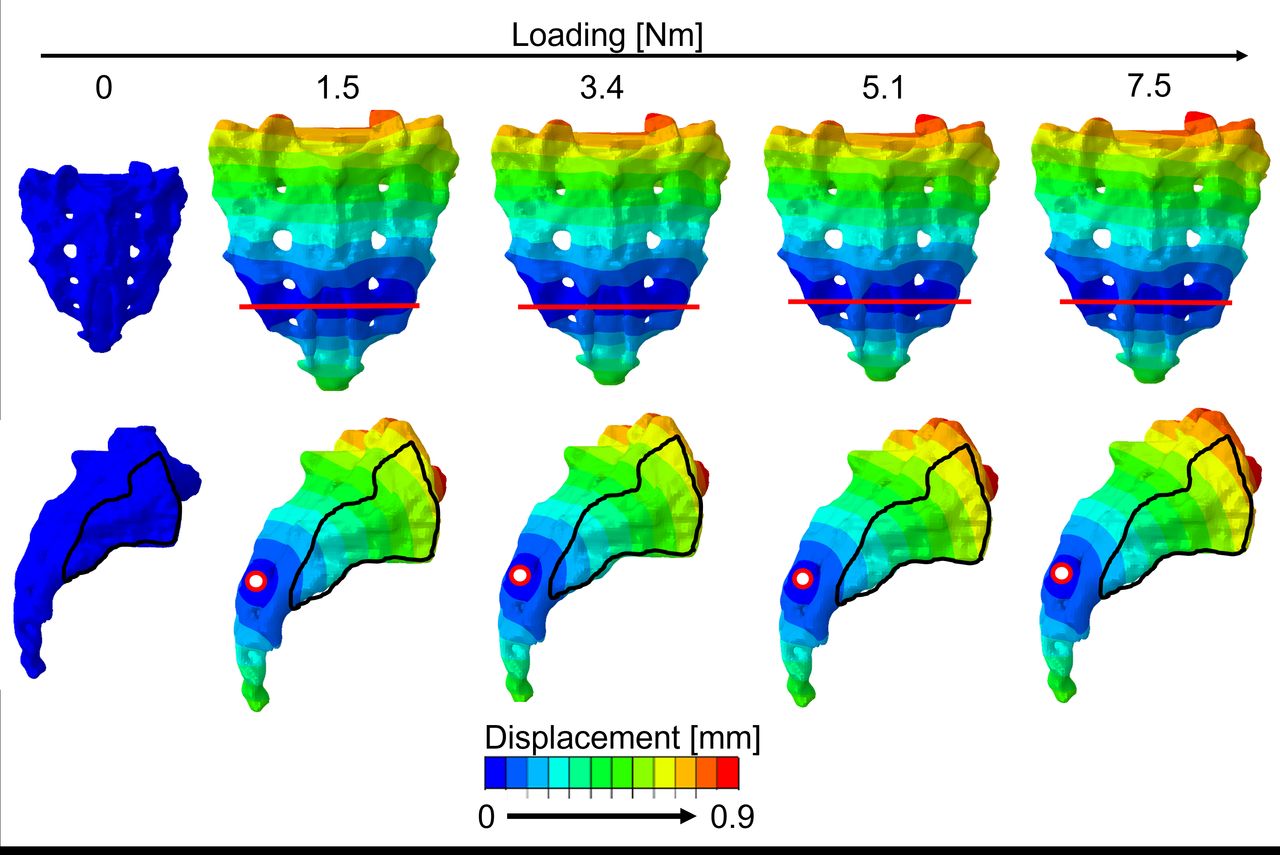
Qualitative axis of rotation (line drawn) in the frontal plane of the sacrum and center of rotation (point) in the sagittal plane of the sacrum for 5 loading values (0, 1.5, 3.4, 5.1, 7.5 Nm) in flexion for the intact model.
AoR and CoR of the Instrumented Models
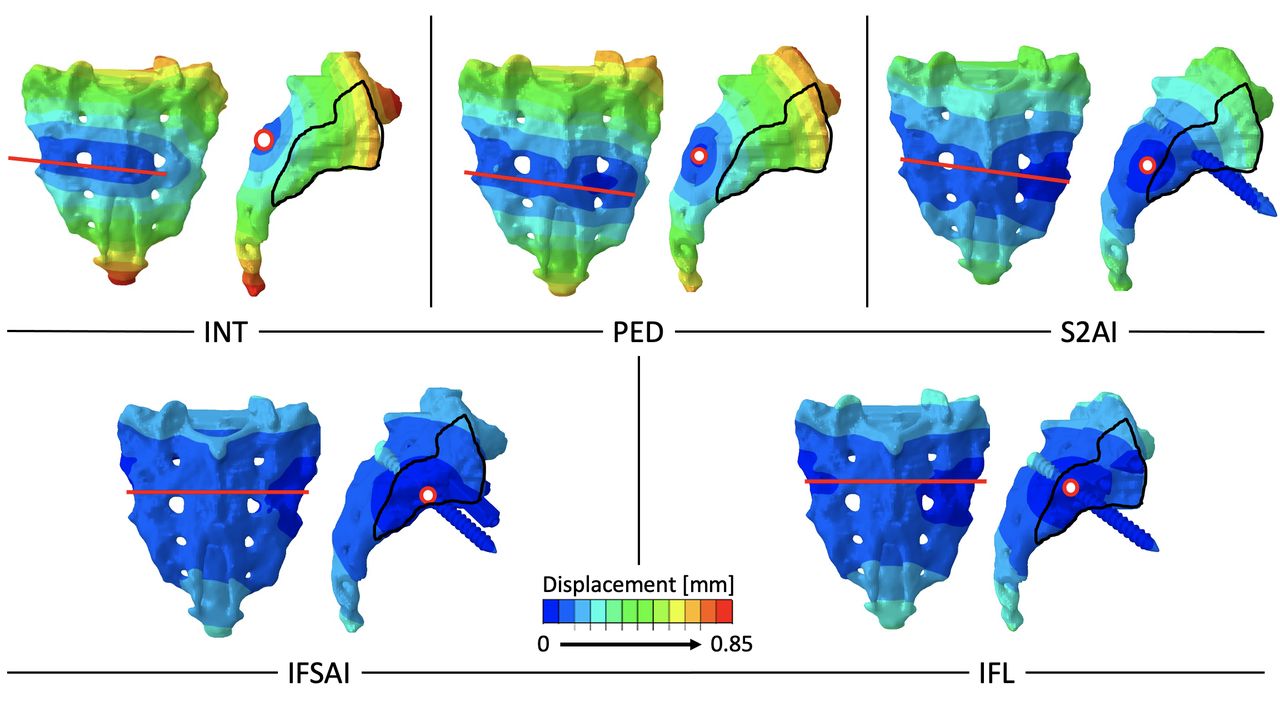
In extension, adding pedicle screws (PED) resulted in a similar AoR and a CoR location closer to the SIJ with respect to the intact model (Figure 5), while in flexion the implantation of the screws resulted in only marginal differences in AoR and CoR (Figure 6).

Qualitative axis of rotation (line drawn) in the frontal plane of the sacrum and center of rotation (point) in the sagittal plane of the sacrum for the 5 configurations: intact (INT), pedicle screws (PED), S2 alar-iliac screws (S2AI), bilateral S2AI and triangular implants inserted bilaterally in a sacral alar-iliac trajectory (IFSAI), bilateral S2AI and 2 bilateral triangular implants inserted in a lateral trajectory(IFL) in extension for the last step (7.5 Nm).

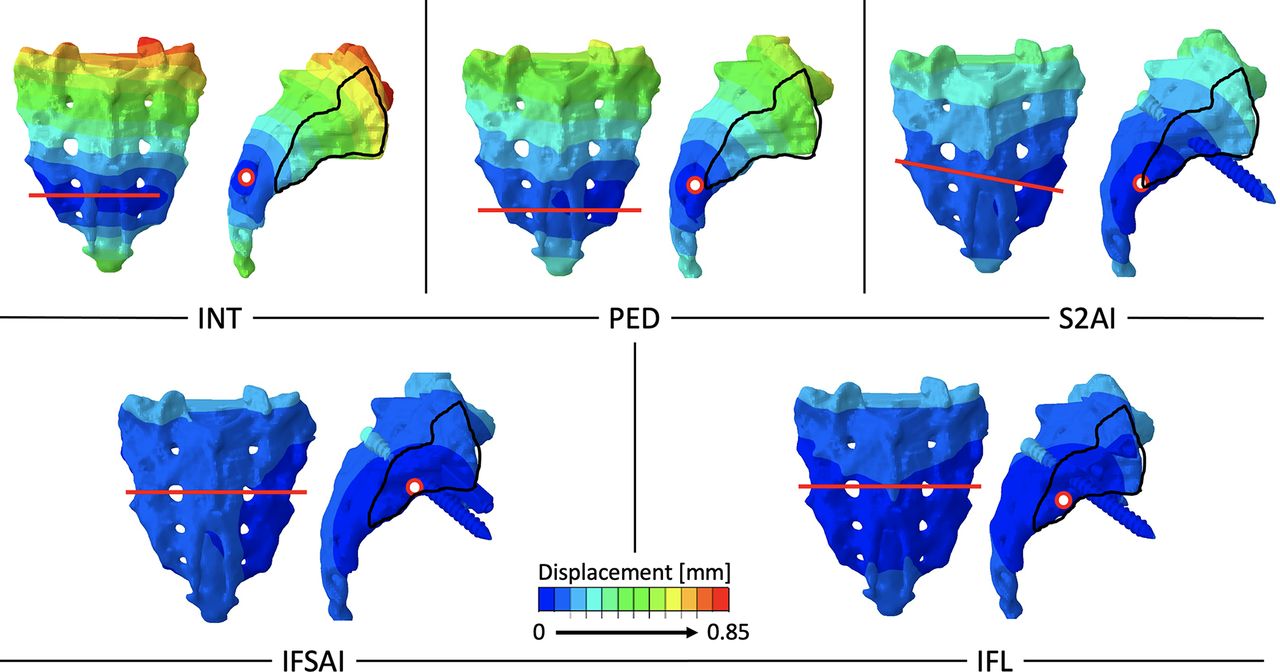
Qualitative axis of rotation (line drawn) in the frontal plane of the sacrum and center of rotation (point) in the sagittal plane of the sacrum for the 5 configurations: intact (INT), pedicle screws (PED), S2 alar-iliac screws (S2AI),bilateral S2AI and triangular implants inserted bilaterally in a sacral alar-iliac trajectory (IFSAI), bilateral S2AI and 2 bilateral triangular implants inserted in a lateral trajectory (IFL) in flexion for the last step (7.5 Nm).
With the S2AI, the magnitude of the rotation of the sacrum in lateral bending and axial rotation decreased with respect to PED; nevertheless, the AoR was almost horizontal meaning that the rotation of the sacrum was mainly in flexion-extension. The CoR was located on the border of the SIJ (Figure 5). In flexion, the rotation of the sacrum decreased with respect to PED, but the coupled rotation in lateral bending and axial rotation increased. The CoR was located inferiorly with respect to the SIJ (Figure 6).
When triangular titanium implants were simulated in addition to S2AI, the motion of the SIJ decreased further. Both cases, IFSAI and IFL, showed that the AoR passed through the SIJ, and the CoR was found within the SIJ. Minimal differences were found between these 2 configurations in extension and flexion. Despite this, the CoR in extension was very near to the center of the SIJ for the IFSAI configuration, while it was on the border between the SIJ and the sacrum for the IFL configuration. Similarly, in flexion, IFSAI resulted in a CoR location near to the center of SIJ with respect to IFL (Figure 5, Figure 6).
Discussion
This study investigated the biomechanical behavior of the SIJ, specifically the effect on AoR and CoR, following the application of incremental loads. Additionally, the AoR and CoR were qualitatively compared among intact and instrumented configurations.
First, the comparison among loading steps for the intact model showed that increasing the load intensity led to an increase of the rotation of the sacrum in the direction of the loading for both extension and flexion but did not markedly change the CoR of the SIJ. While it was not influenced by the load intensity, the position of the SIJ’s CoR was impacted by the addition of fixation implants in the sacrum.
The results of the comparison among the instrumented models following the application of 7.5 Nm in extension showed that all the considered sacropelvic fixation techniques were effective in reducing the rotation of the sacrum and stabilized the SIJ, in particular for those configurations involving triangular implants. In fact, the CoR fell inside the SIJ or on its border following sacropelvic instrumentation via triangular implants.
In extension, the AoR for the configurations with the triangular implants showed a more stable rotation of the SIJ in flexion-extension, that is, a pure rotation with a minimal translational component, in comparison with S2AI fixation. The CoR for the configurations with the triangular implants was nearer to the center of the SIJ, especially for IFSAI (where 2 implants were inserted near to each other).
In flexion, the AoR of the SIJ had approximately the same behavior as the extension case. The sagittal view showed that S2AI was not sufficient to move the CoR inside the SIJ, while adding triangular implants (IFSAI and IFL) resulted in the CoR residing in the joint boundary.
Since the comparison of AoR and CoR of the SIJ in configurations including the triangular implants is reported here for the first time, only a comparison with studies in which other sacropelvic fixation implants were used was possible. In their computational study, Bruna-Rosso and colleagues simulated 6 sacropelvic fixation scenarios with 1 or 2 screws placed in a posterolateral trajectory on 1 side. Implants were placed in 2 different trajectories under compression loads in order to evaluate the SIJ mobility in terms of displacement (rotation and translation).33 They found that SIJ fixation devices were able to reduce the motion, mainly rotational, between sacrum and ilium, and found sacroiliac displacement patterns similar to that described in the present study. They also found that the simulations of the configurations with 2 implants showed no significant improvement of the stabilization as compared with equivalent configurations with 1 implant and attributed this result to the location of the second implant located near the SIJ AoR. The authors noted that “the implants located away from the SIJ AoR showed a better capability to reduce the SIJ motion.”33 In agreement with this finding, when the triangular titanium implant was inserted away from the SIJ AoR (IFSAI and IFL) in the present study, a further reduction of the SIJ motion was noted. This issue may be further explored in future studies in which comparisons between S2AI and iliac screws, and between IFL and a configuration with only 1 laterally placed triangular titanium implant, are performed.
In a previous study, the same 5 configurations were compared in terms of residual flexibility, stresses in the instrumentation, and bone-implant interaction. The results obtained in the study confirmed that IFSAI resulted in the highest reduction in SIJ motion, which was in agreement with the previous work.27
As per the findings of this study, the construct becomes more rigid as additional sacropelvic fixation is added with the least amount of motion observed for IFSAI and IFL. These results demonstrate that at least 2 implants across the SIJ facilitate its stabilization. Clinically, added stabilization suggests a decreased risk of secondary SIJ pain following implementation of a long construct. While the exact origin of SIJ pain is not fully understood, it has been suggested that nociceptive receptors in periarticular structures of the SIJ may contribute to some of the pain.34 In particular, Szadek et al identified the anterior capsular ligament and interosseous ligament as potential sites of nociceptive fibers. In the current study, these same locations had reduced motions as the CoR moved closer to the center of the SIJ with increasing fixation. Another clinical interpretation of this data may suggest the potential for better bone bridging across the SIJ as oblique motion is eliminated, represented by the more horizontal AoR in configurations with increasing fixation. In vivo studies would be needed to demonstrate whether these interpretations are clinically significant.
The finite element models presented in this study have the same limitations reported in our previous study in which flexibility and stresses were compared.27 In brief, the models include several simplifications in the intervertebral discs and facet joints; nevertheless, the rotation and displacements of the intact sacrum in the current study were validated against the literature, specifically Jacob et al’s work.7 Additional simplifications included simulating the posterior rods as beam elements and representing tulips via kinematic constraints. Also, only the intact model has been validated, due to the lack of experimental and in vivo studies directly comparable with the present findings. Similar approaches, however, are commonly accepted and widely employed in the available literature.35–37 Finally, a simplified loading scenario (consisting of pure moments) was used; this approach was the same as that adopted in a number of previous studies.27,38–40 These loading conditions induce values of flexibility in the sacrum similar to those measured in vivo.7
Conclusion
In conclusion, this finite element study highlighted that increasing load intensity increases the rotation of the sacrum in the direction of the loading but does not affect the CoR. Moreover, this study suggests that sacropelvic fixation in combination with long thoracolumbar instrumentation increases the stability of the SIJ by decreasing its rotation. Supplementing S2AI screws with triangular implants located away from the SIJ AoR may, from a biomechanical point of view, provide additional stability to the SIJ; however, this conclusion should be confirmed by clinical studies.
Footnotes
Funding The study was funded by SI-BONE, Inc, and partially supported by the Italian Ministry of Health (“Ricerca Corrente”).
Declaration of Conflicting Interests D.P.L. is an employee of SI-BONE, has stock options/stock in SI-BONE, and has pending patents EP3782586, JP2021180928, and US20220117640 and granted patents EP3193752, JP6542362, JP6932741, US9662157, US10194962, and US11071573. S.A.Y. is an employee of SI-BONE, has stock options/stock in SI-BONE and has pending patents EP3782586, JP2021180928, and US20220117640 and granted patents EP3193752, JP6542362, JP6932741, US9662157, US10194962, and US11071573. R.D.C. is an employee of SI-BONE and has stock options/stock in SI-BONE. D.W.P. is a paid consultant of SI-BONE and royalties’ bearer.
Authors’ Contributions Conception and design: R.D.C., D.P.L., S.A.Y, M.B.B., F.G; Acquisition and data: M.P., R.D.C., D.P.L., T.M.T.V., F.G; Analysis and interpretation of data: M.P., R.D.C., D.P.L., S.A.Y, D.W.P., M.B.B., T.M.T.V., F.G.; Drafting of the manuscript: M.P., R.D.C., F.G.; Critical revision of the manuscript for important intellectual content and approval of the submitted and final version : M.P., R.D.C., D.P.L., S.A.Y, D.W.P., M.B.B., T.M.T.V., F.G.
Availability of Data and Material All data are available from the corresponding author upon reasonable request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.