


Abstract
Background Pedicle screw loosening is a complication of spinal instrumentation in osteoporotic patients. Dual-energy x-ray absorptiometry scans are not able to detect variations in bone mineral density (BMD) within specific regions of vertebrae. The purpose of this study was to investigate whether spine T scores correlate with cortical and cancellous BMD of pedicles and other 6 anatomical regions of lumbar spine.
Methods Eleven cadaveric spines with a mean age of 73 years were digitally isolated by applying filters for cortical and cancellous bone on computed tomography images. Eleven L5 vertebrae were separated into 7 anatomical regions of interest using 3-dimensional software modeling. Hounsfield units (HU) were determined for each region and converted to cortical and cancellous BMD with calibration phantoms of known BMD. Correlations between T scores and HU values were calculated using Pearson correlation coefficient.
Results Mean vertebral T score was 0.15. Cortical BMD of pedicles was strongly correlated with T score (R 2 = 0.74). There was moderate correlation between T score and cortical BMD of lamina, inferior articular process (IAP), superior articular process (SAP), spinous process, and vertebral body. There was weak correlation between T score and cortical BMD of transverse process (R 2 = 0.16). Cancellous BMD of vertebral body was strongly correlated with T score (R 2 = 0.82). There was moderate correlation between T score and cancellous BMD of pedicles, spinous process, and transverse process. There was weak correlation between T scores and cancellous BMD of lamina, IAP, and SAP.
Conclusions There is a strong correlation between T scores and cortical BMD of lumbar pedicle. There is strong correlation between T scores and cancellous BMD of vertebral body. Cortical and cancellous BMD of transverse process and lamina were weakly correlated with T score and less affected by osteoporosis.
Clinical Relevance Patients with osteoporosis may especially benefit from the development of extrapedicular fusion strategies due to the relatively higher bone density of these fixation sites.
- regional densitometry
- spinal fixation
- fixation strength
- spine construct failure
- spine DEXA score
- spine BMD
Introduction
Low bone mineral density (BMD) is a major risk factor for spine construct failure such as pedicle screw loosening and pullout.1 Furthermore, osteoporosis is becoming more common among patients requiring spine surgery.2 Reported rates of construct failure among patients with osteoporosis undergoing pedicle screw fixation are as high as 10.3%.3
Several adjunctive techniques have been devised to help reduce the risk of spinal construct failure in patients with low BMD, including cement augmentation, expandable pedicle screws, undertapping the screws, and increasing the number of fixation points.4,5 Screw fixation strength relies greatly on BMD,1 yet pedicle screw fixation is currently the preferred method of posterior fixation in the lumbar spine. Extrapedicular regions of the vertebrae possess greater bone density and may be better options for fixation.6–9 Mai et al compared the BMD of the fixation points between traditional pedicle screws and lumbar cortical screws. The authors found that the bone density of the cortical screw trajectory was significantly higher. Interestingly, the difference in bone density between the 2 trajectories was greater for patients with osteoporosis than for those without osteoporosis. Hohn et al and Rosinski et al both reported that the laminae and inferior articular processes (IAPs) of the lumbar spine have significantly higher BMD than the pedicles and other vertebral regions.
The goal of this study was to measure and compare the bone quality of the lumbar spine in cadavers with varying degrees of osteoporosis and to analyze the effect of osteoporosis on the bone quality of several anatomical regions. We investigated the bone quality of these regions by assessing 7 different anatomical regions of the lumbar spine using computed tomography (CT) imaging and 3-dimensional software modeling. We selectively compared the cortical BMD, cortical volume, cancellous BMD, cancellous volume, and total volume for each anatomical region. Our hypothesis was that bone quality in the regions nearest to the vertebral body would strongly correlate with osteoporosis.
Methods
Using CT images, 11 cadaveric L5 vertebrae (mean age of 73 years) were digitally isolated by applying filters for cortical and cancellous bone. Dual-energy x-ray absorptiometry (DEXA) scans of the lumbar spine were obtained for each specimen to determine the T scores. In addition, high-resolution helical CT images were performed on each specimen. The L5 vertebrae were chosen because of their widespread use in Hounsfield unit (HU) measurement on computer tomography to diagnose osteoporosis. All scans were performed using the same scanner (GE Lightspeed VCT) with the same imaging parameters (64 slices, 512 × 512 pixel resolution) to reduce interspecimen variability. Using 3-dimensional software modeling (Mimics; Materialise, Leuven, Belgium), each L5 vertebra was segmented into 7 predefined anatomical regions including the superior articular process (SAP), IAP, lamina, pedicle, spinous process, transverse process, and vertebral body. When visible, suture lines were utilized as anatomic boundaries between vertebral regions. The same team member segmented each vertebral region to reduce interobserver variability. This team member segmented the L1-L5 transverse processes, pedicles, IAPs, and SAPs twice from 2 of the study specimens to assess the inherent variability in the manual segmentation protocol. A previous study using this method of segmentation produced an average difference in BMD of 1.5% between the first and second measurements of the same anatomical region (SD ±0.7%).7 The largest discrepancy between the repeated measures was 3.0%.
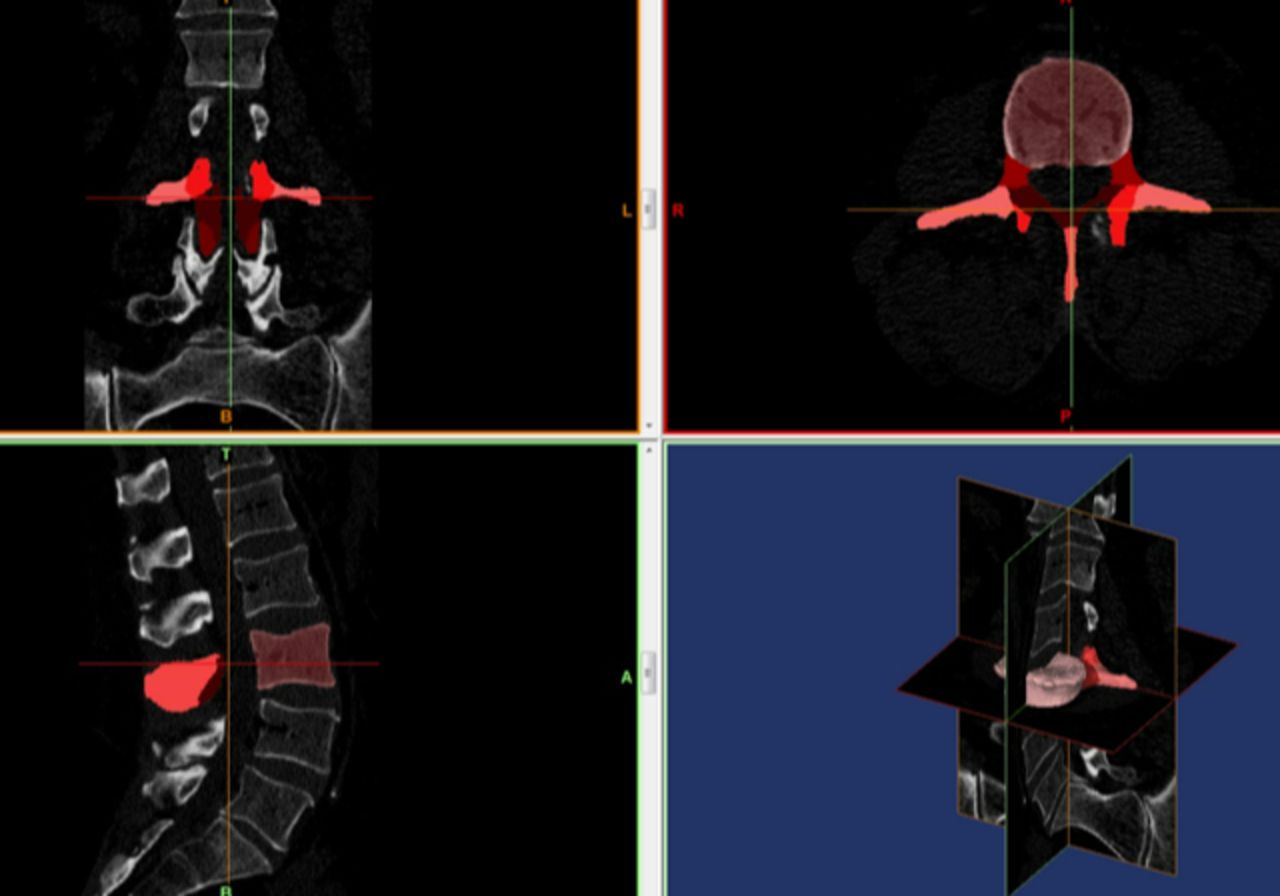
Cortical and cancellous bones were separated using a filter algorithm provided by the segmentation software. The filter for cancellous bone included pixels with HUs between 200 and 450. For cortical bone, the filter included pixels between 450 and 1400 HU. Average total, cortical, and cancellous BMD measurements of each anatomical region of the L5 vertebrae were recorded. The cortical bone, cancellous bone, and nonbone volumes were also assessed (Figure 1). The nonbone volume reflects the porosity of the anatomical regions.
Images depicting the data collection process, including the conversion of computed tomography (CT) images to engineering solid models. The 2-dimensional images are segmented from a series of CT images to define volumes. Each vertebra was divided into 7 regions followed by further segmentation of cancellous and cortical bone within each anatomic volume. Cortical and cancellous bone were separated by a filter algorithm provided by the segmentation software.
Conversion from HU to BMD units (mg/cm3) was performed using previously described guidelines.8,10 The average HUs were determined for each region and converted to cortical and cancellous BMD with calibration phantoms of known BMD. In brief, HUs were converted to BMD through a calibration equation derived from CT images of tissue surrogate materials (Electron Density Phantom, Model 62; CIRS) using the same scanning protocol for all specimens. “Phantoms” of 200 and 800 mg/cm3 were utilized to account for the known range of BMD in various anatomic locations.8 These “phantom” blocks have been previously reported to produce reliable calibration formulas between HU and BMD and are not influenced by CT mode, slice thickness, reconstruction algorithm, or pitch factor.8,10 The results of a previous HU to BMD analysis produced a linear calibration relationship of 1 mg/mL for every 0.78 HU.7 Validation studies using this protocol report that the bone mineral content of vertebrae can be measured with an accuracy of 6% compared with the ash weight gold standard. Similar work by Cann et al found no significant differences between direct measurement of calcium ash and CT measurements of BMD in the thoracic vertebrae.11
Statistical Methods
The primary outcome measures from densitometry were mean total, cortical, and cancellous BMD for each anatomical region of the L5 vertebrae. The cortical, cancellous, and nonbone volumes were also measured for each anatomical region. Correlations between T scores and HU values were calculated using the Pearson correlation coefficient. While there is little consensus in the literature regarding cutoff points, we applied a conventional and widely used guideline for interpreting correlation coefficients (Table 1).12
Guideline for interpreting correlation coefficients.13
One-way analysis of variance was performed to identify any significant differences in the cortical volume and cortical thickness of the vertebral regions, with alpha equal to 0.05. All analyses were performed using JMP version 15.0 (SAS Institute, Cary, NC).
Results
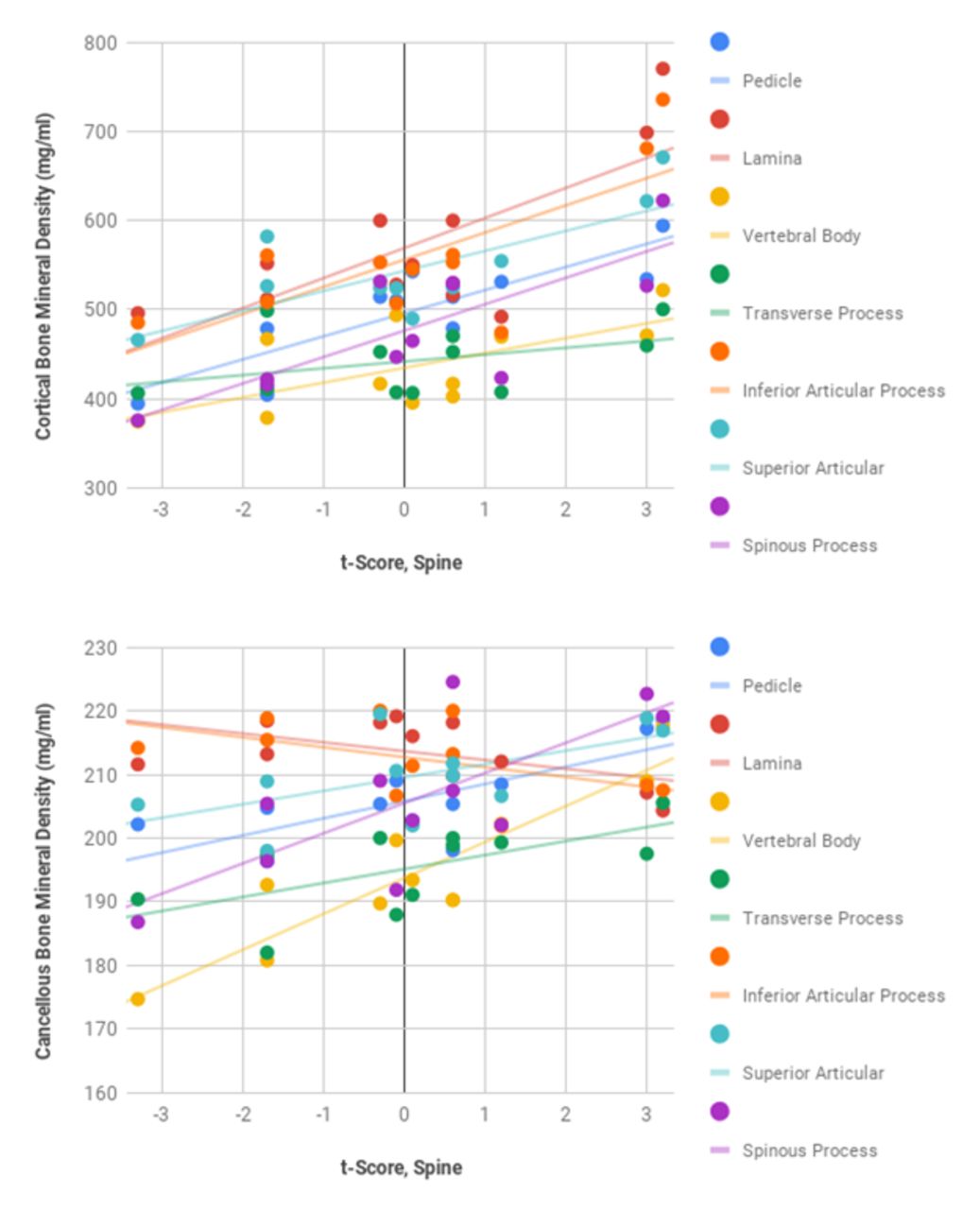
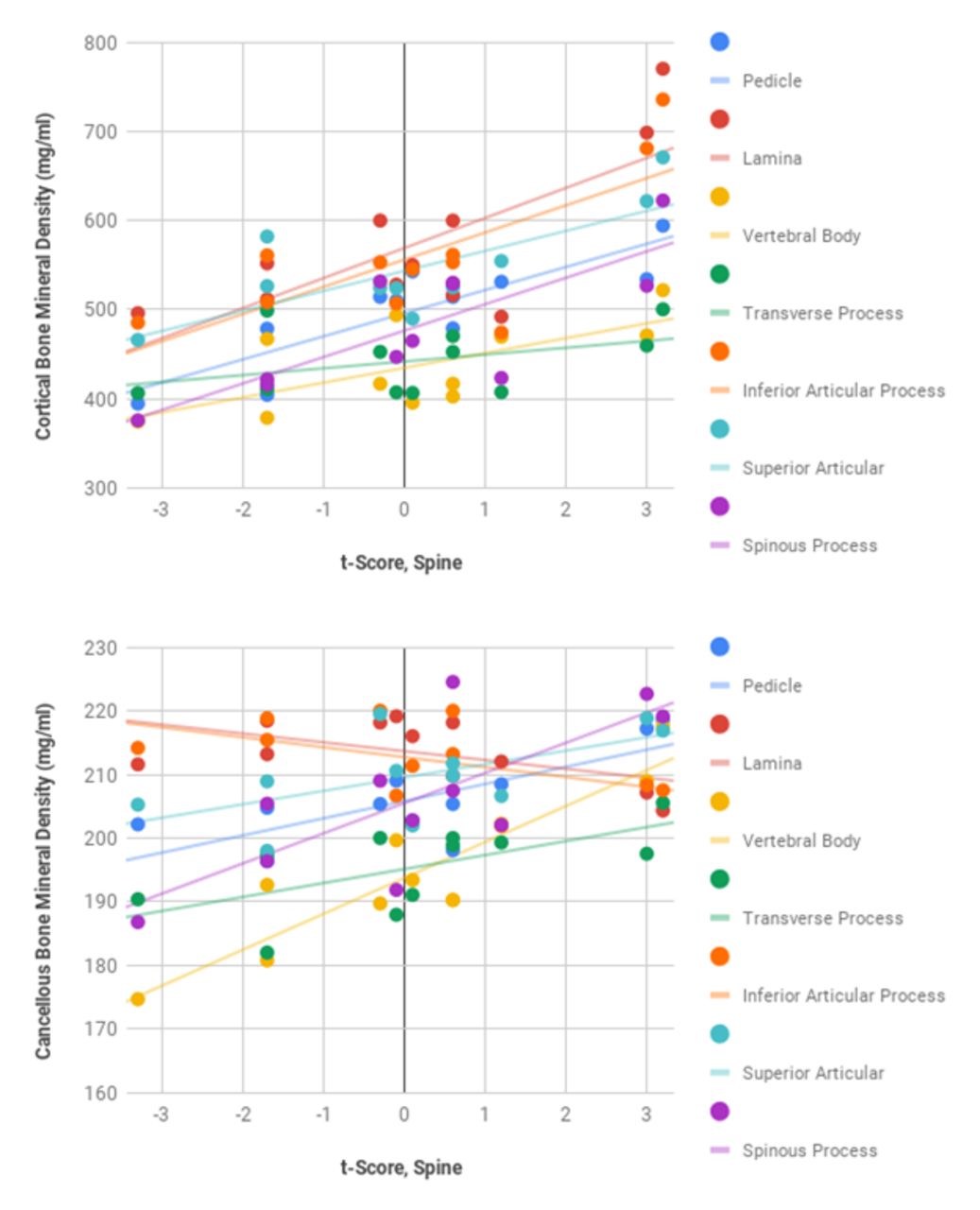
The mean T score was 0.15 and ranged from −3.3 to 3.2. The relationships between the lumbar spine T score and the BMD of each vertebral region of the L5 vertebrae are shown in Table 2 and Figure 2.
Pearson correlation coefficients demonstrating the relationship between dual-energy x-ray absorptiometry T scores and the BMD of cortical and cancellous bone for each of the 7 anatomical regions of the lumbar spine.

Scatter plots demonstrating the relationship between dual-energy x-ray absorptiometry T scores and bone mineral density of cortical and cancellous bone for each of the 7 anatomical regions of the lumbar spine.
Cortical BMD
The cortical BMD of the pedicles was strongly correlated with the T score (R 2 = 0.74, P < 0.05). Similarly, the cortical volume of the pedicles was also strongly correlated with the T score (R 2 = 0.77, P < 0.05). There was a moderate correlation between the T score and the cortical BMD of the lamina, IAP, SAP, spinous process, and vertebral body. On the other hand, there was a weak correlation between the T score and the cortical BMD of the transverse process (R 2 = 0.16, P = 0.22).
Cancellous BMD
The cancellous BMD of the vertebral body was strongly correlated with the T score (R 2 = 0.82, P < 0.05). There was a moderate correlation between the T score and the cancellous BMD of the pedicles, spinous process, and transverse process. There was a weak correlation between the T score and the cancellous BMD of the lamina, IAP, and SAP. Similarly, there was a negligible correlation between the T score and the cancellous volume of the lamina and IAP (R 2 = 0.09 and 0.05, respectively; P < 0.05 for each comparison). The cancellous volume of the SAP was moderately correlated with the T score (R 2 = 0.47, P < 0.05).
Discussion
In our study, the cancellous BMD of the vertebral bodies showed the strongest correlation with osteoporosis. Both the cortical and cancellous BMD of the transverse process and lamina were weakly correlated with T scores and therefore less affected by osteoporosis. Previous studies suggested that aging and degeneration of the spine result in the increased compressive load transmission through the posterior column.13,14 According to Wolff’s law, bones adapt their mass and architecture according to the magnitude and direction of the forces that are regularly applied to them.15 Similarly, reduced loading over time causes progressive bone loss. If Wolff’s law is applied to the degenerative lumbar spine, then an increased cortical volume percentage and thickness would be expected among the posterior elements.
While the previous investigations have found that the posterior elements had a significantly higher BMD compared with the anterior column of the spine, they did not report on how that is correlated with osteoporosis. In addition, any differences between the extrapedicular regions were unable to be detected since it required a more granular comparison between the regions. Because the cancellous bone is more affected by osteoporosis compared with the cortical bone,16 anatomical regions of the lumbar spine with a higher cortical-cancellous bone ratio may represent ideal sites for extrapedicular fixation in patients with osteoporosis. Previous studies suggest that regional alterations in the trabecular architecture influence the biomechanics of the vertebral body with little effect on the overall bone density.13,17 Therefore, it is possible that variations in the cortical-cancellous bone ratio also exist among the posterior elements despite their similarity in the average BMD as observed previously by Hohn et al. Prior studies suggest a relative strengthening of the posterior elements over time (particularly among elderly patients).15 One of the postulated mechanisms of the posterior column strengthening involves the relative shift of the axial force transmission posteriorly with aging. As degenerated lumbar discs lose several millimeters in height, the posterior elements of adjacent vertebrae move closer together so that they are able to transmit a greater proportion of compressive force acting on the spine.13,18,19 As a result, the vertebral bodies are likely to become stress-shielded by the posterior elements over time. Thus, it might be expected that the bone of the posterior spinal column adapts to this increase in stress through the development of sclerosis and increased cortical thickness.13
To our knowledge, this is the first study that specifically analyzed the regional densitometry of a lumbar spinal segment. In addition, our study used multiple measures of bone quality including cortical thickness and the cortical-cancellous bone ratio. As shown previously by Pollintine et al, specific anatomical regions within the spine may demonstrate differences in trabecular bone architecture without altering the overall BMD measured. We found that the cancellous BMD of the vertebral bodies and the cortical BMD of the pedicles have the strongest correlation with the reported T score. As part of the preoperative optimization of patients undergoing spinal instrumentation and especially adult spinal deformity correction, the diagnosis and treatment of osteoporosis are crucial in improving patient outcomes. Osteoporosis is a significant factor in the screw pullout, fusion rates, progression of the deformity, loss of correction, proximal and distal junctional failure, as well as suprajacent and subjacent compression fractures.
DEXA scans are a crude 2-dimensional measure of generalized bone quality. At times, a DEXA scan is an average of appendicular bone density taken from the hips, shoulders, wrists, and feet. In patients with significant spondylosis and spinal deformity, the spine is frequently excluded from the DEXA scan, since acquiring spine images may result in spuriously high T and Z scores due to the endplate and facet sclerosis. CT data including quantitative CT images have been shown to be a more accurate predictor of the volumetric bone density and potential fixation strength.20
Understanding the risk profile of each patient based on the level-specific and region-specific bone density data and designing an appropriate surgical strategy (which at times may include avoiding the surgery altogether) to minimize potential mechanical complications are critically important.
Future research on the regional bone quality in the lumbar spine may identify ideal anatomical sites for extrapedicular fixation. A greater understanding of the bone density may be useful when developing new fixation strategies to reduce the risk of screw loosening, hardware pullout, and construct failure. Screw loosening becomes an even bigger problem in longer constructs for deformity correction, especially at the cephalad (proximal junctional failure) and caudal (distal junctional failure) ends of the construct. Since osteoporosis is common among patients requiring spine surgery, several adjunctive techniques have been developed to help reduce the risk of fixation failure in patients with low BMD. Those techniques include cement augmentation and expandable pedicle screws.21 A common technique in long constructs for adult spinal deformity is to cement the upper instrumented vertebra screws.22 Nevertheless, osteoporosis remains a significant risk factor for the proximal junctional failure in the adult and especially in senile spinal deformity surgery.23
Limitations of our study include a limited sample size which may have underpowered the study to collect any subtle differences. The second limitation is that we have used CT images and image processing software to determine the bone density of 7 predefined anatomic regions of the lumbar spine. CT scanners do have a limited resolution and may not be as accurate as direct anatomical measurements. The third limitation is that our study was limited to the analysis of the L5 vertebrae only. While this may help in predicting the bone quality at the distal end of the construct, further studies of the upper lumbar vertebrae, thoracolumbar junction, and thoracic vertebrae may improve our understanding of the proximal junctional pathology. Last, no analysis was done to detect if our specimens had any underlying spinal pathology. Further studies could compare the specimens with known various spinal pathologies to understand any changes in bone quality, and include biomechanical, stress, and pullout tests to determine how the implants would withstand simulated motions of the spine.
Conclusion
Patients with osteoporosis may especially benefit from the development of extrapedicular fusion strategies due to the relatively higher bone density of these fixation sites. The vertebral body may offer a compromised fixation in the osteoporotic patients due to the higher ratio of cancellous to cortical bone. Further clinical studies are necessary to determine whether these differences in bone quality support any alternative or augmented fixation methods.
Acknowledgments
The authors would like to thank Victor Ungurean Jr for their assistance with manuscript preparation.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Disclosures Dimitriy Kondrashov reports consulting fees from SI-Bone and Spineart and payment for expert testimony from Meridian and Exam Works.
Ethics Approval Institutional IRB approval was received prior to the initiation of the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data Availability Statement All of the raw data is available upon request.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.