


Abstract
Background Traumatic lumbosacral instability is a rare but potentially devastating injury. These injuries are frequently associated with neurologic injury and often result in long-term disability. Despite their severity, radiographic findings can be subtle, and multiple reports exist in which these injuries were not recognized on initial imaging. Transverse process fractures, high-energy mechanisms, and other injury features have been suggested as indications for advanced imaging, which has a high degree of sensitivity in detecting unstable injuries.
Case Presentation A 21-year-old man presented to our level I trauma center after being ejected in a rollover motor vehicle collision. He sustained multiple injuries, including multiple lumbar transverse process fractures and a unilateral superior articular facet fracture of S1.
Primary Outcomes Initial supine computed tomography (CT) images showed no displacement of the fracture and no listhesis or instability. Subsequent upright imaging in a brace, however, demonstrated significant displacement of the fracture with dislocation of the contralateral L5-S1 facet joint and significant anterolisthesis. The patient underwent open posterior reduction and stabilization of L4-S1 followed by L5-S1 anterior lumbar interbody fusion. The patient demonstrated excellent alignment on postoperative imaging. At 3 months postoperatively, he had returned to work, was ambulating without assistance, and reported minimal back discomfort and no lower extremity pain, numbness, or weakness.
Conclusion This case serves as a warning that supine CT imaging alone may not be sufficient to rule out unstable lumbar spine injuries, such as traumatic L5-S1 instability, and that upright radiographs in these potentially unstable injuries may represent a hazard to patients. Fractures involving the pedicle, pars, or facet joints as well as multiple transverse process fractures and/or a high-energy mechanism of injury should all raise suspicion of instability and warrant additional imaging.
Clinical Relevance This article provides guidance on approaching treatment for patients with potential traumatic lumbosacral instability.
Level of Evidence 5.
INTRODUCTION
Traumatic L5-S1 instability is a rare but well-documented injury. Since it was first described in 1940 by Watson-Jones,1 numerous cases have been reported in the literature. A recent systematic review of traumatic lumbar spondylolisthesis found 93 cases of L5-S1 disruption.2 This represented 74.4% of all reported cases of traumatic spondylolisthesis at any lumbar level. The higher frequency of traumatic instability at L5-S1 is believed to be due to the anatomy of the lumbosacral junction, which makes it more susceptible to the shear and hyperflexion forces thought to cause lumbosacral injuries.3
Traumatic lumbar/lumbosacral instability typically occurs via high-energy mechanisms, with 53% attributable to motor vehicle collisions.2 The rate of neurologic compromise is high, with 40% of patients presenting with nerve root deficits and 10.4% of patients presenting with cauda equina syndrome.2 For L5-S1 dislocations specifically, 1 report listed the rate of abnormal neurological findings as high as 68.4%.4 Due to the high rate of associated neurologic injuries, long-term follow-up suggests that many of these patients go on to develop chronic pain, sexual dysfunction, and urinary and bowel dysfunction.5
The majority of traumatic lumbar/lumbosacral instability (at all levels) occurs with concomitant fracture at the injured level: 26.4% with facet fracture, 8.0% with pars fracture, 10.4% with pedicle fracture, and 27.2% with a complex body fracture.2 In L5-S1 injuries, dislocation can occur through 1 or both facets with or without fracture. Vialle et al proposed a classification system based on the associated factors and reported a series of 11 patients in which 3 patients had no fracture (27.2%), 4 patients had unilateral facet fracture (36.4%), and 4 patients had bilateral facet fractures (36.4%).6
Traumatic instability at L5-S1 can occur with displacement anteriorly, posteriorly, or, in rare cases, laterally.7,8 Most cases of lumbosacral instability present with spondylolisthesis evident on initial imaging. However, perhaps due to the rarity of these injuries and the fact that radiographic findings can be subtle, there are several reports in which these injuries have been apparent, but not recognized, on initial imaging.3,4,9–11 In some cases, instability may not manifest immediately. In those cases, initial radiographs were unavailable or reported as normal, but over the course of weeks to months, increasing spondylolisthesis developed.12–15
Transverse process fractures have been proposed as sentinel fractures for this injury.3,10,16,17 Roche et al recommend reflexive computed tomographic (CT) imaging for patients with multiple lumbar transverse process fractures.17 However, because of the high incidence of isolated, stable transverse process fractures18 and many reports of lumbopelvic dislocation without transverse process fractures, transverse process fractures are somewhat limited in their usefulness as an indicator for lumbosacral instability.19,20
In modern times, the majority of high-energy trauma patients undergo supine CT imaging to assess the extent of their injuries before any other spine imaging is performed. Here, we present a case in which supine CT imaging failed to reveal the evidence of instability in a patient with traumatic L5-S1 instability. The following case was reported in accordance with case report guidelines.
CASE PRESENTATION
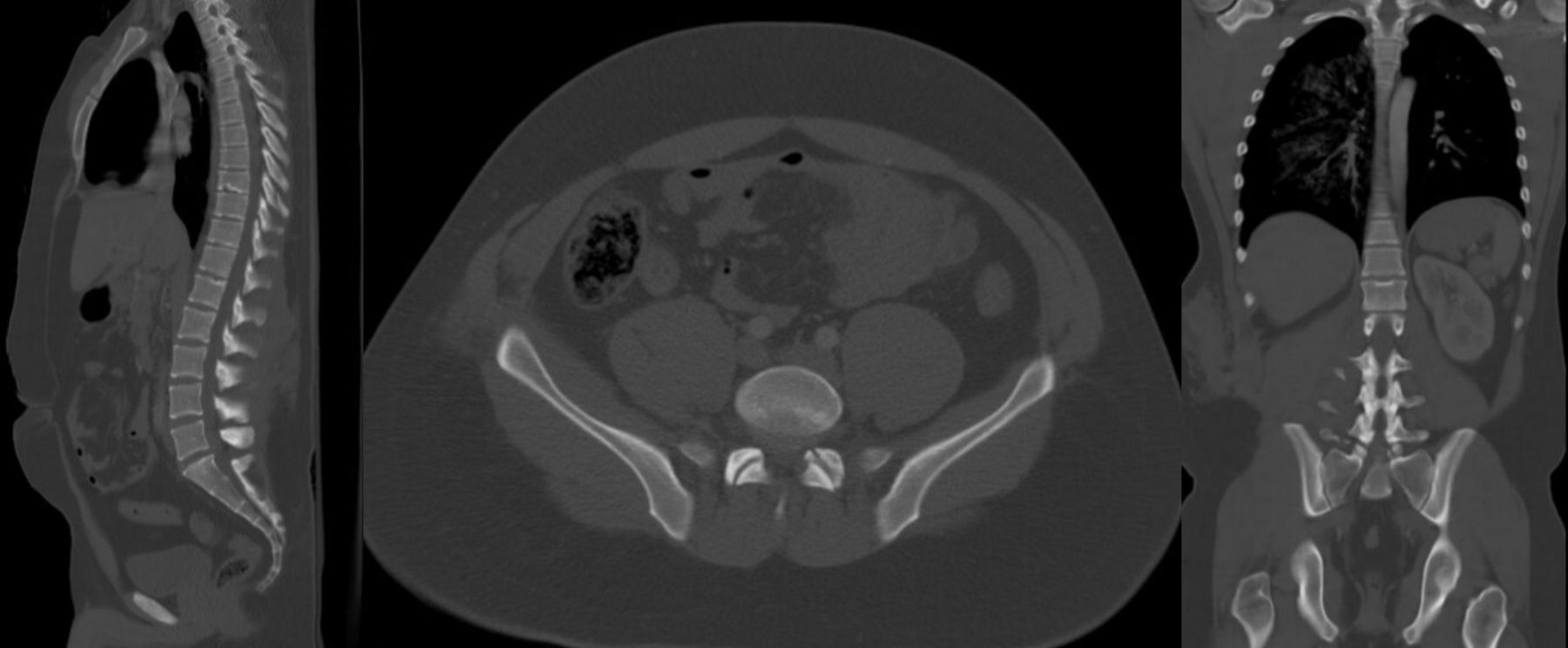
A 21-year-old man presented to our level I trauma center after a rollover motor vehicle collision in which he was ejected through the driver side window. He presented with multiple other injuries, including a right hemopneumothorax, multiple rib fractures, and a liver laceration. The spine surgery service was initially consulted for right-sided L1-L5 transverse process fractures, T8-T9 spinous process fractures, and a nondisplaced left S1 superior articular facet fracture identified on supine CT imaging. Initial CT imaging showed substantial soft tissue injury but did not reveal any evidence of spondylolisthesis or fracture displacement (Figure 1). The patient reported lower back pain and was found to be neurologically intact on examination. Given the absence of obvious instability, the decision was made to fit the patient with a brace and obtain upright plain radiographs.
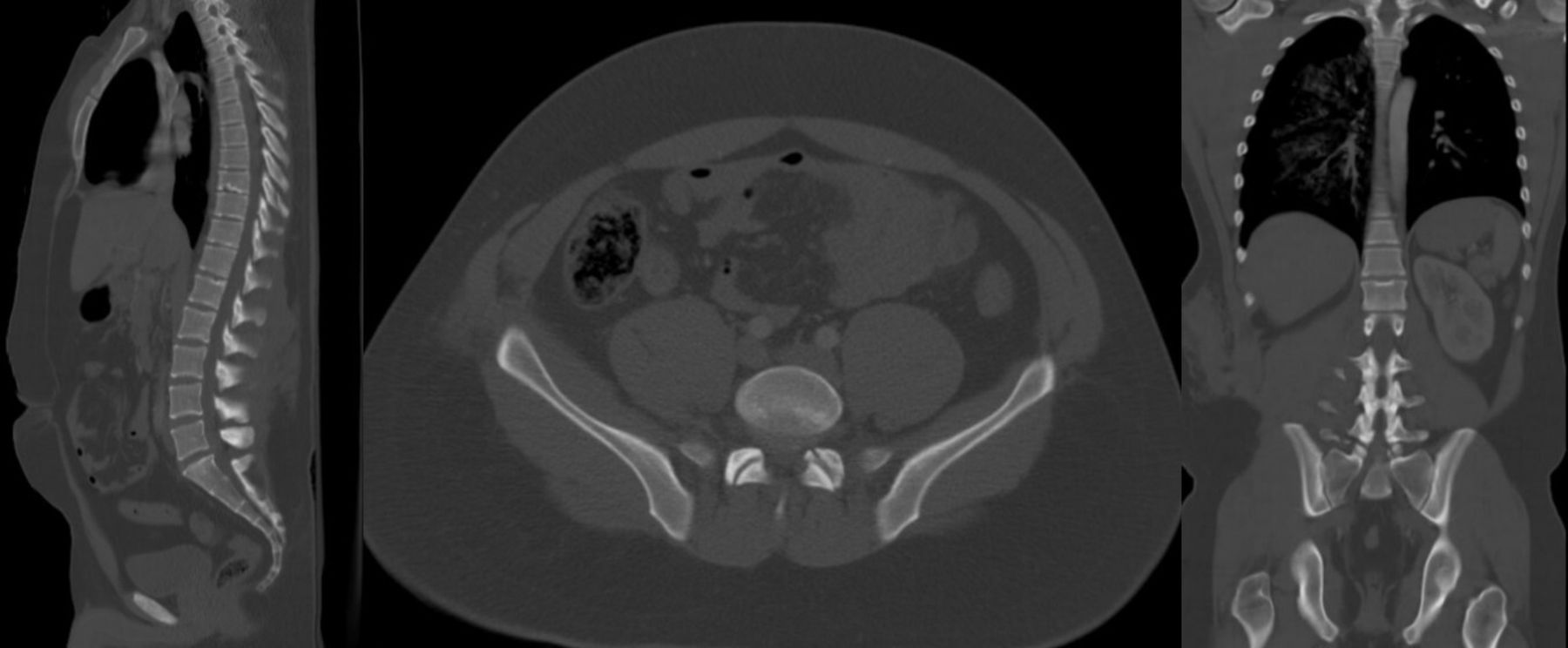
Initial computed tomography imaging.
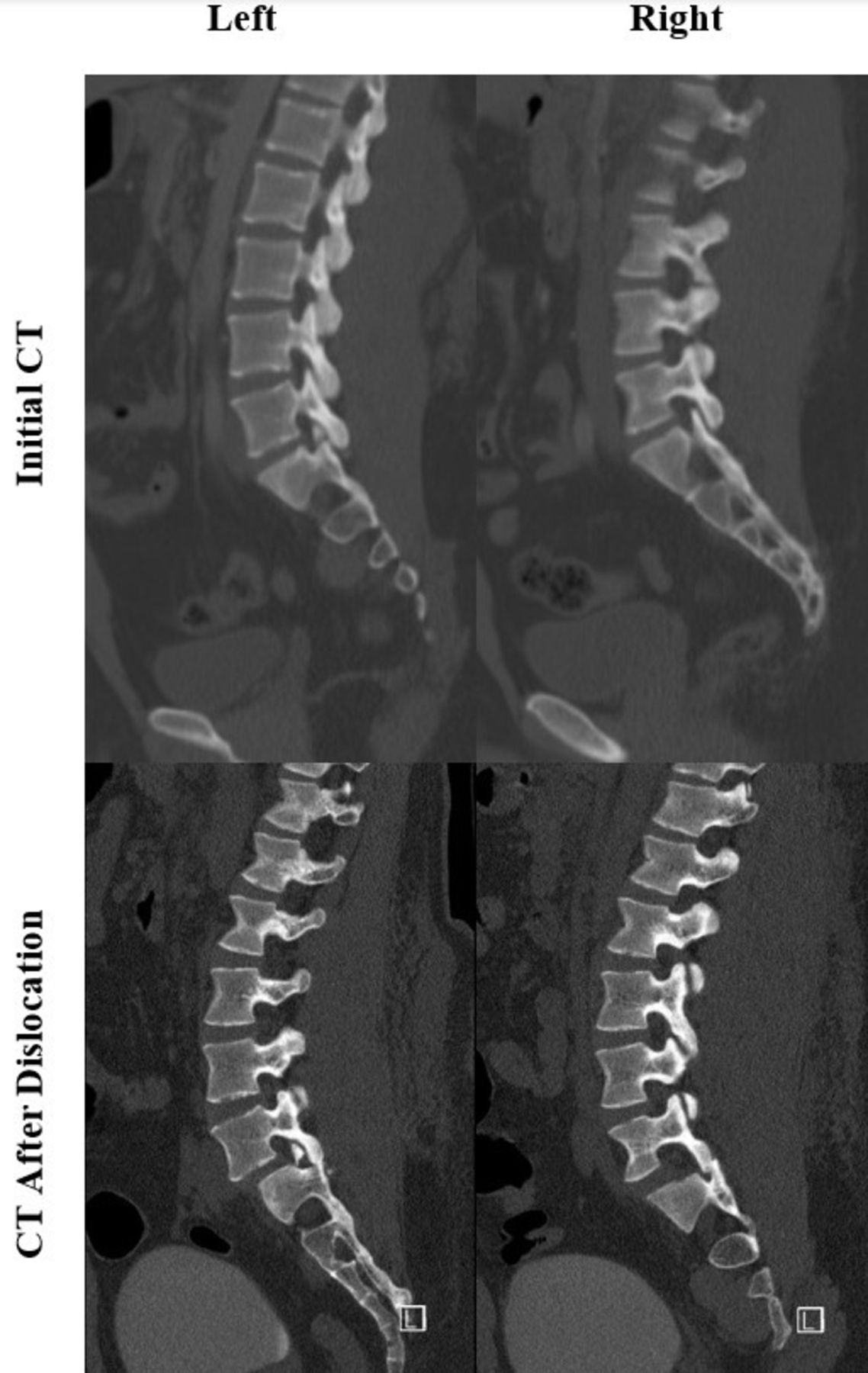
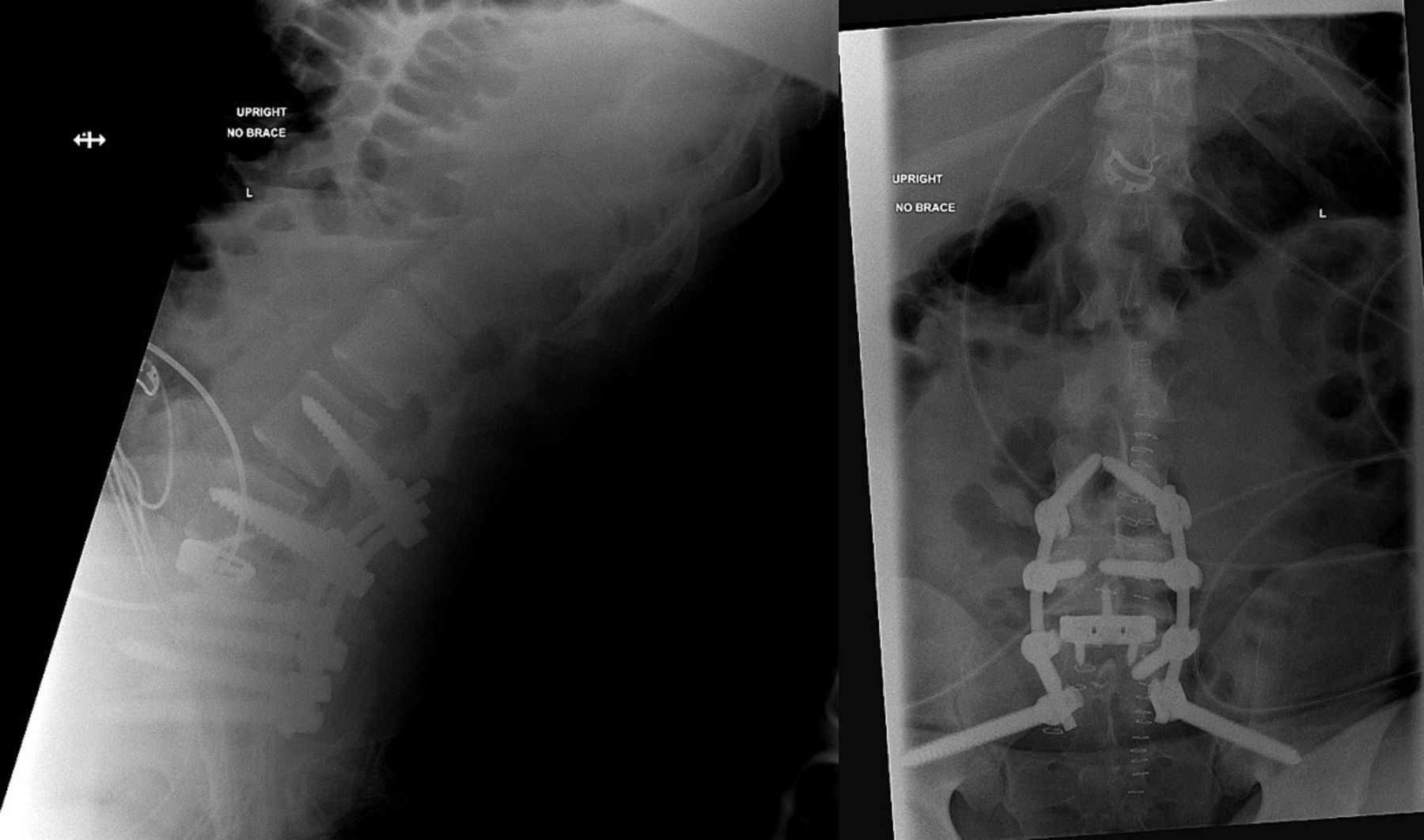
Upright radiographs of the lumbar spine (anterior-posterior/lateral view) revealed a new grade I anterolisthesis concerning for instability. The patient was immediately placed on full spine precautions and sent for repeat CT imaging which demonstrated displacement of the fracture with a dislocated L5-S1 facet joint on the contralateral side (Figures 2–4). The patient remained neurologically intact and was scheduled for urgent open posterior reduction and stabilization. Intraoperatively, we found significant soft tissue injury and marked instability at the L5-S1 level. Given the high degree of instability, we felt that L5-S1 anterior lumbar interbody fusion in addition to posterior stabilization and fusion was indicated to provide sufficient stability and surface area for fusion.

Upright imaging in Jewett brace showing L5-S1 dislocation.

Repeated computed tomography imaging demonstrating L5-S1 dislocation.

Sagittal computed tomography (CT) demonstrating the left S1 facet fracture and right facet before and after dislocation.
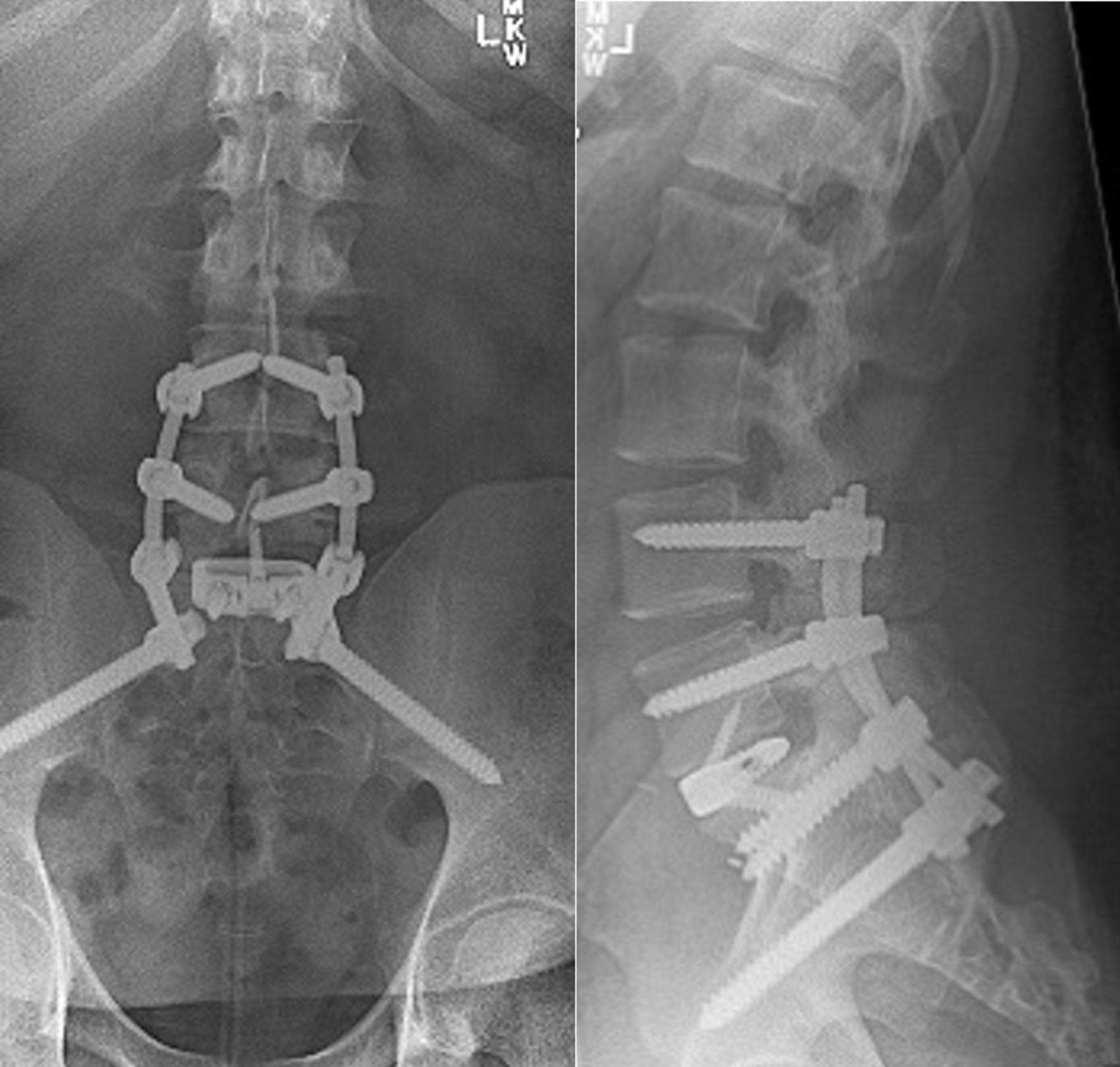
The patient tolerated both procedures well, and postoperative imaging showed excellent alignment (Figure 5). Ancef Q8H was administered postoperatively for 24 hours. The patient was discharged on hospital day 8, with instructions to ambulate with the assistance of a walker. Postoperative bracing was not recommended.

Postoperative plain radiographs.
At both 2-week and 6-week follow-up, the patient was following appropriate activity restrictions and ambulating multiple times per day with the assistance of a walker. At 6 weeks, the patient was instructed to discontinue walker use, and at 3 months, the patient was released to full activity and permitted to return to work (Supplemental Digital File). At 1-year follow-up, the patient reported minimal back discomfort and no lower extremity pain, numbness, or weakness. He also reported normal sexual function and urinary/bowel function. Plain radiographs revealed intact hardware and maintenance of anatomic lumbosacral alignment (Figure 6). There were no adverse or unanticipated events.
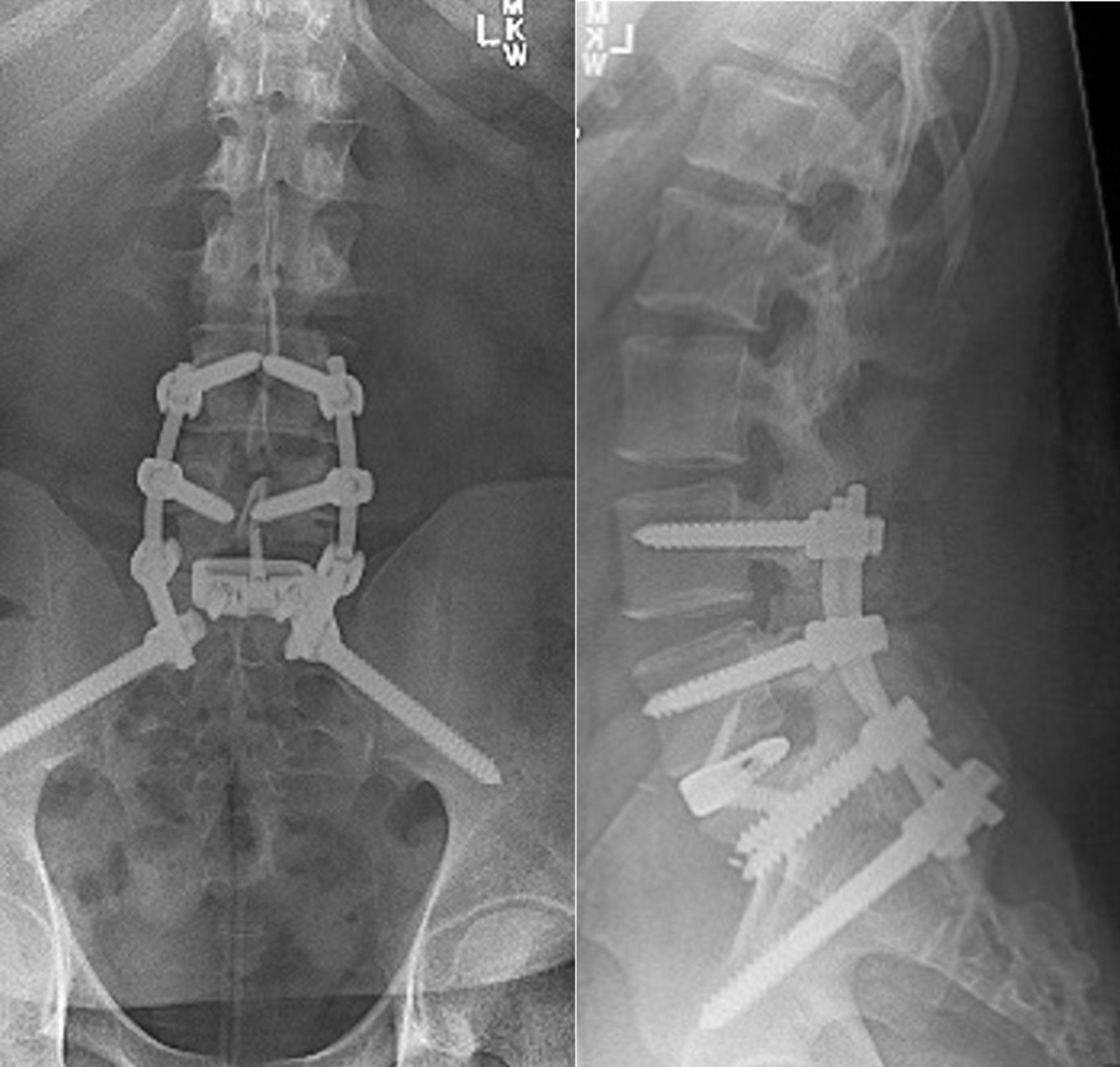
The 3-month follow-up plain radiographs.
Procedures performed in studies were in accordance with the ethical standards of the institutional research committee and with the Helsinki Declaration (as revised in 2013). Written informed consent was obtained from the patient.
DISCUSSION
This case of a patient whose initial supine CT imaging failed to demonstrate lumbosacral instability serves as a useful reminder of the value of additional imaging beyond supine CT in assessing suspected lumbosacral instability. This case also raises the question of whether upright radiographs may pose a potential hazard in patients without obvious instability noted on initial supine imaging but in whom instability is suspected based on the injury pattern.
Traumatic L5-S1 Spondylolisthesis and Related Injuries
Traumatic injuries at the L5-S1 level may occur with a variety of injury patterns. Traumatic instability can present with fractures including the pars, pedicle, and/or facet joints as well as facet dislocation with no fracture (Figure 7).
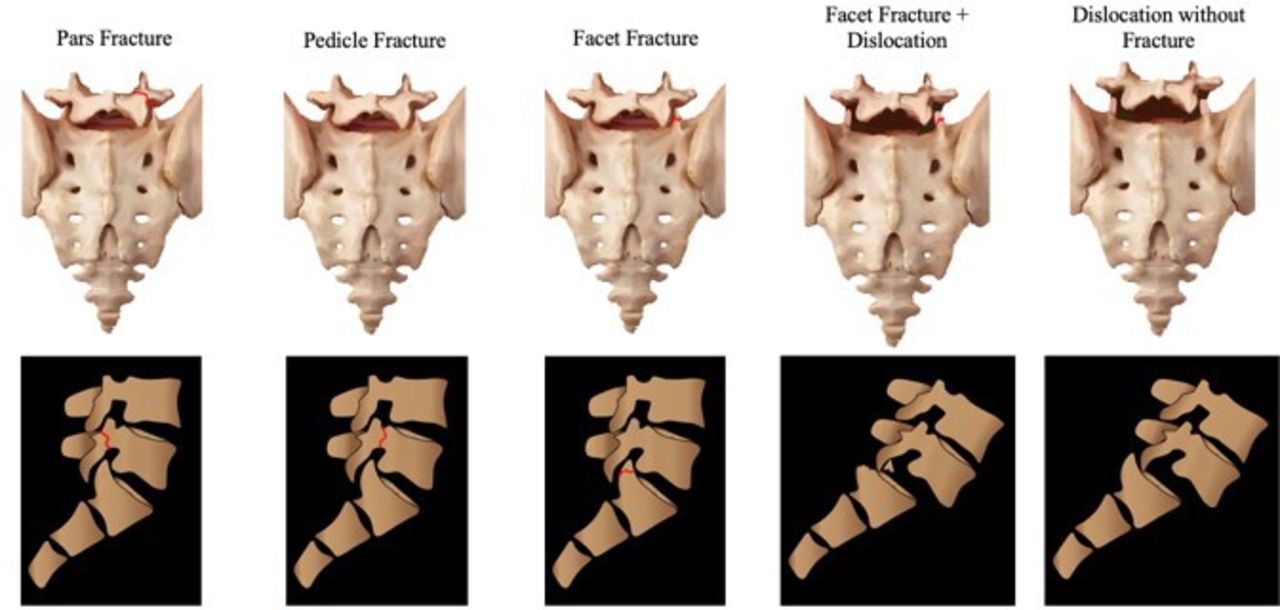
Injuries commonly associated with lumbosacral dislocations.
Approximately, 8% of reported traumatic lumbar/lumbosacral instability cases occur with a concurrent pars fracture.2 Traumatic pars fractures include fractures at the junction of the pars laminae, pars superior articulating process, pars inferior articulating process, and pars pedicle (Figure 8). Traumatic pars fractures are typically accompanied by damage to ligamentous structures. Traumatic lumbar/lumbosacral instability can also present with pedicle fractures (10.4% of all reported traumatic lumbar/lumbosacral instability cases).2 Facet fractures are present in 26.4% of patients with traumatic lumbar/lumbosacral instability. Facet dislocation without fracture occurs in 24.8% of reported cases of lumbosacral instability.2 Facet dislocation can be either unilateral or bilateral and is primarily due to hyperflexion of the spine or, in the case of unilateral dislocation, rotational forces.16,21 Patients with unilateral facet dislocation are less likely to present with neurological deficits than those with bilateral facet dislocations.22 Due to the disc and ligamentous injuries associated with the above fractures, anterior and posterior fusion is recommended in the majority of cases.22 In select cases, such as those of unilateral facet fractures and other patterns with less instability, posterolateral fusion with or without concurrent decompression might be indicated.22 This should be at the surgeon’s discretion based on the degree of instability assessed on preoperative imaging and identified intraoperatively.
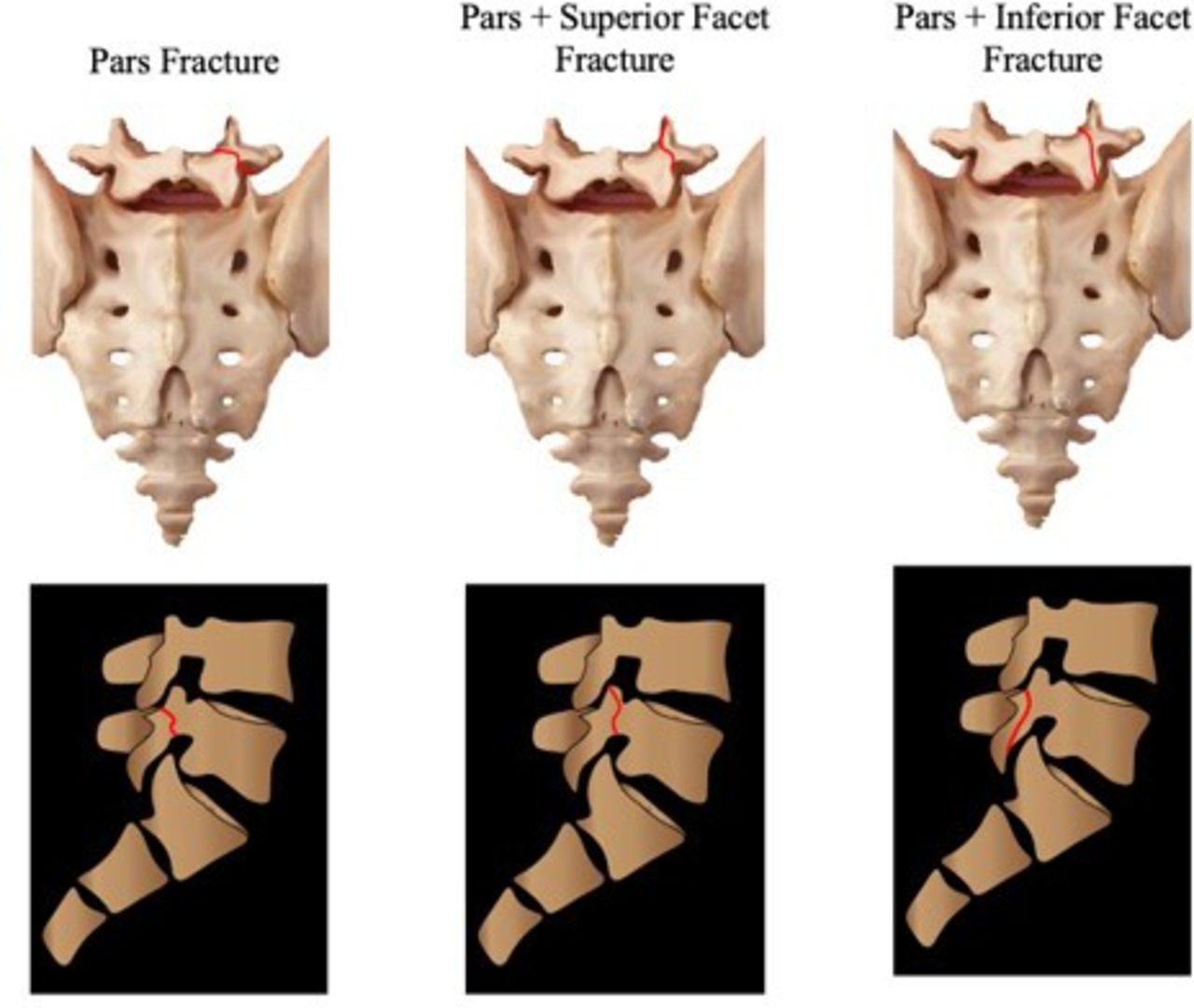
The various types of pars fractures seen in lumbosacral dislocations.
Imaging of Traumatic L5-S1 Injuries
In modern practice, given that supine CT imaging is performed in most trauma patients presenting with high-energy mechanisms, it is often assumed that unstable injuries will be evident on a CT image. This case highlights that CT imaging alone may not be sufficient to rule out instability, and magnetic resonance imaging (MRI) should be considered to evaluate the integrity of the intervertebral disc and posterior ligamentous complex. However, even when upright plain radiographs are obtained, lumbosacral dislocation may be missed due to the difficulty of interpreting these images and, sometimes, the subtle findings on plain radiographs.3,10,23
Furthermore, in cases where significant instability exists, upright radiographs may result in significant listhesis and possibly neurologic compromise. This could represent a potential hazard to patients—particularly, those who present neurologically intact. In this case, the initial supine CT images did not show anterolisthesis or facet joint dislocation. However, upright radiographs demonstrated bilateral L5-S1 facet joint dislocations and significant listhesis. Even without the objective evidence of instability on initial imaging, as was the case in this patient, a high index of suspicion for instability may warrant proceeding directly to MRI without obtaining upright imaging due to the potential risks of obtaining such imaging. It is therefore critical that clinicians be aware of fracture and injury characteristics that raise suspicion for instability and therefore warrant additional investigation in the form of MRI.
Identifying the Unstable Injury—When to Worry
Transverse process fractures have been recommended as an indicator for potential lumbar/lumbosacral intability.10,16,17 The vast majority of lumbar transverse process fractures, however, are incidental findings that rarely indicate the presence of instability or require operative management.18 Therefore, the recommendation to obtain reflexive MRIs in every patient with multiple transverse process fractures is not practical. In patients with multiple transverse process fractures, consideration should be given to other fractures present and the mechanism of injury. Because lumbosacral instability occurs only with high-energy mechanisms, a patient with a high-energy mechanism of injury should be considered differently than those with low-energy mechanisms.
The presence of fractures, involving the L5-S1 vertebral bodies, pedicles, pars, or facet joints, should raise suspicion for instability. Facet fractures are the most commonly observed fractures in cases of traumatic lumbar/lumbosacral instability and have been reported in 26.5% to 72.8% of patients.2,4 Fractures involving the pars, pedicle fractures, and /or vertebral body fractures are seen but are less common.2 When taken together, lumbosacral dislocations occur concomitantly with one of these fractures over 70% of the time in all reported cases.2,4 Assessing lumbar spine trauma requires consideration of many factors, but special consideration to high-energy mechanisms, soft tissue injury, and concomitant fractures will help the treating physicians’ patients with unstable injuries who need special care and advanced imaging.
Strengths and Limitations
One limitation of this case report is the absence of presurgical MRI. This would have provided additional insight into the extent of the ligamentous and soft tissue injury. Obvious instability was noted on upright radiographs; therefore, MRI was not necessary to determine whether operative intervention was required. Surgical intervention in this and similar cases should include the minimum number of levels necessary to provide stability and obtain fusion. Given the degree of instability and soft tissue injury noted intraoperatively, we felt that having additional levels of fixation at L4 and in the pelvis was indicated. We were also concerned that the fracture at the base of the right L5 transverse process could potentially compromise the pedicle fixation at that level. The addition of additional levels does add to the morbidity of the procedure, and this should be taken into consideration, particularly in younger, more active patients. In cases with less marked instability, isolated fixation at L5-S1 would likely be sufficient, and it is possible that it would have provided adequate stability in the present case as well. We recommend that decisions regarding the number of levels and the need for anterior-posterior be determined by the operating surgeon based on the preoperative imaging and intraoperative findings. Discretion should be utilized when choosing to add additional levels. This is an area of potential future investigation.
CONCLUSION
Traumatic lumbar/lumbosacral instability is a rare injury with potentially devasting complications. The injury is often missed on plain radiographs. Special care should be taken in the evaluation of patients with fractures involving the L5-S1 levels, including the vertebral bodies, pedicles, pars, and/or facet joints and/or patients with multiple transverse process fractures. A high-energy mechanism of injury should further raise suspicion of instability. Standard supine CT imaging may not be sufficient for diagnosing stability, and upright radiographs may present a potential hazard to patients. Clinicians should therefore be quick to obtain MRI in patients in whom potential instability is suspected.
Footnotes
Declaration of Conflicting Interests The authors have no conflicts of interest to declare.
Disclosures Byron Stephens has received institutional research support from NuVasive and Stryker Spine. Amir Abtahi has received institutional research support from Styker Spine. All other authors have nothing to disclose.
IRB Approval Vanderbilt University Medical Center provided proper IRB approval.
Ethical Considerations The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.