


Abstract
Background For patients with back pain from osteoporotic vertebral compression fractures (VCFs), vertebral augmentation remains the most utilized surgical intervention. Previous studies report 30-day readmission and mortality rates of up to 10% and 2%, respectively. These studies, however, have included patients with pathologic fractures and combined patients in different admission settings. We undertook the current study to address such shortcomings, which make risk stratification and appropriate counseling difficult.
Methods Four consecutive years of the National Surgical Quality Improvement Program database were queried. Patients who underwent vertebral augmentation for osteoporotic VCFs were divided into 3 groups: (1) outpatient group (defined as patients with same-day discharge), (2) inpatient group (defined as those who were admitted postoperatively), and (3) preprocedure hospitalized group (defined as those who were already inpatient or were at acute/intermediate care facilities and transferred). Postoperative 30-day complications and readmission rates were compared between different groups and examined using multivariate analyses.
Results A total of 1023 patients underwent outpatient surgery; 503 were admitted on the day of surgery; and 149 patients were already in-hospital or were transferred from other facility. Mortality rates were 0.68%, 0.60%, and 2.68%, and readmission rates were 6.26%, 6.76%, and 12.8%, for outpatient, inpatient, and preprocedure hospitalization cohorts, respectively. Multivariate analyses identified preprocedure hospitalization as an independent risk factor for urinary tract infection (UTI; OR = 3.98, 95% CI = 1.41–11.20, P = 0.028), pneumonia (OR = 19.69, 95% CI = 3.81–101.65, P < 0.001), readmission (OR = 1.86, 95% CI = 1.06–3.26, P = 0.032), and mortality (OR = 4.49, 95% CI = 1.22–16.53, P = 0.024).
Conclusion Our findings suggest that published rates of complications and mortality are substantially impacted by the cohort of patients who are already hospitalized or transferred from other facilities. Such patients are at a higher risk of UTI, pneumonia, readmission, and mortality. Conversely, we show that a relatively healthy patient being offered outpatient same-day augmentation has a readmission risk 40% lower and a mortality risk 3 times lower than previously reported.
Level of Evidence 3.
Introduction
Vertebral compression fracture (VCF) is a common fracture in elderly populations, accounting for approximately 700,000 fractures in the United States annually1 and responsible for estimated annual medical costs of $12.2 to $17.9 billion.2 Most patients are initially treated conservatively with pain management, medical osteoporosis treatment, bracing, or physical therapy with good results. For those with unremitting pain, however, vertebral augmentation procedures may be an option.3
Vertebral augmentation procedures include vertebroplasty and kyphoplasty. Vertebroplasty involves percutaneous injection of bone cement into a collapsed vertebra to stabilize the vertebral body and improve pain. Vertebroplasty is cement augmentation alone without restoration of vertebral height and has been associated with a high rate of cement extravasation into the canal, up to 67% cases in early series,4,5 though a majority are clinically insignificant. Kyphoplasty utilizes inflation of a small balloon tamp in the vertebral body to restore height and create a cavity prior to cement injection.6
The efficacy of vertebral augmentation procedures was brought into question following 2 double-blind randomized trials utilizing sham surgery controls published in 2009. Debate ensued following the studies due to concerns regarding the low enrollment numbers, inclusion criteria, and particularities of cement injection techniques. There was a sharp decline in the number of both the vertebroplasty and kyphoplasty procedures following the publication; however, kyphoplasty has seen a recent increase in its utilization with an increasing number of outpatient procedures performed.
Available literature on short-term complications of vertebral augmentation utilizing large databases exist and report a mortality rate of approximately 2% and a readmission rate up to 10.8%.7–9 Most such studies, however, combined VCFs of all etiologies, including pathologic fractures secondary to malignancy, which may affect both measures. Moreover, previous studies did not stratify patients based on different delivery settings. Patients undergoing same-day surgery as outpatients; those getting admitted the same-day postprocedure; and those who were already inpatients due to pain, immobility, or other conditions may have different risk profiles, which may impact the perioperative course. Such shortcomings make it difficult for surgeons to accurately counsel individual patients regarding their risks for the procedure.
The purpose of this study was to compare the 30-day postoperative complications following vertebral augmentation for osteoporotic VCFs in different admission settings using a large national database. Our hypothesis is 2-fold. We hypothesized that (1) patients undergoing surgery on an outpatient basis and those getting admitted on the day of surgery would have a similar rate of postoperative complications and (2) preprocedure hospitalized patients would have a higher rate of postoperative adverse outcomes.
Materials and Methods
Data Source
The American College of Surgeons National Surgical Quality Improvement Program (NSQIP) was queried for database years 2011 to 2014. The database is a collection of more than 150 patient variables, including demographic data, comorbid conditions, Current Procedural Terminology (CPT) codes, length of hospital stay, and 30-day postoperative complications, unplanned reoperation, and unplanned readmission. The data are abstracted from medical records, operative reports, and patient interviews. The NSQIP project began in 1994 as a quality improvement initiative within the Veterans Administration health system, and the program was subsequently expanded to include private hospitals starting from 1998.10,11 For year 2014, the most recent database year queried for the study, the database included more than 750,000 admissions from approximately 500 hospitals. The CPT codes for vertebral augmentations have changed in 2015, and the new codes were not tracked by the NSQIP. Database quality is maintained by trained on-site surgical clinical reviewers and an internal auditing process, which controls inter-rater reliability.
Study Population
Patients who underwent kyphoplasty were identified using CPT codes 22523, 22524, and 22525, and those who underwent vertebroplasty were identified using CPT codes 22520, 22521, and 22522. To identify typical elective augmentation procedures, patients who underwent other concurrent spinal procedures or those who were dependent on a ventilator were excluded. To select only the osteoporotic VCFs and exclude pathologic fractures, patients diagnosed with disseminated cancer and those who underwent recent chemotherapy (<30 days from the surgery) or radiotherapy (<90 days from the surgery) for malignancy were excluded.
Patient Cohorts
Patients were divided into 3 groups based on admission setting: outpatient, inpatient, and preprocedure hospitalization groups. The outpatient group was defined as those who underwent same-day surgery and were discharged that day. The inpatient group referred to those admitted to the inpatient hospital postprocedure on the day of surgery. The preprocedure hospitalization group included patients who were already inpatient prior to the surgical date, those who were admitted through the emergency department and remained as inpatient after the procedure, and those transferred from an outside facility (acute care facility or intermediate care facility) prior to the procedure.
Patient Factors and Outcome Variables
Patient variables assessed in the study were age, race, body mass index, and preoperative functional status. Dependent functional status was defined as requiring partial or total assistance for activities of daily living. Activities of daily living was defined as “the activities usually performed in the course of a normal day in a person’s life” and included feeding, dressing, bathing, toileting, and mobility. Comorbid conditions investigated included cardiovascular comorbidities (congestive heart failure, myocardial infarction, previous percutaneous coronary intervention, previous cardiac surgery, angina, hypertension, and peripheral vascular disease), pulmonary comorbidities (smoking status, chronic obstructive pulmonary disorder, and dyspnea), dialysis, cerebrovascular comorbidities (stroke with deficits, stroke without deficits, and transient ischemic attack), recent weight loss, diabetes mellitus, and corticosteroid use for chronic conditions. The type of procedure that a patient underwent (kyphoplasty vs vertebroplasty) was also assessed.
Postoperative complications investigated were mortality, sepsis/septic shock, myocardial infarction, unplanned reintubation, pneumonia, renal complications (acute renal failure or progressive renal insufficiency), hospital-acquired conditions (wound infection, wound dehiscence, urinary tract infection [UTI], deep vein thrombosis, and pulmonary embolism), and intraoperative/postoperative transfusion. Other outcome variables assessed were unplanned readmission, unplanned reoperation, and discharge destination. Nonhome discharge to facility included skilled care facility (acute care facility, transitional care unit, subacute hospital, ventilator bed, or skilled nursing home), unskilled facility (nursing home or assisted facility, if not patient’s home preoperatively), or rehabilitation facility.
Statistical Analysis
Patient demographics, comorbid conditions, perioperative characteristics, and postoperative complications were compared between the inpatient vs outpatient cohort and the preprocedure hospitalized vs outpatient cohort. The outpatient cohort was selected as a reference since the majority of patients underwent vertebroplasty on outpatient basis. Student t test was employed for continuous variables, and χ 2 test was used for categorical variables. Statistical significance level was set at 2-sided alpha level of 0.05. The SAS software (version 9.3, SAS Institute Inc., Cary, NC, USA) was utilized for statistical analyses.
Multivariate logistic regressions were performed to evaluate whether inpatient and preprocedure hospitalization status were independent risk factors for postoperative adverse events found to be significantly associated with admission settings. For each multivariate analysis, patient variables and comorbid variables found to be moderately associated (P < 0.2) were included in the model to control for confounding variables. Multivariate logistic regression’s predictive accuracy was measured with c-statistic, and the cutoff was set at 0.65.
Results
Patient Demographics
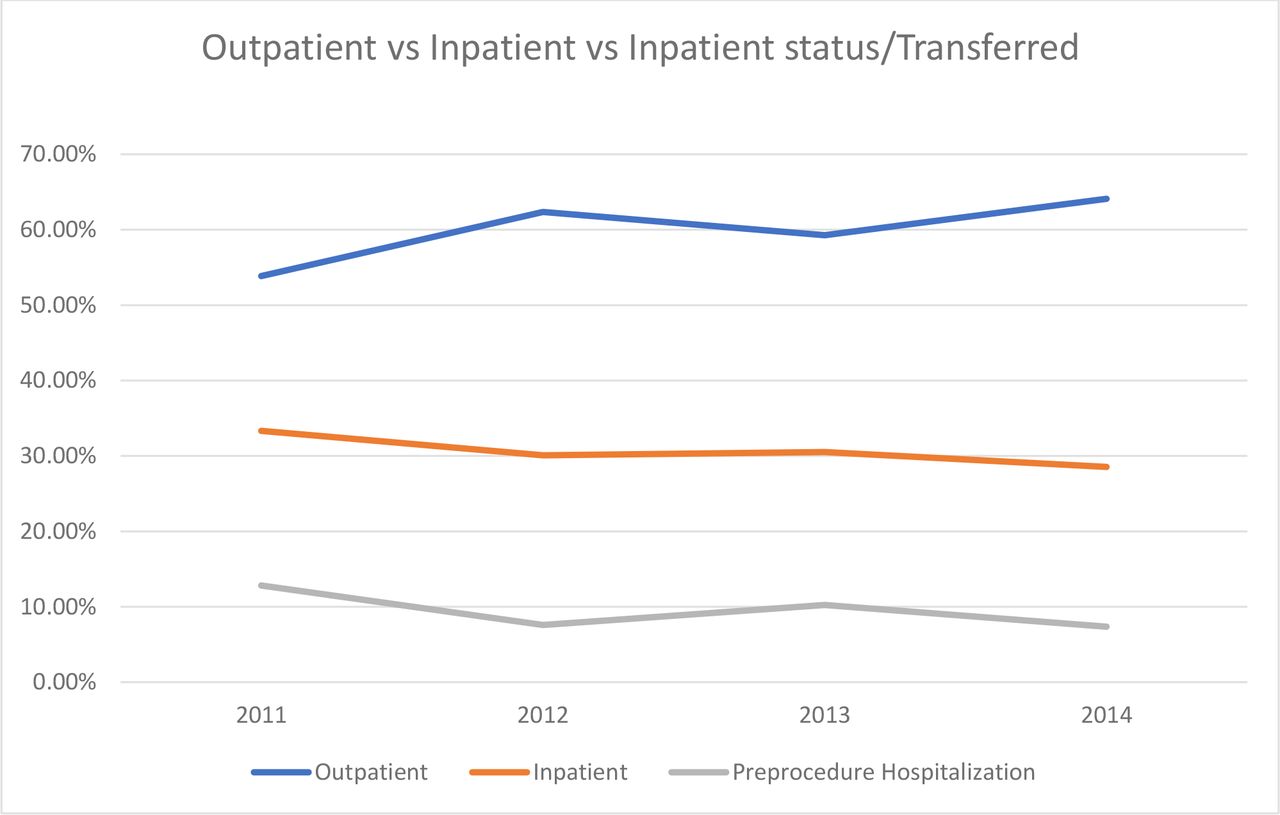
Over the database years analyzed, the proportion of outpatient cases increased from 53.9% in 2011 to 64.1% in 2014. The proportion of same-day admission inpatient group decreased from 33.3% in 2011 to 28.6% in 2014, while the proportion of patients in the preprocedure hospitalization cohort decreased from 12.8% to 7.4% (Figure).

Percentages of inpatient vs outpatient vs preprocedure hospitalized cohorts who underwent vertebral augmentations by year. From 2011 to 2014, the percentage of patients who recieved outpatient vertebral augmentation increased from 53.9% in 2011 to 64.1% in 2014. The percentage of patients who underwent the procedure as inpatients decreased from 33.3% in 2011 to 28.6% in 2014. The proportion of patients who were hospitalized before the procedure decreased from 12.8% in 2011 to 7.4% in 2014.
A total of 1675 patients satisfying our inclusion and exclusion criteria were identified. Of those patients, 1023 patients underwent vertebral augmentation on an outpatient same-day basis. Also, 503 patients were admitted as inpatients on the day of surgery, and 149 patients were in the preprocedure hospitalization group. The mean ages for the outpatient, inpatient, and preprocedure hospitalization groups were 74.0, 75.9, and 79.6 years, respectively. Each group consisted of approximately 70% of female patients, with no significant difference. Preinjury functional status did not differ significantly between the outpatient and the inpatient cohorts, with approximately 90% in each group having independent functional status. However, only 66.4% of patients in the preprocedure hospitalization group were functionally independent, which was significantly lower than the percentage for the outpatient cohort (Table 1). Approximately 90% of patients underwent kyphoplasty instead of vertebroplasty, and this proportion did not differ significantly across surgical settings.
Demographics of patients receiving vertebral augmentation by surgical setting.
Patient Comorbidities by Surgical Setting
The complete profiles of comorbidities for each group are presented in Table 2. The inpatient group had a significantly higher rate of chronic obstructive pulmonary disease (COPD) at 14.5% compared with that of the outpatient cohort at 10.6% (P = 0.025). Compared with the outpatient cohort, the preprocedure hospitalized group had significantly higher rates of hypertension that required medication (73.8% vs 62.1%, P = 0.005) and significantly higher rates of COPD (20.8% vs 10.6%, P < 0.001). Other comorbid variables were not found to be significantly different.
Comorbidities and operative variables by surgical setting.
30-Day Postoperative Outcomes by Surgical Setting
Compared with the outpatient cohort, the inpatient cohort had significantly higher rates of sepsis/septic shock (1.19% vs 0.1%, P = 0.003), myocardial infarction (0.4% vs 0%, P = 0.044), and perioperative transfusion (0.6% vs 0%, P = 0.013). Compared with the outpatient cohort, the preprocedure hospitalization group had higher incidences of mortality (2.68% vs 0.68%, P = 0.018), sepsis/septic shock (1.34% vs 0.1%, P = 0.005), pneumonia (4.03% vs 0.2%, P < 0.001), UTI (4.03% vs 0.98%, P = 0.003), perioperative transfusion (0.67% vs 0%, P = 0.009), and readmission (12.08% vs 6.26%, P = 0.009) (Table 3).
Short-term postoperative outcomes by surgical setting.
From the multivariate analyses, the surgery in inpatient setting was not found to be an independent predictor for any of the tracked postoperative adverse outcomes. However, preprocedure hospitalization, when compared with outpatient setting, was found to be an independent risk factor for UTI (OR = 3.98, 95% CI = 1.41–11.20, P = 0.028), pneumonia (OR = 19.69, 95% CI = 3.81–101.65, P < 0.001), readmission (OR = 1.86, 95% CI = 1.06–3.26, P = 0.032), and mortality (OR = 4.49, 95% CI = 1.22–16.53, P = 0.024) (Table 4). Similarly, when compared with surgery in the inpatient setting, surgery in the preprocedure hospitalized setting was found to be an independent risk factor for pneumonia (OR = 7.22, 95% CI = 1.70–30.69, P = 0.007) but not for UTI, readmission, or mortality (Table 4).
Evaluation of surgical setting as a risk factor for selected postoperative complications.
Discussion
VCF is one of the more common fractures, accounting for approximately 700,000 fractures in the United States with associated annual medical costs of $12.2 to $17.9 billion.2 VCFs can cause pain and deformity, which in turn may lead to reduced function and increased mortality in those affected. While many patients may improve with conservative modalities, including pain control, medical treatment of osteoporosis, bracing, or physical therapy, those with debilitating back pain often undergo vertebral augmentation.
Two recent double-blinded studies that used a sham surgery group as the control group have brought into question the efficacy of vertebral augmentation procedures.12,13 After these studies were published, there was a marked drop in the utilization of kyphoplasties and vertebroplasties in the United States.14 Much debate on the subject ensued, particularly regarding the methodologies, low patient enrollment numbers, inclusion criteria, and the cement injection techniques.15,16 Despite the controversy, there has been a recent rebound in the utilization of vertebral augmentation procedures,17 and the procedures remain the most utilized surgical intervention for VCFs.
Several recent studies have investigated short-term postoperative adverse events following vertebral augmentation.7–9 However, these studies were limited in 2 regards. The investigators did not differentiate patients based on etiologies of VCFs and combined pathologic and osteoporotic VCFs, while patients undergoing surgeries for spinal tumor tend to be associated with worse postoperative outcomes.18 Additionally, these investigations combined patients in different surgical settings. These shortcomings make precise informed consent more elusive since the risk profiles may differ given these circumstances.
To address this, we excluded VCFs due to pathologic fractures and divided patients into 3 cohorts: those undergoing the procedure on an outpatient same-day basis, those who were admitted as inpatients postoperatively, and those who were hospitalized preoperatively. More precisely, the preprocedure hospitalized cohort consisted of those who were inpatient preoperatively and those who were transferred from other facilities or emergency departments.
We report the 30-day postoperative mortality rates of approximately 0.6% for both the outpatient and the inpatient groups. This is much lower than the previously reported 30-day mortality rates of 1.5% to 2.0% following vertebral augmentation.8,9 The difference could be attributed to the stratification of surgical setting and the exclusion of pathologic VCF cases. On the other hand, the mortality rate for the preprocedure hospitalized group was found to be 2.68%, and preprocedure hospitalization was found to be an independent risk factor for mortality from multivariate analysis. Considering the mortality rate of 0.23% in elective spinal surgeries as reported by Ottesen and colleagues’ analysis of 173,778 patients,19 the mortality rate of 2.68% from a minimally invasive surgery is significant.
Thirty-day readmission rates were found to be 6.26%, 6.76%, and 12.08% for the outpatient, inpatient, and preprocedure hospitalized cohorts, respectively. The readmission rates for the outpatient and inpatient groups were significantly less than the previously reported rates of 10.6% to 10.8%.8,9 Again, the disparity is attributable to more focused patient selection and stratification of surgical settings. The readmission rates of 6.26% to 6.76% are in line with the reported readmission rates of various lumbar spinal surgeries reported by Pugely et al.20 In their analysis of more than 15,000 patients who underwent lumbar spinal surgery, the readmission rates ranged from 3.3% for lumbar discectomy and 8.95% for deformity correction. In our study, the readmission rate of 12.08% for the preprocedure hospitalized cohort is substantial and may be attributable to higher comorbidity and lower baseline function. While the preprocedure hospitalization status was found to be an independent risk factor for readmission (OR = 1.86, 95% CI = 1.06–3.26, P = 0.032), we believe that numerous factors in this subset cumulatively resulted in its distinctly higher perioperative adverse outcomes. For example, there was a very strong association between functional status and surgical setting, and, to correct for potential multicollinearity, we opted to exclude the functional status variable in the multivariate analysis.
The comparison of the outpatient and inpatient cohorts is worth noting. Although patients who were admitted postoperatively had higher rates of COPD and a higher percentage of patients with the American Society of Anesthesiologists 3 or higher compared with those who were discharged the same day, the rates of mortality and readmission between the 2 groups were similar. The inpatient cohort, however, had higher rates of sepsis (1.19% vs 0.1%, P = 0.003), myocardial infarction (0.4% vs 0%, P = 0.044), and perioperative transfusion (0.6% vs 0%, P = 0.013). Altogether, this implies that the current level of clinical decision-making on postoperative admission is sound and adequate and that there is a subset of patients who would benefit from inpatient care after surgery.
If the comparison between the outpatient and inpatient cohorts reflects the sound level of clinical acumen in deciding whom to discharge and keep in-house postoperatively, the comparison between the inpatient and preprocedure hospitalized groups highlights that those who were hospitalized prior to surgery may benefit from closer observation. When compared with those who were admitted postoperatively, preprocedure hospitalization was found to be an independent risk factor for postoperative pneumonia (OR = 7.22, 95% CI = 1.70–30.69, P = 0.007). Though not found to be a significant risk factor for mortality (OR = 1.86, 95% CI = 1.06–3.26, P = 0.032) and readmission (OR = 4.78.86, 95% CI = 1.06–3.26, P = 0.032), it is worth noting that the preprocedure hospitalization status was reaching significance as an independent risk factor (Table 4).
There are limitations to the study that should be taken into account when interpreting the findings. The study was limited by the retrospective study design. Although associations could be elucidated between variables, no definitive conclusion could be drawn regarding causation. In a way, the surgical setting is an optimal proxy for evaluating one’s functional status. The study was also limited by the use of the NSQIP database. Though comprehensive, the NSQIP database may not be granular enough to capture all the variables related to surgical decision-making. For example, patient’s social circumstances, individual pain tolerance level, and physician’s preference and experience could potentially affect the decision. Moreover, the NSQIP database does not collect variables specific to vertebral augmentation such as duration and modalities of nonoperative management a patient may have had preoperatively. This limitation prevented the analysis of surgical timing from fracture to intervention as a variable that could affect postoperative complications. This question warrants future research utilizing a different study design. Additionally, the postoperative complications are only tracked up to 30 days postoperatively, and long-term prognosis or the efficacy of vertebral augmentation could not be evaluated.
Conclusion
Despite the limitations, the current study is the first to our knowledge to analyze the short-term adverse events focusing on the osteoporotic VCF cases, stratified by different admission settings. Our findings suggest that the patients who are being transferred from other facilities, including emergency departments, and those who are already hospitalized are at a higher risk of sustaining multiple postoperative adverse outcomes, including UTI, pneumonia, readmission, and mortality. Specifically, we showed that a relatively healthy patient being offered outpatient same-day augmentation has a readmission risk 40% lower and a mortality risk 3 times lower than previous studies have reported. Given the prevalence of osteoporotic VCFs and increasing utilization of vertebral augmentation, the lack of accurate data to serve as a basis for informed consent has been concerning. The current study should aid surgeons in stratifying risk and in appropriately counseling patients and their families.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
Ethics Approval This study was qualified as exempt by the Rutgers University New Jersey Medical School Institutional Review Board.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.