


Abstract
Background Our objective is to describe a minimally invasive endoscopic surgical technique for performing lateral lumbar interbody fusion (LLIF). LLIF is a common approach to lumbar fusion in cases of degenerative lumbar disease; however, complications associated with psoas and lumbar plexus injury sometimes arise. The endoscopic modification presented here diminishes the requirement for sustained muscle retraction, minimizing complication risk while allowing for adequate decompression in select cases.
Methods Endoscopic LLIF (ELLIF) was performed in 3 patients from 2019 to 2021. Surgeries were performed in the lateral position under general anesthesia with neurophysiological monitoring. Discectomy, endplate preparation, and harvesting of iliac crest bone were performed through a working channel endoscope. The introduction of an interbody cage (Joimax EndoLIF) was performed over a nitinol blunt-tip wire (Joimax). No expandable blade retractors were required.
Results At 2-year follow-up of these 3 patients, the mean visual analog scale (VAS) score for leg pain improved from 9.3 to 1.7, and the mean Oswestry Disability Index (ODI) score improved from 40 to 8.3. There were no complications, readmissions, or recurrence of symptoms during the 2-year follow-up period. Patients spent an average of 36 hours in the hospital postoperatively and returned to normal daily activities after an average of 48 days.
Conclusions A minimally invasive modification to the LLIF procedure is presented that offers several potential advantages due to the application of endoscopic techniques: reduced muscle retraction, smaller incision, and the opportunity to perform both indirect decompression and endoscopically visualized discectomy in the same fusion procedure.
Clinical Relevance The proposed endoscopic lateral lumbar interbody fusion and decompression is a minimally invasive technique that may provide patients with minimal complications, quick recovery, and good functional recovery.
Level of Evidence 4.
- endoscopic spine; lateral lumbar interbody fusion
- radiculopathy
- minimally invasive spine
- indirect decompression
Introduction
Lumbar interbody fusion (LIF) is an indicated procedure for patients with 1 or 2 levels of degenerative disease of the lumbar spine.1 LIF is performed after discectomy, with a cage or spacer placed into the intervertebral space.2 There are many different approaches to LIF, including posterior (PLIF), transforaminal (TLIF), oblique (OLIF), anterior (ALIF), and lateral (LLIF). The LLIF approach has the advantage of allowing larger cages to be placed with less dissection of surrounding tissues.3 Additionally, LLIF lends itself well to minimally invasive surgery (MIS). MIS for lumbar fusion has been shown to yield improved patient outcomes such as decreased pain, fewer complication rates, and shorter length of stay postoperatively.4 OLIF with a spinal endoscope is a minimally invasive approach that has been shown to achieve discectomy and fusion with direct spinal cord decompression.5,6
LLIF and OLIF are not without potential serious complications. Studies show that as many as 48% of patients who underwent OLIF had perioperative complications; however, only about 2% of these were permanent.7 More serious complications such as bowel perforation and fatality from vascular injury have also been reported in LLIF.8,9 Many operative complications from LLIF may result from a lack of visualization of anatomical structures. Although there are only preliminary data, the utilization of an endoscope for visualization of the lumbar plexus and iliac vessels has demonstrated success in avoiding the most serious complications of LLIF.10 However, a complication that remains with endoscopic-assisted LLIF is iatrogenic damage due to psoas and lumbosacral plexus retraction needed to perform discectomy.11
We present an endoscopic modification to LLIF to mitigate the previously mentioned complications while retaining the advantages of MIS and LLIF in addition to several novel advantages. Endoscopic LLIF (ELLIF) is beneficial because it is minimally invasive and enables both indirect decompression of the spinal cord and nerve roots and discectomy under direct endoscopic visualization.12 The purpose of this technical note is to describe the minimally invasive ELLIF procedure and its benefits. Here, we present 3 patients who underwent ELLIF surgery and their subsequent postoperative improvements.
Materials and Methods
Operative Procedure
For all ELLIF (Joimax EndoLIF) spine procedures, the patient was under general anesthesia and positioned in the lateral decubitus position with flexed hips and knees. The procedure can also be done in a prone position, but the lateral approach adds to the advantage of avoiding root damage or damage to the dural sac. Figure 1 demonstrates the positions of the patient and surgeon (Figure 1A), along with the key steps of endoscopically harvesting the iliac crest graft (Figure 1B), packing the interbody cage (Figure 1C), and placing the interbody cage over a nitinol wire (Joimax) (Figure 1D,E).
A 2- to 3-cm incision is made on the skin centered on the junction of the anterior third and the middle third of the disc space in the lateral fluoroscopic projection. A safe area is targeted away from root emergence and anterior vascular structures. The trajectory through the retroperitoneal space to the psoas and lumbar spine is digitally palpated (using the elastic relief of the psoas musculature as a guide element and the transverse process of the vertebrae as a static element). Electrophysiological monitoring is used with a blunt dilator to determine that the path is free of neural elements. Successive dilators are then placed in the disc and then the final 7-mm beveled tubular retractor. Once inside the disc, the working channel endoscope can be introduced. Under endoscopic visualization, the surgeon can perform a discectomy for fusion preparation, a discectomy for contralateral foraminal decompression, endplate preparation, and anterior longitudinal ligament (ALL) transection to increase lordosis. The ALL is visualized through the endoscope, and its fibers are partially resected until it is weakened enough to ensure an improvement in lordosis. It is not necessary to resect it completely and visualize vascular structures.
An ipsilateral transforaminal endoscopy to decompress the foramen can be done along with interlaminar decompression through the same incision in the lateral or prone position before or after percutaneous instrumentation, to work on the foramen, disc, or anterior structures of the spinal canal. Reaching the ALL and ipsilateral foramen is feasible through the same incision, made possible simply through the anatomy of the region and approach with the endoscope. If necessary, interlaminar endoscopy can be performed through a separate posterior incision to reach the spinal canal and its posterior structures.
Prior to cage placement, the same incision is used to harvest iliac crest. The method used is cannulation of the iliac crest with a Jamshidi needle and then use of sequential dilators and reamers up to 16 mm until a 7-mm beveled tubular retractor is placed in the crest. A working channel endoscope and endoscopic graspers are used to harvest crest bone. With the working cannula and retractor removed, a titanium cage (Joimax EndoLIF of 35 mm length and 14 mm height) packed with iliac crest is placed over a superplastic nitinol blunt-tip wire (Joimax) through the psoas under fluoroscopic guidance. Larger cages may be possible in this procedure; however, there is currently a limit in the number of over-the-wire cages that have been developed. Patients undergoing cage placement with ALL release can have endoscopic screw fixation to the adjacent vertebral body to prevent graft migration as performed in 2 cases, but the process is difficult and the materials are not currently designed for it.
Percutaneous pedicle screw placement is performed in a standard fashion in the lateral position. Irrigation accumulation in the retroperitoneal space through the endoscope is of minimal concern and therefore not monitored due to the clear exit path through the working cannula and low pressure. Additionally, 60% to 70% of the surgical procedure is performed with over-the-wire instruments as opposed to the irrigated endoscope and only a small amount of time with the endoscope placed in the disk space, which is not completely opened to the retroperitoneal space.

Operative images demonstrating endoscopic lateral lumbar interbody fusion procedure. (A) The patient is positioned in the lateral position with the surgeon demonstrated holding the endoscope and performing the discectomy with fluoroscopic and endoscopic visualization. (B) The endoscope and endoscopic grasper are used to retrieve iliac crest graft for packing the interbody titanium cage. (C) The titanium cage being packed with iliac crest autograft. (D and E) The titanium cage delivery over a nitinol blunt-tip wire is demonstrated, with zoomed-in details shown in (D) and zoomed-out views presented in (E).
Case 1
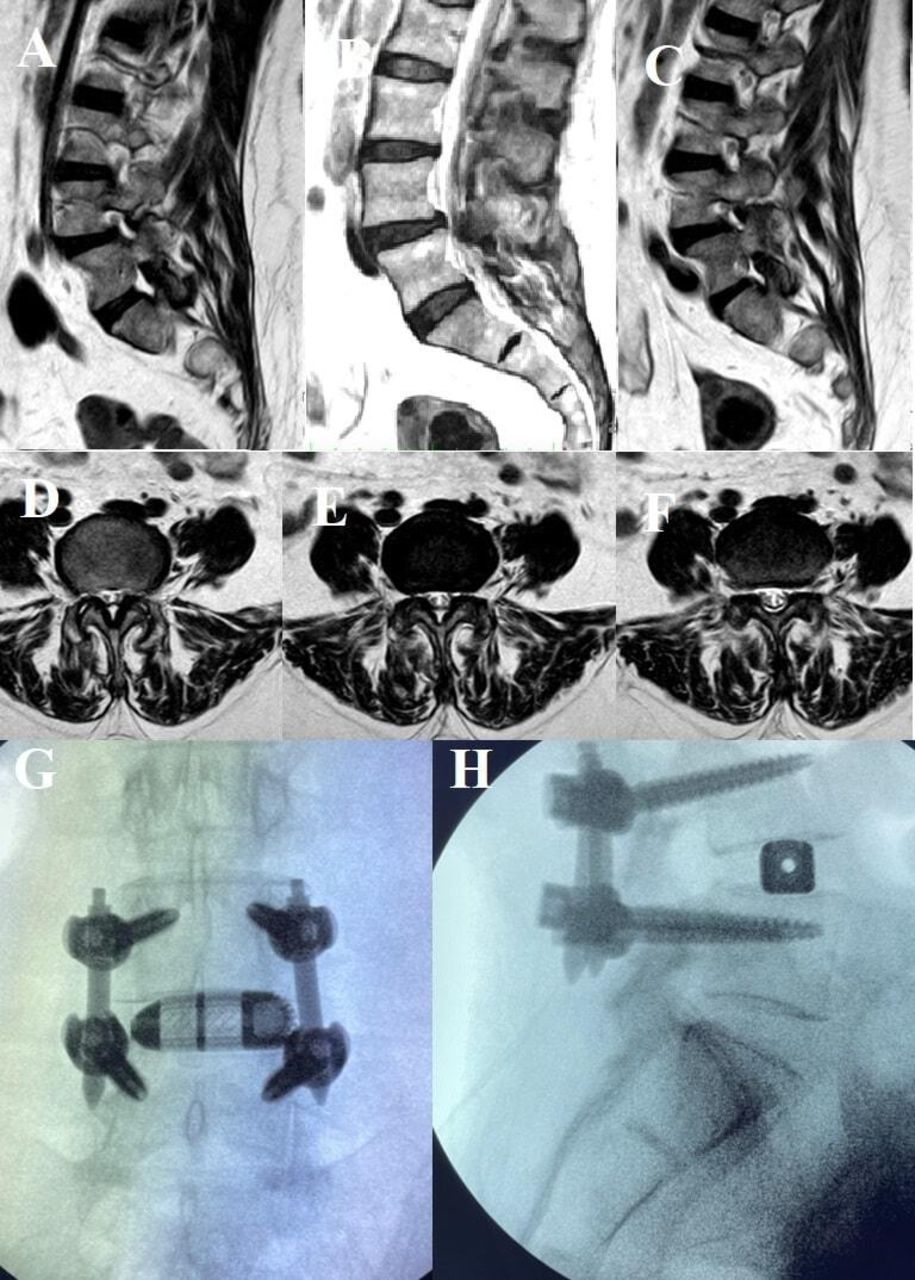
A 64-year-old woman presented with symptoms of severe left L5 radiculopathy and intense back pain. The patient reported a 2-year history of leg and back pain despite physical therapy and injections. A magnetic resonance image (MRI) demonstrated grade 1 spondylolisthesis, endplate changes at L4-5, and severe bilateral foraminal narrowing at L4-5 (Figure 2A-F). The patient underwent L4-5 ELLIF (Figure 2G-H). Figure 3 shows the step-by-step fluoroscopic images of the procedure (Figure 3A-R). At her 2-year follow-up, the patient’s visual analog scale (VAS) score had improved from 8 to 2 and her Oswestry Disability Index (ODI) score had improved from and 32 to 10.

Endoscopic lateral lumbar fusion of L4-5. (A–C) Sagittal T2 magnetic resonance images (MRIs) from right (A), midline (B), and left (C), demonstrating grade 1 spondylolisthesis and severe left foraminal narrowing. (D–F) Axial T2 MRI of the lumbar spine demonstrating severe L4-5 foraminal narrowing in axial images from the bottom of the L4 endplate (D), through the L4-5 disc (E), and through the top of the L5 endplate (F). (G and H) Anteroposterior and lateral fluoroscopic images demonstrate the final position of the lateral interbody fusion device and pedicle screw instrumentation.

Step-by-step endoscopic lateral lumbar fusion (ELLIF) of L4-5. (A–R) Anteroposterior (AP) and lateral fluoroscopic intraoperative images of the key operative ELLIF procedure. (A) AP fluoroscopic image demonstrates the beveled tubular retractor placed through the psoas, and the endoscopic grasper is shown performing the discectomy. (B) AP fluoroscopic image demonstrating the endoscopic curette preparing the endplate for arthrodesis. (C and D) Joimax EndoLIF titanium interbody cage is introduced into the disc space over a nitinol wire. (E and F) Lateral fluoroscopic images demonstrate the placement of the interbody cage with the wire (E) and then with the wire removed (F).(G and H) AP fluoroscopic images of the Jamshidi needle used for placement of the K-wires in the L4 pedicles (G) and L5 pedicles (H). (I) AP fluoroscopic image of the wire placement. (J–M) Lateral fluoroscopic images demonstrate the endoscopic right lumbar L4-5 lateral recess stenosis decompression and discectomy. (J) Endoscopic Shrill drill shown decompressing the lateral recess. (K) Endoscopic Kerrison rongeur shown completing the lateral recess stenosis decompression. (L and M) Lateral fluoroscopic images demonstrating the endoscopic grasper beginning (L) and completing (M) the discectomy as part of the lateral recess decompression. (N and O) AP fluoroscopic images demonstrate iliac crest graft harvesting. (N) Wire cannulates the iliac crest. (O) Crown reamer after placement over dilator shown harvesting iliac crest though ELLIF incision. (P and Q) Lateral fluoroscopic images demonstrate percutaneous pedicle screw placement over the wires. (R) Final AP fluoroscopic image of the fusion construct.
Case 2
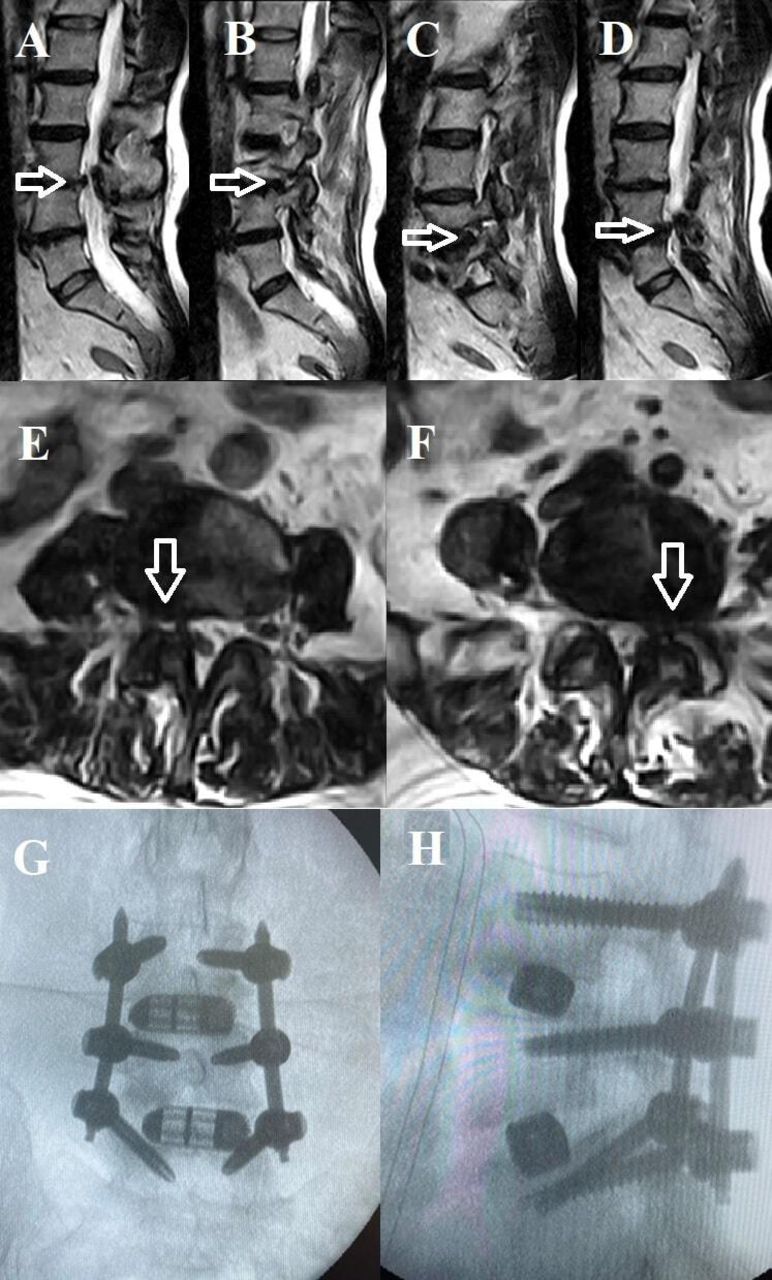
A 71-year-old woman presented with severe back pain and bilateral L4-5 radiculopathy (more intense on the left) despite conservative treatment. Her MRI demonstrated severe right-sided L3-4 and left L4-5 foraminal stenosis and endplate changes at L3-4 and L4-5 (Figure 4A-F). She underwent a transforaminal decompression of her foramen and L4-5 ELLIF through the same incision (Figure 4G,H). She was discharged from the hospital on postoperative day 1 without complication. At her 2-year follow-up, her preoperative VAS score had improved from 10 to 2 and her preoperative ODI score had improved from 42 to 10.

Endoscopic lateral lumbar fusion of L3-5. Sagittal T2 magnetic resonance image (MRI) reveals severe right L3-4 foraminal narrowing and endplate changes at L3-4 (A is paracentral and B is foraminal) (open arrows) as well as severe left L4-5 foraminal narrowing and endplate changes at L4-5 (C is foraminal and D is paracentral) (open arrows). (E and F) Axial T2 MRIs of the right L3-4 foraminal narrowing (E, open arrow) and the left L4-5 foraminal narrowing (F, open arrow). (G and H) AP and lateral fluoroscopic images demonstrate the final position of the lateral interbody fusion devices and pedicle screw instrumentation.
Case 3
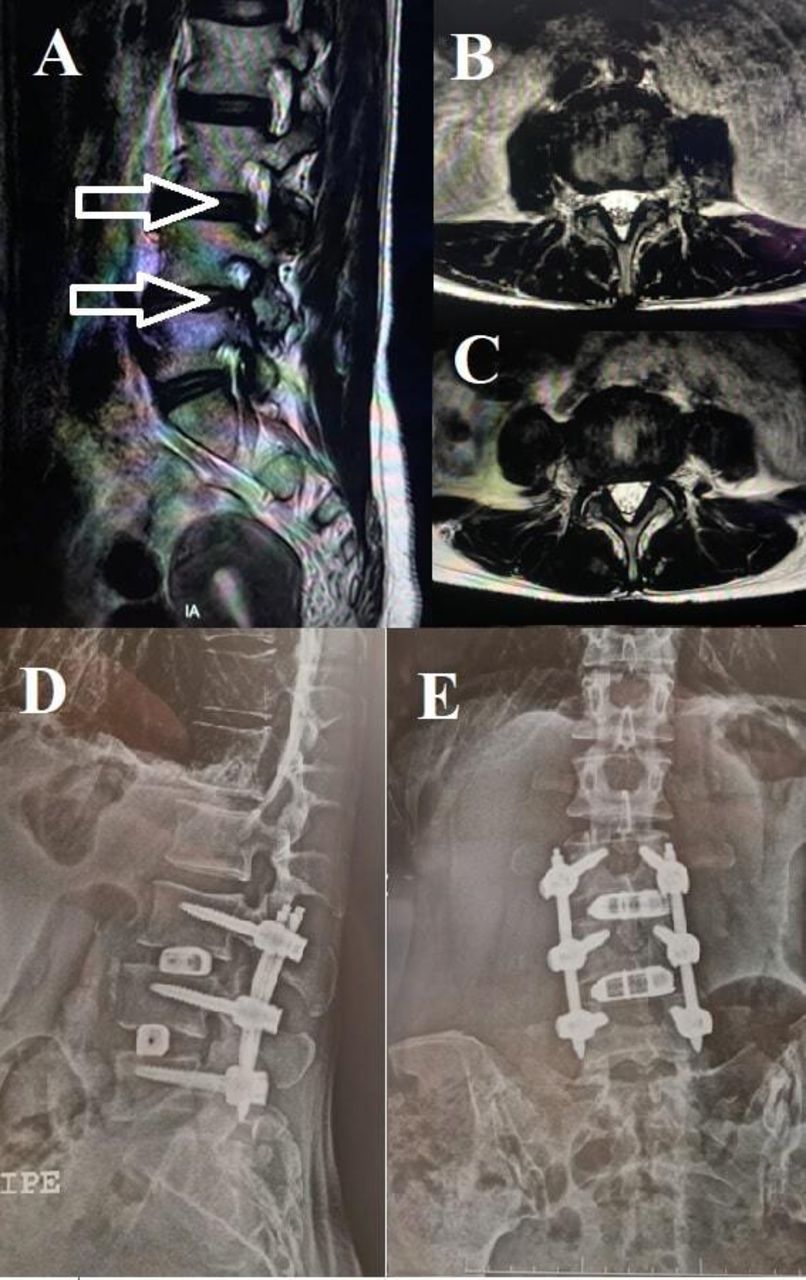
A 49-year-old woman presented with a 2-week history of worsening back and leg pain and was unable to walk. She described a 2-year history of back and bilateral leg pain in L4 distribution. Lumbar anterior-posterior x-ray demonstrated a moderate coronal deformity, and her MRI demonstrated moderate L3-4 bilateral foraminal narrowing and severe L4-5 foraminal narrowing (Figure 5A-C). She underwent multilevel ELLIF at L3-4 and L4-5 (Figure 5D,E). At 2-year follow-up, her preoperative leg VAS score had improved from 10 to 1 and ODI score had improved from 46 to 5. She was discharged from the hospital on postoperative day 2 without complication.

Endoscopic lateral lumbar fusion of L3-5. (A) Sagittal T2 magnetic resonance image (MRI) demonstrates moderate right L3-4 and severe right L4-5 foraminal narrowing (open arrows). (B and C) Axial T2 MRI demonstrates moderate bilateral L3-4 (B) and severe bilateral L4-5 (C) foraminal narrowing. (D and E) Anteroposterior and lateral fluoroscopic images demonstrate the final position of the lateral interbody fusion devices and pedicle screw instrumentation.
Results
Among these 3 patients who underent ELLIF, there were no complications, readmissions, or recurrence of symptoms during the 2-year follow-up period. There were no instances of infection, worsening neurologic status, or durotomy. There were no postoperative hernias or complaints referrable to abdominal nerve branches. There were no patient complaints of pain in the groin or lower extremity and no dysesthesias on the operative side following separation of the psoas branches by the beveled tubular retractor or the placement of the titanium cage over the wire. The patients each had excellent improvement in pain and functionality postoperatively, with significant improvement at only 1 month and average reductions of 82 and 78% in their VAS and ODI at 2 years, respectively (Table 1). Additionally, the 3 patients spent no longer than 2 days in the hospital and had returned to normal daily activities within 2 months (Table 2).
Summary of postoperative changes in VAS and ODI scores at 1-month and 2-year follow-up.
Summary of postoperative recovery.
Discussion
LLIF is a minimally invasive procedure that has been shown to be effective in accomplishing indirect decompression and useful in restoring coronal and sagittal balance. The endoscopic modification of the procedure presented here is intended to reduce retraction on the psoas and lumbar plexus during the discectomy portion of the procedure in an effort to further reduce the complication profile. Standard, nonendoscopic LLIF surgery carries the risk of lumbar plexus and psoas motor deficits as a result of prolonged muscle retraction.13,14 Studies have reported incidences of >25% for immediate, transient postoperative neurologic, and motor deficits, with an incidence of 2.9% to 4.1% for persistent neurologic deficits and 5% for femoral nerve injury.14–18 While the majority of these complications resolve in the 12 to 18 months following surgery, their presence and impact on the patient should not be overlooked.
In the present article, we report 3 patients who underwent ELLIF with very good outcomes, quick recovery, and no complications, transient or persistent. While this limited dataset is insufficient to fully comment on the rates of lumbar plexus or psoas injury, it lays the groundwork for future studies to investigate the proposed improvements through the endoscopic approach. We recognize that the present study is underpowered to detect the aforementioned complications with rates of 2.9% to 5%; however, the purpose is to present a potential endoscopic modification to the LLIF procedure that will eliminate or minimize retractor time, where possible. Further iterations of this work will analyze and present a larger cohort of patients having undergone ELLIF and their respective outcomes. Previous reports have also begun to elucidate the benefits of endoscopic-assisted lumbar fusion. Endoscopic-assisted transforaminal lateral interbody fusion (TLIF) has demonstrated shortened recovery time and earlier back pain relief.19 Additionally, endoscopic-assisted LLIF has been shown to yield low complication rates; however, significant advantages in outcomes compared to standard LLIF are yet to be definitively shown.20
In addition to reduced muscle retraction and a smaller incision, the advantages of the ELLIF approach include the abilities to endoscopically harvest iliac crest bone graft through the original incision and perform endoscopic discectomy for direct decompression of the contralateral foramen. These are all additional benefits that may be afforded to a patient undergoing endoscopic lumbar lateral fusion.
In the context of the aforementioned advantages, we propose the following uses or applications for the ELLIF approach:
Disc, vertebral, or psoas biopsies.
Discectomy and preparation of disc endplates for introduction of both interbody cages “over the wire” and simple or screwed LLIF cages.
Section of the anterior vertebral common ligament to allow better corrections of the sagittal profile.
Excision of herniated discs occurs "inside-out," addressing both central-posterolateral and contralateral foraminal regions.
Endoscopic assistance for treatment of vertebral fractures.
Irrigation/debridement and/or evacuation of retroperitoneal or psoas hematomas or abscesses.
As a second approach to another lateral fusion in the same laterality.
Rescue of a lumbar fusion instrumented with a pedicle system without an interbody device and with signs of pseudoarthrosis.
Adjacent level fusion to avoid revision of the previous dorsal approach.
Finally, multiport work (lateral+ transforaminal + interlaminar) permits the separation of risks of isolated endoscopic decompression from the risks of introducing a cage. For example, in L3-L4 with severe stenosis and discopathy, the interbody cage can be introduced laterally with decompression performed interlaminar “over the top.”
Conclusion
In the current article, we present an endoscopic modification to the standard LLIF procedure. Advantages include smaller incision size, minimization of psoas retraction, ability to harvest iliac crest graft through the same incision, and the option of performing direct endoscopic contralateral foraminal decompression in the setting of an indirect decompression procedure. While specific materials need to be improved and developed to make this approach even simpler and more reproducible, the presented ELLIF has the potential for improved immediate patient outcomes and a wide range of applicability.
Footnotes
Funding The authors received no funding for this work.
Declaration of Conflicting Interests The authors declare that there are no conflicts of interest.
Disclosures The authors have no financial disclosures or conflicts of interest to disclose. Institutional Review Board and Research Ethics Committee approval were deemed not applicable for this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}