


Abstract
Background Microdiscectomy for patients with chronic lumbar radiculopathy refractory to conservative therapy has significantly better outcomes than continued nonoperative management. The North American Spine Society (NASS) outlined specific criteria to establish medical necessity for elective lumbar microdiscectomy. We hypothesized that insurance providers have substantial variability among one another and from the NASS guidelines.
Methods A cross-sectional analysis of US national and local insurance companies was conducted to assess policies on coverage recommendations for lumbar microdiscectomy. Insurers were selected based on their enrollment data and market share of direct written premiums. The top 4 national insurance providers and the top 3 state-specific providers in New Jersey, New York, and Pennsylvania were selected. Insurance coverage guidelines were accessed through a web-based search, provider account, or telephone call to the specific provider. If no policy was provided, it was documented as such. Preapproval criteria were entered as categorical variables and consolidated into 4 main categories: symptom criteria, examination criteria, imaging criteria, and conservative treatment.
Results The 13 selected insurers composed roughly 31% of the market share in the United States and approximately 82%, 62%, and 76% of the market share for New Jersey, New York, and Pennsylvania, respectively. Insurance descriptions of symptom criteria, imaging criteria, and the definition of conservative treatment had substantial differences as compared with those defined by NASS.
Conclusion Although a guideline to establish medical necessity was developed by NASS, many insurance companies have created their own guidelines, which have resulted in inconsistent management based on geographic location and selected provider.
Clinical Relevance Providers must be cognizant of the differing preapproval criteria needed for each in-network insurance company in order to provide effective and efficient care for patients with lumbar radiculopathy.
Level of Evidence 5
Introduction
Radiculopathy due to lumbar disc herniations is a common ailment affecting up to 5% of patients per year.1 A vast majority of these patients will have significant improvement in their symptoms with the implementation of nonoperative management.1–4 A subset of patients will have persistent radiculopathy and limitations in activity, despite a course of conservative management necessitating surgical intervention. Thus, the best management is observation and waiting for the first 6 weeks following onset. Evidence-based care path algorithms are critical to helping patients navigate the initial nonsurgical treatment course. Various stakeholders, including payers, societies, and the government, have created guidelines describing the appropriate interventions and duration of nonsurgical treatment of patients who have had lumbar radiculopathy. For example, such guidelines have been developed by the North American Spine Society (NASS) using a multidisciplinary, unbiased, evidence-based approach to spinal care in the United States (Table 1).3 All the guidelines are purported to be based upon scientific reviews of the medical literature, recommendations of practicing providers, or empirical evidence. Furthermore, some stakeholders, including NASS, invite public comment on draft guidelines and clearly disclose financial relationships that may create the appearance of a conflict of interest. Medical necessity criteria are a set of clinical conditions that must be met for payers to deem surgery appropriate. The variability in medical necessity criteria among payers results in varied patient treatment for the same pathology. Therefore, the purpose of the present study is to evaluate policy criteria in our geographic region (New York [NY], New Jersy [NJ], and Pennsylvania [PA]) for lumbar microdiscectomy (Current Procedural Terminology [CPT] 63030) and assess the consistency of requirements as compared with nationally based providers. All selected payers, including any contracted companies, will be compared with NASS recommendations for lumbar microdiscectomy.
NASS-recommended insurance coverage criteria for lumbar microdiscectomy.
Methods
A cross-sectional analysis of selected US national and local insurance companies was conducted in December 2021 to assess their policies on coverage recommendations for lumbar microdiscectomy (CPT 63030). Insurers were selected based on their enrollment data and market share of direct written premiums as reported by the National Association of Insurance Commissioners in their 2020 Market Share Report.5 The top 4 national insurance providers, in addition to the top 3 state-specific providers in NY, NJ, and PA, were selected. The selected national insurers composed roughly 31% of the market share in the United States. For states, the combined share of the selected national- and state-specific insurance providers was approximately 82%, 62%, and 76% of the market share for NJ, NY, and PA, respectively (Table 2).
Market share data for selected insurers.
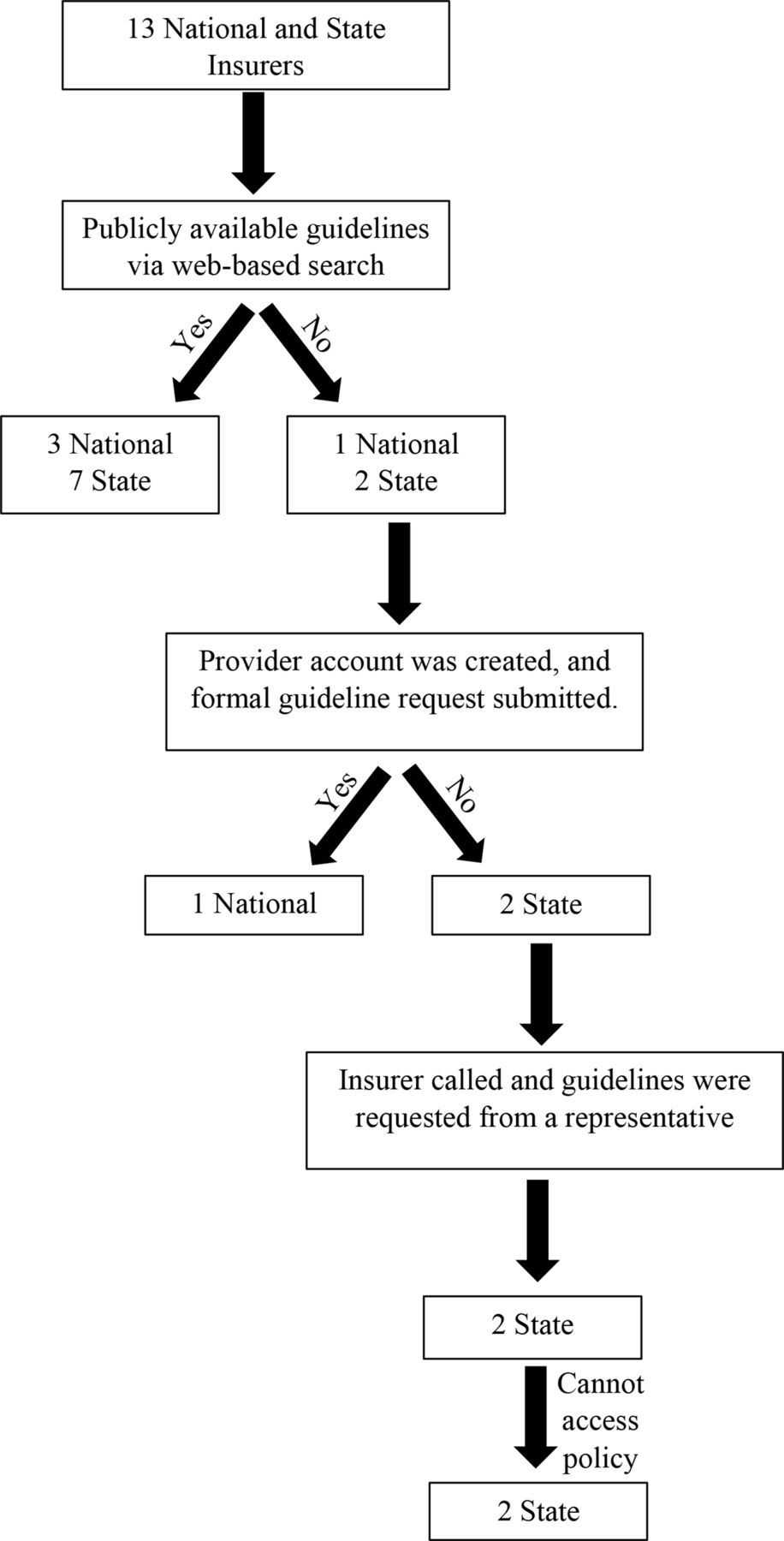
Insurance coverage guidelines and requirements were accessed through a web-based search of the selected insurers. If the guidelines were not publicly available, as defined by inaccessibility via the insurer website, a provider account was created, and a formal request was submitted. If the request remained unanswered, the insurance provider or contracted company was called. The representative confirmed the presence or absence of specific guidelines for the CPT code under investigation. Finally, if no policy was provided, we documented it as such (Figure).

Flow chart depicting study methodology.
Categorical data were compiled into a spreadsheet that outlined specific coverage requirements for each insurance company (Table 3). We then compared the different preapproval criteria for the selected insurers to assess for discrepancies between insurance companies. Additionally, criteria for each insurer were compared with the current coverage recommendations for lumbar microdiscectomy (CPT 63030) as outlined by NASS. Data were compiled into a preformatted spreadsheet, and descriptive analysis was performed using Microsoft Excel (version 16.33; Microsoft Corp., Redmond, WA) as seen in Table 4. These 13 subcategories were consolidated into 4 main categories: symptom criteria, examination criteria, imaging criteria, and conservative treatment (Table 5). Urgent and emergent indications were not considered as preapproval is typically not required.
Criteria for determining insurance coverage by insurance provider.
Criteria categories needed for coverage by recommendation set.
Eligibility criteria for each insurer and analysis of agreement between insurers.
Results
A total of 13 insurance companies were selected for inclusion in this study. Eight providers contracted with outside companies to establish and manage their surgical eligibility criteria, 4 established their criteria from within their own system, and 1 had no preapproval criteria (Table 6). Three (23.1%) of the 13 insurance companies did not have publicly available data, 2 of which contracted Orthonet from whom all attempts at obtaining preapproval criteria were unsuccessful. Kaiser is the only provider with no preapproval criteria required, making it the sole provider that is less restrictive than the NASS recommendations. United Healthcare uses the NASS criteria apart from 9 states, 2 of which were NJ and PA. Therefore, for the purpose of this study, none of the selected insurers had complete consensus with the NASS eligibility criteria.
Insurance guidelines and availability.
Physical Examination and Symptom Criteria
Symptom criteria were quite varied with 73% of companies having more requirements than NASS and only 55% agreement among providers. Evicore, the most contracted company, required documentation of neurogenic claudication affecting activities of daily living (ADL) daily, with a VAS pain score of 7 or greater and recent imaging that is concordant with patient’s symptoms. American Imaging Management (AIM) Specialty Health, the second most common contracted company with publicly available guidelines had similar, albeit less restrictive, criteria. They require documentation of VAS pain >3 that results in an inability to perform 2 or more ADLs.
Lifetime Healthcare Group (NY) and UPMC (PA) were the only 2 state-specific companies that established their surgical guidelines internally. Lifetime Healthcare Group requires a documented positive nerve root tension sign on physical examination with associated motor, sensory, or reflex changes. UPMC is the only group requiring either myelopathy or hyperreflexia as well as pain that affects ADLs with accompanying motor or sensory changes.
Aetna and United, both of which are national providers, also establish their surgical guidelines in-house. Aetna requires documentation of radiculopathy or neurogenic claudication associated with the levels being treated. While United uses NASS criteria for 41 states, the remaining 9 states, 2 of which are NJ and PA, have unique guidelines that were not accessible despite multiple inquiry attempts.
Imaging Criteria
All insurance companies, regardless of whether guidelines were established in-house or by a third-party company, require magnetic resonance imaging (MRI) or computed tomography scan that is concordant with the patient’s symptoms. While NASS states decompression is indicated when imaging confirms neurological compression on cross-sectional imaging, no descriptive or quantitative parameters are provided. Evicore requires imaging within 6 months. AIM Specialty Health specifies that if there is a discrepancy between the radiologist interpretation and surgeon interpretation, the radiologist will take precedence. Lifetime does not specify a timeframe for patient imaging, and UPMC and Aetna require that the stenosis be categorized as moderate to severe.
Conservative Treatment
There is consensus among all providers regarding exemption from physical therapy (PT) in the setting of adequate documentation. Despite this single point of agreement, the definition of conservative therapy varied significantly from the NASS recommendations with 91% of providers having more restrictive requirements. Evicore, AIM Specialty Health and Lifetime Health Care Group had complete consensus in their definition of conservative management, which includes 6 weeks of PT as well as 2 of the following complementary treatments: (1) prescription strength analgesics, (2) steroids and/or nonsteroidal anti-inflammatory drugs, or (3) epidural steroid injections. Interestingly, these 3 sets of guidelines conflated PT, chiropractic treatment, and manipulative treatment modalities. Aetna’s guidelines are more restrictive than NASS and the previously mentioned companies as the PT is required to be in-person with proof by either visit notes or patient claims history. Aetna also requires the use of both anti-inflammatory medications and tricyclic antidepressants. UPMC is the only provider that requires 12 weeks of conservative therapy to include in-person PT and anti-inflammatories or analgesics.
Discussion
Lumbar spinal stenosis with associated radiculopathy is a common pathology affecting approximately 5% of all low back pain diagnoses.1 Ninety percent of these patients will have resolution of these symptoms with conservative management.1 It is widely accepted that urgent, or emergent, surgical decompression is indicated in the presence of red flag symptoms including cauda equina, acute motor or sensory loss, fracture, infection, and tumors. In efforts to streamline and standardize patient care, NASS provided evidence-based clinical practice guidelines for the management of lumbar disc herniations with radiculopathy.3 While identifying specific patient factors that predispose failure of nonoperative treatment, the literature has proven improved patient outcomes in patients that fail conservative management.6–9 Although a relatively uniform data source informing the treatment of lumbar disc herniations including prospective, level 1 studies exist, there is significant variability among various insurance payers and informatics companies in the criteria for lumbar discectomy in the setting of a lumbar disc herniation. Despite herculean efforts to provide the best treatment for patients by establishing societies, such as NASS, the American Medical Association, the American Society of Plastic Surgeons, and many others, there is 1 common obstacle to implementing well-developed evidence-based guidelines: insurance companies. While this obstruction to patient care has been documented in other fields,10–12 to our knowledge, this is the first study reporting on insurance guidelines in orthopedic surgery.
The NASS guidelines were formulated utilizing a rigorous 11-step process including an exhaustive literature review on the management of lumbar disc herniations with radiculopathy.3 These guidelines were established to allow all physicians to treat patients with the most up-to-date information on all aspects of diagnosis, including nonsurgical and surgical management. This, in effect, eliminates the variability in patient care and theoretically should provide a basis for defining “medical necessity” when conservative therapy fails. Unfortunately, providers define “medical necessity” based on either a third-party contracted company or in-house parameters as opposed to strictly following medical society guidelines.
Consumers are posed with a difficult task when choosing insurance coverage from the menu of available providers. The average consumer prefers higher-quality health insurance plans with lower monthly premiums.13 However, consumers may be more willing to pay higher premiums for plans that cover care from their personal doctor.14 With a multitude of options, it has become increasingly challenging for consumers to select their ideal plan. The Affordable Care Act mandated that policymakers provide clear and simple benefit descriptions to mitigate this problem.15 Nonetheless, selecting a health insurance policy is complex and requires understanding of insurance terminology to properly compare plans appropriately.16 In a study by Loewenstein et al, only 14% of consumers were able to correctly answer 4 multiple-choice questions regarding basic components of traditional health insurance design.17 The lack of a basic understanding of health insurance seems to be the biggest barrier to consumers making sound decisions regarding health insurance selection.18 If patients were to attempt to compare surgical guidelines for an ailment, in this case, lumbar spinal stenosis with radiculopathy, they would be faced with an even more complicated situation due to the substantial variability among providers. None of the insurance companies evaluated in this study reached an 80% consensus with one another. The highest consensus among insurers was in the imaging and conservative treatment criteria at 73%. There was a considerable range of variability (18%–91%) as compared with NASS criteria, with imaging criteria having the most agreement with medical society guidelines (82%) and conservative management having the least (9%). Furthermore, some insurance providers’ guidelines are inaccessible. This is particularly problematic as it may result in patients electing a more expensive plan in hopes of having their surgery covered by their provider.
Aside from the lack of transparency, several of the assessed guidelines include criteria that appear to be based on no current literature recommendations. For example, AIM Specialty Health requires a VAS pain score of 3 or greater to be documented, while Evicore and Lifetime Health Care require a VAS pain score of 7 or greater for prior authorization of surgical intervention. NASS has no such threshold, which is reflected in the guidelines provided by UPMC, Aetna, and United Health Care. In a randomized controlled trial by Heyward et al,10 a visual analog score of 6.7 was more predictive of surgery as compared with that of 6.4 in the nonsurgical group, which did not hold true at 1 year postrandomization. They did determine, however, that surgery lead to faster relief of their radiculopathy.19,20 A single article identified from the Netherlands looking at 9 Dutch hospitals found that a VAS of 7 was a significant predictor for poor outcomes with conservative management at 5 years.21
Furthermore, arbitrary determinations by insurance companies were found in both imaging interpretation and minimum time of conservative management required. For example, both UPMC and Aetna require that the stenosis found on MRI be categorized as moderate to severe, yet a study performed by Gupta et al demonstrated that the percentage of the spinal canal occupied by a herniated disc does not predict who will fail nonoperative treatment and require surgery.22 Additionally, one contracted company (AIM) specifically indicated that if there is a discrepancy between the radiologist and surgeon interpretations of a patient’s MRI, the radiologists read will take precedence. This specification seems subjective as the literature has found no such difference between these 2 specialties.23 We also noted a substantial deviation from the NASS recommendation of 4 weeks of conservative management. United Health Care was the only provider out of the 13 assessed that also required only 4 weeks. Evicore, AIM Specialty Health, Lifetime Health Care, and Aetna all required 6 weeks of conservative therapy for surgical preapproval and UPMC required twice that duration (Table 3). The findings by Parker et al confirmed these recommendations, indicating that patients with lumbar disc herniations who failed 6 weeks of nonoperative management are better served with surgical intervention.24
It is important to note the difference in how insurers define conservative therapy as this directly impacts which treatment modalities a patient can be offered in clinic. Per the NASS recommendations, conservative therapy should begin with 4 weeks of PT and adjunctive treatments, such as chiropractic care or epidural steroid injections, may be added.3 While there was consensus among insurers regarding exemption from PT, no such agreement was seen regarding the inclusion of PT in the conservative management algorithm. UPMC is the most stringent in their definition of conservative management requiring 12 weeks of PT, epidural steroid injections, and prescription strengthnonsteroidal anti-inflammatory drugs or pain relievers. Lifetime Health Care, United Health Care, and the 4 companies contracted with Evicore include PT as an option for conservative therapy; however, their guidelines conflate PT, chiropractic manipulation, and osteopathic manipulation (Table 7). This is most consistent with the landmark Spine Patient Outcomes Research Trial (SPORT), which required 6 weeks of conservative management for inclusion in their randomized controlled trial.25 Their nonoperative protocol consisted of active PT, counseling with home exercise instruction, and NSAID use if not contraindicated.25
Components of conservative therapy.
After an exhaustive search on Thomson Reuters Westlaw, a federal statute that took effect in 2014 mandated that criteria for medical necessity determinations be made available by the insurance provider to any “current or potential participant, beneficiary, or contracting provider upon request.”26 This statute also indicated that prior authorization is not needed for any mental health or substance abuse treatment. Interestingly, no such laws exist for medical or surgical procedures. While the implementation of medical necessity determinations was in part meant to minimize wasteful services, they are ungovernable and result in disparate treatment.27 Unfortunately, with such heterogeneity in coverage, patients with the same disease process may receive different treatments based on their geographic location and selected insurer. This study sheds light on the current landscape of orthopedics and insurance companies in the tristate area. Due to the variability in required documentation for preapproval of surgical decompression, surgeons should attempt to obtain the surgical guidelines and definitions of medical necessity for all in-network companies in hopes of minimizing delay in treatment as surgery before 6 months leads to faster recovery and improved long-term outcomes.19,28–30 Unfortunately, the office staff may not be able to obtain these documents from some insurers and third-party contractors, adding an undue complexity and delay to the preapproval process.
Conclusion
Consumers are faced with a dilemma in choosing the insurance company and unique plan for coverage. Even with an increasing level of literacy among patients, the lack of transparency and availability of medical necessity criteria compound this problem. Although surgeons use evidence-based medicine in patient management, they should be cognizant of the preapproval requirements imposed by the most encountered providers in their practices to minimize delays in patient care as a result of insurance denials. Policymakers should hold insurance companies accountable for providing clear and standardized preapproval criteria that are both transparent and easily accessible by patients and physicians alike.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.