


Abstract
Background Patients with radiculopathy caused by contained disc herniations are less likely to have good outcomes following discectomy surgery than patients with disc herniations that are not contained. The author presents his 4-year results from a prospective trial regarding the efficacy and safety of a tubular transforaminal radiofrequency-assisted manual decompression and annulus modulation of contained disc herniations in 58 patients.
Methods Fifty-eight patients with lumbar radiculopathy due to a contained disc herniation were enrolled in a prospective clinical study. Visual analog scores (VAS) for back pain and leg pain, quality of life assessment, Macnab criteria, and SF-12 were collected from patients before treatment, at 2-years and 4-years post-treatment.
Results At 4 years, results were obtained from 47 (81%) of patients. Compared to mean pre- treatment assessments, mean 4-year VAS for back pain improved from 8.6 to 2.3 points, and mean VAS for leg pain improved from 7.8 to 2.3. Eighty-three percent of respondents reported that they were “satisfied” or “very satisifed” with their quality of life at 4-years as per SF-12. At 4 years, recurrence was noted in 3 (6.4%) of respondents and no complications were reported.
Conclusions The 2-year and 4-year study results are nearly identical, suggesting durable benefit out to 4 years. These results also suggest that in carefully selected patients with sustained contained disc herniations who have failed conservative treatments, manual decompression combined with radiofrequency-assisted decompression and annulus modulation are very likely to have good outcomes 4 years post-treatment.
- discectomy
- nucleotomy
- contained disc
- disc decompression
- back pain
- degenerative disc disease
- microdiscectomy
Introduction
Disc abnormalities causing low back and/or leg pain (lumbar radiculopathy) are associated with enormous costs to society because they are extremely common and potentially debilitating. Approximately eighty percent of the population of industrial societies will be affected during their lifetime.1 Over the last several years, the surgical treatment of lumbar disc abnormalities has dramatically increased worldwide, with wide variation among regions attributed to (among other factors) differences in reimbursement, technology, and culture.2, 3
The increasing number of spinal surgeries is related to several factors including aging populations and more sensitive diagnostic tools.4
Common spinal disorders of back and leg pain, are due to degeneration of lumbar vertebral discs. Painful abnormality of discs is usually caused by herniation of the nucleus pulposus due to inflammation and/or compression of nerves. Fortunately, sixty to eighty percent of patients with acute painful disc herniations get better within six to twelve weeks without treatment.5, 6 Among those who do not improve, conservative treatments often succeed in getting most patients back to work or other related activities.7–9
Contained disc herniations are thought to cause leg and/or back pain when the nerve roots become irritated by nucleus material within the posterior annulus. Beside anatomical and patholgical studies this has been demonstrated with endoscopic visualization by T. Yeung.10 Disc herniations cause back and/or leg pain when a spinal nerve root becomes inflamed and/or compressed as it passes adjacent to the herniated disc. Clinical findings linked to disc herniations have significant symptoms due to different patho etiologies. The etiologies of disc pain, versus radicular pain, versus pseudo-radicular pain are not clearly understood.11–15
In recent years, minimal invasive techniques have emerged to treat patients diagnosed with disc herniations that cause both back and/or leg pain. They are intended to relieve pain or improve a neurological deficit causing functional limitations. The concept is to reduce tissue damage, scar tissue formation, and nerve root irritation while achieving good clinical outcomes when compared to conventional surgery. The goal of all these techniques is to close the gap between failed conservative treatment and open surgery, especially for contained herniated discs.16–27
Every technique should be evaluated and compared to the results of the existing standards and should focus on causing less trauma, less scarring in the epidural space which may become clinically symptomatic.28–31
The treatment studied and under review is a microtubular discectomy system indicated to treat patients suffering from: intractable back and/or leg pain, numbness, and/or cramping in the legs; secondary to a diagnosis of a symptomatic disc herniation with integrity of the posterior ligament while not responding to conservative treatment.
This procedure combines multiple treatment options that include manual discectomy augmented by radiofrequency-assisted nucleus ablation, annulus modulation and irrigation of the disc.
The purpose of this study is to investigate the long term outcomes of this microtubular procedure compared to published long term results of standard discectomy techniques. Similar outcomes from surgery for contained hernias are still not universally achieved due to their challenging nature.32
With this technique the hope was to show outcomes that were at a minimum equivalent to open surgery for cases of contained hernias, while causing less trauma to the patient.
Materials and Methods
All surgeries were performed by one surgeon between 2006 and 2008. 58 patients were enrolled in this prospective cohort outcome evaluation study. The study was discussed and approved by an internal commission from the hospital to check GCP practise. The average age of the 47 participating patients at the time of the index procedure was 43 years; range 24-67 years. 15 (32%) were female, 32 (68%) were male. Sixty-nine levels were treated during the index procedure. The number of procedures per level are as follows: L1-2 (n=1), L2-3 (n=1) L3-4 (n=5), L4-5 (n=31), L5-S1 (n=31).
Inclusion criteria
Inclusion criteria included concordant symptoms (leg, buttock, or groin pain with a VAS >5, numbness and/or cramping, with or without back pain) caused by a contained protruded lumbar disc (with an intact annulus fibrosis) or sometimes bulging black disc confirmed by imaging studies (MRI and/or CT). The precondition for a contained hernia was defined as: slipped nucleus material was within an intact outer annulus or a capsule composed of the outer annulus and the posterior longitudinal ligament, independent from the size of the protrusion but not in direct contact with epidural tissue shown in the images. Further in most cases a discography was performed prior to the surgery to exclude cases with epidural leakage of contrast, though a discography in of itself was determined not to be necessary in order to be part of the study and not used to confirm the source of the pain. The important point was that annular integrity was shown.
All patients signed an informed consent. Patients aged 18 to 68 years old were enrolled. 58 patients who met the inclusion criteria were treated with the same technique by a single surgeon (author) at one institution over the course of 18 months. These patients were followed out to two years and four years after the index procedure.33
Although no minimum duration of symptoms was established as a criterion for inclusion, in each case, the treating surgeon determined that not only were the symptoms of sufficient duration to warrant surgical intervention (usually, at least six weeks) but that the patients had also demonstrated failure to respond to conservative treatments (including but not limited to documented treatment by a licensed physical therapist experienced in treating disc herniations, and a minimum of at least two trials of epidural steroid injections).
Exclusion criteria
Exclusion criteria included patients who exhibited any of the following: progressive neurological deficits, sequestrations of HNP, severe stenosis, fracture, tumor, severe disc degeneration, disc collapse > 50%, clinical evidence of cauda equina syndrome, and fixed motor deficit. Patients with segmental instability shown by advanced osteochondrosis or spondylosis (Modic signs II or more) or listhesis were not considered (Table 1).
The patients were evaluated pre-surgery, post-surgery, at 1 and 6 weeks by the surgeon to control surgery related complications as well as at 3, 12 and 24 months by questionnaire.
Out of the total population from an earlier investigation at 2 years, all of the patients who were fluent in German (N=58) were enrolled in this > 4 year prospective cohort outcome evaluation study by an independent research organization.
Questionnaires sent to these patients were based upon the current life situation of the patients regarding the past 4 weeks prior to the follow-up after 4 years postoperative and evaluated the following parameters: (a) individual analysis of complications (b) recurrence (c) back and leg pain according to a 0 (no pain) to 10 point (unbearable pain) VAS scale (d) subjective patient satisfaction; grading the results of the operation as: excellent, good, fair or unsatisfied (e) subjective grading of sensibility disturbance: Lower Extremity Paresthesias (f) subjective grading of leg strength: Lower Extremity Strenght (g) bodily capacity according to Macnab : Lifetime Satisfaction, (h) SF-12.
Surgical Technique
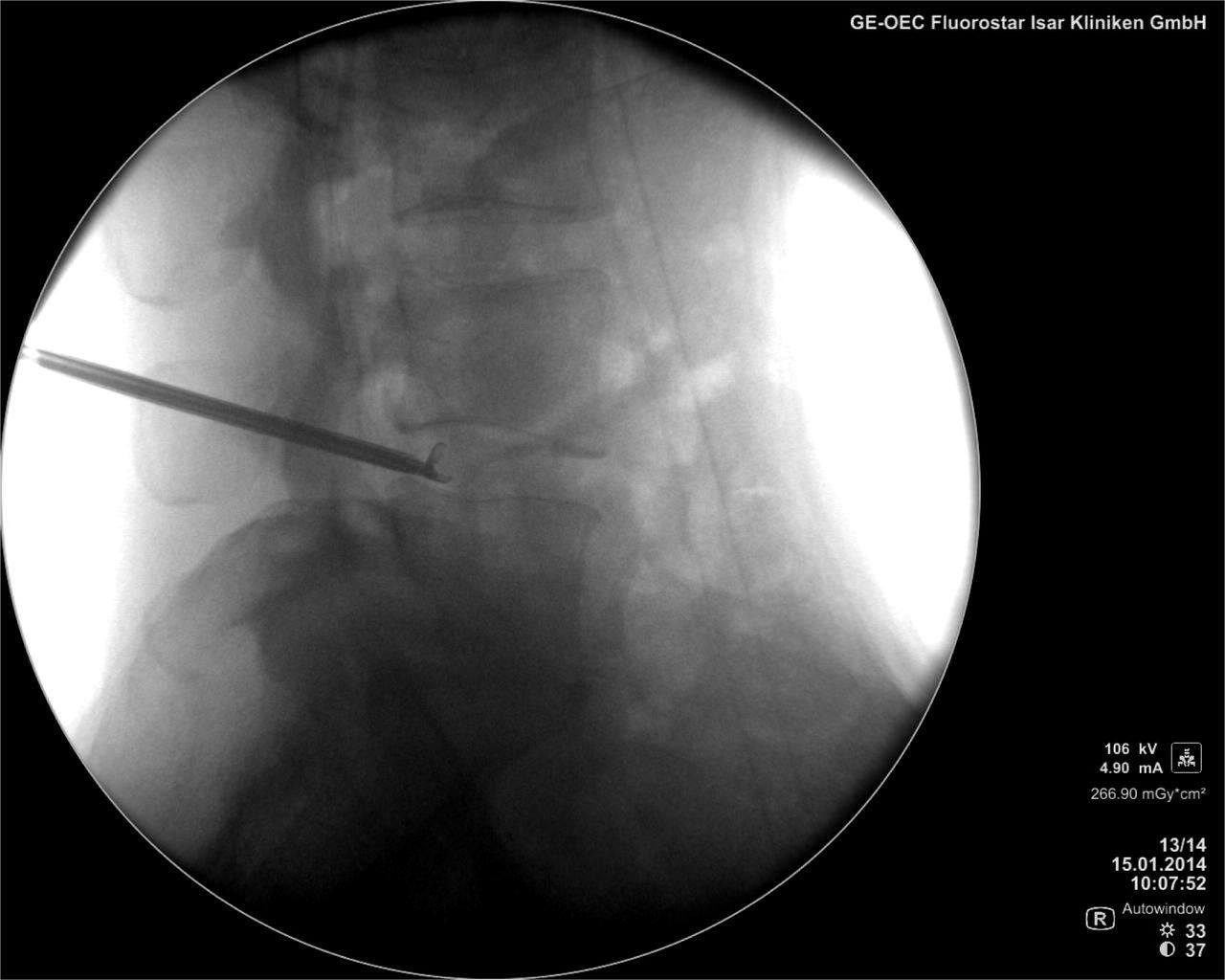
Procedures were performed via posterolateral approach, using 1% lidocaine at the entry point, 0.5% Mecaine (Marcaine) near the facet (patients were positioned either prone or in lateral decubitus position—symptomatic side up). Fluoroscopic imaging was used to measure and mark an entry point on the skin so that the posterolateral annulus fibrosis at the affected level could be targeted via a transforaminal trajectory. Sterile preparation and draping of the skin incorporated the entry site, and this area was infiltrated with local anesthetic. A 16G x 8 inch needle is passed under sequential fluoroscopic guidance into the annulus fibrosis. The general target is to place the tip of the needle at the inner pedicle line in A/P fluoroscopic imaging, while at the same time be in the posterior 1/3 of the disc in Lateral fluoroscopic imaging. The stylet is removed and a flexible, blunt guide wire is passed through the needle and beyond the needle tip into the nucleus pulposus. The needle is removed leaving the guide wire in place. Once this step is completed, a dilator is passed over the guide wire and a microtubular system is advanced over the dilator on the outer annulus. With the microtubular system in a fixed position against the annulus, the dilator is removed and a trephine is used to perform an annulotomy over the slipped nucleus. All of these steps were performed with fluoroscopic imaging in awake patients to provide feedback to the surgeon. Patients were instructed to notify the surgical team if they experienced any pain or paresthesia during the procedure. In order to avoid nerve root irritation, patients were frequently questioned during the procedure about any sign that might be interpreted as an indication of pain.
The cannula can be fixed using a depth stop and an initial decompression of approximately one cubic centimeter of intradiscal nucleus material is performed using a pituitary grasping forceps. This is followed by inserting the Trigger-Flex Bipolar System device to ablate the nucleus using high-frequency-low temperature radio energy. This special waveform produces controlled localized heat that ablates the nucleus material and further helps free up herniated disc material that can be removed with the pituitary grasping forceps.
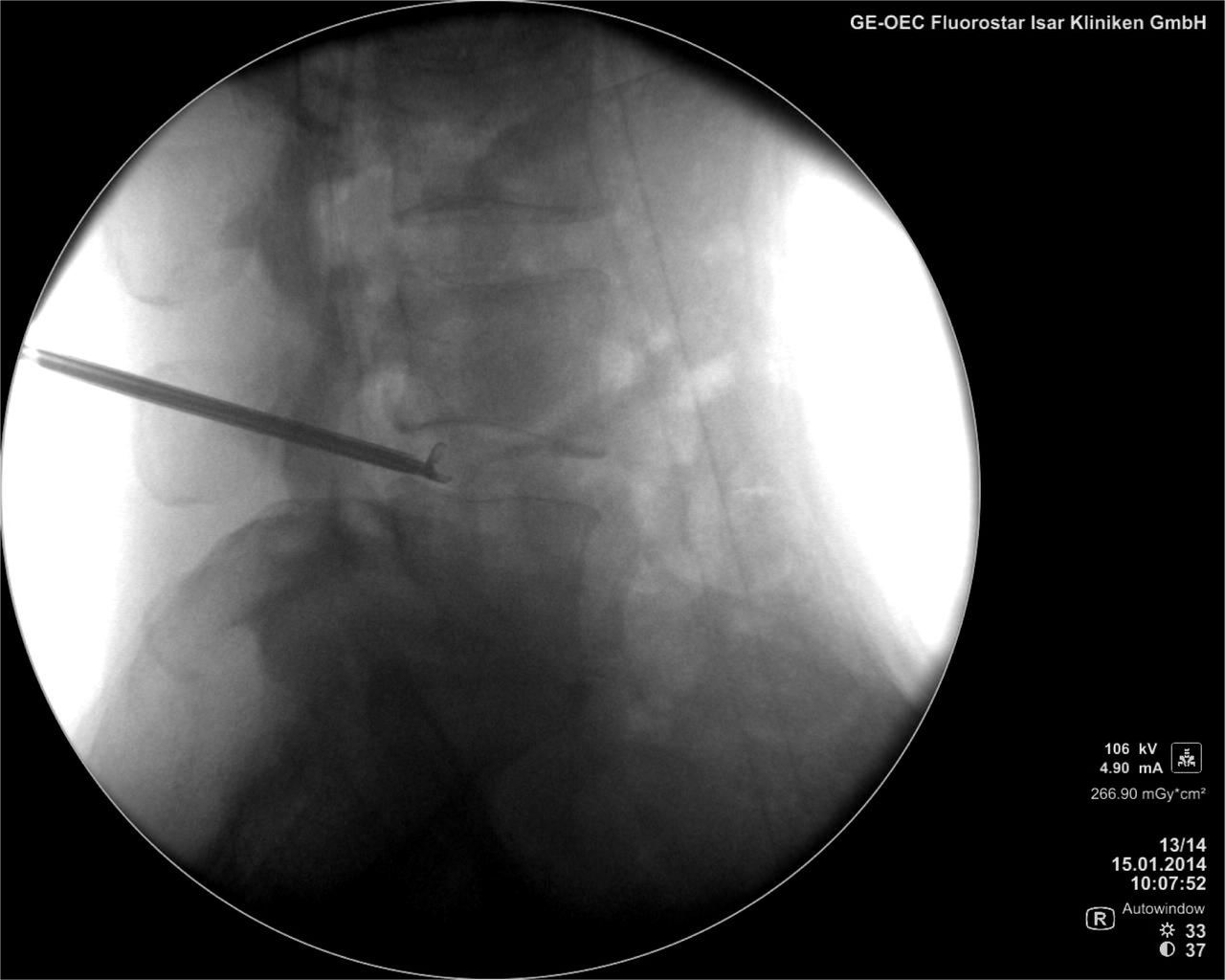
Fluroscopic Picture
Saline is applied during the nucleus ablation to irrigate the system. The cannula is then pulled back into the outer annulus in order to shrink and stabilize the annulus with the Trigger-Flex using a special Bipolar Hemo waveform. Subsequent extraction of nucleus material is performed with the grasping forceps if necessary.34 Total delivery of energy to the nucleus and annulus should be limited to 6 applications of 6 seconds each, at a power setting of 25 on both Bipolar Turbo and Bipolar Hemo. It is important that the bipolar electrode does not touch the endplates during application.
For postsurgical care patients were given a de-lordotic brace for 4 to 6 weeks to reduce the posterior load in the disc during the healing, as well as stabilizing exercises after 2 weeks.
Primary endpoints of this survey were: subjective life improvement, Visual Analog Scale (VAS), SF-12 Health Survey, Macnab questionnaire, recurrence rate all compared to the earlier evaluated findings.
The secondary endpoints were operative complications.
Statistical Methods
Though we acknowledge that due to the small sample size statistical significance cannot be adequately determined, we nonetheless felt that by doing a statistical analysis we would obtain a baseline against which we can compare later data.
Explorative statistical data analyses was performed using Microsoft Access (Microsoft, Corp.,Redmond, WA) and SPSS software (version 16.0;SPSS Inc. Chicago, IL).
SPSS descriptive statistical analysis showed no normally distributed population p<0,05 for both VAS leg and back pain (metric scale). The results obtained were analysed using:
Wilcoxon test was used for statistical analysis -> dependent sample -> not normally distributed.
Kolmogorov-Smirnov test for dependent sample was used, with significance acceptance at p< 0.001
The author was not involved in the collecting or evaluation of this data.
Results
Of the 58 patients initially enrolled in this prospective outcome study clinical results from 47 patients (81%) were available for review at 4 years. 9 patients could not be located, 1 patient died after 3 years for reasons unrelated to surgery.
Complications: As in the previous evaluations at 6 months and 2 years, no complications were reported.
Early Recurrence: Three patients (6,4%) required additional microsurgical treatment less than six months after the index procedure. The timing of the onset of recurrent symptoms: 4 weeks (n=1); 6 weeks (n=1); and eleven weeks (n=1). Results in these three patients after the second procedure were deemed to be “very good”.
Late Recurrence: Three patients (6.4% of respondents) reported symptoms that required additional surgical treatment more than six months after the index procedure. The first of these three patients initially refused open fusion surgery and chose instead to try radiofrequency intradiscal decompression treatment for intractable back pain and so was enrolled in this study. Twelve months after the index procedure, this patient was treated with a two-level instrumented posterolateral fusion at L3-4 and L4-5 for continued axial back pain. The index procedure in the second patient included treatment at two-levels (L3-4 and L4-5). At 15 months after the index procedure, the patient experienced new symptoms and imaging confirmed reherniation of the in L4-5 disc on the same side as the index procedure. This patient was treated with endoscopic discectomy and was deemed to have a “good” result from the second procedure. The third patient showed a recurrent extruded disc herniation 24 month after the index procedure and underwent microdiscectomy without a significant change in his symptoms.
In 87% of the patients an open surgery was therefore successfully avoided.
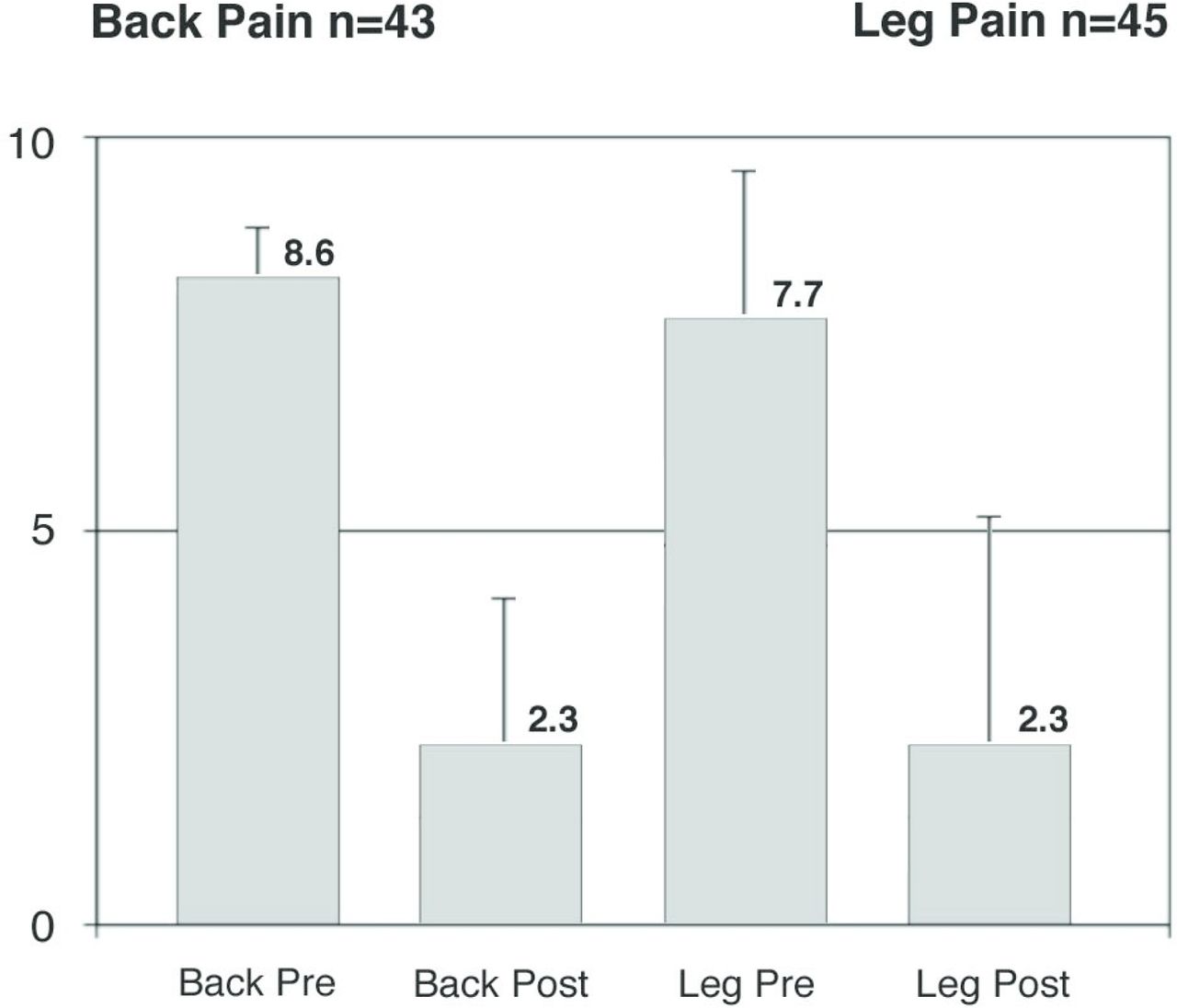
VAS Back Pain: In 47 patients, mean VAS scores improved from a pre-treatment (baseline) of 8.6 (s.d. ±1.26) to 2.3 (s.d. ± 2.32) four-years after the index procedure (P>0.0001) using Kolmogorov Smirnov test for dependent sample. Forty-six patients reported decreased VAS back pain scores; one patient reported increased VAS back pain score: pretreatment score 7 increased to 8 after four years.
Subjective patient satisfaction
VAS Leg Pain: 43 patients reported leg pain before the index procedure. The mean VAS leg pain score decreased from 7.8 (s.d. ± 1.86) to 2.3 (s.d. ± 2.77) at four-years after the index procedure (P>0.0001) using Kolmogorov Smirnov test for dependent sample. 42 patients reported decreased VAS leg pain scores; one patient in the recurrence group reported increased VAS leg pain score: pretreatment score 7 increased to 8 after four years.
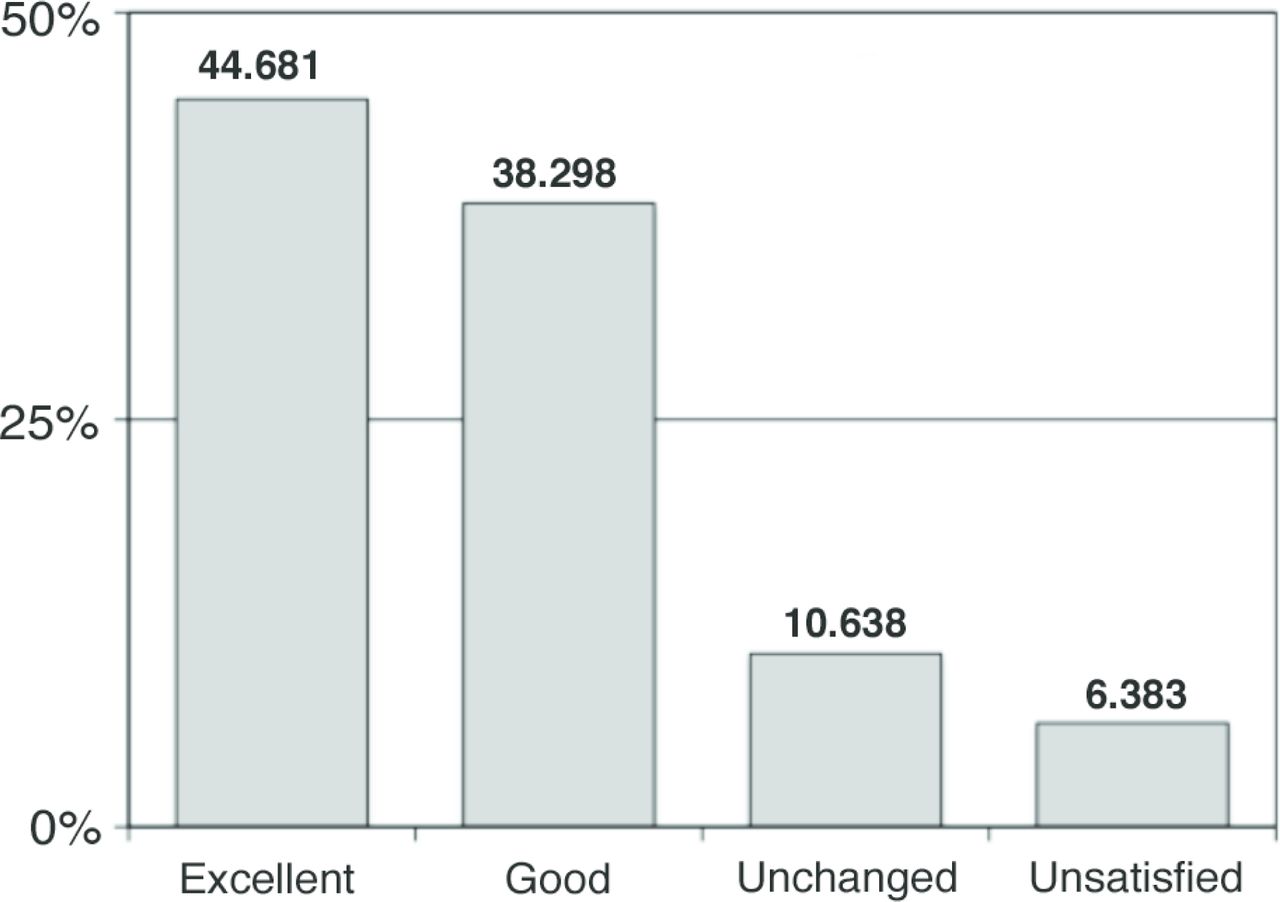
Patient Satisfaction: 47 patients reported their satisfaction with the index procedure after four years according to one of four categories: very satisfied (n=21 or 45% of respondents), satisfied (n=18 or 38%), neutral (n=5 or 11%), or unsatisfied (n=3 or 6%). Among three unsatisfied patients, two provided explanations for their disappointment: one experienced no relief of back pain after the index procedure and went on to be treated (unsuccessfully) with a two-level posterolateral instrumented fusion by a different surgeon. Another patient experienced a recurrent disc herniation (late reherniation) requiring microdiscectomy.

VAS Back and Leg Pain
Lower Extremity Paresthesia: 40 patients reported lower extremity paresthesia before the index procedure. Patients reported lower extremity paresthesia four years after the index procedure according to one of four categories: fully recovered (n=25 or 63% of respondents), improved (n=9 or 23%), unchanged (n=5 or 13%), or worse (n=1 or 3%).
Lower Extremity Strength: 38 patients reported subjective lower extremity weakness before the index procedure. Patients reported lower extremity weakness four years after the index procedure according to one of four categories: fully recovered (n=18 or 47% of respondents), improved (n=13 or 16%), unchanged (n=6 or 16%), or worse (n=1 or 3%).
Lifetime Satisfaction: live with this situation for the rest of your life N=47
The quality of life score showed that 83% were satisfied with their current quality of life.
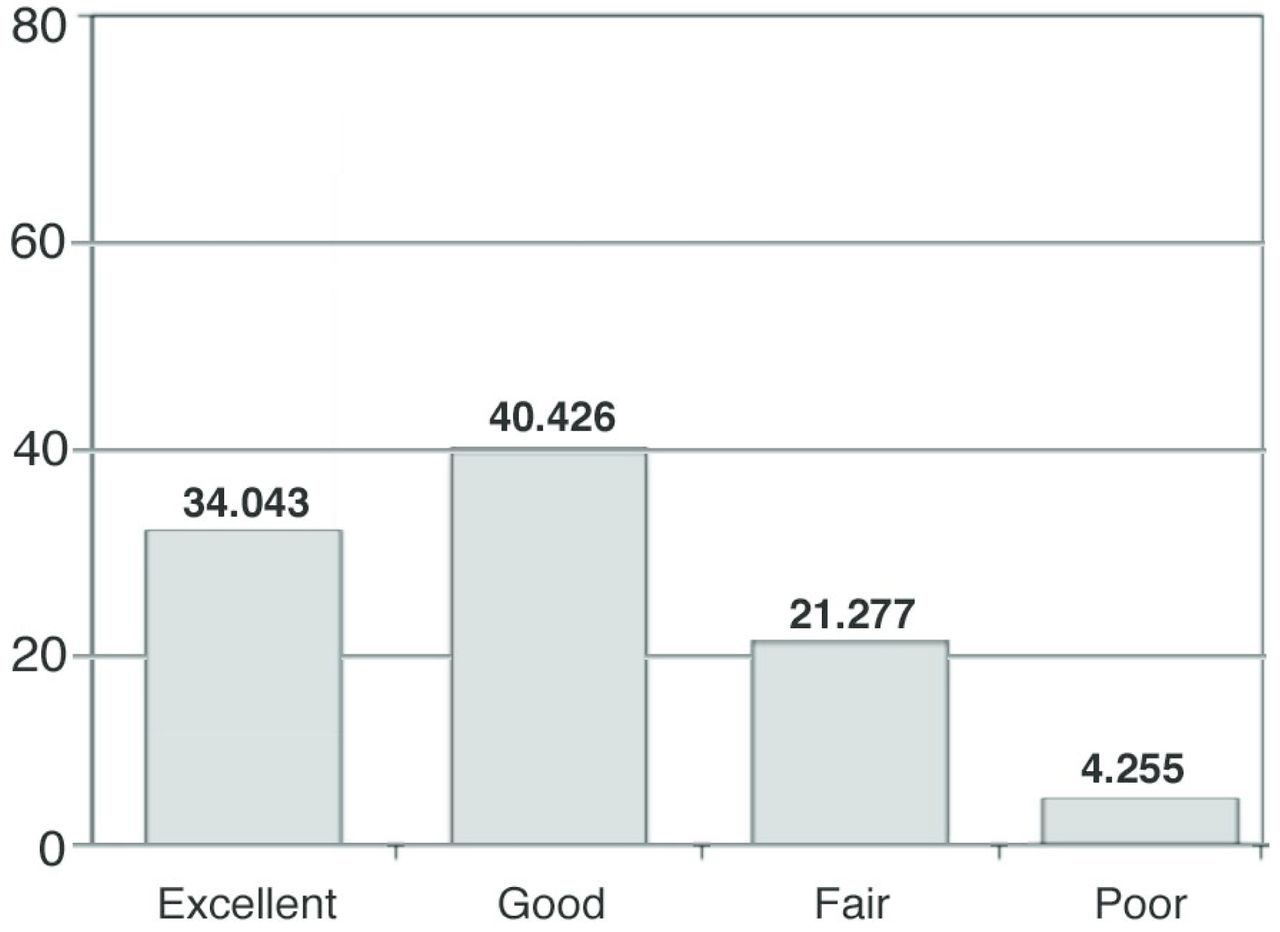
body capacity according to Macnab N=47
In regards to SF-12, Macnab, patients also showed very steady and promising results. 16 patients reported an excellent result with a fully regained body capacity (34%), 19 patients reported a good result with minor restrictions (40.4%), 10 patients reported a fair result with restrictions in their body capacity (21.3%) and 2 patients reported poor results with no or insufficient improvement (4.3%). According to the Macnab criteria a satisfactory result was also registered in 95.3%.

Macnab at 4 yrs (N=47)
Discussion
A previous evaluation of a multicenter study with the device under investigation showed very promising results at 6 months.35 A further investigation of patients from one site at two years confirmed these findings, showing no significant changes and a stable patient outcome.28
The device used in this study is designed as a microtubular discectomy system to treat patients suffering from spinal pain caused by a disc herniation. It is the author‘s belief that this procedure should be placed in the cascade of treatment options for disc diseases: after failed conservative treatment and before open surgery.
If patients do not respond to conservative treatment and the symptoms do not allow them to follow their normal daily life activities within a certain time, very often a more aggressive therapy is demanded and considered.
Currently, patients presenting radicular low back pain not responding to conservative treatment are most commonly treated by open or microsurgical discectomy. If further degenerative changes are present maybe even a fusion surgery is required. As previously stated, there is a constant increase in the number of these surgeries in developed societies, which is associated with an increase of costs. Hout and Peul et al. evaluated the cost efficacy of early surgery to be an extremely expensive method from a health care economic perspective.36
The complications after a standard microsurgery have been described up to 8% with haematoma 0.05%, incidential durotomy 3.3%, nerve injuries 4.5%, cauda equine syndroms 0.05% and epidural fibrosis.37
In addition to clinical outcomes, consideration of trauma caused by an approach and potential complications are important factors for assessing the value of a surgical method. All studies on Disc-FX or similar procedures have shown that the risk of any kind of complication is clearly decreased compared to open techniques.
While open surgery seems to be an unsatisfactory and too invasive treatment for patients with contained hernias, a small lateral approach can be a promising alternative if conservative therapy fails or symptoms are ongoing for a long time in these cases.
Using the extensive experiences from minimal invasive procedures, such as the endoscopic procedures, especially the SED System by Tony Yeung with the experience of thermal annuloplasty, the Disc-FX System was developed in the hope of addressing the unsatisfactory clinical outcomes for contained herniations. The positive effects of high radiofrequency have been proven in endoscopic spine surgery as well in neurosurgical applications already. Additionally, the knowledge gained from single percutaneous applications like Nucleo- and annuloplasty was used.38–40 As shown in the full endoscopic techniques, the combination of different steps improves the outcome.41 Other authors have also demonstrated that a combination of different procedures can be helpful.42–48
The technical aspects and the basic surgical technique for this procedure have been very well investigated in several independent pre-clinical testings.33 However to prove a technique to be equivalent to the accepted existing treatment options, outcome and the patient's satisfaction in a long period are important. Comparing the outcomes, reoperation and complication rates to the standard open surgery, the existing study shows that the combination procedure causes less trauma, delivers significant pain relief and should be considered as an alternative treatment in the presence of contained hernias.15, 16, 50
Compared to the published literature of results for open surgery in the presence of contained hernias, this technique seems to be more than equivalent. A direct comparison of this microtubular technique to open surgery for discal hernias has been published by Liao Xiang.51 The paper quotes that at 12 months both groups showed comparable outcomes in VAS and ODI.
Looking at an overview of open as well as percutaneous studies, this technique demonstrates equal results to open techniques for contained hernias and superiority to percutaneous nonendoscopic needle based procedures regarding outcomes, complications and recurrence rates.
Compared to the previous investigation at 2 years, this study shows no significant change in outcome at 4 years. Furthermore, 82% of the patients continued to have a significant improvement in leg pain. The improvement in low back pain as an expression of discogenic pain for 87% of the patients after 4 years was unexpected. It indicates that a less traumatizing approach to the lumbar spine combined with the proven effects of radiofrequency have a positive impact on this problem and can help to avoid open surgery or even a fusion.55 Huang et al. have shown that the posterolateral minimal invasive approach has a lower systemic response in postsurgical metabolism.56 Additionally, the opportunity to do this procedure under local anaesthesia gives the patient a diminished peri- and postoperative stress. A faster recovery, mobilization and less postoperative pain are advantageous to the patients undergoing this procedure.
Other studies to extend the statistic power of this limited number of patients are on their way to underline these findings.
Conclusion
Overall, the results from this 4 year study are very encouraging and qualify the safe continuous use of the technique in carefully selected patients with low back and radicular pain of discogenic origin. Comparing the outcomes, reoperation and complication rates to open surgery, the presented procedure (83% satisfaction rate, 6.3% late reoperation, no complications) shows no inferiority, causes less surgical trauma, delivers significant pain relief and should be considered as an option in the presence of contained hernias. The intention is to give the patient a chance to avoid an open surgery and leave the dorsal approach virgin.
Disclosures
Dr. Hellinger has received honoraria for speaking and teaching from elliquence LLC.
- Copyright © 2014 ISASS - International Society for the Advancement of Spine Surgery
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.