


Abstract
Background Loss of lumbar lordosis has been reported after lumbar interbody fusion surgery and may portend poor clinical and radiographic outcome. The objective of this research was to measure changes in segmental and global lumbar lordosis in patients treated with presacral axial L4-S1 interbody fusion and posterior instrumentation and to determine if these changes influenced patient outcomes.
Methods We performed a retrospective, multi-center review of prospectively collected data in 58 consecutive patients with disabling lumbar pain and radiculopathy unresponsive to nonsurgical treatment who underwent L4-S1 interbody fusion with the AxiaLIF two-level system (Baxano Surgical, Raleigh NC). Main outcomes included back pain severity, Oswestry Disability Index (ODI), Odom's outcome criteria, and fusion status using flexion and extension radiographs and computed tomography scans. Segmental (L4-S1) and global (L1-S1) lumbar lordosis measurements were made using standing lateral radiographs. All patients were followed for at least 24 months (mean: 29 months, range 24-56 months).
Results There was no bowel injury, vascular injury, deep infection, neurologic complication or implant failure. Mean back pain severity improved from 7.8±1.7 at baseline to 3.3±2.6 at 2 years (p < 0.001). Mean ODI scores improved from 60±15% at baseline to 34±27% at 2 years (p < 0.001). At final follow-up, 83% of patients were rated as good or excellent using Odom's criteria. Interbody fusion was observed in 111 (96%) of 116 treated interspaces. Maintenance of lordosis, defined as a change in Cobb angle ≤ 5°, was identified in 84% of patients at L4-S1 and 81% of patients at L1-S1. Patients with loss or gain in segmental or global lordosis experienced similar 2-year outcomes versus those with less than a 5° change.
Conclusions/Clinical Relevance Two-level axial interbody fusion supplemented with posterior fixation does not alter segmental or global lordosis in most patients. Patients with postoperative change in lordosis greater than 5° have similarly favorable long-term clinical outcomes and fusion rates compared to patients with less than 5° lordosis change.
Introduction
Aging is associated with progressive loss of lumbar lordosis and a gain of thoracic kyphosis.1, 2 Several studies have shown lumbosacral interbody fusion surgery results in loss of lumbar lordosis and development of flat back deformity due to improper patient positioning and use of distraction instrumentation.3, 4 The impact of lumbosacral fusion surgery on lumbar lordosis appears to be highly dependent on surgical approach.1, 2, 5–8 Significant loss of lumbar lordosis may accelerate adjacent segment intervertebral disc degeneration, resulting in further back pain and dysfunction.9
Clinical and radiographic outcomes with axial lumbar interbody fusion (AxiaLIF) have been previously described.10–15 However, there is limited published information on the effects of axial lumbar interbody fusion on segmental and global lumbar lordosis in patients undergoing L4-S1 fusion.16 Therefore, we performed a retrospective analysis of patients who underwent two-level axial lumbar interbody fusion and supplemental posterior fixation to determine the changes in segmental and global lumbar lordosis and the associated impact of these changes on clinical outcomes and fusion rates though a minimum of 2 years post-surgery.
Methods
Patient Characteristics
We retrospectively reviewed prospective data collected on 58 consecutive patients who underwent L4-L5 and L5-S1 interbody fusion with the AxiaLIF 2L or 2L plus system (Baxano Surgical, Raleigh, NC) with at least 24 months follow-up (mean: 29 months, range 24-56 months). The requirement for informed consent was waived at each site due to the retrospective nature of the study. The typical patient presented with disabling back pain and 90% reported concomitant radicular symptoms. Degenerative disc disease was the primary diagnosis in 38, spondylolisthesis in 10, spinal stenosis in 4, radiculopathy in 3, and failed previous decompression and attempted fusions in 3 (Table 1).
Baseline Patient Characteristics
All patients underwent 6 months or more treatment prior to surgical intervention. Indications for surgery were pain and disability not responsive to medical treatment, physical therapy, lumbar epidural steroids and selective nerve root blocks. Patients with previous pelvic surgery, infection, radiation therapy, inflammatory bowel disease, or rectal disease were excluded.
Pre-treatment assessment
All patients provided a detailed medical and medication history and underwent comprehensive physical and neurologic examinations, in accordance with the Milliman Care Guidelines for lumbar fusion. Preoperative imaging studies included magnetic resonance imaging, contrast and non-contrast enhanced computed tomography (CT), discography, electrodiagnostic studies, and anteroposterior and lateral flexion/extension x-rays.
Surgical procedure
Patients underwent a two-level interbody fusion procedure utilizing the AxiaLIF 2L or 2L plus implants supplemented with pedicle or facet screws. The 2L device was approved by the FDA in 2008 and the 2L plus implant was approved in 2010. The four-component AxiaLIF 2L plus rod is designed to provide improved fixation and resistance to subsidence compared to the 2L implant.
The two-level interbody fusion procedures began with the patient positioned on a radiolucent extension frame (Jackson table) with hips and knees in extension to maximize lordotic posture. The presacral plane was entered through an incision at the level of the paracoccygeal notch. A preplanned trajectory using templates and anterior-posterior and lateral C-arm images were used to navigate to the central portion of the L5 vertebra and the anterior part of the L4 vertebral body. After preparation of a 12 mm bony channel in the sacrum, the L5-S1 disc space was entered and nitinol cutters were used to debulk the nucleus pulposus and denude the superior and inferior endplates to bleeding bone in preparation for fusion. In a similar fashion, the L4-L5 interspace was prepared for fusion and the L4 vertebral body was reamed taking care not to penetrate the superior endplate of L4. A combination of autogenous bone and bone marrow aspirate from the iliac crest and vertebral bodies was used together with bone graft extenders and allograft bone to provide material for fusion. Rh BMP-2 was used in 39 (67%) patients. A 2L or 2L plus axial rod was inserted in the prepared channel. Care was taken not to place the L4 portion of the rod in the proximity of the superior endplate of L4. The rod system may be placed with or without distraction; overdistraction is to be avoided. In some cases, the axial rod was inserted after placement of pedicle screws. Distraction of the L5 and L4 pedicle screws against locked S1 screws can be performed to increase the height of the resected disc space and improve sagittal and coronal alignment of the L4 to sacral segments. Pedicle screws and rods were used in 33 patients, facet screws in 15 patients, and combinations of pedicle and facet screws in 10 patients. Most of the posterior devices were placed percutaneously and all posterior constructs were bilateral.
Clinical and Radiographic Analysis
Clinical and radiographic data were collected during regularly scheduled office visits including pre-treatment, 3 months, 6 months, 12 months, and 24 months. Postoperatively, fusion mass quality and implant stability were assessed with anterior-posterior and lateral radiographs taken in flexion and extension in all patients. Postoperative fusion status was assessed with CT scans except in 2 patients with post-treatment x-rays only. Fusion was defined as the presence of bridging bone from vertebral endplate to endplate occupying greater than 50% of the interspace on CT scan and no motion on flexion-extension films.10, 17 Axial back pain severity was assessed at each visit with a 10-point numeric scale. Back function was evaluated with the Oswestry Disability Index (ODI)18 at two of the four sites. Odom's criteria was used to rate clinical outcome at each site.19
Segmental and global lordosis measurements were made using the Cobb method on standing lateral radiographs.20 Surgimap Spine (New York City, NY, USA) and Study Share (McKesson, San Francisco, CA, USA) software were used to perform the Cobb angle measurements. The angle of the L4-S1 segment was measured by the intersection of lines drawn parallel to the superior endplate of L4 and the superior end plate of S1. The angle of the L1-S1 segment was measured by the intersection of lines drawn parallel to the superior endplate of L1 and the superior endplate of S1. Loss or gain of lordosis was defined as a > 5° Cobb angle decrease or increase, respectively, compared to preoperative angles.21
Statistical Methods
Data were analyzed using Predictive Analytics Software (v. 18, SPSS, Inc., Chicago, IL, USA). Continuous data were reported as mean ± SD and categorical data were reported as frequencies and percentages. Paired samples t-tests were used to assess changes in back pain severity, ODI, and lumbar lordosis from baseline to 2 years. Clinical improvement was defined as ≥30% improvement in back pain scores22, 23 and ≥30% improvement in ODI.22, 24 Statistical significance was set at p < 0.05 for all analyses.
Results
There was no bowel injury, vascular injury, deep infection, neurologic complication or implant failure. Median procedural blood loss was 250 cc (range: 50-1,000 cc) and median length of hospital stay was 3 days (range: 0 to 9 days).
Mean back pain severity improved from 7.8±1.7 at baseline to 3.3±2.6 at 2 years (p < 0.001). Pain severity improvement ≥30% at 2 years was reported in 77% of patients. Mean ODI scores improved from 60±15% at baseline to 34±27% at 2 years (p < 0.001). ODI improvement ≥30% at 2 years was reported in 52% of patients. At final follow-up, 48 (83%) patients were rated as good or excellent, 8 (14%) were fair, and 2 (3%) were poor using Odom's criteria. Interbody fusion was observed in 111 (96%) of 116 treated interspaces at final follow-up. Non-union was identified at both levels in one patient and at L4-L5 only in three patients.
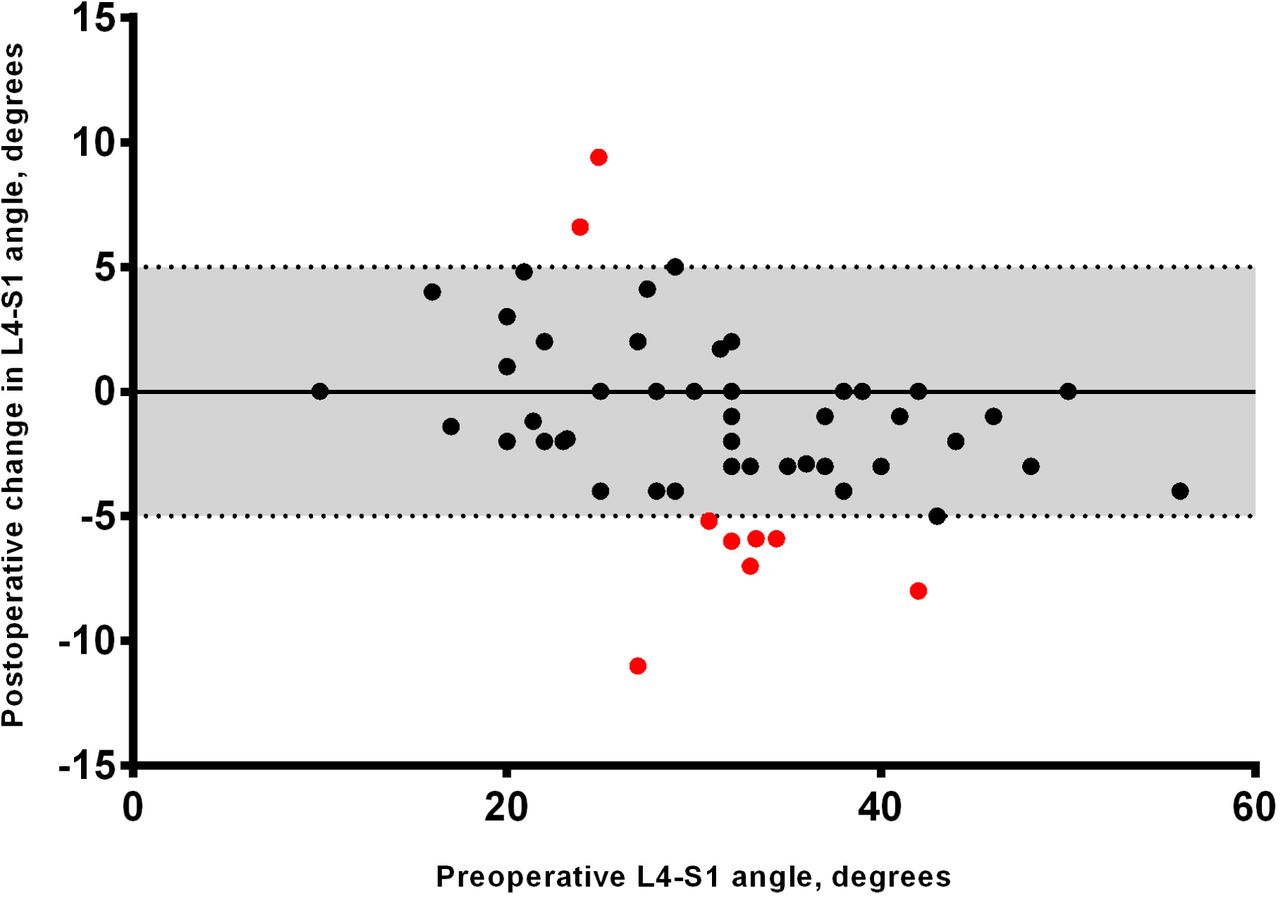
Mean global lordosis was unchanged and mean segmental lordosis decreased 1°. The magnitude of change in global lordosis 2 years after surgery was moderately inversely correlated with preoperative L1-S1 lordosis (r = -0.44, p < 0.001) (Figure 1). A weak inverse correlation (r = -0.33, p = 0.01) was also observed in preoperative segmental lordosis and postoperative change in segmental lordosis (Figure 2). Maintenance of lordosis, defined as a change in Cobb angle ≤ 5°, was identified in 84% of patients at L4-S1 and 81% of patients at L1-S1 (Figure 3, Figure 4). Patients with loss or gain in segmental or global lordosis experienced similar 2-year outcomes versus those with less than a 5° change (Table 2).

Scatterplot demonstrating relationship between preoperative lordosis and postoperative lordosis change at L1-S1. The grey shaded area represents ±5° compared to pre-treatment values. Patients with lordosis change > 5° are represented in red.

Scatterplot demonstrating relationship between preoperative lordosis and postoperative lordosis change at L5-S1. The grey shaded area represents ±5° compared to pre-treatment values. Patients with lordosis change > 5° are represented in red.

Lateral standing radiograph showing a) lordosis of 24° at L4-S1 and 50° at L1-S1 at pre-treatment, and b) 24° L4-S1 and 52° L1-S1 lordosis 2 years after two-level axial lumbar interbody fusion.
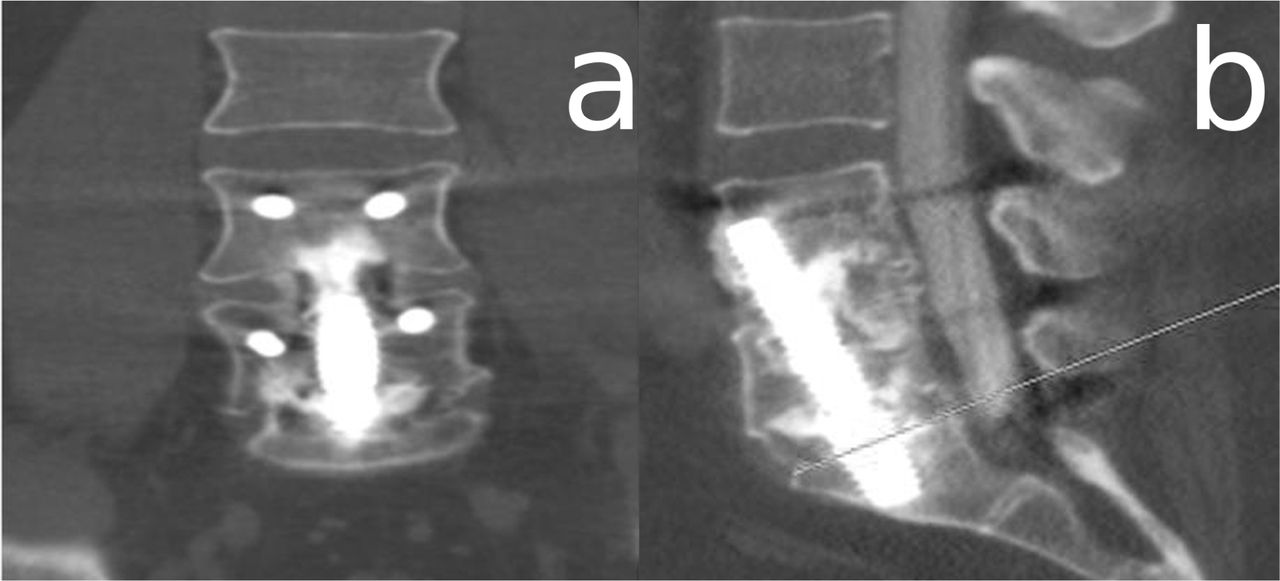
a) Anteroposterior and b) lateral CT scan of 2-level AxiaLIF and posterior instrumentation demonstrating solid fusion at 2 years.
Relationship of Lordosis Change with 2-year Clinical Outcomes and Fusion Rates.
Four patients treated with BMP had subsidence (range: 3 to 7 mm) of the proximal portion of the implant. In one patient, the superior endplate of L4 was breached. Implant subsidence resulted in no symptoms or complications requiring treatment. Seven additional procedures were performed in these 58 patients following the index surgery. One patient had a repair of a L4-L5 non-union by placement of a TLIF cage without removal of the axial rod. One patient had extravasation of bone graft into the lumbar canal that was removed by laminectomy with no neurologic deficit. Three patients underwent removal of misplaced facet screws and one patient required repositioning of a pedicle screw. One patient had a laminectomy at 6 months for removal of a BMP-induced cyst.
Discussion
This retrospective analysis of 58 patients who underwent L4-S1 lumbosacral fusion demonstrated that axial lumbar interbody fusion results in acceptable clinical outcomes and fusion rates through 2 years. Additionally, axial lumbar interbody fusion does not cause a meaningful change in global or segmental lordosis in most patients. In patients who experienced change in lordosis of greater than 5°, clinical outcomes and fusion rates were not compromised.
Previous studies of lumbar interbody fusion have reported inconsistent postoperative lumbar lordosis changes. Preservation of lumbar lordosis in patients undergoing thoracolumbar and lumbosacral fusions has not been successful in many cases due improper patient positioning.4 Goldstein et al.25 found greater loss of lordosis at 2 years following the use of posterior placed threaded interbody cages compared to anterior L4-L5 or L5-S1 interbody fusions. However, all Cobb angles remained within normal ranges and no relationship with clinical outcomes was demonstrated.
Dimar et al.26 compared restoration of lumbar lordosis following four commonly used techniques of single-level instrumented fusion and found that anterior interbody fusion with lordotic threaded cages resulted in greater gain in lumbar lordosis and maintenance of disk space height postoperatively while posterolateral fusion was associated with a mean 10° loss of lordosis. Jagannathan and coworkers27 found that transforaminal lumbar interbody fusion (TLIF) was highly effective in improving lordosis, restoring sagittal balance, and correcting spondylolisthesis. Hsieh et al.28 found that anterior lumbar interbody fusion (ALIF) was superior to TLIF in improving sagittal balance, restoring foraminal height, and local disc angle; however, clinical outcomes through 2 years were comparable between the groups. Jiang and coworkers29 reviewed nine studies comparing ALIF with TLIF and found that ALIF was superior to TLIF in restoration of disc height and global and segmental lordosis, although clinical outcomes and fusion rates were similar.
Overall, it appears that postsurgical loss of lordosis does not portend poor clinical outcomes. Similar to the findings of previous studies, the patients in the current study who gained or lost more than 5° lordosis had comparable clinical and fusion results. Patient- and surgery-related factors that are associated with satisfactory clinical outcomes in patients with lordosis loss or gain have yet to be clearly elucidated. Guanciale and coworkers3 found that patients positioned for spinal fusion on an Andrews frame with the hips and knees flexed had a statistically significant loss in global (L1-S1) and segmental (L4-S1) lumbar lordosis compared to patients positioned on a four poster type frame with hips and knees extended. Jackson et al.30 reported that each patient has a unique posture and spinopelvic balance and that sagittal alignment varies with age, gender, weight and pelvic morphology. It is, therefore, likely that a complex patient- and surgery-specific interplay of multiple factors exists that explain the relationship between lumbar lordosis and postoperative patient symptomatology.
There is concern that placing a straight axial rod from the sacrum to L4 will reduce global and segmental lordosis and that distraction applied through the rod will result in further loss of lordosis. The trajectory for the rod is designed not to change the lordotic curve, but to provide anterior column support and fixation of the L4, L5 and S1 vertebrae. The application of distraction through the axial rod results in variable disc height restoration and support of the collapsed disc spaces. As an alternative approach, pedicle screws can be placed before the rod is inserted. After removal of the intradiscal contents through the presacral approach, distraction of the pedicle screw-rod construct is performed. This results in an increase in disc space height and preservation of lumbar lordosis without the need to apply distraction to the axial rod. With proper patient positioning and avoidance of excessive distraction, loss of lumbar lordosis and creation of flat back deformity is avoidable. There were no clinical findings of flat back syndrome in any patients in this study.
This study has several shortcomings. First, ODI was collected from patients at two of four sites and, therefore, the reported outcomes may not be representative of the entire study cohort. Despite this limitation, other clinical outcomes and fusion rates were similarly favorable. Second, pre- and postoperative disc height measurements were not made. Third, the low incidence of lordosis loss greater than 5° prevents the use of formal statistical comparisons to patients that maintained lordosis. Much larger studies would be required to statistically test the hypothesis that change of lordosis influences clinical outcomes. Finally, retrospective, single-arm studies are susceptible to confounding and bias concerns; consequently, the results of the current study represent Level IV evidence.
Conclusions
Two-level axial interbody fusion supplemented with posterior fixation does not meaningfully change segmental or global lordosis in most patients. Patients with postoperative change in lordosis greater than 5° have similarly favorable long-term clinical outcomes and fusion rates compared to patients with less than 5° lordosis change.
Disclosures
WDT, TJR, NA, LEM, and RJN are consultants to Baxano Surgical. MAM and RJE report no conflicts.
- Copyright © 2014 ISASS - International Society for the Advancement of Spine Surgery
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.