


Abstract
Background In this preliminary study we used a goat model to quantify pressure at an interbody bone graft interface. Although the study was designed to assess fusion status, the concept behind the technology could lead to early detection of implant failure and potential hazardous complications related to motion-preservation devices. The purpose of this study was to investigate the feasibility of in vivo pressure monitoring as a strategy to determine fusion status.
Methods Telemetric pressure transducers were implanted, and pressure at the bone graft interfaces of cervical interbody fusion autografts placed into living goats (Groups A and B) was evaluated. Group A constituted the 4-month survival group and Group B the 6-month survival group. One goat served as the study control (Group C) and was not implanted with a pressure transducer. An additional six cadaveric goat cervical spines (Group D) were obtained from a local slaughterhouse and implanted with bone grafts and ventral plates and used for in vitro biomechanical comparison to the specimens from Groups A and B.
Results All goats demonstrated an increase in interface pressure within the first 10 days postoperatively, with the largest relative change in pressure occurring between the sixth and ninth days. The goats from Groups A and B had a 200% to 400% increase in relative pressure.
Conclusions Although this was a pilot study to assess pressure as an indicator for a fusion or pseudarthrosis, the preliminary data suggest that early bone healing is detectable by an increase in pressure. Thus, pressure may serve as an indicator of fusion status by detecting altered biomechanical parameters.
INTRODUCTION
Postoperatively, the status of a fusion and the incorporation of bone across a destabilized spinal segment can be difficult to assess and has led to a 20% underestimation of the fusion grade.1, 2 In addition, conventional imaging techniques are limited in utility and cannot provide the surgeon with information regarding the dynamics of the fusion mass, adequate visualization of bone incorporation into the host bone (ie, vertebral endplates), mechanical integrity of the fusion mass, and the real-time bone remodeling scenario. An alternative mechanism for assessment with greater accuracy would be desirable.
We propose the novel concept of pressure measurement at the host bone and graft interface to monitor the spine fusion process.
This choice of pressure as the monitoring parameter is based on some precedent. First, pressure is a well-defined physiological assessment parameter, particularly in the cardiovascular arena. Second, pressure measurement has been investigated for other areas in medicine, including the orthopedic arena.3–8 For example, many researchers and clinicians have examined the relationship between intradiscal pressure and pain or the extent of motion segment degeneration.3, 9, 10 Nevertheless, there is a dearth of research exploring the relationship between pressure and bone healing.
Telemetric transmission of biomechanically derived information for in vivo healing and implant behavior assessment is not a novel concept.8, 10–12 Researchers have attempted to employ strain gauges on spinal implants, using telemetric data transmission for in vivo serial monitoring of loads following fusion during daily activities.12 Unfortunately, these systems were plagued with complications. The telemetric unit was bulky, and internal wire breakage was a common occurrence. Consequently, long- term measurements (> 4–6 months) of in vivo axial loads on implants and bone healing were not accomplished. In our study, we used a commercially available implantable telemetric transducer with two gel-filled catheters that were implanted at the graft and vertebral endplate interface at the bone graft site in the goat cervical spine. These transducers housed all of the electronic components within a hermetically sealed chamber and used the two gel-filled catheters for pressure transmission. Therefore, there was little risk of internal wire breakage and loss of signal transmission.
In vivo animal studies are often used to investigate the effects of altered biomechanical parameters and their association with evolving biological events. The goat's cervical spine has greater bone density than that of humans, shows less variability within the species, is kinematically different, and possesses anatomical differences from that of humans.13 Nevertheless, several factors make the goat a suitable model for measurement of interbody bone graft pressure. The upright posture of the goat's cervical spine is ideal for interbody fusion studies because the cervical spine is axially loaded.13, 14 In addition, although the cervical disc interspace of a goat spine is essentially a ball and socket joint and the human disc interspace is elliptically shaped, the range of motion is similar. 15
This preliminary study was designed to assess the in vivo healing status of the spine, with an overall goal to demonstrate that changes in the in vivo biomechanical parameters (ie, pressure in this scenario) can be measured over time. The basic concept of the study was to establish the feasibility of using telemetric pressure sensors to assess the process of bone healing in vivo. Information generated from studies like this could contribute to future development of implantable microsized biosensors using microelectromechanical systems (MEMS) technology for in vivo chronic monitoring of orthopedic implant performance and tissue healing.6, 16–18 However, this technology is not yet commercially available, and the ability to actually monitor the in vivo bone healing and to sense a change in biomechanical parameters must be addressed before the technology can be developed. Therefore, preliminary proof-of-concept studies using conventional pressure transducers are required to provide the necessary information to design and develop implantable biosensors that might employ novel technologies such as MEMS. Once it is deemed a feasible concept to investigate further, the potential of such a technology is infinite. Possible applications include incorporation of microsized implantable biosensors onto orthopedic implants to detect early migration of the implant, loss of fixation at the bone and implant interface, and changes in tissue performance based on these measurements.
A goat cervical interbody fusion model was employed in this study to address the feasibility of using pressure measurements to monitor the process of bone healing by differentiating between the successful initial acquisition of fusion and the development of a pseudarthrosis during the early postoperative period. Therefore, we focused on the use of pressure as an indicator of changes in healing patterns that can be indicative of fixation loss and pseudarthrosis.
MATERIALS AND METHODS
Over view
A goat cervical interbody fusion model was employed. Four study groups were analyzed. Six male castrated Alpine goats underwent a ventral fusion operation at C3-C4, following discectomy. Iliac crest autograft, with an accompanying ventral cervical fixation plate (DOC; Depuy-Acromed, Raynham, Massachusetts), was employed. Five of the goats were implanted with a dual-channel telemetric pressure transducer and were sacrificed at either 4 (Group A) or 6 (Group B) months (Table 1). The remaining goat functioned as an operative control in which telemetric hardware was not placed, but a bone graft at C3-4 was placed (Group C). This goat was sacrificed at 4 months. In vivo contact pressure at the bone graft and vertebral endplate interface was assessed in each goat in Groups A and B three times daily. At the termination of the study, each goat was euthanized, and the spines were harvested for further evaluation of the fusion status via non-destructive biomechanical testing, histological sectioning, or micro-CT imaging.
Study Group Composition and Fusion Status Assessments Conducted
Pressure Transducer and Calibration Procedure
Prior to surgical implantation, the calibration of the DSI dual-channel, telemetric pressure transducer (Physiotel Multiplus Implant, TL11M3-D70-PCP Data Science International, St. Paul, Minnesota) was evaluated by placing a manual contact load onto each catheter following the configuration of the device once in vivo. Each transducer had an accuracy of ± 0.1 kPa and a maximal pressure shift of 2%, with two independent catheters used to monitor in vivo contact pressure at the bone graft interface site in the goat spines (Figure 1). The battery was rated at a nominal lifespan of 3.5 months for continuous use and was housed with the transmitter. Two 1.2-mm-diameter silicone, elastomeric, close-ended, compressible tube catheters with pressure sensors housed at the proximal end of the fluid- filled tubes were used to measure pressure at the bone graft and vertebral endplate interfaces under compressive loading. Each closed catheter was affixed within a circular canal at the bone graft and vertebral endplate interface and transmitted the contact pressure measurements from the bone graft to the pressure sensor sealed within each catheter.

The DSI telemetric pressure transducer (Physiotel Multiplus Implant, TL11M3-D70-PCP Data Science International, St. Paul, Minnesota, housing two pressure sensors within the fluid-filled catheters, with one catheter being compressed to a measured displacement to demonstrate the catheter compliancy. (a) Pressure transmitter and receiver, (b) maximum compression of the catheter is shown and will transmit load to the pressure sensor, (c) catheters housing pressure sensors in a fluid-filled tube.
Prior to implantation of each pressure transducer, the linearity and tracking behavior of each pressure transducer was measured against the compressive loading applied by the Instron test apparatus. This was accomplished by applying six cycles of a known compressive load to each transducer and comparing it to the pressure measurements acquired. A sinusoidal load at a frequency of 0.1 Hz and a maximum compressive load of 200 N were applied under load control using the servohydraulic materials test apparatus (Instron 8874, Instron Corp., Canton, Massachusetts) to the pressure transducer. To do so, the catheter was restrained within a semicircular canal and directly compressed by the Instron testing apparatus. The compressive loading cycles applied by the testing apparatus were mapped against the measured pressure cycles to assess the transducers’ performance with respect to phase lags, accuracy, and/or nonlinearities in response to the compressive loading (Figure 2). The maximum catheter deformation under compressive load for each sample was also measured. A linear regression analysis was conducted to assess the linearity of the pressure transducer and the phase lag in response to the compressive loading. The configuration and operation of the pressure transducers was by Dataquest A.R.T. version 2.3 software (DSI) to sample all of the recorded pressure at a sampling rate of 500 Hz. Finally, the subsidence across the C3-C4 motion segment was quantified by measuring the ventral and dorsal motion during cadaveric biomechanical testing for six of the cervical spine specimens using the MaxTRAQ version 1.41 software image analysis system (Innovision Systems Inc., Lapeer, Michigan).

Correlation of the pressure transducer with a 200-N applied load from the Instron testing apparatus. A sinusoidal waveform input from 0 N to 200 N in pure compression at a rate of 0.1 Hz was applied for five cycles of loading. The accuracy of the transducers is demonstrated by the linear correlation between pressure and the applied load, R2=0.9998.
Surgical Procedure for the Cer vical Interbody Fusion
An incision was made ventral to the sternocleidomastoid muscle (SCM). The spine was approached between the strap muscles, esophagus, and trachea medially and the carotid sheath and SCM laterally. After the longus coli muscle was retracted laterally, a ventral discectomy was performed at the C3-C4 segment after localization with fluoroscopy. An osteotome was used to craft mortises by cutting out a box-shaped region (1.3 cm3 for placement of the bone graft (Figure 3). Autogenous bone was harvested from the goat's iliac crest, properly sized, and gently impacted into the C3-C4 disc space (Figures 3 and 4). Each bone graft for all five goats was reproducible in size to an error of less than 10%. A 2.8-cm DOC ventral cervical rigid plate (DePuy Spine, [J&J subsidiary], Raynham, Massachusetts), with 4-mm-by-16-mm divergent fixed angle screws, was used to immobilize the C3–C4 motion segment once the bone graft was in place (Figure 4).

Cuboid-shaped autogenous bone graft crafted from the iliac crest of the goat. The dimensions closely matched that of the host sites at C3-C4.
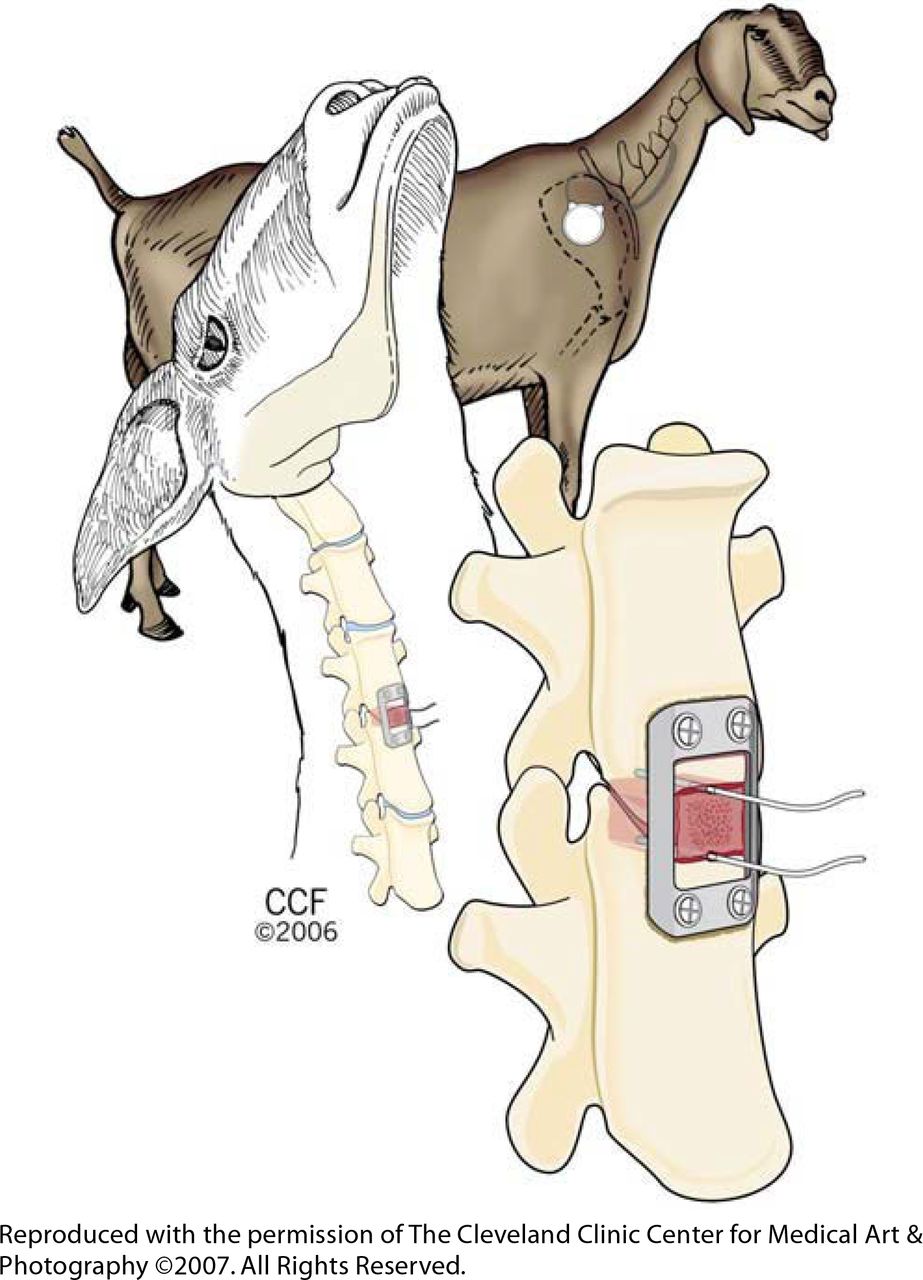
An illustration of the two catheter placements from the DSI pressure transducer into the goat cervical spine. The catheters were inserted approximately 1 cm in depth at the superior and inferior bone graft and vertebral endplate interface.
The telemetric pressure transducer was implanted after the bone grafting procedure by insertion of each catheter above and below the bone graft into two pre-awled locations at the bone graft–vertebral endplate interfaces and sutured into place (Figure 4). Each pressure-sensing catheter was seated into a circular channel that was created at the bone graft– vertebral endplate interface to provide localized containment of the catheters for the transmission of contact pressures. The transmitter and battery portions of the transducer were implanted in a submuscular pocket created in the dorsolateral region in each goat's neck.
The goats were monitored daily for signs of infection and distress for the duration of the study (4–6 months). This time frame has been used successfully for cervical interbody fusion in goats.19–21 One of the six original goats demonstrated early signs of wound infection and was dropped from the study analysis. Pressure was recorded three times daily for the duration of 2 minutes per trial while the goats stood idle with their necks in an upright position. Efforts were made to calm each animal prior to sampling pressure data to ensure minimal physical activity during data sampling. At the end of 4 to 6 months, the goats were euthanized with an overdose of pentobarbital (75 mg/kg) using a standardized protocol that is compliant with the Animal Review Committee for the Cleveland Clinic.
Histological Preparation
Two goats (one each in Groups A and B) were used for histological evaluation. Tissue samples were fixed in 70% ethanol and rough-cut with a band saw to remove adherent soft tissue and the spinous processes. Tissue blocks were then slowly dehydrated without decalcification in a graded series of ethanols and embedded in methylmethacrylate (MMA) using a vacuum chamber at 2°C to 8°C over a 23-day period. Without removing the fixation hardware, sagittal cuts were made using an Exakt diamond saw (EXAKT, Appartebau, Germany), in three sections (central, medial, and lateral) of each C3–C4 level. Each section was ground to a final thickness of 10 to 40 µm and stained with Villanueva's mineralized bone stain (Poly Scientific, Bay Shore, New York). With this staining technique, the mineralized bone stains green, osteoid seams stain magenta, and the remaining tissue stains blue and pink. Once the sections were stained, a board-certified pathologist meticulously assessed each slide for signs of new bone growth and adverse tissue reactions.
Biomechanical Testing
An in vitro biomechanical evaluation of the fusion status for three of the Group A and B goats was conducted and compared to the biomechanical behavior of six cadaveric goat spines implanted with a bone graft and ventral cervical plate at C3-C4 (Group D) to assess the status of the fusions in the implanted goat spines postmortem. Group D consisted of six cadaveric goat cervical spines obtained from a local slaughterhouse and implanted with bone grafts and ventral plates, just prior to the time of biomechanical testing. In these Group D specimens, snug bone-on-bone contact was achieved with an accompanying overlying ventral plate. This position resembles the clinical situation that exists immediately after surgery, when healing and arthrodesis have not yet begun. Variations in contact pressure at the graft interface were examined for possible relationships to fusion status.
Nine goat spines were used for the biomechanical evaluation of the fusion site to determine whether a fusion was present. Three spines were harvested from Groups A and B (Table 1). Six additional spines (Group D) were obtained from a local slaughterhouse vendor and used as a biomechanical comparison for the immediate nonfused grafted situation at C3-C4.
In preparation for testing, the spines were embedded at C2 and C5 into customized gripping fixtures and mounted onto a servohydraulic biaxial testing apparatus (Instron 8874). Each spine was secured to the Instron testing apparatus in a cantilever loading fashion and preconditioned for 20 cycles to 200 N in compression. The center of rotation was located by applying a 200-N maximum compressive load to the upper jig and reapplied until no angular motion was detected by the upper rotational potentiometer. Following the preconditioning and alignment phases, each cervical spine was nondestructively cycled under load control in compression to 200 N at 0.1 Hz for six continuous cycles at a data sampling rate of 50 Hz.19–22
Micro-CT Imaging
Micro-CT images of three of the five goats from Group A and B specimens (Table 1) were obtained by collecting one hundred and eighty 512-by-512 twelve-bit projection radiographs at 1° intervals around half of the entire specimen.23 The images were collected at 90 kVp, 28mA, and with a 1-second exposure time with the image intensifier operating in 7-inch mode and at twice the magnification. Off-line image corrections of the x-ray projection data were conducted following the protocol of Grass et al.24 The micro-CT images provided high-resolution x-ray imaging of the fusion sites for each goat specimen and provided details of the trabecular structure.
Data Analysis
For the pressure measurements, care was taken to capture data while each animal stood idle and was not engaged in chewing or swallowing. The relative change in pressure from the three daily trials was averaged and normalized to the pressure recorded on day 0 and then plotted against time (Figure 5). The means and standard deviations were calculated for each daily data set and the means presented in Figure 5. The maximum relative change in pressure within the first 10 days of pressure recordings is shown in Table 2. Due to the small sample size of the animals used for fusion in this study, the trends in relative pressure changes were examined, and a limited statistical analysis was conducted for bone graft sizing using a one-way analysis of variance (ANOVA).

Graphical representation of the relative change in pressure from day 0 for all of the goats. A rapid increase in pressure was observed within the first 10 days of healing with peak pressure occurring between days 6 and 9.
Fusion Outcomes and Relative Changes in Pressure (Groups A and B - First 10 Days)
RESULTS
Evaluation of the Pressure Transducer
Figure 2 demonstrates the output performance of the pressure transducers while loaded from 0 N to 200 N in pure compression by the Instron test machine. The 200-N compressive load correlated with a mean deformation of 1.37 ± 0.04 mm for the catheter and approximately 20 MPa of pressure recorded from the catheter. A linear regression and correlation was conducted on the load and pressure, yielding an R2 of 0.998, indicating the presence of a high degree of linearity of the pressure transducer. Very little phase lag (< 1 second) was observed between the Instron load cycles and the pressure measured at the bone graft a interface. The lag is attributable to the delay in the actual hydraulics of the Instron testing apparatus and the delay in the viscoelastic response of spinal tissues.
Fusion Status
None of the remaining five goats exhibited external evidence of infection, distress, or catheter extrusion within the first 20 days postoperatively. Long-term complications after 20 days, however, were observed in three of the goats implanted with the pressure transducers. Seroma formation and catheter extrusions were observed in these goats after 20 days. Fortunately, each pressure transducer housed two independent recording catheters. Hence, the extrusion of a single catheter did not affect the pressure monitoring process. The pressure measurements from the caudal catheter are presented in this report. The caudal catheter pressure readings were consistently greater than the rostral catheter readings by a small margin (< 10% for all goats). This is attributable, at least in part, to the added weight of the graft and the additional load transmission to the caudal portion of the vertebral body at C3–C4.
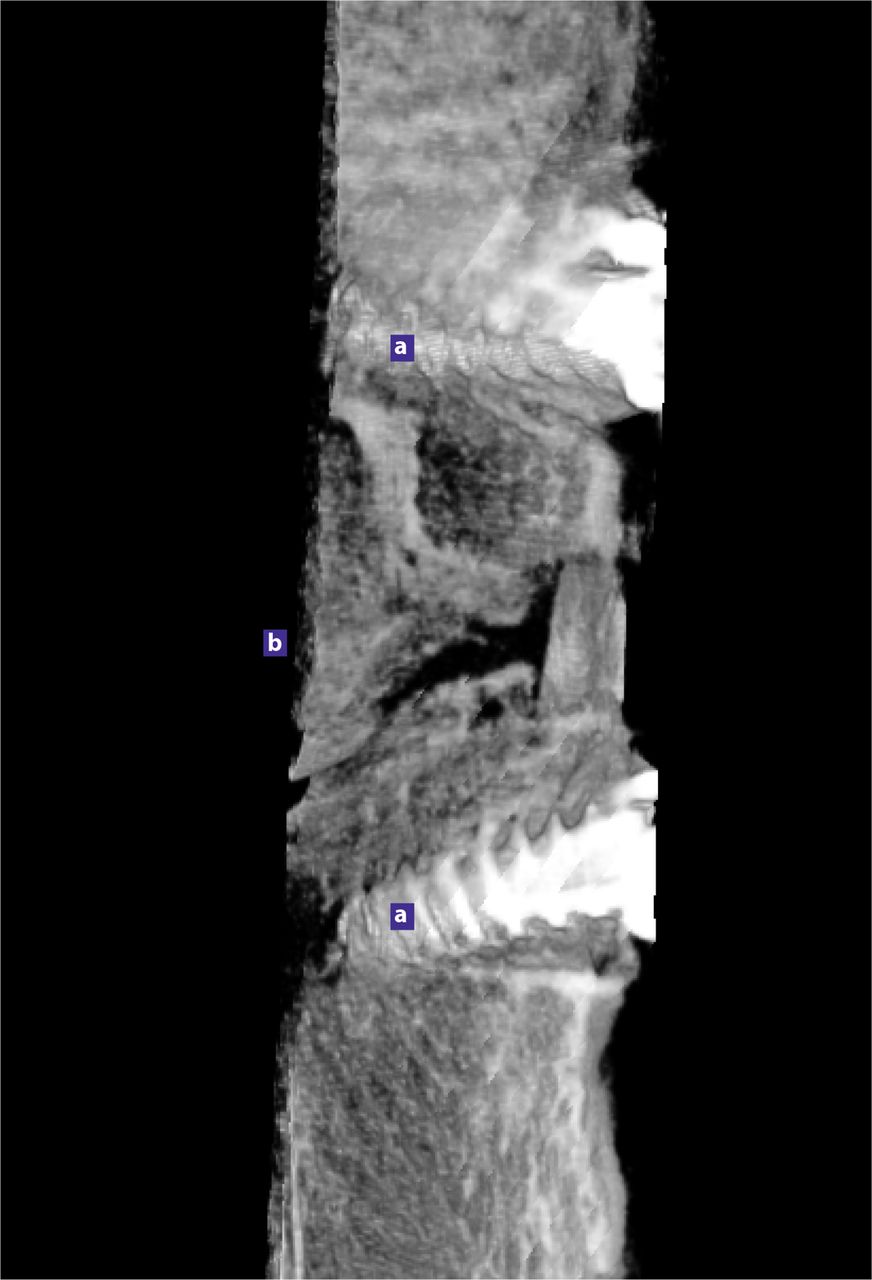
For all 11 goat spines that were grafted (Table 2), no significant difference was observed between the bone graft sizes for any of the goat spines (P > 0.5). None of the goats from Groups A or B, however, achieved a solid bony fusion (Table 2). The histological and micro-CT images demonstrated a pseudarthrosis at the C3-C4 bone graft site in the goats implanted with pressure transducers (Figures 6 and 7). The single goat (Group C) that did not receive a pressure transducer demonstrated histological evidence of a solid fusion at C3-C4 after four months (Table 2).

MicroCT depicting the sagittal view through the C3–4 fusion site. A solid arthrodesis has not formed at 6 months postoperatively, and bone graft remnants that have not completely resorbed are visible. (a) DOC screw, (b) posterior.
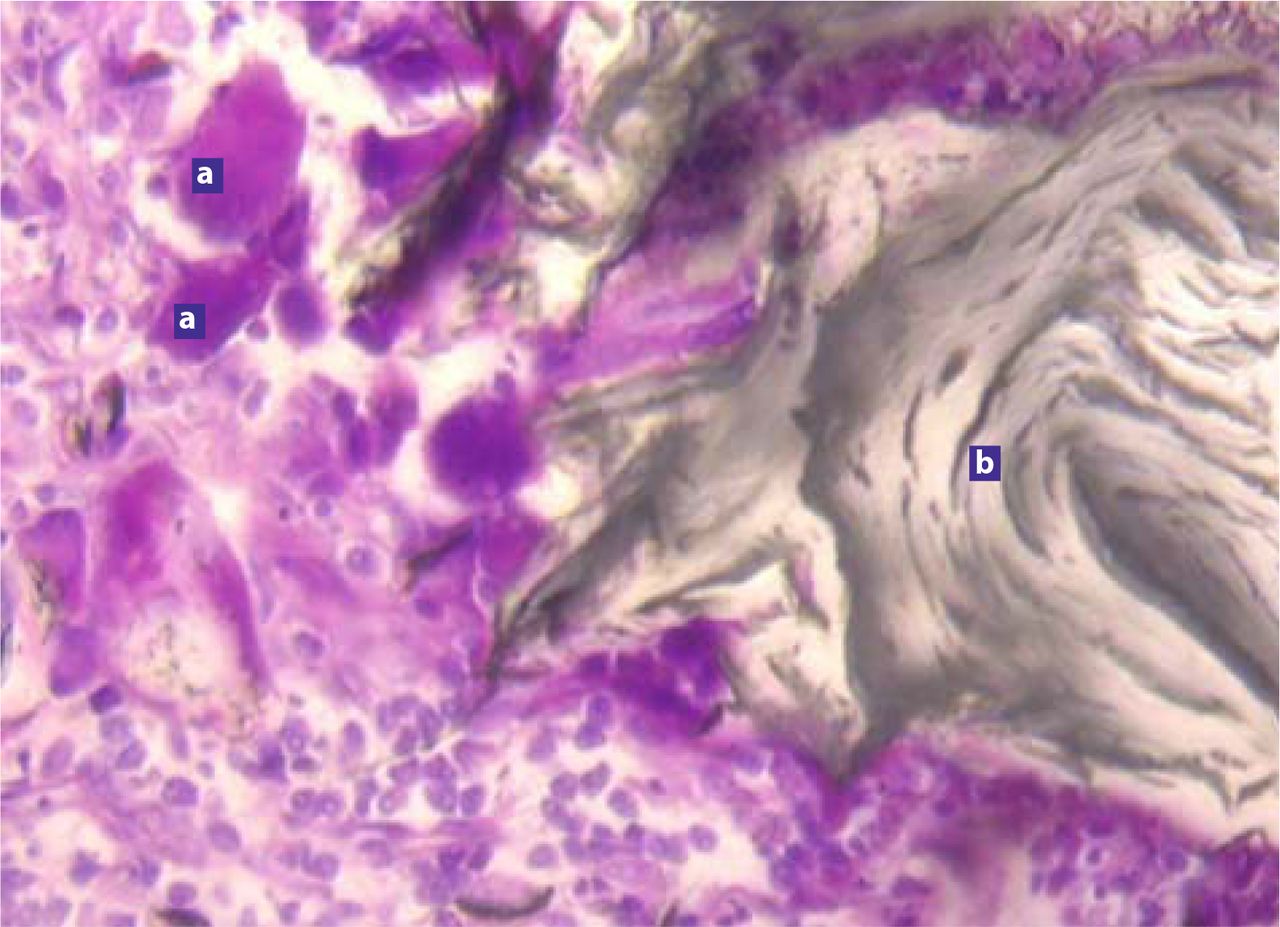
A proprietary gel contained within the catheter was found in the surrounding tissues at the operated sites. Histologically, an inflammatory reaction associated with this gel was present near the bone interface where the gel had egressed from the implanted catheters (Figure 7).

Undecalcified histological section depicting the inflammatory response observed surrounding the gel exudates from the pressure transducer catheters. (a) Giant cells, (b) catheter gel.
Pressure
Table 2 depicts the relative maximum change in pressure for Groups A and B within the initial 10 days of recordings. The pressure measurements at day 0 ranged from 0.6 MPa (Goat 5) to 3.6 MPa (Goat 4). All of the data for each goat were normalized to day 0 for valid comparisons. Goat 2 (Group A) demonstrated the highest change in pressure, with a 410% increase within the first 10 days (Table 2). All of the goats demonstrated consistent increases in interface pressure within the first 10 days postoperatively, ranging from a 200% to 400% increase (Figure 5 and Table 2). The absolute pressure ranged from 2.5 MPa for Goat 2 to 7.6 MPa for Goat 4, with the standard deviations ranging from 0.01 to 1.00 for the average daily means among all of the goats studied. The peaks in pressure occurred between days 6 and 9 for all goats. From day 10 to day 20, all of the goats demonstrated a decline in pressure. Erratic pressure was observed thereafter. With respect to the extent of quantifiable subsidence measured during the in vitro biomechanical testing of the Group D specimens, a mean subsidence of 0.25 ± 0.10 mm was measured across the C3-C4 bone grafted site.
DISCUSSION
This preliminary study defines the pressure changes that occur during the development of a non-union after attempted cervical spine fusion. An increase in pressure during the early stages (first 10 days) correlates with an expected early graft subsidence. Postoperative subsidence increases the load borne by the graft, thus increasing the pressure observed at the interface between the bone graft and the vertebral endplate.25 The initiation of graft instability and pseudarthrosis appears to be heralded by the appearance of erratic fluctuating pressure patterns at the bone graft–vertebral body interface. A rise in the interface pressure was consistently observed in all goats within the first 10 days of monitoring in the study presented here. As previously stated, early graft settling or subsidence occurs within the first week of surgery. In humans, a mean subsidence of 1.4 mm with ventral cervical fusion using autologous bone graft at 1 to 2 weeks after surgery has been reported.25, 26 It is therefore likely that the reproducible increase in pressure during this phase of healing is attributable to early bone graft subsidence at the fusion site, as validated during the in vitro testing conducted on the Group D spines. An interesting point to consider is that the DOC ventral cervical rigid plate used divergent fixed angled screws that by nature of design provide an anterior localized compression to the bone graft where the plate meets the bony margin of the vertebral body. This type of plating causes the center of rotation (COR) of the spine, which is naturally located halfway between the anterior and posterior vertebral margin, to shift toward the proximity of the plate fixation.27, 28 This shifting of the COR toward the plate contributed to a localized compression at the anterior portion of the vertebral body and bone graft. This would technically stress shield the posterior portion of the bone graft but provide greater stress upon the anterior and middle portion of the graft. Therefore, higher pressure would have been expected but was masked by this phenomenon.
There were some limitations to this preliminary study. The absence of fusion in this study could be attributed to the adverse reactions to the catheter and its gel, as well as the eventual seroma formation. An inflammatory reaction was found to be associated with the catheter gel in the surrounding tissue at the fusion site. Additionally, one of the disadvantages of currently available implantable telemetric units is that the bulky implants cause inflammation in the juxtaposed musculature, resulting in irritation and seroma formation.
Fortuitously, the ensuing pseudarthroses provided the opportunity to document the pressure changes associated with a failed fusion. The erratic pressure was observed following the initial subsidence phase of healing, during which interface pressure was elevated. This is intuitively associated with motion and pseudarthrosis. If stability were present, motion at the graft site would not occur and fluctuations of pressure at this site would similarly not be observed. Therefore, erratic fluctuations of pressure are consistent with pseudarthrosis, whereas elevations of pressure are consistent with the expected subsidence that accompanies the nonpathological events that ensue during the early postoperative healing period. Nevertheless, the proof-of-concept goal of this study—that is, the ability to monitor pressure fluctuations with early bone healing— was achieved even with a small sample size. This concept can be applied further to the potential use of implant performance and tissue reaction for numerous motion- preserving and dynamized devices. However, improved clinical methods for telemetric pressure assessment are eagerly anticipated, with the hope that these improvements will facilitate the development of a microsized implantable biosensor using MEMS technology.
Footnotes
The Cleveland Clinic Foundation (the “Clinic”) holds a substantial equity ownership interest in OrthoMEMS, LLC (“OrthoMEMS”) and is entitled to royalty payments from OrthoMEMS upon commercialization of OrthoMEMS's products. Authors Lisa Ferrara, Shuvo Roy, Aaron Fleischman, and Edward Benzel are entitled to a share of any such royalty payments and to a share of proceeds when the Clinic liquidates its equity ownership. Certain Clinic officials serve on the OrthoMEMS Board of Managers. Research related to OrthoMEMS's products, including early-stage research essential to the development of those products, has been conducted at the Clinic by individuals who hold a financial stake in the successful outcome of that research.
Institutional and individual conflicts of interest in research are disclosed to, and reviewed and managed by, the Clinic's Conflicts of Interest Committee and are subject to approval by the Clinic's Institutional Review Board. The Clinic has retained independent monitors to review the protocols, subject enrollment and follow up, and data reporting and analysis of the research reported in this publication.
The treatment and euthanizing of animals in this study followed standardized protocol compliant with the Animal Review Committee for the Cleveland Clinic.
- Received May 29, 2007.
- Accepted October 27, 2007.
- Copyright SAS - Spine Arthroplasty Society 2008
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.