


Abstract
Background The observed rate of recurrent disc herniation after limited posterior lumbar discectomy is highest in patients with posterior wide annular defects, according to the Carragee classification of type II (fragment-defect) disc hernia. Although the recurrent herniation rate is lower in both type III (fragment-contained) and type IV (no fragment-contained) patients, recurrent persistent sciatica is observed in both groups. A higher rate of recurrent disc herniation and sciatica was observed in all 3 groups in comparison to patients with type I (fragment-fissure) disc hernia.
Methods In total, 40 single-level lumbar disc herniation cases were treated with limited posterior lumbar microdiscectomy and posterior dynamic stabilization. The mean follow-up period was 32.75 months. Cases were selected after preoperative magnetic resonance imaging and intraoperative observation. We used the Carragee classification system in this study and excluded Carragee type I (fragment-fissure) disc herniations. Clinical results were evaluated with visual analog scale scores and Oswestry scores. Patients’ reherniation rates and clinical results were evaluated and recorded at 3, 12, and 24 months postoperatively.
Results The most common herniation type in our study was type III (fragment-contained), with 45% frequency. The frequency of fragment-defects was 25%, and the frequency of no fragment-contained defects was 30%. The perioperative complications observed were as follows: 1 patient had bladder retention that required catheterization, 1 patient had a superficial wound infection, and 1 patient had a malpositioned transpedicular screw. The malpositioned screw was corrected with a second operation, performed 1 month after the first. Recurrent disc herniation was not observed during the follow-up period.
Conclusions We observed that performing discectomy with posterior dynamic stabilization decreased the risk of recurrent disc herniations in Carragee type II, III, and IV groups, which had increased reherniation and persistent/continuous sciatica after limited lumbar microdiscectomy. Moreover, after 2 years’ follow-up, we obtained improved clinical results.
Lumbar disc herniation is a common disease that usually presents itself with low back and leg pain and sometimes with serious neurologic symptoms, as a result of root nerve or cauda equina compression. Mixter and Barr1 described a disc excision operation technique for the treatment of sciatica due to disc herniation in 1934; however, they observed that the operation had not released patients from chronic low back pain. Historically, radical discectomy operations were performed; endplates were removed with disc tissue, by use of curettes.2, 3 None of these operations prevented lower back pain and continuous sciatica.4–6 The observed rate of continuous or recurrent sciatica was as high as 40%.7–9 Notably, the reported rate of recurrent disc herniation is 25%, and on average, 10% of patients undergo reoperation because of recurrent pain.8, 10, 11 After radical discectomy techniques had been performed for some time, subtotal discectomy techniques were developed, involving the removal of disc tissue by use of curettes without the endplates being touched. The purpose of this modified technique was to prevent low back pain without disrupting segmental stability. The standard microdiscectomy technique, which is still commonly used today, was first described in 1977.6, 12 Williams13 reported, for the first time, encouraging results after removing minimal intervertebral disc tissue from a small group of patients who had free disc fragments compressing the nerve root. Spengler14 described a less invasive limited discectomy in 1982. In this technique only extruded disc fragments and tender disc tissues need to be removed. Curettes were not used in limited discectomy; only disc fragments were removed.
In 2003 Carragee et al8 described a lumbar disc herniation classification system, according to the degree of annulus and the presence of extruded/free disc fragments. They published limited discectomy results, according to disc herniation type. In this classification system, they described 4 groups of disc herniation: (1) fragment-fissure herniation (disc herniation with minimal annular defect and presence of 1 extruded or sequestered fragment); (2) fragment-defect herniation (presence of extruded or sequestered fragments with wide annular rupture; rupture >6 mm); (3) fragment-contained herniation (intact annulus but with 1 or more fragments below the annulus; such fragments are removed by oblique incision to the annulus); and (4) no fragment-contained herniation (annulus is intact and without free fragments under the annulus). Carragee et al observed high rates of recurrent and persistent continuous sciatica after limited discectomy in the latter 3 groups.
To prevent the risk of failed back syndrome or recurrent disc herniation, as well as to decrease the frequency of postoperative sciatica, we performed posterior dynamic transpedicular stabilization without fusion with limited posterior lumbar microdiscectomy in 40 patients. In this study dynamic fixation was a non–Food and Drug Administration–approved indication for this procedure. We discuss the patients’ clinical results as observed at 2 years’ follow-up.
Materials and methods
Limited lumbar microdiscectomy with posterior dynamic transpedicular stabilization was prospectively performed in 40 patients who were grouped according to the Carragee classification system as type II, III, or IV between 2004 and 2008. These were a consecutive series of patients, and 4 surgeons were involved in this study. All were cases of single-level lumbar discopathy. Cases were selected by use of preoperative magnetic resonance imaging (MRI) and intraoperative observation.15 The Carragee classification system was used in this study, and the Carragee type I (fragment-fissure) group was excluded. The mean postoperative follow-up time was 32.75 months (range, 6–56 months). In this study 37 patients completed 1 year of follow-up and 34 patients completed 2 years’ follow-up. Clinical results were evaluated by use of a visual analog scale (VAS) for leg pain and Oswestry scores (Oswestry Disability Index [ODI]). Patients’ reherniation rates and clinical results were evaluated and recorded at 3, 12, and 24 months postoperatively (Table 1). MRI was also performed on all patients at the above-mentioned time periods. Recurrent sciatica and persistent symptoms were appreciated clinically, and recurrent herniation rates were evaluated according to reimaging with MRI.
Preoperative and postoperative patient characteristics: clinical outcomes according to fragment type and annular defect
Criteria for inclusion in the study were (1) physical examination and patient report consistent with sciatica, (2) single-level disc herniation that was confirmed with MRI, (3) non-emergent elective operational cases, (4) patients who had not had previous operations, (5) patients who were aged between 18 and 60 years, (5) patients who had a neurologic deficit and sciatica, and (6) patients with confirmed wide-based disc herniation on MRI with predominant sciatica and back pain. Infection, instability, scoliosis, insufficient documentation, Carragee type I (fragment-fissure), and malignity were criteria for exclusion.
Surgical technique
All operations were performed in the same hospital by use of operational microscopy and standard surgical technique, by 4 neurosurgeons. Single-dose prophylactic antibiotics were administered to all patients before incision. A limited lumbar posterior microdiscectomy procedure was performed. Discectomy was performed from the interlaminar space in some patients, whereas in others it was performed via a small laminotomy, formed by a high-speed drill. During the operation, disc type was identified according to the Carragee classification system. If the disc type was identified as type I (fragment-fissure), the patient was excluded from the study. When patients were identified as type II (fragment-defect), extruded or sequestered disc fragments were removed and the disc space was cleaned of loose and easily accessible disc fragments, by use of forceps. Curettes were not used in the disc space, and intact annulus parts were left untouched. Because there were no annular defects in intraoperatively identified Carragee type III and IV discs, the annulus was opened with an oblique incision with a No. 15 blade. Sub-annular fragments were removed with rongeurs; such patients were recorded as type III. If there were no free disc fragments in the sub-annular space, patients were recorded as Carragee type IV; extensive annulotomy was performed in such cases, and protruding disc fragments were removed. At least 2 surgeons evaluated and recorded the state of the annulus and free disc fragments during all operations. After discectomy, with the help of lateral intraoperative fluoroscopy, posterior dynamic transpedicular stabilization was performed for Carragee type II, III, and IV cases, by use of the Wiltse approach via the inner paravertebral muscle.16 Cosmic (Ulrich GmbH & Co. KG, Ulm, Germany) and Safinaz (Medikon, Ankara, Turkey) dynamic transpedicular screws with rigid rods were used (Fig. 1).
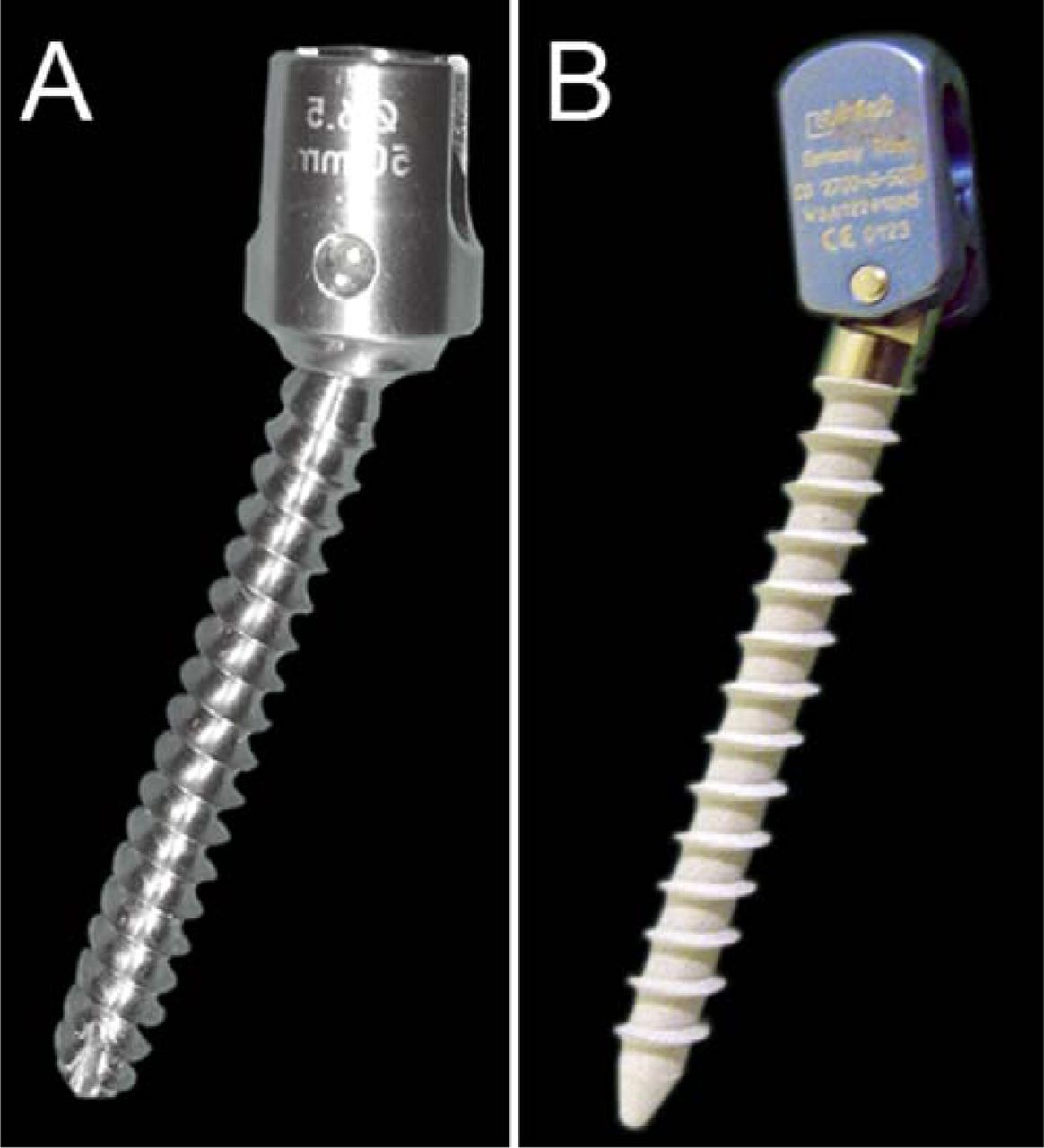
(A) Safinaz dynamic transpedicular screw (Medikon). (B) Cosmic dynamic transpedicular screw (Ulrich GmbH & Co. KG).
Results
The most common herniation type in our study was type III (fragment-contained), with 45% frequency. The frequency of fragment-defect cases was 25%; the frequency of no fragment-contained cases was 30%. The perioperative complications observed were as follows: 1 patient had bladder retention that required catheterization, 1 patient had a superficial wound infection, and 1 patient had a malpositioned transpedicular screw. The malpositioned screw was corrected with a second operation that was performed 1 month after the first. We observed that recurrent/persistent sciatica rates were significantly lower among Carragee types II, III, and IV. Significant postoperative improvements were observed for the ODI and VAS measurements. Recurrent disc herniation was not observed during the follow-up period. The summary of patients’ preoperative and postoperative ODI scores, VAS scores, characteristics, and clinical outcomes are provided in Table 1.
Discussion
This prospective study relied on the recently developed Carragee classification system. Carragee types II, III, and IV were identified intraoperatively in patients with single-level lumbar disc herniation, and posterior dynamic transpedicular stabilization with limited posterior lumbar microdiscectomy was performed. The purpose of this study was to prevent failed back syndrome by reducing the high rate of recurrent disc herniation observed in type II patients (described as fragment-defect) and to prevent the high rate of recurrent/persistent sciatica observed in type III and IV patients (fragment-contained and no fragment-contained, respectively). Ultimately, better clinical results resulted. This approach yielded lower reherniation rates and vastly improved clinical results.
Unlike previous disc herniation classifications, the Carragee system elaborates a new disc classification according to the presence of extruded/sequestered or sub-annular fragments and annular stability.8 In their series of 187 cases, Carragee et al8 reported recurrent/persistent sciatica, reherniation, and reoperation at a frequency of 1.1% among the type I group. The type I group had small annular fissures and sequestered fragments; they were treated with sequestrectomy. After performing sequestrectomy, we excluded the type I group from our study because of the positive clinical results. The clinical results and reherniation rates among the other 3 groups were not satisfactory. The rate of recurrent/persistent sciatica and reherniation in the type II (fragment-defect) group was as high as 27.3%; the reoperation rate was significantly high, at 21.2%. The rates of recurrent/persistent sciatica, reherniation, and reoperation among types III and IV were 11.9%, 9.5%, and 4.8%, respectively, and 37.5%, 12.5%, and 6.3%, respectively. In comparison to the Carragee type III group, the Carragee type IV group had much higher rates of recurrent/persistent sciatica. The Carragee type III group had a higher rate of recurrent/persistent sciatica than the Carragee type I group. Similarly, the rates of reherniation and reoperation observed in this study for Carragee types III and IV were not as high as those observed for the Carragee type II group; however, the rates were much higher than those observed for the type I group. Because of the study of Carragee et al, it was surmised that more satisfactory results and decreased rates of both recurrent herniation requiring reoperation and recurrent/persistent sciatica would follow a limited posterior lumbar microdiscectomy with posterior dynamic transpedicular stabilization. After evaluating the results of 40 cases, after at least 2 years’ follow-up, we observed no recurrent disc herniation. Recurrent/persistent sciatica rates were significantly lower in all 3 types examined compared with the study of Carragee et al and other studies.9, 17, 18
According to the relevant literature, unsatisfactory results are reported in 38% of patients who undergo lumbar discectomy.7, 19 Mochida et al20 confirmed that removing the disc material less aggressively yields better clinical and radiologic results. Williams13, 21 reported, for the first time, encouraging results after removing minimal tissue from the intervertebral disc space. His clinical success rate was 90%, and the rate of recurrence was 4% to 9%. Rogers22 described recurrent disc herniation, after removing only disc fragments, in 7 of 33 patients (21%). In a study by Thome et al,6 recurrent herniation was observed in 4 of 42 patients (10%). A recent study by Barth et al23 compared the results at 2 years’ follow-up for lumbar microdiscectomy and microscopic sequestrectomy. The microdiscectomy patient group presented deterioration in functional and radiologic results due to segmental degeneration at 2 years, whereas sequestrectomy was associated with better functional results after 2 years.
Some clinical and radiologic studies reported that looseness in the ligaments and facet joint capsules is observed with the decrease in disc altitude after disc operations. As a result, increased load on facet joints may cause segmental instability and spondylosis.4–6, 24, 25 Segmental instability in the lumbar spine is one of the reasons for failed back syndrome. Yorimitsu et al,26 in their follow-up study of more than 10 years, reported the frequency of chronic lower back pain, rather than sciatica, after lumbar disc surgery due to decreased disc space height as 75%. Lumbar instability can be confirmed both clinically and radiologically.27, 28 Studies examining clinical instability showed that radiologic findings were not always in agreement with clinical findings.29, 30 Notably, it is thought that degenerative disc disease is one of the major causes of spinal instability.28, 29, 31, 32 According to the literature, the rate of instability in patients with lumbar disc herniation is 20%.31, 32
Kotilainen and Valtonen33 treated 190 patients with single-level lumbar disc herniation by performing lumbar microdiscectomy. During the observation period, 10% of patients complained of sciatica and as many as 29% of patients had lower back pain. Clinical examination showed various signs and symptoms of segmental instability of the lumbar spine in 22% of the surgical patients. In another study Kotilainen et al34 reported poor clinical results in patients with protruded disc herniation, as compared with patients with sequestered fragments or prolapse, who displayed better results. According to Kotilainen et al, such results may arise because of segmental instability resulting from the diffuse nature of disc disease. Frymoyer and Selby31 acknowledged that massive central L4-5 disc herniation, which is often observed with severe low back pain, presents a remarkable situation and exhibits a tendency toward degenerative instability. The diffuse/massive-natured disc hernia descriptions of Kotilainen et al and Frymoyer and Selby are in line with the Carragee classification of the type IV group. In such cases Carragee et al8 removed protruded disc pieces via extensive annulotomy. They reported a very high rate of recurrent/persistent sciatica (37%) in this group. It is our opinion that the unsatisfactory results of Carragee et al were due to segmental instability; therefore limited discectomy with posterior dynamic transpedicular stabilization was performed in our patients.
The concept of dynamic stabilization was established to control abnormal motion by transferring the weight-bearing load carried by the spine without performing spinal segment fusion.35 Thus dynamic stabilizations aim to relieve the pain.35 Some recently published studies showed that dynamic stabilization (by use of a dynamic pedicular screw–rod system) biomechanically provides stability that is similar to that provided by rigid systems.36 Moreover, theoretically, it is thought that dynamic stabilization systems have advantages over rigid spinal implants. It is an easier surgery to perform, requires a shorter operative time, and does not have the associated risks of donor-site pain, pseudarthrosis, and adjacent segment degeneration that fusion surgery entails.37, 38 Studies by Schaeren et al39 and Stoll et al40 reported good clinical results from the procedure and recommended dynamic stabilization as a safe and effective method of treatment for patients with degenerative chronic instability. Putzier et al37 reported that disc degenerations showed far less progression in patients who had nucleotomy with posterior dynamic system applications than patients who did not have dynamic stabilization after 34 months’ follow-up. In our experience, posterior dynamic transpedicular stabilization decelerates the degeneration of disc tissue (Fig. 2). It can reduce the occurrence of failed back syndrome. In this study dynamic fixation was a non–Food and Drug Administration–approved indication for this procedure. This study and favorable results in the literature have shown that posterior dynamic transpedicular stabilization can be used in segmental degenerative instability to reduce the risk of failed back syndrome or recurrent disc herniation and to decrease the frequency of postoperative sciatica and mechanical low back pain. This seems to be a compelling argument for a new indication for use of posterior dynamic transpedicular stabilization.

MRI scans in 38 year-old female patient, showing L5 transitional vertebrae and disc herniation in Carragee group IV. The patient had severe back pain and sciatica. (A) The preoperative MRI scan shows a moderate black disc and diffuse bulging. (B) The postoperative MRI scan after posterior dynamic transpedicular stabilization shows deceleration in the degeneration process.
In this prospective study we performed limited lumbar microdiscectomy in single-level disc herniation patients who were grouped according to the Carragee classification system as type II, III, or IV. To obtain more satisfactory clinical results and to decrease the rates of instability due to segmental degeneration, as well as to reduce the rates of recurrent disc herniation and recurrent/persistent sciatica with failed back syndrome, we also performed posterior dynamic transpedicular stabilization in the same patients. This approach yielded much improved clinical results.
The main deficiency of this study is short follow-up. The study of Carragee et al,8 which served as the cornerstone for our study, had a median follow-up period of 6 years, with minimum follow-up of 2 years, and the recurrence of symptoms occurred after a long time interval. More clinical studies need to show the positive results after posterior dynamic transpedicular stabilization with limited lumbar discectomy.
- © 2010 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.