


Abstract
Background Total disc replacement (TDR) and total facet replacement (TFR) have been the focus of recent kinematics evaluations. Yet their concurrent function as a total joint replacement of the lumbar spine's 3-joint complex has not been comprehensively reported. This study evaluated the effect of a TFR specifically designed to replace the natural facets and supplement the function with the natural disc and with TDR. The ability to replace degenerated facets to complement a pre-existing or simultaneously implanted TDR may allow surgeons to completely address degenerative pathologies of the 3-joint complex of the lumbar spine. We hypothesized that TFR would reproduce the biomechanical function of the natural facets when implanted in conjunction with TDR.
Methods Lumbar spines (L1-5, 51.3 ± 14.2 years, N = 6) were tested sequentially as follows: (1) intact, (2) after TDR implantation, and (3) after TFR implantation in conjunction with TDR, all at L3-4. Specimens were tested in flexion-extension (+ 8 Nm to − 6 Nm), lateral bending (± 6 Nm), and axial rotation (± 5 Nm). A 400 N compressive follower preload was applied during flexion-extension tests. Three-dimensional segmental motion was recorded and analyzed using analysis of variance in Systat (Systat Software Inc., Chicago, Illinois) and multiple comparisons with Bonferroni correction.
Results The TDR implantation (TDR + natural facets) allowed similar lateral bending (P = .66), but it generally increased flexion-extension (P = .06) and axial rotation (P < .05) range of motion (ROM) at the implanted level compared to intact. The TFR + TDR (following replacement of the natural facets with TFR) decreased ROM to levels similar to intact in lateral bending (P = .70) and axial rotation (P = .23). The TFR + TDR flexion-extension ROM was reduced in comparison to intact and TDR + natural facets (P < .05).
Conclusions The TFR with TDR was able to restore stability to the lumbar segment after bilateral facetectomy, while allowing near-normal motions in all planes.
The clinical presence of motion preserving devices in the lumbar spine has been advanced by the approval of total disc replacements (TDR) such as the CHARITÉ Artificial Disc (DePuy Spine, Raynham, Massachusetts) and the ProDisc-L (Synthes Spine, West Chester, Pennsylvania). Extending the notion of functional replacement of the spinal anatomy, facet replacement devices have recently seen investigation in clinical studies and kinematic studies.
As total facet replacement (TFR) becomes a more accepted interventional treatment in the lumbar spine, it likely will be combined clinically with anterior column restoration, such as TDR. Recent literature has reported that TDR implantation can alter the loading on the facets1–3 and in some clinical cases degenerative changes in the facets have been observed.4, 5 Additionally, facet arthrosis is a contraindication for treatment with TDR, limiting the patient population.6 As such, replacement of both the natural disc and the natural facets is probable, and it is critical to understand the functional biomechanics of associated TDR and TFR prior to clinical use.
The function of each TDR design may alter the native biomechanics of the spine, and care should be taken in the design of a TFR to be used as an adjunct device. The TFR may require specific features so as not to alter the function of the TDR while protecting the unaltered anatomy. A functional TFR must account for the mechanical interaction of the entire joint. The natural facets provide graded resistance to motion through complementary mechanics of the facet capsule and opposing articulating surfaces. The TFAS-TL (Archus Orthopedics, Inc., Redmond Washington) couples a spherical cephalad bearing that is mated with a cuplike caudal bearing. The profile of the caudal bearing provides graded resistance to angular motion of the associated functional spinal unit in the 3 major planes of motion similar to the natural anatomy. Specifically, it was designed to complement an unconstrained TDR while allowing the native elements of the spine to continue their function in stabilizing and controlling the lumbar spine.
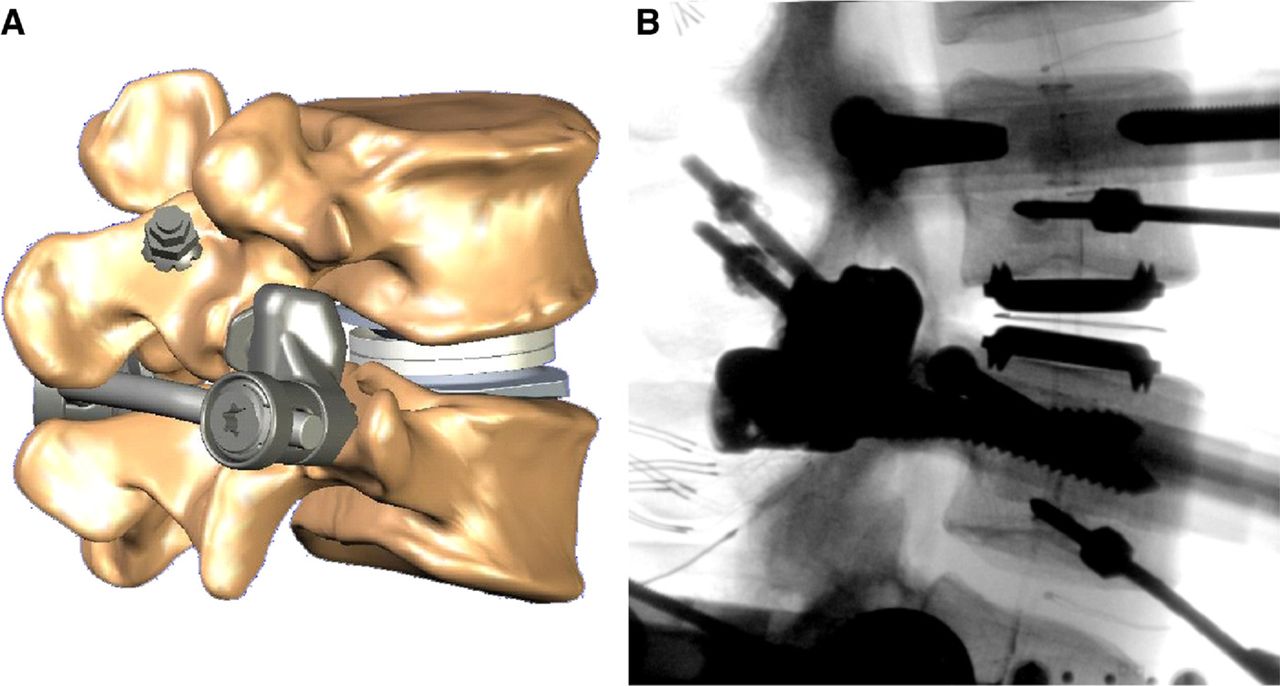
This study evaluated the functional performance of the TFAS-TL (TFR, Fig. 1) when coupled with an unconstrained CHARITÉ Artificial Disc (TDR). We hypothesized that a TFR will reproduce the biomechanical function of the natural facets when implanted in conjunction with a TDR.

Representative illustration (A) and photo (B) of an implanted TFAS-TL.
Materials and methods
Specimens and experimental setup
Six fresh-frozen human cadaveric spines (L1-5, mean age: 51.3 ± 14.2 years) with no previous spinal surgery and without bridging osteophytes and osteoporosis were tested. Prior to testing, the specimens were thawed for 24 hours at room temperature (approximately 20°C) and the paravertebral muscles were carefully resected to prevent iatrogenic damage to the discs, ligaments, and posterior elements. Hydration of the discs during testing (at room temperature) was maintained by wrapping the discs in saline-soaked towels.
The terminal vertebrae were potted using bone cement and pins, and the L5 vertebral body was fixed to a 6-axis load cell (Model MC3A-6-250; AMTI Inc., Watertown, Massachusetts) and the L1 vertebral body was unconstrained.
Specimens were tested by applying a moment to the L1 vertebra in flexion-extension (+8 Nm to −6 Nm), lateral bending (±6 Nm), and axial rotation (±5 Nm). The moment was applied by controlling the flow of water into bags attached to loading arms fixed to the L1 vertebra. This technique allows for minimal application of shear forces to the specimen.
A 400 N compressive follower preload was applied during flexion-extension tests to stabilize the spine under physiologic loads.7
Biaxial angle sensors (Applied Geomechanics Inc., San Francisco, California) were mounted on each vertebra to provide real-time feedback for the optimization of the follower load path (via a cable and guide mounts connected to each vertebral body) so that changes in lumbar lordosis were minimized. Follower load was not applied during lateral bending and axial rotation due to the potential for erroneous results with the current test setup.
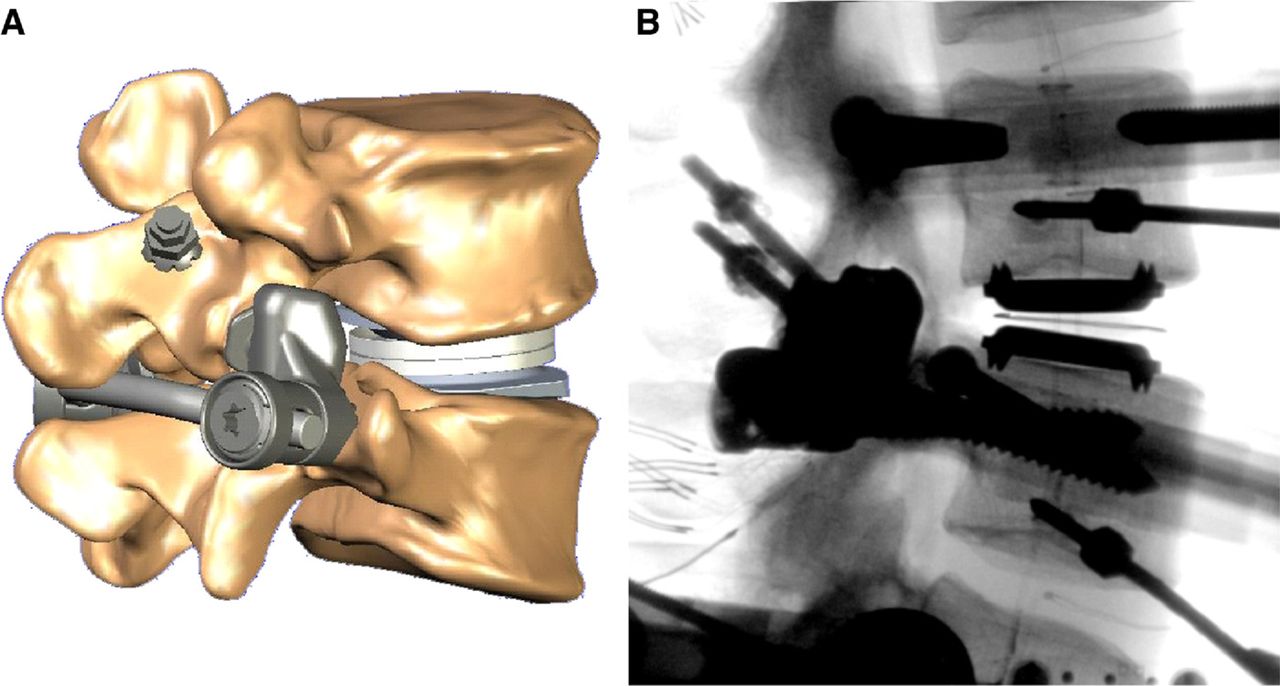
Each specimen was tested in the following order: (1) intact; (2) after TDR implantation, (3) after TFR implantation in conjunction with TDR (Fig. 2), all at L3-4. The independent motion of each vertebral body relative to the potted caudal segment (L5) was measured using optoelectronic components (Optotrak 3020, Northern Digital Inc., Waterloo, Ontario, Canada). During implantation and flexion-extension testing, implant and vertebral positioning were monitored using fluoroscopic imaging (OEC 9800 Plus digital fluoroscopy machine; GE Healthcare, United Kingdom).
Representative illustration (A) and X-ray (B) of an implanted TFAS-TL construct with a CHARITÉ TDR.
Statistical methods
Load-displacement curves were analyzed to determine L3-4 angular range of motion (ROM) in flexion-extension, lateral bending, and axial rotation. Additionally, L3-4 segmental stiffness values (Nm/degree) were calculated using previously described techniques.8
The statistical analysis was performed using repeated-measures analysis of variance in Systat (Systat Software Inc., Chicago, Illinois) and post hoc tests using Bonferroni correction for multiple comparisons. The following pair-wise comparisons were made: (1) intact versus TDR, (2) intact versus TDR + TFR, and (3) TDR versus TDR + TFR.
Results
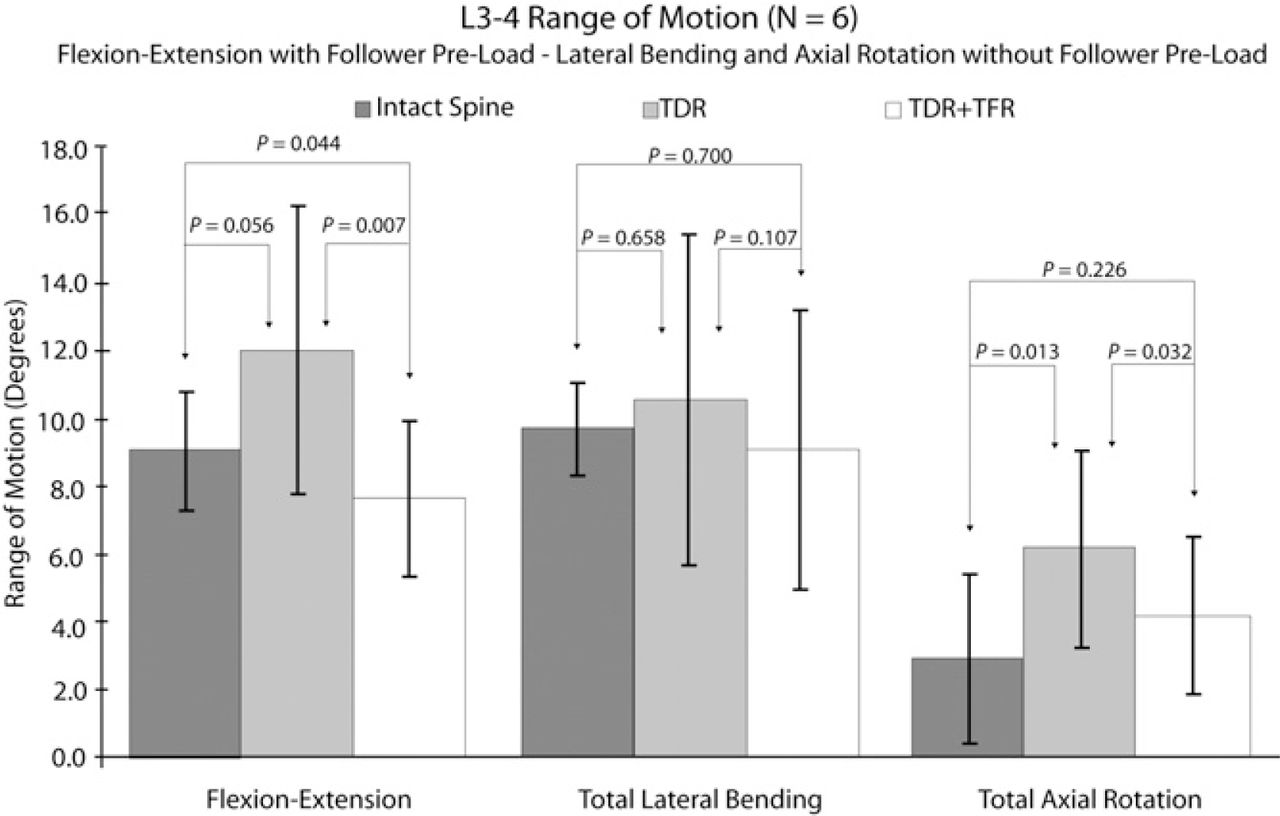
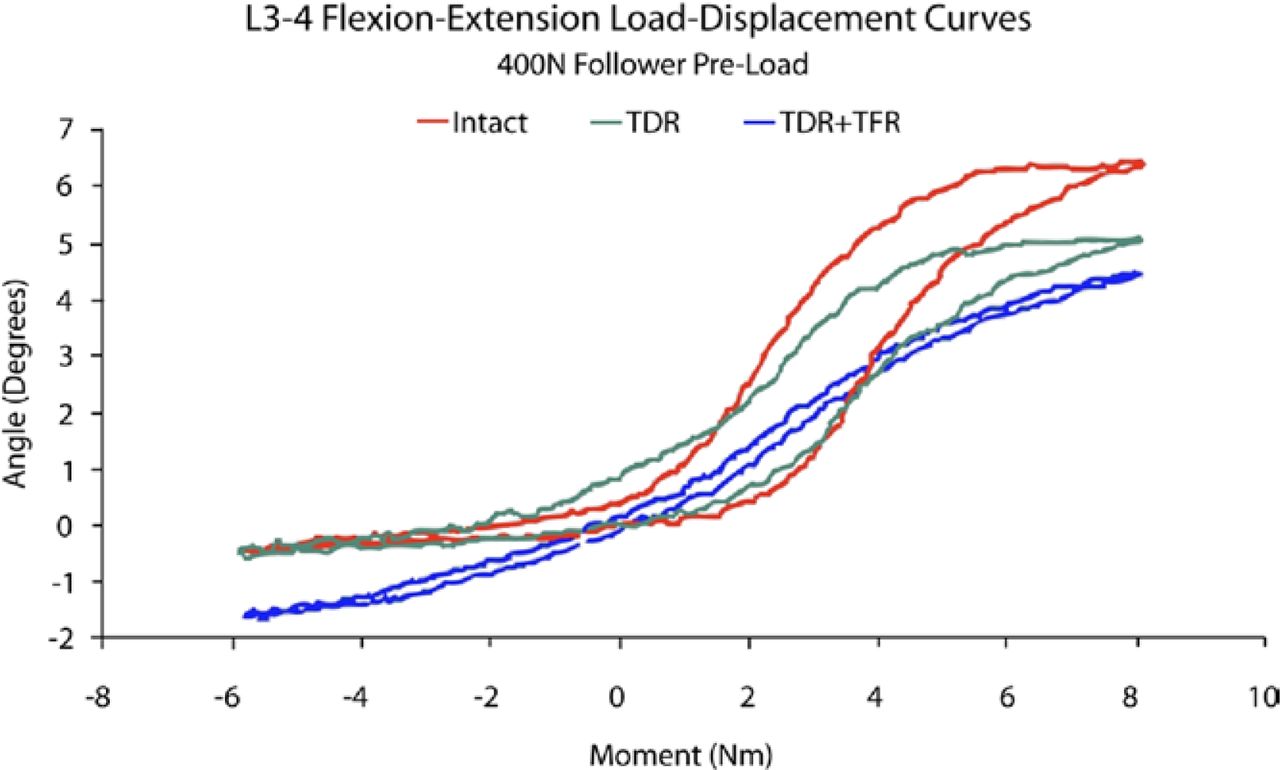
The TDR implantation (with natural facets) allowed similar lateral bending (P = .66), but it generally increased flexion-extension (P = .06) and axial rotation (P < .05) ROM at the implanted level compared to intact. The TFR implantation with complementary TDR (TDR + TFR) decreased ROM to levels similar to intact in lateral bending (P = .70) and axial rotation (P = .23) (Fig. 3). The TDR + TFR flexion-extension ROM was reduced in comparison to intact and TDR with natural facets (P < .05). Figure 3 details the average ROM levels for each condition in each motion. Figure 4 demonstrates a typical flexion-extension moment curve for one specimen.
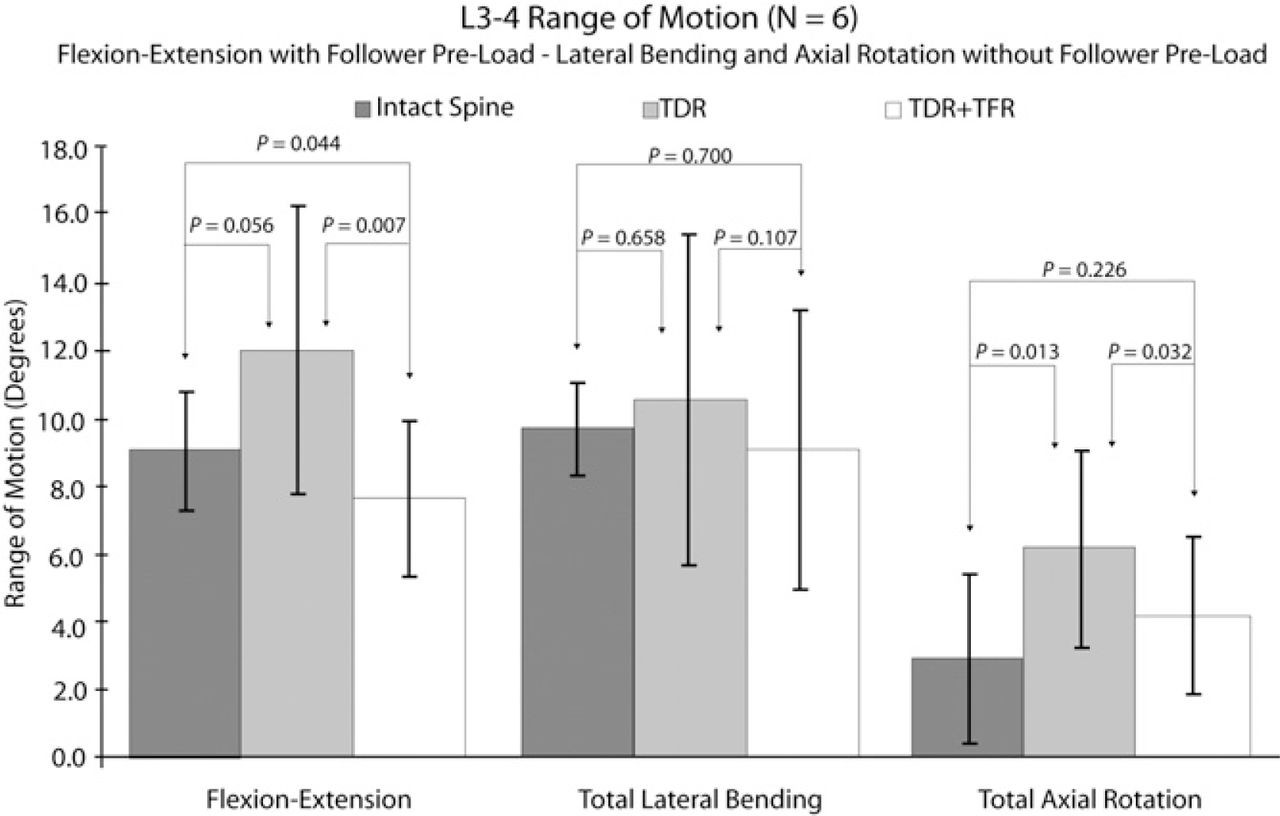
Average L3-L4 range of motion.
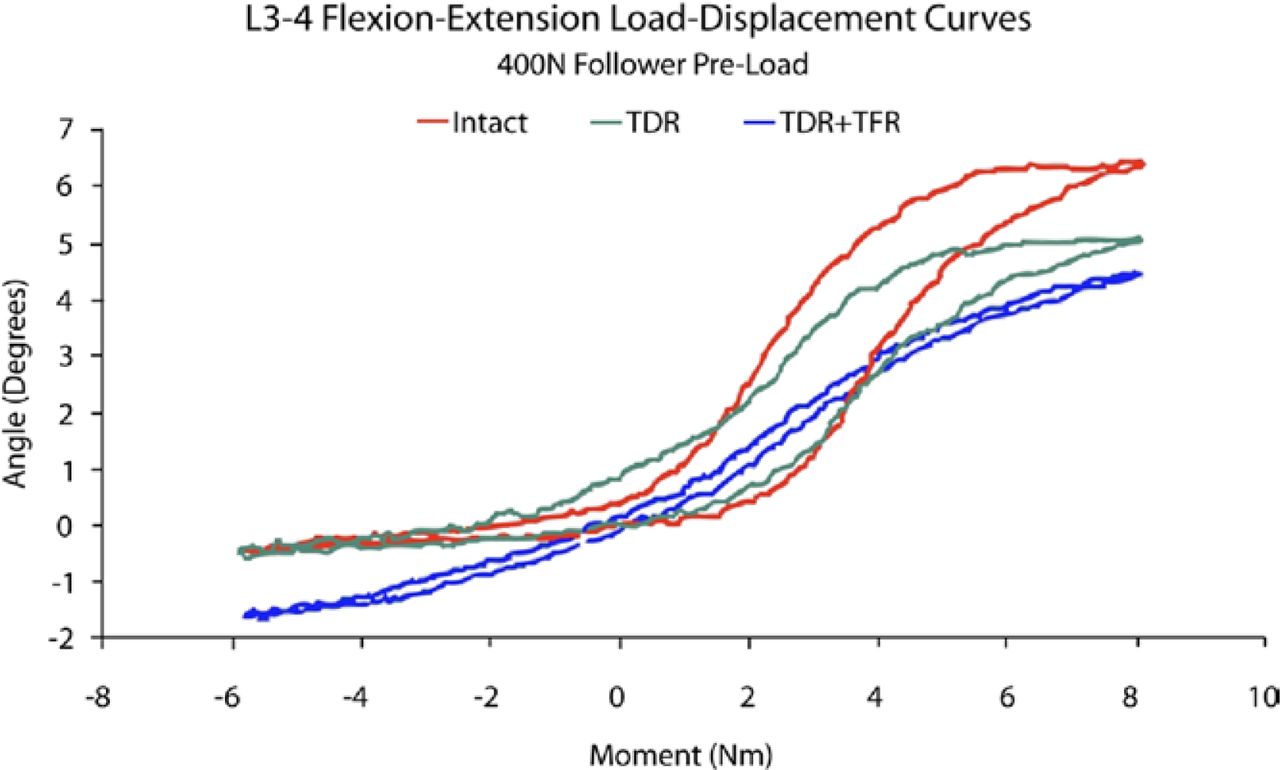
Typical flexion-extension moment versus angle curve for operated level.
Discussion
The TFR (Fig. 1) is designed to replace the facets in the lumbar spine after total facetectomy.8 It's design provides for articulation of spherical bearings, rigidly connected to the lamina of the superior vertebral body, over two socket type bearings connected to the inferior vertebral body via pedicle screws. The caudal bearing's design promotes replication of the natural anatomy's function via surface profiles that, in flexion-extension, lateral bending, and axial rotation, provide both graduated resistance to angular motion and limits to prevent excessive motion and maintain stability. The natural facets act to guide proper motion in both flexion and lateral bending, but in extension and axial rotation they also function as a limiter at the extremes of motion to prevent instability. As such, when coupled with a TDR, the requirement of a TFR to prevent instability is magnified, particularly in axial rotation and extension, to ensure stability of the restored segment.
The TFR with TDR was able to restore stability to the lumbar segment after bilateral facetectomy, while allowing near normal motions in all planes. The ROM of the segment in lateral bending and axial rotation with TDR and TFR was generally similar to intact and within physiological norms, maintaining proper stability. While the flexion-extension ROM of TDR + TFR was statistically significantly smaller than intact and also with TDR with natural facets (P = 0.044), the resultant motion averaged 7.6 ± 2.2°, and was only 1.4 ± 1.3° smaller than the motion of the intact specimens in our sample. It should be noted that this was an in vitro study using human cadaveric specimens and the sample size was relatively small (N = 6).
The kinematic analysis did not include calculations of the center of rotation of the lumbar segments before and after implantations of the artificial disc as well as the artificial facets. When an artificial facet replacement is used in conjunction with an artificial disc, the centers of rotation of the two devices must be complementary in order for the two devices to function together. A disc prosthesis with a mobile core, such as the TDR discussed in this study, could potentially adapt to the kinematics of the facet replacement prosthesis. Further studies are needed to investigate the behavior of the center of rotation of the implanted segment in these scenarios using disc prostheses of different designs.
These results suggest that together, TDR and TFR function synergistically without one device compromising the performance of the other. Clinically, the ability to replace degenerated facets to complement a preexisting or simultaneously implanted TDR may allow surgeons to address degenerative pathologies of the 3-joint complex of the lumbar spine.
Extended references
Total disc replacement positioning affects facet contact forces and vertebral body strains.
Rundell SA, Auerbach JD, Balderston RA, Kurtz SM.
STUDY DESIGN: A validated nonlinear three-dimensional finite element (FE) model of a single lumbar motion segment (L3-L4) was used to evaluate the effects of total disc replacement (TDR). The model was implanted with a fixed-bearing TDR (ProDisc-L) at 2 surgically relevant positions and exercised about the 3 anatomic axes. Facet forces, range of motion (RoM), and vertebral body strains were evaluated. OBJECTIVE: The objective of the current study was to evaluate how TDR implantation and positioning affects facet joint forces and vertebral body strains. We hypothesized that facet contact forces (FCFs) would increase with TDR to compensate for the loss of periprosthetic load-bearing structures, and that vertebral body strains would increase in the region around the metallic footplates. SUMMARY OF BACKGROUND DATA: TDR has the potential to replace fusion as the gold standard for the treatment of painful degenerative disc disease. However, complications after TDR include index level facet arthrosis and implant subsidence. Alterations in facet and vertebral body loading after TDR and their dependence on implant positioning are not fully understood. METHODS: An FEM of L3-L4 was created and validated using RoM, disc pressure, and bony strains from previously published data. A TDR was incorporated into the L3-L4 spine model. All models were subjected to a compressive follower load of 500 N and moments of 7.5 Nm about the 3 anatomic axes. RESULTS: Overall RoM and FCFs tended to increase with TDR. FCFs increased by an order of magnitude during flexion. Posterior placement of the device resulted in an unloading of the facets during extension. Areas of strain maxima were observed in the anterior portion of the vertebral body during flexion after TDR. The area of initial bone resorption signal under the metal footplate was greater when the device was anteriorly placed. CONCLUSION: The current study predicted a decrease in segmental rotational stiffness resulting from TDR. This resulted from the removal of load bearing soft tissue structures, and caused increased loading in the facets. Additionally, vertebral body strains were generally higher after TDR, and tended to increase with decreased rotational stiffness. Posterior placement of the device provided a more physiologic load transfer to the vertebral body.
Degenerative changes of discs and facet joints in lumbar total disc replacement using ProDisc II: minimum two-year follow-up.
Park C-K, Ryu K-S, Jee W-H.
STUDY DESIGN: A retrospective clinical and radiologic data analysis. OBJECTIVE: To determine the radiologic changes in the discs at the adjacent levels and facets at the index and adjacent levels after total disc replacement (TDR) using ProDisc II in a minimum 2-year follow-up. SUMMARY OF THE BACKGROUND DATA: The main purposes of TDR are to preserve the physiologic segmental motion at index level, and to prevent accelerated degeneration at the index and adjacent segments. However, there are few reports dealing with the effects of TDR on the degenerative changes in a long-term followup. METHODS: After TDR using ProDisc II, the degree of disc and facets degeneration at the index and adjacent levels was assessed by observing lumbar magnetic resonance imaging (MRI) and computed tomography (CT) images before surgery and at minimum 26 months after operations. The degenerative changes of the discs and facets were determined in relation to the clinical outcome, various perioperative factors, and prosthesis factors. RESULTS: Thirty-two patients with 41 TDR included in this investigation. The progression of facets degeneration (PFA) was observed in 12 of 41 TDR levels. Among 47 adjacent segments, the progression of disc degeneration and PFA were observed in 2 levels (4.3%), and 3 levels (6.4%), respectively. All cases of PFA occurred only in those with preoperative degeneration of grade 1. PFA at the index segments was positively related with female in gender (P = 0.008), the malposition of prosthesis on frontal plane (P = 0.025), and 2-level TDR in the number of TDR level (P = 0.008). CONCLUSION: After TDR using ProDisc II, the degenerative changes in the discs and facets at the adjacent segments appeared to be minimal. However, in 29.3% of the TDR segments, the facet joints presented PFA, which was more common in female, malposition of prosthesis on frontal plane, and 2-level TDR in a minimum 2-year follow-up.
Incidence of contraindications to total disc arthroplasty: a retrospective review of 100 consecutive fusion patients with a specific analysis of facet arthrosis.
Wong DA, Annesser B, Birney T, et al.
BACKGROUND CONTEXT: The role of total disc arthroplasty (TDA) in the treatment of spinal pathology is unclear. TDA has been touted as an alternative to fusion. However, not all back pain is purely discogenic in origin. Contraindications to TDA exist. At Spine Week in Porto, Portugal, Cammisa's group from the Hospital for Special Surgery in New York presented a series of 56 fusions where 100% of patients had one or more of 10 contraindications to TDA. En face, this appears to be an extremely large number. PURPOSE: The purpose of the study was to repeat the Hospital for Special Surgery study in another cohort of fusion patients. STUDY DESIGN/SETTING: This study was an independent, retrospective record review of 100 consecutive lumbar spinal fusions performed at a tertiary care private medical center. PATIENT SAMPLE: All adult patients having primary 1–3 level lumbar spinal fusions from January 2003 to May 2004 were assessed. OUTCOME MEASURES: Physiologic measures included imaging, range of motion, and response to facet blocks. METHODS: A retrospective chart review was performed of 100 consecutive patients having primary 1–3 level lumbar fusion by all five active staff spinal surgeons (3 orthopedic and 2 neurosurgeons). The review was performed independently by the doctorate level physiotherapist who serves as the medical center's research coordinator, reporting to the chairman of the Hospital institutional review board. The same 10 contraindications from Cammisa's study were noted. Additional facet arthrosis data were collected, including mention on imaging reports or operating room notes. Clinical notes were reviewed for documentation of range of lumbar motion (ROM) and whether there was restricted or painful extension ROM. Note was made if patients had facet blocks as another clinical indicator of facet arthrosis. RESULTS: All 100 patients had at least one contraindication to TDA. The average was 3.69 (range 1–7). Only one patient had facet arthrosis as their only contraindication. Facet arthrosis was documented on imaging reports or operating room notes in 97/100. Reduced extension was present in 71/75 charts that documented ROM. Facet blocks were performed in 12/100 and gave greater than 50% relief in nine. CONCLUSIONS: Both our study and Cammisa's indicate that all lumbar fusion patients in our two institutions have at least one contraindication to TDA. The average fusion patient does not appear to have isolated discogenic pain. A large proportion of the patients appeared to have facet arthritis. The point where facet arthrosis definitely constitutes a contradiction to TDA will require analysis during long-term arthroplasty follow-up studies. Suitable patients for TDA may not represent a significant cohort presently undergoing lumbar fusion.
A follower load increases the load-carrying capacity of the lumbar spine in compression.
Patwardhan AG, Havey RM, Meade KP, Lee B, Dunlap B.
STUDY DESIGN: An experimental approach was used to test human cadaveric spine specimens. OBJECTIVE: To assess the response of the whole lumbar spine to a compressive follower load whose path approximates the tangent to the curve of the lumbar spine. SUMMARY OF BACKGROUND DATA: Compression on the lumbar spine is 1000 N for standing and walking and is higher during lifting. Ex vivo experiments show it buckles at 80 –100 N. Differences between maximum ex vivo and in vivo loads have not been satisfactorily explained. METHODS: A new experimental technique was developed for applying a compressive follower load of physiologic magnitudes up to 1200 N. The experimental technique applied loads that minimized the internal shear forces and bending moments, made the resultant internal force compressive, and caused the load path to approximate the tangent to the curve of the lumbar spine. RESULTS: A compressive vertical load applied in the neutral lordotic and forward-flexed postures caused large changes in lumbar lordosis at small load magnitudes. The specimen approached its extension or flexion limits at a vertical load of 100 N. In sharp contrast, the lumbar spine supported a load of up to 1200 N without damage or instability when the load path was tangent to the spinal curve. CONCLUSIONS: Until this study, an experimental technique for applying compressive loads of in vivo magnitudes to the whole lumbar spine was unavailable. The load-carrying capacity of the lumbar spine sharply increased under a compressive follower load, as long as the load path remained within a small range around the centers of rotation of the lumbar segments. The follower load path provides an explanation of how the whole lumbar spine can be lordotic and yet resist large compressive loads. This study may have implications for determining the role of trunk muscles in stabilizing the lumbar spine.
Effect of the total facet arthroplasty system after complete laminectomy-facetectomy on the biomechanics of implanted and adjacent segments.
Phillips FM, Tzermiadianos M, Voronov LI, et al.
BACKGROUND CONTEXT: Lumbar fusion is traditionally used to restore stability after wide surgical decompression for spinal stenosis. The Total Facet Arthroplasty System (TFAS) is a motion-restoring implant suggested as an alternative to rigid fixation after complete facetectomy. PURPOSE: To investigate the effect of TFAS on the kinematics of the implanted and adjacent lumbar segments. STUDY DESIGN: Biomechanical in vitro study. METHODS: Nine human lumbar spines (L1 to sacrum) were tested in flexion-extension (+8 to −6Nm), lateral bending (+/− 6Nm), and axial rotation (+/− 5Nm). Flexion-extension was tested under 400 N follower preload. Specimens were tested intact, after complete L3 laminectomy with L3-L4 facetectomy, after L3-L4 pedicle screw fixation, and after L3-L4 TFAS implantation. Range of motion (ROM) was assessed in all tested directions. Neutral zone and stiffness in flexion and extension were calculated to assess quality of motion. RESULTS: Complete laminectomy-facetectomy increased L3-L4 ROM compared with intact in flexion-extension (8.7 +/− 2.0 degrees to 12.2 +/− 3.2 degrees, p < .05) lateral bending (9.0 +/− 2.5 degrees to 12.6 +/− 3.2 degrees, p = .09), and axial rotation (3.8 +/− 2.7 degrees to 7.8 +/− 4.5 degrees p < .05). Pedicle screw fixation decreased ROM compared with intact, resulting in 1.7 +/− 0.5 degrees flexion-extension (p < .05), 3.3 +/− 1.4 degrees lateral bending (p < .05), and 1.8 +/− 0.6 degrees axial rotation (p = .09). TFAS restored intact ROM (p > .05) resulting in 7.9 +/− 2.1 degrees flexion-extension, 10.1 +/− 3.0 degrees lateral bending, and 4.7 +/− 1.6 degrees axial rotation. Fusion significantly increased the normalized ROM at all remaining lumbar segments, whereas TFAS implantation resulted in nearnormal distribution of normalized ROM at the implanted and remaining lumbar segments. Flexion and extension stiffness in the high-flexibility zone decreased after facetectomy (p < .05) and increased after simulated fusion (p < .05). TFAS restored quality of motion parameters (load-displacement curves) to intact (p > .05). The quality of motion parameters for the whole lumbar spine mimicked L3-L4 segmental results. CONCLUSIONS: TFAS restored range and quality of motion at the operated segment to intact values and restored near-normal motion at the adjacent segments.
Acknowledgment
Institutional research support provided by the Department of Veterans Affairs, Washington, D.C., and Archus Orthopedics, Inc., Redmond, WA.
Footnotes
Investigation performed at the Musculoskeletal Biomechanics Laboratory, Edward Hines Jr. VA Hospital, Hines, Illinois
Conflicts of Interest: Simon G. Sjovold, MASc, Archus Orthopedics, Employee; Michael Funk, MS, Archus Orthopedics, Employee; David M. Rosler, MS, Archus Orthopedics, Employee; Avinash G. Patwardhan, PhD, Loyola University Chicago, Institutional research support provided by the Department of Veterans Affairs, Washington, D.C., and Archus Orthopedics, Inc., Redmond, WA.
- © 2009 SAS - The International Society for the Advancement of Spine Surgery. Published by Elsevier Inc. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution-Noncommercial 3.0 Unported License, permitting all non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Investigation performed at the Musculoskeletal Biomechanics Laboratory, Edward Hines Jr. VA Hospital, Hines, Illinois
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.