


Abstract
Standard surgical approach for extradural paraspinal tumours has been through a unilateral facetectomy, inter-transverse or retroperitoneal approach. Some of these approaches destabilise the spine and consequently require a fusion procedure. Access to these tumours through a minimal access route can decrease tissue damage, fasten post-operative recovery and obviate the need for a concomitant fusion procedure. However, proper case selection and adequate pre-operative planning are important in choosing cases for a minimally invasive approach.
We discuss three cases of giant extradural, paraspinal schwannomas. One case that was associated with listhesis along with the tumour situated more anteriorly and embedded in the psoas muscle was managed by lateral retroperitoneal route with simultaneous interbody graft followed by posterior interspinous stabilising device. The other two cases were managed by minimal access route using a 22mm fixed tubular retractor, one by a paramedian approach and one by far lateral approach. The technique and merits of the procedure are discussed.
Introduction
Nerve sheath tumours are the most common spinal neoplasms and make up for 40% of extramedullary tumors of the spinal column.1–4 Majority of these lesions are purely intradural (50-80%) or intradural with extradural extension (10-20%). Purely extradural schwannomas account for 1-10% of all spinal schwannomas2, 3, 5, 6, 7 and are more often seen in the cervical region. Lumbar extradural schwannomas have accounted for 2.4-3.2% of all nerve sheath tumours.3, 4
Complete surgical excision is the treatment of choice in schwannomas anywhere in the spinal axis.1 Extradural tumours require a more extensive approach with longer incisions, adequate exposure lateral to the facet joint and a partial or complete facetectomy.1, 3–5, 8 Some tumours may need to be addressed by a multi-stage approach 9, 10 and also necessitate a concomitant fusion procedure to avoid subsequent instability, thus adding to the surgical morbidity.1, 3
Minimal access spinal techniques (MAST) have ushered in a new concept in spine surgery and are being increasingly used to treat a variety of spinal pathologies, most notably degenerative spine diseases. Recently, these techniques have also been used to treat spinal tumours and intradural pathologies with considerable success.1, 3, 8, 11–15 Minimal access techniques reduce tissue destruction, thus resulting in reduced blood loss and post-op pain, quicker post-operative recovery and can obviate the need for a concomitant fusion procedure when used to treat extradural and foraminal tumours.4
We report 3 cases of giant lumbar extradural, paraspinal schwannomas. One of them was managed by a mini-open retroperitoneal approach, while the other two were removed using fixed tubular retractor. A brief technical note on the minimally invasive approach and its merits are discussed.
Case 1
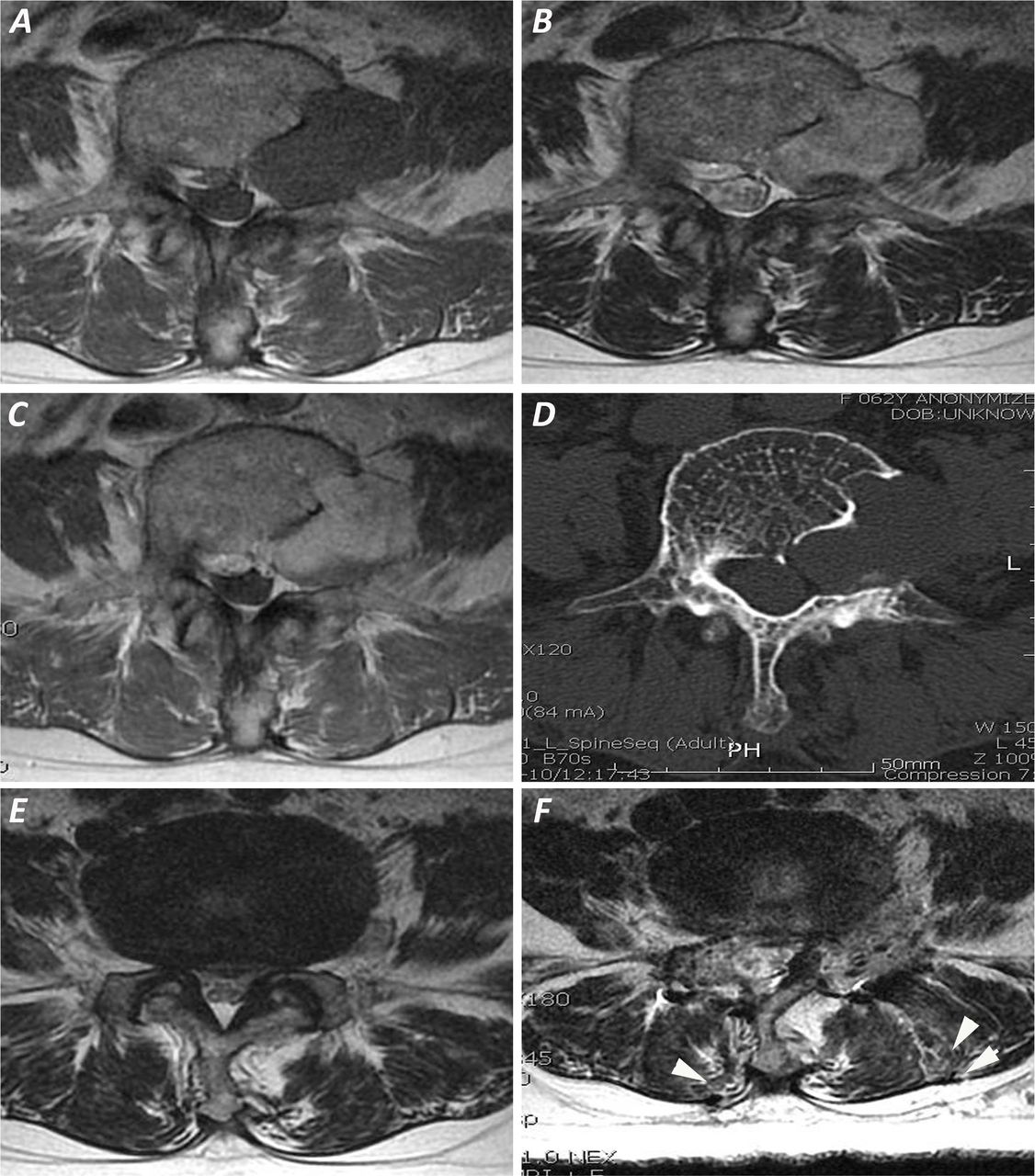
A 62 yr lady presented with history of low back pain, right leg pain, neurogenic claudication and weakness of right great toe dorsiflexion. Imaging revealed spinal stenosis at L4-5 (Figure 1E) and a well defined contrast enhancing lesion on the left side of L4 body (3.4x2.2x2 cm) encroaching on adjacent pedicle (Figure 1A-D).
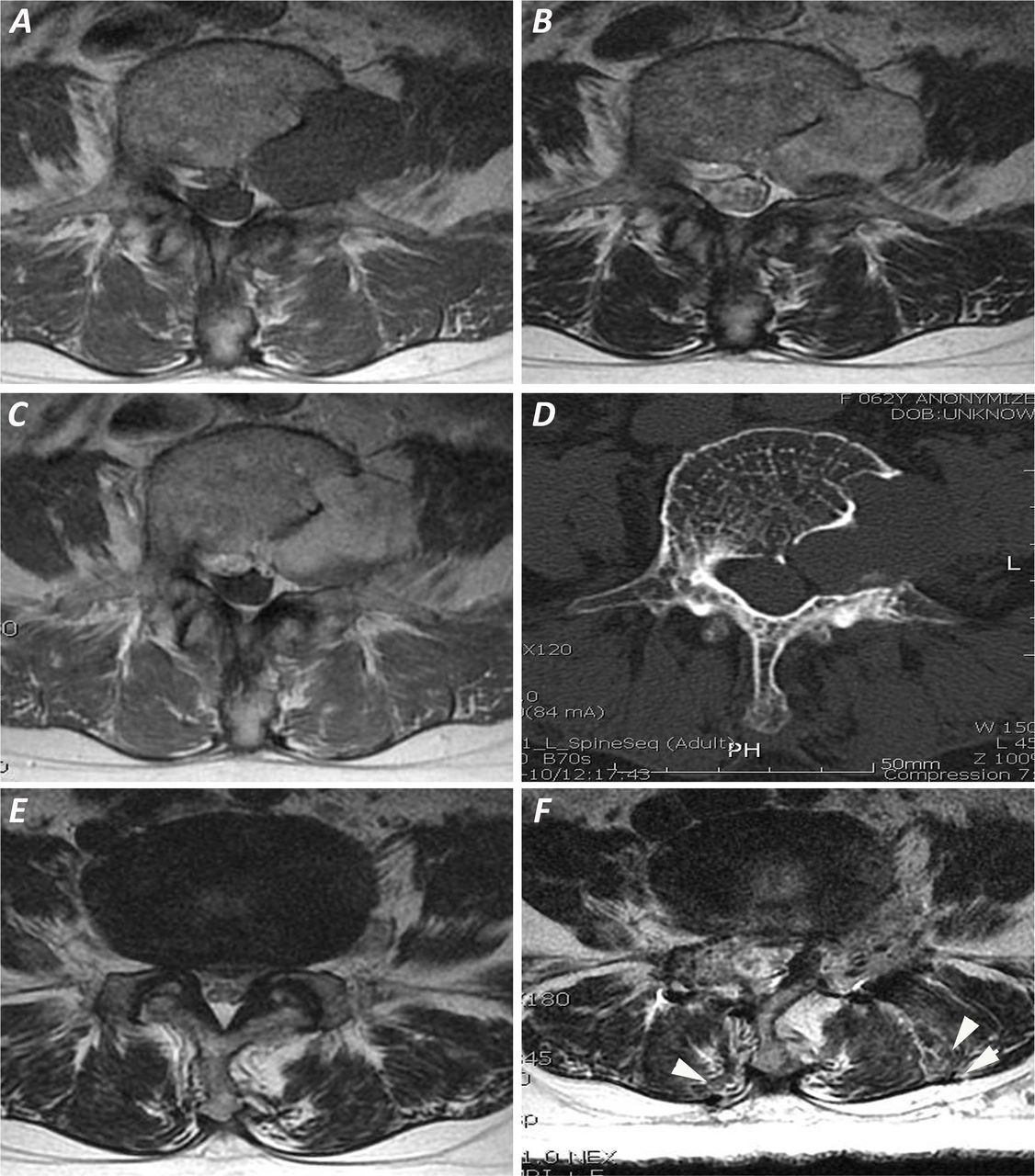
T1W (A), T2W (B) and Contrast enhanced (C) axial MRI sections showing an extradural tumour on left side of L4 body with large foraminal component. Axial CT scan section (D) at the level of tumour showing scalloping of L4 body due to the tumour with a widened foramina. T2W axial section (E) at the level of L4-5 disc showing diffuse disc bulge with lateral recess stenosis. Post-operative MRI (F) showing gross total tumour resection and right medial facetectomy and spinal decompression. Grade 1 signal changes in the paraspinal muscle due to the far lateral track on the left side (double arrowheads) and paramedian track on the right side (single arrowhead) can be noted (22).
This patient required treatment for the left L4 extradural lesion and L4-5 spinal stenosis. After initial preparation (prone position, Epidural analgesia), a vertical 2cm incision was placed 5 cm lateral to the midline overlying the L4 body and an 18mm tubular retractor was docked directed medially so as to visualise the lateral part of facet complex and the inter-transverse area lateral to it. The lateral part of facet joint and medial part of the upper transverse process was drilled, inter-transverse ligament and muscle were removed to visualise the left L4 nerve coursing over the tumour. The nerve was mobilised from the tumour capsule, internal decompression followed by total capsular excision was done. The medial facet was preserved and the most medial portion of the tumour was mobilised using a right angled probe directed through the foramen anterior to the nerve root. Anatomical integrity of the L4 nerve confirmed after excision. Following this, a 2cm vertical incision was placed over L4-5 disc space, 1 cm to the right of the midline and bilateral decompression done with an 18mm fixed tube. Post-operative period was uneventful. Post-op MRI showed gross total tumour removal with adequate dural tube decompression (Figure 1F). Histopathological report was Cellular schwannoma.
Case 2
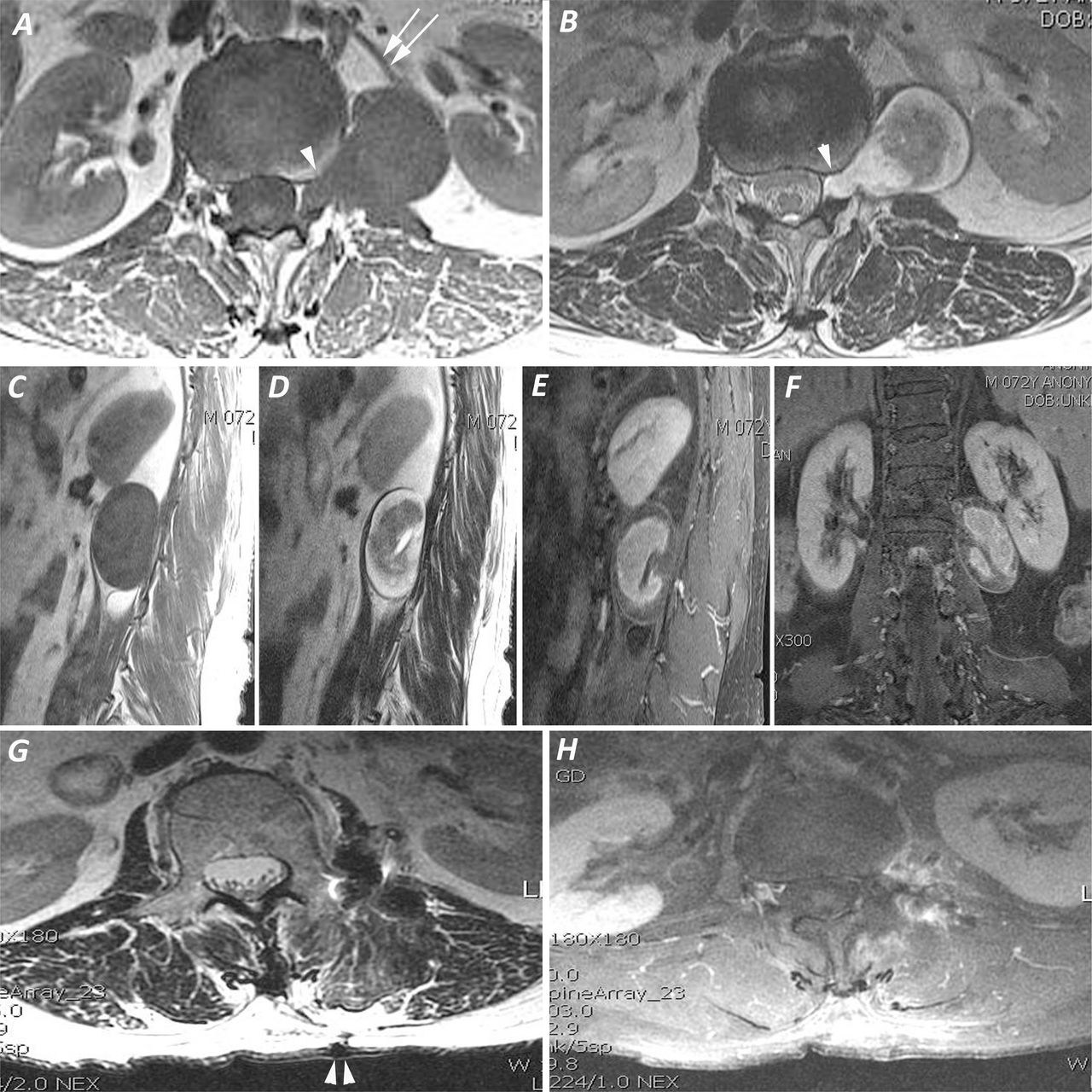
A 63 yr old lady presented with left lower limb radicular pain and normal neurological examination. MRI revealed a large (5.3x3.1x3.3 cm) enhancing lesion in the left lateral aspect of L1 and L2 vertebral bodies with a small extension into the L1-2 foramina (Figure 2A-F ). In this case, while using a classical far lateral approach with the tubular retractor, the lesion would be broadest just beneath the tubular aperture and the extent of manoeuvring the tubular retractor to visualise the entire extent of the lesion may be more. Also, with a lateral to medial trajectory, the portion of the tumour lateral to the tubular retractor may be difficult to visualise unless the retractor is positioned to orient laterally, again increasing the extent of manoeuvring and underlying muscle dissection required. A more tangential view to the long axis of the tumour, where a larger area of the tumour is visualised through the limited aperture of the tubular retractor may be helpful in this case. A significant foraminal portion may be a hindrance to this approach, but was not the case here as the foraminal portion was small.
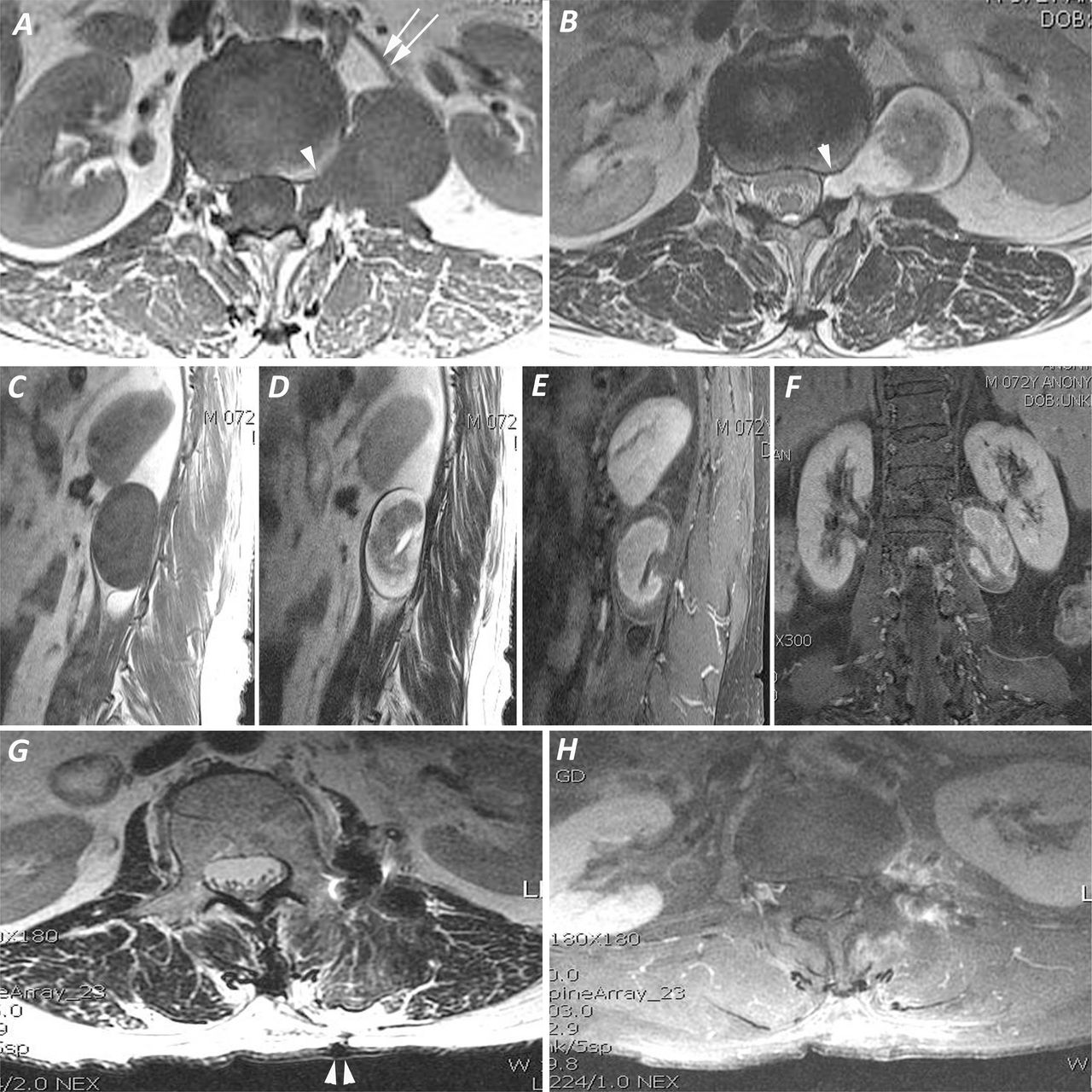
T1W (A) and T2W (B) axial sections showing a large paraspinal tumour with a small extension into the left L1-2 foramina (single arrowheads) without any foraminal widening. The close relation to renal artery (double arrows) can be noted. Saggital T1W (C), T2W (D), contrast enhanced saggital (E) and coronal (F) images showing tumour extension across two segmental levels in the paraspinal area medial to the left kidney. Post-operative T2W (G) and contrast enhanced (H) axial sections showing gross total tumour resection. The paramedian entry point on the skin can be noted (G, double arrowheads) with grade 1 signal changes in the underlying paraspinal muscles (22).
Under epidural analgesia, a 2.5 cm vertical incision was made 2cms to the left of midline over upper part of L1 body and a 22 mm tubular retractor was docked on the lateral edge of the facet joint complex. Lateral 1/3rd of the facet joint was drilled using a high speed burr. The intertransverse muscle and ligament were removed and the lesion was visualised. The ipsilateral root was probably displaced anteriorly and was not visualised on the posterior surface of the tumour. Internal decompression, pericapsular dissection and total capsular excision was progressively carried out, after which the root was visualised. Once the root was seen, it was traced medially and intraforaminal portion (free from the nerve and rest of the tumour) was removed using a right angled probe. Care was taken to remove the most anterior part of the lesion which was in close proximity to the renal artery. Post-operatively she complained of tingling sensations in the left upper thigh which improved at follow-up. There were no fresh deficits. Post-op MRI showed gross total tumour excision (Figure 2G,H). Histopathology report was cellular schwannoma.
Case 3
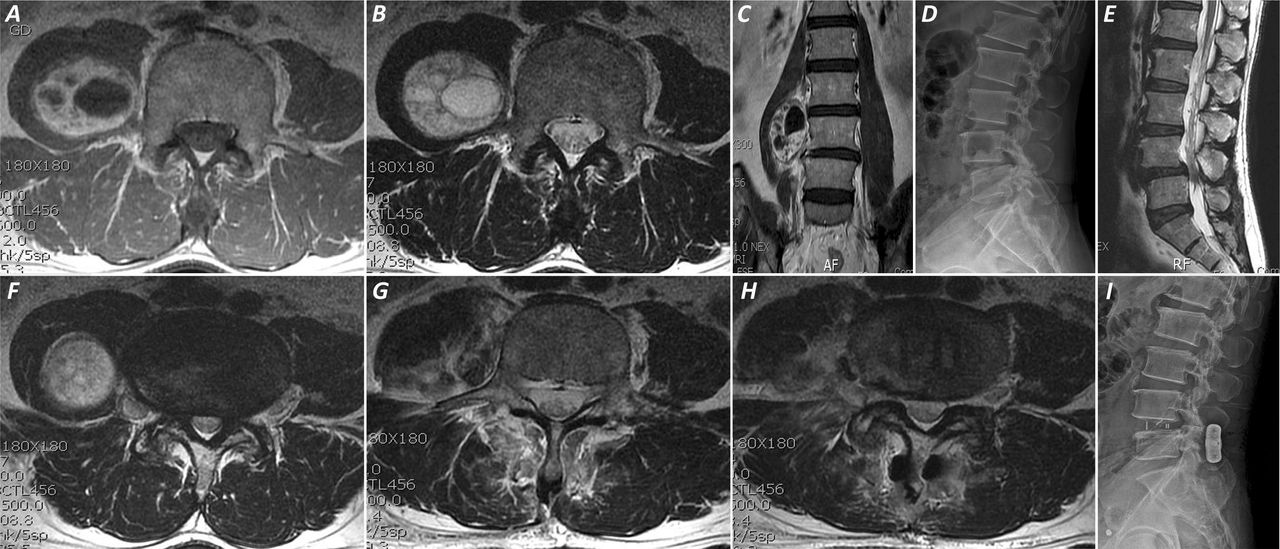
This 57 yr old male presented with history of chronic low back pain and recent onset right leg radicular pain. He did not have any focal deficits. MRI showed a large (5.2x3.7x4.1cm) enhancing right paraspinal mass at the level of L4 vertebral body (Figure 3A-C). The lesion was partially embedded within the psoas muscle. He also had Grade 1 stable L4-5 spondylolisthesis causing lateral recess stenosis (Figure 3D-F).

Axial T1W (A), T2W (B) and contrast enhanced coronal (C) images showing tumour extension in case 3. The tumour imbedding in the psoas muscle and its relative anterior location as compared to the tumour in case 2 can be noted. Lateral neutral radiograph (D) and T2W saggital MRI showing grade 1 spondylolisthesis at L4-5. T2W axial MRI section (F) at the level of L4-5 disc showing lateral recess stenosis and the lateral location of the tumour. Post-operative MRI (G,H) showing gross total tumour resection with a faint outline of interbody cage. Post-operative lateral radiograph (I) showing the interbody cage and interspinous SPIRE in situ. The relative increase in posterior disc height and foraminal height (indirect decompression) in comparison to pre-op radiograph can be noted.
This patient underwent a direct lateral mini-open retroperitoneal, trans-psoas approach and complete excision of the lesion. The anterior part of psoas muscle was targeted to reach the lesion thus preventing injury to the lumbar plexus which is situated in the middle and posterior part of the psoas muscle at this level. After tumour resection was completed, L4-5 discectomy was done and an interbody cage was inserted. This was followed by insertion of a posterior interspinous stabilisation device (SPIRE). Post-operatively, he developed right hip flexion weakness of grade 4/5 and painful hip movements. His knee extension was normal. With an intensive physiotherapy regime, he made gradual recovery and regained normal hip flexion in 3 months duration. Post-op imaging showed complete tumour removal, increased posterior disc and foraminal height (Figure 3G,H,I), and flexion-extension radiographs at 1 yr showed no movement at the level of listhesis.
Discussion
Extradural schwannomas with an extraspinal component larger than 2.5 cm in maximum diameter are considered to be ‘giant’.9, 16, 17 There have been numerous articles on the appropriate approach to the surgical management of these complex lesions.3, 9, 10, 17, 18 Giant dumb-bell tumours are effectively managed by a combined posterior and anterolateral approach or a single stage lateral extracavitary approach. Tumours with a large foraminal and paraspinal component limited to one segmental level can be managed either by 1) Hemi-laminectomy, unilateral facetectomy and intertransverse approach (inside-out approach) or 2) Wiltse's muscle splitting approach with unilateral facetectomy (outside-in technique). Purely paraspinal nerve sheath tumours have been traditionally approached through 1) posterior midline incision with muscle dissection lateral to the facet and tip of transverse process 2) Wiltse's muscle splitting intertransverse approach or 3) lateral retroperitoneal approach. Each of these approaches have their own merits and demerits, the discussion of which are beyond the scope of this article.
With the advent of minimal access spinal techniques, there has been increasing trend towards minimizing muscle injury that was inevitable with extensive exposures in conventional techniques.4 In Mannion et al's series of 11 patients of intradural, extramedullary spinal tumours treated by a minimally invasive approach, only one patient had a schwannoma with extradural component.12 This patient required a total facetectomy and pedicle screw fixation to maintain a stable spine. Haji et al reported on 20 cases managed by minimal access technique, six of which were extradural dumbbell schwannomas and two had paraspinal extension.1 Weil et al reported removal of a giant extradural schwannoma extending across 1 segmental level through a 18mm tubular retractor, identical to case 1 in this series.4 However, case 1 in the present report also underwent decompression for symptomatic spinal stenosis at the same level, which by a conventional approach thus preserving the integrity of bilateral facet joints. A conventional approach to this case would have necessitated a laminectomy, medial facetectomy on the side contralateral to the tumour and total unilateral facetectomy on the side of the tumour, thus requiring a fusion procedure to maintain spinal stability which was avoided with a minimal access route.
To the best of our knowledge, case 2 in this series is the first paraspinal tumour extending to more than 2 segmental levels being treated with a 22mm fixed tubular retractor. We think this was possible due to a modified paramedian approach used in this case to obtain a tangential view to the tumour rather than the classical far lateral approach. The validity and reproducibility of this concept, however, needs to be tested in subsequent cases. Also, we would like to stress the fact that a paramedian approach could be successfully used only when the foraminal component is small. A similar approach in the case of a larger foraminal component (for example in case 1) would necessitate almost total facetectomy to visualise the complete tumour, thus affecting spinal stability and necessitating a fusion procedure (Figure 4).

Diagrammatic illustration of the size of foraminal component influencing choice of approach and field of vision through a tubular retractor in case 1 (A & B) and case 2 (C & D). The white arrows indicate the line of sight. The large foraminal portion of case 1 could be easily visualised with minimal lateral facet resection from a far lateral angle (A), while a paramedian approach in this case would have led to complete facetectomy to visualise the foraminal component (B; Solid arrow indicates line of sight with safe facet resection. Dotted arrow shows degree of facet resection to visualise the medial portion of the tumour). In case 2 (C & D), foraminal portion could be adequately visualised with paramedian approach which also helped in visualising inferolateral portion of the tumour from a superomedial angle.
Case 3 presented unique challenges. It was situated more anteriorly (deeper from a posterior approach) and was partially embedded within the psoas muscle. Both these points were presumed to complicate a minimal access procedure from a posterior route.10
We do not think that size of the tumour was a factor in choosing the approach as the tumour in case 2 was of similar size. Intra-operative neuro-monitoring is a useful adjunct in such cases, which can identify the proximity of lumbar plexus to the surgical tract and make the procedure safer19. Also, the listhesis was managed using the same lateral approach to insert an interbody cage and a limited posterior dissection to place an interspinous stabilisation device (SPIRE). The interspinous device has been shown in biomechanical studies to be comparable to bilateral pedicle screws in limiting segmental mobility.20 As earlier pointed out, newer concepts in minimally invasive spinal surgery are open to question and further modifications. It would, as such be tempting to attempt minimal access removal of the tumour in case 3 and combine it with a mini-TLIF procedure for the listhesis at the same sitting.
Conclusion
Extradural paraspinal schwannomas can be effectively managed by minimal access techniques with proper pre-operative planning. Minimal access techniques fasten recovery time, decrease tissue damage and obviate the need for a concomitant fusion in several situations. However, until sufficient experience is gained in these techniques, it is important to understand the present day limitations of tumour resection surgery through a tubular retractor and a conventional approach may still be a proper choice in select complex cases.
Disclosures
The authors declare no relevant disclosures.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.