


Abstract
Purpose A retrospective study to compare the radiologic and clinical outcomes of 2 different anterior approaches, multilevel anterior cervical discectomy with fusion (ACDF) using autologus ticortical bone graft versus anterior cervical corpectomy with fusion (ACCF) using free vascularized fibular graft (FVFG) for the management of cervical spondylotic myelopathy(CSM).
Methods A total of 15 patients who underwent ACDF or ACCF using FVFG for multilevel CSM were divided into two groups. Group A (n = 7) underwent ACDF and group B (n = 8) ACCF. Clinical outcomes using Japanese Orthopaedic Association (JOA) score, perioperative parameters including operation time and hospital stay, radiological parameters including fusion rate and cervical lordosis, and complications were compared.
Results Both group A and group B demonstrated significant increases in JOA scores. Patients who underwent ACDF experienced significantly shorter operation times and hospital stay. Both groups showed significant increases in postoperative cervical lordosis and achieved the same fusion rate (100 %). No major complications were encountered in both groups.
Conclusion Both ACDF and ACCF using FVFG provide satisfactory clinical outcomes and fusion rates for multilevel CSM. However, multilevel ACDF is associated with better radiologic parameters, shorter hospital stay and shorter operative times.
Introduction
Cervical spondylotic myelopathy (CSM) is considered the most common cause of spinal cord dysfunction in older persons.1 Although it is generally agreed that surgical intervention positively impacts the prognosis of CSM, the decision algorithm for the selection of the most appropriate surgical technique is complex.
Anterior cervical decompression and fusion was first reported by Smith and Robinson2 and popularized by Cloward3 in the 1950s. The advantages of anterior decompression include the ability to directly decompress offending structures and restore cervical lordosis. Anterior cervical discectomy with fusion (ACDF) can decompress the anterior spinal cord, preserve the stability of the spinal column and is associated with a low prevalence of graft extrusion or migration. However, some authors argue that ACDF may not be the optimal surgical approach for CSM due to the risk of incomplete decompression, limited visual exposure, and a high rate of of pseudoarthrosis secondary to an increase in the number of fusion surfaces.4–6 An alternate means of improving the fusion rate after multilevel decompression is the use of anterior cervical corpectomy with fusion (ACCF).7
Autologous iliac or fibular grafts or fibular allografts are routinely used to bridge the corpectomy defect. Corpectomy and fibular strut grafting has a reported nonunion rate of 27% for autograft and 41% for allograft.8 The nonvascularized grafts need to be replaced by creeping substitution, a process that requires months to years to complete. The free vascularized fibular graft (FVFG) transfer was first reported in 1975 by Taylor et al.9 Vascularized autografts retain their biologic and mechanical properties, heal by primary union with ingrowth to the adjoining bone, hypertrophy in response to load10 and tend to resist higher biomechanical loads than conventional grafts.11, 12
In this study we evaluated the clinical and radiological outcomes to compare the efficacy of ACDF using autologus tricortical iliac bone graft and ACCF using autologus FVFG for multilevel CSM.
Patients
After obtaining the Institutional Review Board approval we conducted this retrospective study to compare the results of (ACDF) using autologus ticortical bone graft versus (ACCF) using (FVFG) for multi-level CSM.
The inclusion criteria were patients who presented primarily with signs and symptoms of CSM due to multilevel cervical affection.
Exclusion criteria were (i) Patients with cervical myelopathy due to other causes as ossification of the posterior longitudinal ligament (OPLL), rheumatoid arthritis, cerebral palsy or tumors; (ii) Previous cervical surgery; (iii) Patients with acute neurologic deterioration following trauma over a spondylotic canal; (iv) Patients with incomplete data.
Ultimately 15 patients (11 men and 4 women) were eligible for this study who were operated between 2005 and 2011in the same hospital by the authors. Patients were divided into two groups based on surgical methods. Group A (n = 7) included patients who underwent multilevel ACDF (Figure 1), Group B (n = 8) included patients who underwent multilevel ACCF (Figure 2).
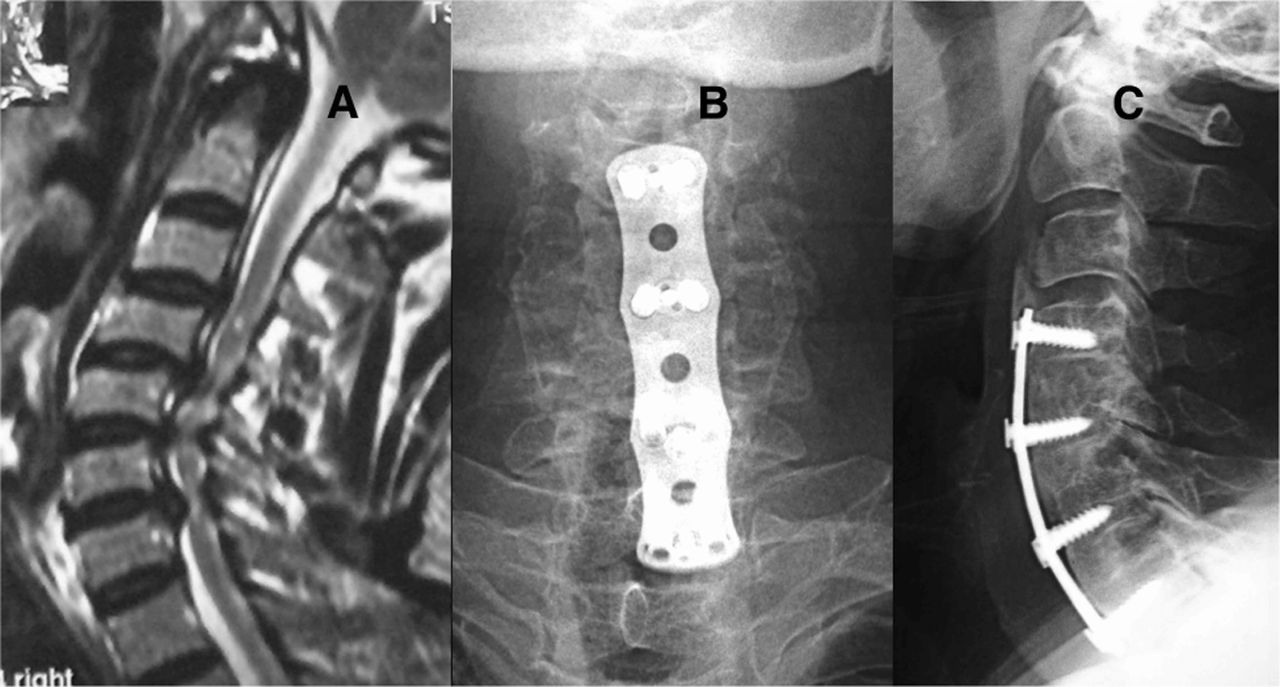
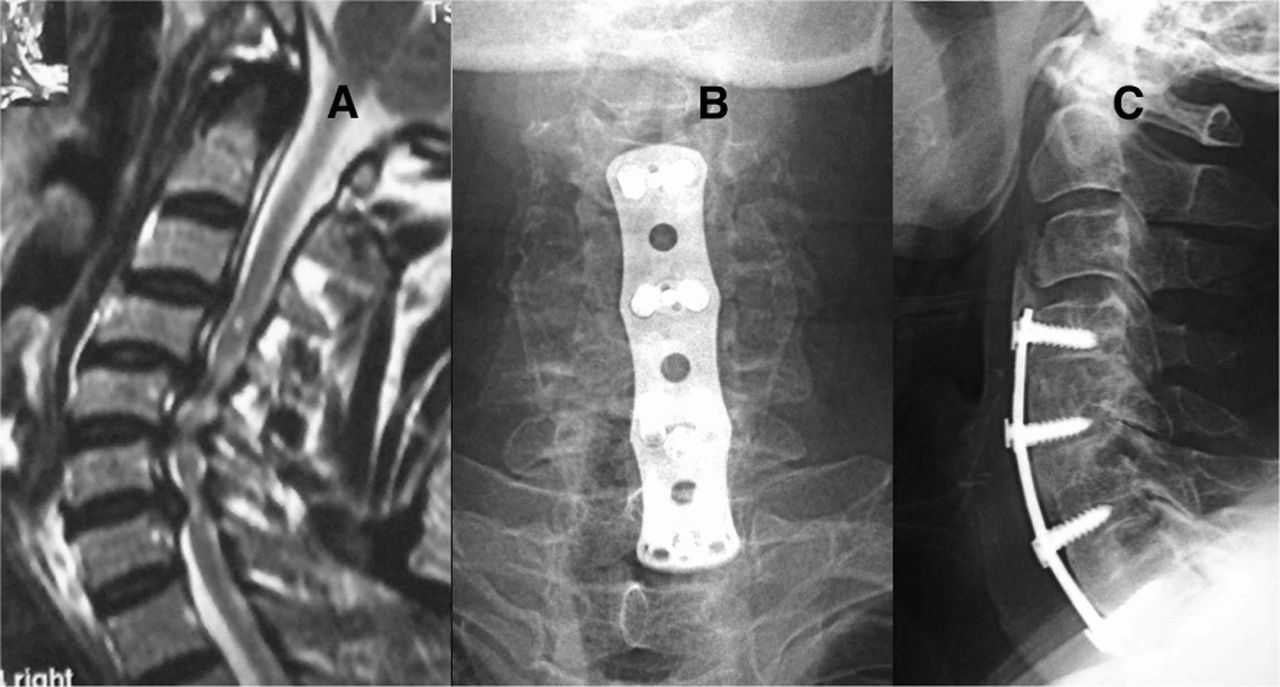
64 year old male with CSM. (A) T2 sagittal MRI showing cord compression and signal changes due to multiple disc herniations between C4-7. (B) and (C) 33 month postoperative antero-posterior and lateral X-ray showing C4-5, C5-6 and C6-7 discectomy and fusion with autologus tricortical iliac bone grafts fixed by anterior locked plate with complete bony fusion and maintenance of cervical lordosis.
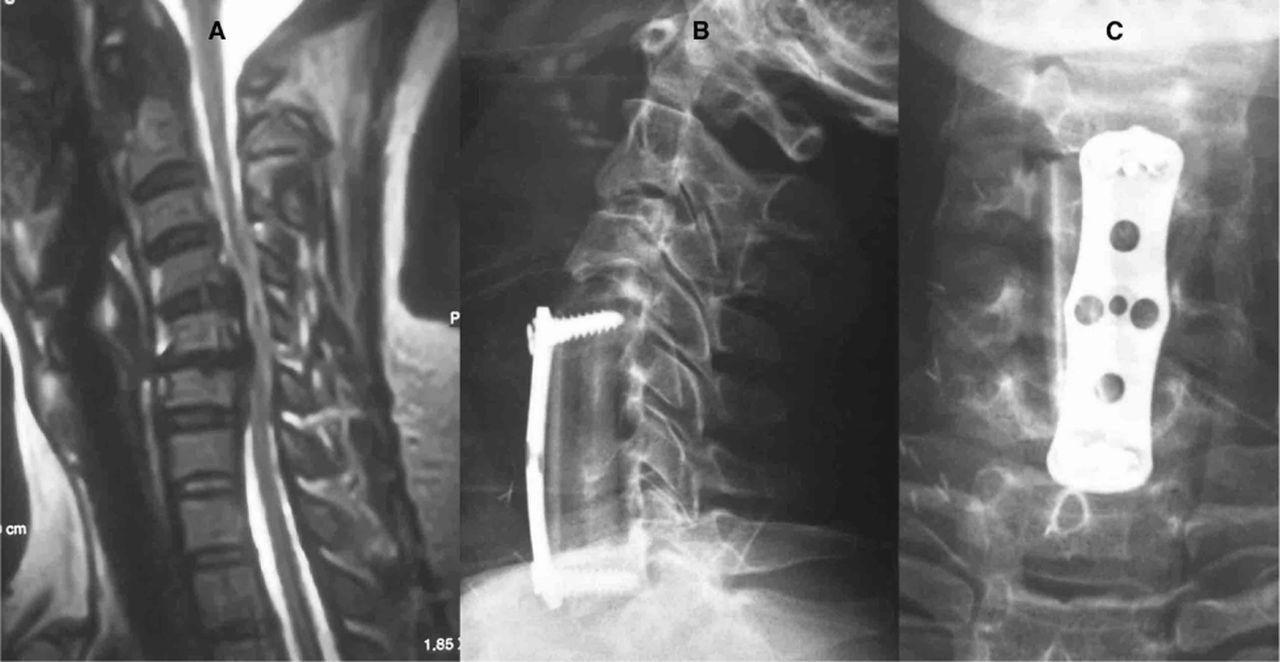
58 year old male. (A) T2 sagittal MRI showing cord compression and signal changes between C4-7, (B) and (C) 31 month postoperative antero-posterior and lateral X-ray showing C5 and C6 corpectomy and FVFG reconstruction fixed by anterior locked plate with solid fusion.
Methods
Patient demographics, duration of symptoms, operative segments, operation time, hospital stay, and complications were recorded. Japanese Orthopaedic Association (JOA) score13 was used to assess the clinical status.The radiological parameters (fusion rate, and cervical lordosis) were examined using anteroposterior (AP), lateral, and flexion/extension plain radiographs.
Radiographic fusion was considered present if the following features were observed: (i) no motion across the fusion site on flexion–extension X-rays, (ii) trabeculae across the fusion site, (iii) no lucency across the fusion site or around any of the screw sites. If the fusion was questionable, CT scans were performed.
Cervical lordosis was defined as the angle formed between the lower endplate of C2 and the upper endplate of C7 by Cobb method on plain lateral radiographs with the patient in a neutral position.
Preoperative MRI was also routinely performed to evaluate spinal cord compression.
Surgical technique
Anterior cervical discectomy and corpectomy were performed as described previously.3, 14
Of the ACDF procedures, the posterior longitudinal ligament was removed in all cases at the discectomy sites. Autologous tricortical bone graft was harvested from anterior iliac crest and cut to the appropriate size to fit the discectomy sites. The grafts were inserted between the vertebral bodies to restore the intervertebral disc space and cervical lordosis. Anterior cervical plating was done.
Of the ACCF procedures, the posterior wall of the vertebral body and posterior longitudinal ligament were removed. FVFG was used to bridge the spinal defect. Two surgical teams work simultaneously. After harvesting the fibular graft through a standard technique.15, 16 The graft is left attached to its vascular pedicle until the moment of actual transfer. The periosteum is removed from the fibular ends and the graft was impacted in the trough created after corpectomy. Arterial anastomosis was generally end-to-end using an operation microscope. We used the superior thyroid artery in all cases. The recipient vein was either the venae comitantes or a branch of the external jugular veins. Depending on the selected recipient vessels, the fibular graft was positioned with the vascular pedicle ending in the direction of the recipient vessels.
Anterior cervical locked plate is applied prior to performing the vascular anastomoses in a fashion to protect the vascular pedicle. A rigid cervical collar for 6 weeks was given to the patients in both groups.
Clinical and radiologic outcomes were collected at admission, immediately after operation, and at outpatient clinic at 3 and 6 months after surgery. Subsequent follow-up examinations were performed at 6-month intervals.
Statistics
SPSS (Version 20) was used for the analysis. Intergroup comparisons were made using the Mann–Whitney U test. Wilcoxon's signed-rank test was used to Compare the results pre- and postoperatively in the same group. P value <0.05 was considered statistically significant.
Results
Of the 15 patients (11 men and 4 women), 7 patients underwent ACDF (group A) and 8 patients ACCF with FVFG (group B) for the management of multi-level cervical spondylotic myelopathy.
The mean age in group A was 58.7±6.87 years and 55.87±6.8 years in group B (p=0.4).
The number of fused levels in group A was 3 in all the cases while in group B, 2 levels fusion was performed in 3 cases, 3 levels in 2 cases, and 4 levels in 3 cases (p=0.7).
The overall follow-up period of group A was 32.71±9.9 months and 35.25±6.3 months in group B (p=1).
The mean operative time was 207.86±13.18 min in group A and 371.25±64.017 in group B (p <0.001).
The mean hospital stay was 3.86±0.89 days in group A and 8.5±1.9 days in group B (p <0.001). No patient received blood transfusion in either group.
A summary of the perioperative parameters is presented in Table 1.
Perioperative parameters.
The JOA score for both groups was improved at the final follow up with no difference between both groups (p=0.61). Table 2 shows the detailed JOA score for all patients both preoperative and at the final follow up.
JOA score.
The average angle of cervical lordosis improved from 8.8±1.5 preoperatively to 15.9±1.6 direct postoperative in group A and from 7.5±2.4 preoperatively to 14.4±0.7 direct postoperative in group B (p=0.04). At final follow-up, the mean angle of cervical lordosiswas maintained at 14.7±1.8 in group A and at 13.2±0.7 in group B, (p=0.02), Table 3.
Radiologic outcome.
Solid fusion was confirmed in all patients at the final follow up, with no graft dislodgment in either group. Hardware-related complications occurred in one case in each group, in group A in the form of partial loosening of screws manifested as radiolucent halo around screw threads and in group B in the form of pullout of the lower screws. However, both patients had no clinical symptoms to require specific management because there was no retropulsion of the plate or bone graft and both patients progressed to solid bony union at final follow-up.
Two patients in group A and three patients in group B developed postoperative dysphagia that improved gradually and spontaneously in all cases.
Three patients complained of donor site pain in group A and one patient in group B. The problem was more marked and persisted longer in group A but no case persisted after the third month postoperative.
Wound infection occurred in one patient in group B in the form of serous discharge from the cervical wound which responded after 2 weeks with antibiotic administration.
No patient with graft harvest site infection in either group.
There were no patients with iatrogenic neurological deterioration, nor were there dural, tracheal, vascular, or esophageal injuries related to operation.
A summary of complications is provided in Table 4.
Summary of complications.
Discussion
Compression of the spinal cord due to a degenerating cervical spine tends to cause progressive clinical symptoms, and surgical decompression can stop this process and lead to functional recovery. As Fessler et al reported, 92% of patients experience symptom improvement after anterior decompression and fusion for CSM, and thus surgery is commonly advocated for its management.17
Although the surgical approach to CSM treatment has proven to be controversial, anterior decompression and fusion can remove the compressive pathology and reconstruct the alignment of the cervical spine, yielding good clinical results. However, the ideal anterior decompression method is also controversial. It was found that fusion after multisegmental anterior decompression is a challenging process as the union rate is inversely proportional to the number of segments fused, with more than 50% nonunion in multisegment fusions.18, 19 The lower fusion rates previously reported for ACDF have been attributed to an increased number of grafts and interfaces that must consolidate with multilevel constructs and to increased stresses and resultant motion at the graft sites.20 However ACCF utilizes only two graft-host interfaces (one single strut graft). Earlier studies have demonstrated that vascularized bone grafts offer superior biologic and mechanical properties when compared with nonvascular grafts.11, 12 We used FVFG to reconstruct the corpectomy site assuming to achieve the best mechanical and biological environment suitable for successful fusion.
Although some relevant studies comparing the ACDF and ACCF have been reported, the evidence regarding whether ACDF is superior to ACCF remains insufficient, owing to ambiguous results.4, 7, 21, 22
We conducted this retrospective study to clarify this point and discuss the pros and cons of each method.
There was no statistically significant difference in the age distribution, number of fused levels and follow up period between both groups.
Both groups demonstrated a significant post-operative increase in JOA scores, an increase that was maintained at the final follow-up. These findings indicate that both groups achieved adequate decompression of the spinal cord and nerve roots, and that these patients benefited from reconstruction of the spinal column.
Both the ACDF and ACCF groups had significantly increased cervical lordosis, but the increase was greater in the ACDF group than in those with ACCF. ACDF can provide multiple points of distraction and fixation in addition to the graft and interbody space shaping. However, ACCF grafts may straighten the cervical spinal column between the remaining vertebral bodies.23
A concern with multilevel anterior corpectomies is graft dislodgement, which has been reported in many articles.7, 23, 24 We noted no case with graft dislodgement due to the rigid fixation with locked anterior plate. The union rate was 100% in both groups.
We found no difference between both groups in the incidence of Hardware-related complications, but the incidence of wound infection and dysphagia was higher in ACCF group which can be explained by the prolonged operative time and the need for more dissection in this group.
The etiology of dysphagia may be multifactorial, including hematoma formation and prolonged retraction and denervation of the upper esophagus by injury to the pharyngeal plexus.25
Although 2 surgical teams were operating simultaneously, one team for cervical corpectomy and the other for FVFG harvesting but the ACCF group showed significantly higher operative time which was spent in the more cumbersome corpectomy and vascular anastomosis.
Longer hospital stay was also needed in this group to detect any anticipated complications related to the more extensive dissection in the donor and recipient sites and the vascular anastomosis.
Conclusions
ACCF using FVFG can be done safely to manage multilevel CSM, however this technique did not yield superior results than ACDF, but on the contrary ACDF was associated with significantly shorter operative time and hospital stay. On the light of these results we can say that ACDF using autologus tricortical bone grafts may therefore be a better alternative for the surgical management of multilevel CSM.
Our study is limited by being retrospective and small sample size.
Disclosures
The authors declare no relevant disclosures.
- Copyright © 2015 ISASS - This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.