


ABSTRACT
Background: Exposure of the anterior cervical spine requires dissection in proximity to critical neurovascular structures. Monopolar electrosurgical (ES) devices generate heat in contacted tissues, resulting in thermal damage and temperature change. This study examined depth of thermal injury and temperature change associated with use of a low-temperature electrosurgical device (LTD) compared to traditional electrosurgery during a cadaveric anterior cervical discectomy and fusion (ACDF) dissection.
Methods: ACDF was performed, using ES or LTD, on cervical spines (C3-4 and C4-5) from 2 fresh human cadavers with intact neck soft tissues and no history of surgery. Cadavers were maintained at 22–23°C, and fiber-optic temperature sensors (Neoptix, Québec City, Québec, Canada) were placed near relevant structures to measure changes during dissection. Depth of thermal injury was assessed by hematoxylin and eosin and Masson's trichrome histology of fixed tissue specimens.
Results: Use of the LTD resulted in a statistically significant reduction in temperature change at platysma (3.0 ± 1.04 vs. 11.41 ± 3.10°C, P = .003), carotid sheath (7.32 ± 1.13 vs. 15.57 ± 2.56°C, P = .007), and longus colli (6.11 ± 1.32 vs. 12.9 ± 3.62°C, P = .016) compared to ES. Temperature change at the trachea was similar between groups (6.06 ± 1.99 vs. 4.96 ± 1.89°C, P = .528). Histology showed that LTD produced less mean and maximal depth of thermal injury compared to ES (mean: 0.5 vs. 1.2 mm; max: 0.9 vs. 1.8 mm; P < .05).
Conclusions: The results of this pilot study demonstrate that anterior cervical spine exposure using an LTD reduces tissue temperature change and depth of thermal injury compared to ES.
Clinical Relevance: Although exploratory, these results suggest that use of an LTD during ACDF may reduce the extent of thermal tissue injury during dissection. Future studies in live animal models are warranted to determine if thermal injury is a potential cause of common exposure-related complications, such as dysphagia and dysphonia.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) is an effective and well-established surgical procedure for the management of symptomatic degenerative cervical disk disease. Although ACDF generally leads to good clinical outcomes and an arthrodesis rate of 95% at 2 years,1 the rare complications associated with ACDF can be debilitating or life threatening. These complications can include laceration of the airway, nerves, vasculature, and other structures; cerebrospinal fluid leakage; laryngeal nerve palsy; persistent swallowing or speech disturbances; bladder and bowel problems; and paralysis.2–5 Such complications may be transient or permanent, depending on the severity of the injury.
Traditional electrosurgical (ES) devices are the mainstay of dissection and bleeding control during surgery, including ACDF. Despite their utility, the heat generated by these devices can cause unintended thermal injury to nearby critical structures and has been shown to impair wound healing, increase inflammation, depolarize nerves, injure vasculature, and lead to other adverse sequelae.4,6–8 Accordingly, novel ES devices have been developed that operate at lower temperatures—between 40°C and 100°C—compared to as high as 300°C for traditional ES devices. These lower temperatures can help to minimize thermal injury to critical structures during dissection and bleeding control with the ultimate goal of limiting the morbidity associated with electrosurgery.
To our knowledge, the evaluation of low-temperature ES devices (LTDs) for ACDF has not been reported in the literature. Thus, the purpose of the present study was to determine whether a representative LTD could reduce heat transfer and depth of thermal injury in adjacent tissues during the ACDF procedure when compared to a traditional ES device. To this end, we used a cadaveric model to measure in situ temperature changes near critical anatomical structures that may be at risk during routine ACDF dissection. The depth of thermal injury was assessed quantitatively by histological analysis of harvested tissues.
MATERIALS AND METHODS
ES Devices
The LTD used for this study was the PEAK Surgery System (Medtronic Advanced Energy, Portsmouth, NH), which consists of the microcontroller-based, isolated output, PULSAR Generator and single-use PEAK PlasmaBlade tissue dissection devices. The representative ES device used in this study was the Valleylab ES pencil, button switch, and disposable (uncoated) metal blade electrode (Model E2450H) powered by the Valleylab Force FX generator (Medtronic Inc., Minneapolis, MN).
Human Cadaver Spines
Two human cadaveric cervical spines (C1–T3) with intact adjacent soft tissues of the neck were obtained from approved vendors (Anatomy Bequest Program, University of Minnesota, Minneapolis, MN). Both cadaveric spines had no history of muscular disease or prior surgery and were less than 120 hours postmortem. On the day of surgery, the cadaveric spines were acclimated to and maintained at room temperature (22–23°C) and prepped in the usual fashion.
Temperature Sensor Placement
The standard for making accurate temperature measurements in an electrically noisy environment (as occurs with ES devices) is a fiber-optic temperature sensor. These devices exploit the property of crystalline materials, which have an optical reflectance that changes with temperature. An excited pulse of light of specific intensity is sent down the fiber-optic cable, and the intensity of the reflected signal is measured by the device so that the temperature can be determined. These sensors can provide real-time, continuous temperature measurements with no radio frequency interference and are therefore considered the standard for temperature measurement of energy-based systems. Fiber-optic sensors of various sizes (as small as <0.5 mm in diameter) are available and have been used in medical research studying ablation and surgical procedures.9,10 The Neoptix Reflex system (Neoptix, Québec City, Québec, Canada; Figure 1) was selected for use in the present study for its ability to provide real-time, reproducible measurements and for the availability of small probe sizes.

Fiber-optic system. The system consists of the measuring unit (left panel) and the fiber-optic temperature sensor (right panel). The bare fiber-optic temperature sensor is 300 microns in diameter (right panel).
Prior to each ACDF dissection procedure, the calibrated fiber-optic sensors were placed and secured at or close to critical structures (as close as 8–10 mm) during the ACDF dissection procedure. Placement was verified by fluoroscopy before continuing the ACDF dissection. Temperature at the sensors was measured continuously in real time as the procedure was performed.
ACDF Procedure
The ACDF procedures were performed on the cadaveric cervical spines (C3-4 and C4-5) under non–good laboratory practices conditions at Physiological Research Laboratories (Minneapolis, MN). Each cadaveric spine was dissected with both the LTD (set at Cut 6 mode, 20 W) and the ES (set on Cut mode, 25 W); the two devices were used on different sides of the spine, chosen at random.
The procedure was carried out as previously described.11 Briefly, a skin incision was performed transversely to the level of platysma. The plane between the carotid sheath (laterally) and the esophagus and trachea (medially) was dissected and the omohyoid divided as necessary. The prevertebral tissues and any visible longus colli muscles overlying the anterior longitudinal ligaments and vertebral bodies were dissected, and an incision of the anterior annulus was performed. A vertical traction was placed on the vertebral bodies, and the cut annulus was removed, along with the anterior two-thirds of the disc. The osseous lips present on the superior and inferior vertebral bodies were drilled, and the disc was removed. The procedure was repeated on the contralateral side with the comparative ES device.
Histopathologic Determination of Thermal Injury in Excised Tissues
Sections of platysma, carotid sheath, and longus colli were excised with scalpel after completion of the ACDF and temperature measurement phase, fixed in 10% normal saline-buffered formalin, and stained with hematoxylin and eosin (H&E) and Masson's trichrome. H&E stain was used for assessing basic tissue structure and inflammation: muscle and other tissues damaged by thermal application appear as bright pink with a hyalinized appearance compared to normal tissues that appear as lighter or darker pink. Masson's trichrome stain was used for identifying collagen, both new and old, along with muscle damage. Damaged muscle appears purple compared to normal muscle, which stains red. Tissue blocks (2 cm long by 4 mm thick) were trimmed, and the depth of thermal injury, defined as the width of the collagen and muscle damage perpendicular from the cut surface and into the tissue, was measured. Measurements were taken at 3 representative locations at each critical anatomical location for the 2 spines and recorded as the maximum depth of injury, the minimum depth of injury, and a middle depth of injury in millimeters. The mean depth of thermal injury was the average of the 3 measurements.
STATISTICAL METHODS
Sample Size
This was a pilot study comparing the temperature changes and thermal injury caused by LTD and ES during ACDF; therefore, no formal sample size calculation was performed. Two cadaver spines were dissected, both with LTD and ES (1 side each), yielding an N of 2 for each device.
Temperature Change Measurements and Analysis
Temperature change (mean ± SD) was calculated from 3–4 peak temperatures recorded from each device in each location in both spines while the devices were in use. P values comparing LTD and ES were calculated using an F test, then by a 2-sided t test for equal or unequal variance with a 2-tailed distribution. Confidence intervals at 95% were plotted as error bars for all data. P values <.05 were considered statistically significant.
Thermal Damage
Maximum, minimum, and middle depth of thermal damage measurements (in mm) were taken at three representative locations of each anatomical location in both spines. The mean was the average of the 3 measurements. P values were calculated using an unpaired Student t test with a prespecified alpha of <0.05.
RESULTS
Cadaveric Spines and Probe Placement
The 2 cadaveric spines used in this study were 78 and 108 hours postmortem. Attempts to place calibrated fiber-optic temperature sensors were successful in all but 4 critical structures (the left and right transverse foramen close to the spinal cord, the vertebral artery, the superior laryngeal nerve, and the recurrent laryngeal nerve). The placement of sensors is provided in Table 1.
Placement of temperature sensors in critical structures.
Temperature Changes in Dissected Tissues
The LTD generated a statistically significant reduction in temperature elevation at the platysma (3.0 ± 1.04 vs. 11.41 ± 3.10°C, P = .003), carotid sheath (7.32 ± 1.13 vs. 15.57 ± 2.56°C, P = .007), and longus colli (6.11 ± 1.32 vs. 12.9 ± 3.62°C, P = .016) compared to ES. Temperature in the trachea, however, was not different in the two groups (6.06 ± 1.99 vs. 4.96 ± 1.89°C, P = .528; Table 2). No change in temperature was observed in the spinal canal. Data for the esophagus were insufficient for analysis.
Temperature changes in critical structures.
Histologic Assessment of Thermal Injury
Histological assessment by H&E and Masson's trichrome staining for depth of thermal injury showed that the LTD produced statistically significantly lower mean and maximum depth of injury in all tissues excised (mean: 0.5 ± 0.2 vs. 1.2 ± 0.4 mm; max: 0.9 vs. 1.8, P < .05) compared to ES. A reduction in maximum depth of thermal tissue injury was also observed in the platysma with the LTD compared to the ES (Table 3), but no statistical analysis could be conducted because only 1 ES tissue section was examined. Representative histopathologic sections of the different tissues are presented in Figures 2 and 3.
Depth of thermal injury.

H&E staining showing depth of thermal injury in the carotid artery and longus colli. Mature adipose, connective, and collagen tissues are stained dark pink, indicating thermal injury to the tissue, while lighter pink indicates no evidence of thermal injury. Upper panel: carotid artery. Lower panel: longus colli. Magnified 20×.
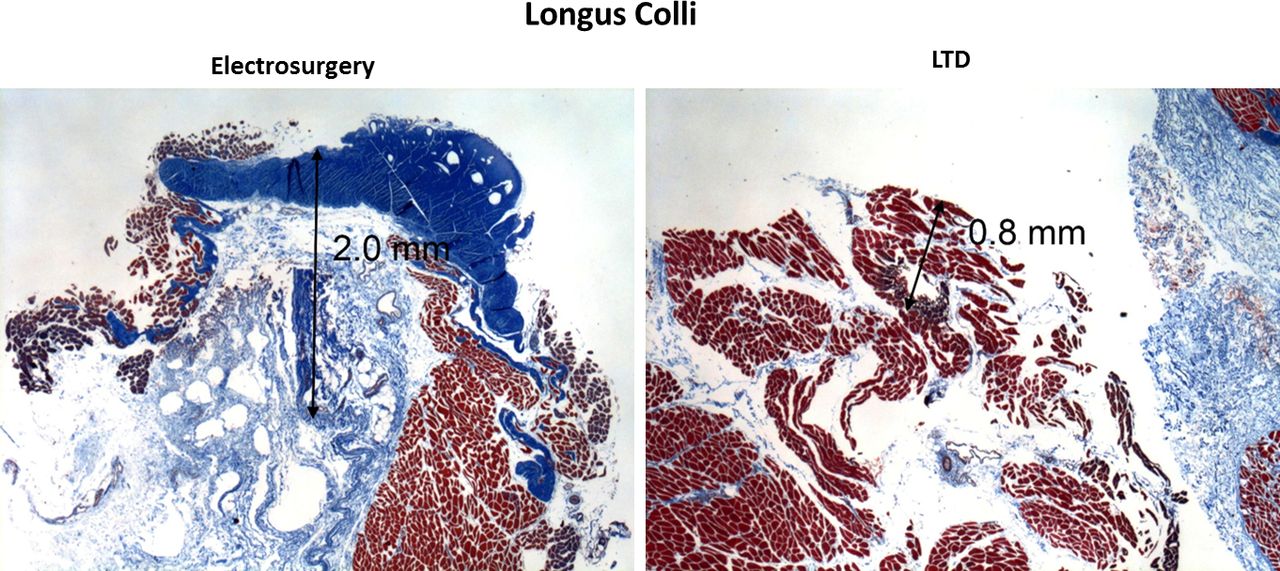
Masson's trichrome staining showing depth of thermal injury in the carotid artery and longus colli. Adipose and connective tissue is stained darker blue, indicating thermal injury, while the adjacent lighter blue indicates no evidence of thermal injury. The damaged collagen is the darkest blue collagen at the top of the image. Upper panel: carotid artery. Lower panel: longus colli. Magnified 20×.
DISCUSSION
Damage to blood vessels and nerves from the use of ES devices has been identified as the cause for many serious complications. Depending on the proximity to the adjacent critical structures and severity of injury, damage to those structures can result in transient or permanent injury.12,13
Several devices have been designed to operate at lower temperature in order to minimize thermal injury to dissected tissues. The LTD used in this study has previously been shown to significantly decrease the depth of thermal injury during dissection of skin and fascia in clinical and preclinical studies, minimizing collateral tissue damage, and providing a healing profile equivalent to scalpel.14–19 This LTD has also been shown to reduce scarring and wound necrosis20 as well as to improve surgery time, hospital stay, and cost in select applications.21
This LTD has not yet been assessed in ACDF; thus, this pilot study was designed to evaluate and compare its properties with ES in a cadaveric model. First, we developed a method to measure changes in temperature within critical structures adjacent to the dissection using sensitive fiber-optic sensors. Using this method, we showed that the LTD resulted in at least 50% less temperature change in the platysma, carotid sheath, and longus colli, which are adjacent structures that could potentially be affected by dissection during an ACDF. Consistent with these measurements, histological assessment of these tissues showed a reduced depth of thermal injury with the use of the LTD. These results are in agreement with those obtained by Naruns et al16 and Ruidiaz et al18 in breast cancer surgery, in which the authors had shown reduced thermal injury to the margin of excised tumor tissue following lumpectomy.
The present study has a number of important limitations. The sample size was small, consisting of only 2 spines. Although the cadaveric spines were maintained at room temperature, results obtained in unperfused tissues may not be fully relevant to results obtained in a live individual; for example, hemostasis was unnecessary in these specimens. In live patients, when the superior thyroid artery at C3-4 or inferior thyroid artery at C6-7 must be sacrificed, the dissection requires ES hemostasis. While this function may cause thermal injury on its own, in our experimental design, its potential effects could not be assessed. However, using human cadavers is the only way to determine histological thermal damage in ACDF because in living patients, no tissue is excised during this procedure except for a small portion of the disc. This is in contrast to tumor resection or abdominoplasty, in which tissues are excised and are therefore readily available for histopathological analysis of thermal damage.
Another limitation of the study was our inability to place temperature sensors at or near 4 critical structures: the left and right transverse foramen close to the spinal cord, the vertebral artery, the superior laryngeal nerve, and the recurrent laryngeal nerve. In cadavers, certain structures, such as nerves, are difficult to locate and successfully place and fix the sensors. Thus, in order to validate and extend the present results in cadavers, temperature measurements in critical structures should be performed during ACDF surgery in live patients. However, to our knowledge, the use of temperature sensors to measure temperature changes has never been evaluated in patients undergoing ACDF. The only study reporting in situ measurements of temperature changes using temperature sensors in live human patients was performed in open hysterectomy.10
Histological analysis of the tissues was not performed in a blinded manner, which could have biased the measurements of the depth of thermal injury, and, finally, correlation of thermal injury to clinical complications was not possible in this study. However, it is possible that the differences in thermal injury in this study may correspond to clinically relevant nerve injury or dysphagia; these represent areas for further study.
In conclusion, the results of this small, comparative temperature and histological pilot assessment suggest a potential benefit for using LTDs during ACDF because they produce less change in temperature and minimize thermal injury in dissected tissues compared with traditional ES devices. Further studies comparing LTDs to ES in living animals and in human patients undergoing ACDF should be performed to confirm these findings. Since histopathological analysis of live tissue in the dissection plane is not possible, the end points measured in these studies should include (1) temperature changes in situ during surgery (using fiber-optic temperature sensors); (2) outcomes including time to healing, scarring, and tissue necrosis; and (3) incidence of postoperative complications, such as dysphagia or dysphonia.
Acknowledgments
The authors thank Kent Wika (Medtronic) for assistance with surgical procedures, Matthew Hoffman (Medtronic) for assistance with temperature measurements, and Jeanne McAdara, PhD, and Florence Paillard, PhD, for medical writing assistance. The authors wish to thank the individuals who donated their bodies for the advancement of education and research.
Footnotes
Disclosures and COI: K. Radcliff is a paid consultant of Medtronic but was not compensated for this study; P. Vijay, R. Sarris, M. Speltz, and J. Vose are employees of Medtronic.
- ©International Society for the Advancement of Spine Surgery
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.