


ABSTRACT
Study Design: A cross-sectional study.
Background: To document dimensions of the lumbar vertebrae and bony canal in an Indian population and to compare with other studies from the subcontinent as well as from other parts of world.
Methods: An observational study was conducted on the basis of a review of thin-cut (3 mm) computed tomographic images of lumbar vertebrae. A total of 302 patients were studied, and various dimensions were analyzed.
Results: In general, the vertebral and bony spinal canal dimensions were found to be greater in male patients. Comparison of populations revealed statistically significant differences in the spinal canal between an Indian population and others.
Overview of Literature: Lumbar canal stenosis is a condition in which the anteroposterior and lateral dimensions of the bony spinal canal are less than normal for corresponding age and sex. Numerous studies have been conducted to determine morphometry of the lumbar vertebrae and spinal canal, mostly in western populations, using fresh cadaver or osteologic specimens. These studies did not mention the difference between the vertebral parameters in men and women. Moreover, many of these studies have limitations such as a small sample size and lack of demographic data including race, age, and sex. In this study, we have conducted morphometric analysis of the lumbar vertebrae in a relatively large number of Indian patients by using computed tomography scan. The morphometric data thus compiled may provide a baseline of body and canal dimensions that could guide clinical experts in their practice.
Conclusions: The dimensions of the lumbar vertebrae and bony canal thus obtained shall provide a baseline normative data for evaluation of patients presenting with low backache and lumbar canal stenosis in an Indian population.
INTRODUCTION
The vertebral column has a complex anatomy and has long been an area of research. Lumbar spondylosis is a problem of adults but is now being increasingly seen in youth, probably due to lifestyle changes. Radiological evaluation forms an important part in evaluation and management of lumbar spondylosis. Multiple factors play a role in spondylosis, but if it is associated with spinal canal stenosis, its management differs. Lumbar canal stenosis is a condition in which the anteroposterior (AP) and lateral dimensions of the bony spinal canal are less than normal for corresponding age and sex. The most common manifestation of lumbar canal stenosis is low backache. Therefore, the dimensions of lumbar vertebrae are very important in clinical diagnosis of lumbar spinal stenosis and lower backache (LBA).
Kirkaldy-Willis et al1 classified lumbar spinal canal stenosis into developmental, degenerative, and other types. Verbiest2 showed that the developmental stenosis is due to the properties of the neural arch, pedicles, laminae, and articular processes in which the interpedicular distances are normal, whereas lateral sagittal diameters are shortened due to thickened laminae and articular processes. The degenerative stenosis with secondary osteoarthritis of the segmental spine is more marked opposite the intervertebral disc and posterior articular processes, whereas AP and lateral diameters may be normal.
The combined stenosis shows overall narrowing of the spinal canal or segmental narrowing, protrusion of a disc, or any combination of these, associated with more neurological symptoms than developmental and degenerative types are.
Numerous studies have been conducted to determine morphometry of lumbar vertebrae in a western population using fresh cadaver or osteologic collections.3–5 They had adequate sample sizes but lacked demographic data including race, age and sex.6 Computed tomographic (CT) images have been used more recently to study lumbar vertebrae.7,8 The recent use of CT for the measurements of the different vertebral dimensions such as canal diameter and vertebral dimension has led to better evaluation of vertebral morphometry as compared with x-ray and cadaveric studies.9
In this study, we conducted morphometric analysis of the lumbar vertebrae in a relatively large number of patients by using CT scans. The morphometric data thus compiled may provide a baseline of body and canal dimensions that could guide clinical experts in their practice.
MATERIALS AND METHODS
This observational study was conducted in one of North India's premier tertiary care institutes. A total of 302 patients over a period of 1 year undergoing diagnostic CT scans for abdominal or genitourinary complaints or patients attending the radiology department for a radiological investigation of regions other than the vertebral column pathology or gross spinal pathology during the study period were included in the study. Of 302 patients studied, 174 (57.6%) were men and 128 (42.4%) were women (Table 1).
Age distribution.
Exclusion criteria included all individuals with age <20 years or age >40 years, with gross spinal pathology and neurological deficit due to spinal condition, major chronic systemic disease such as chronic liver diseases and chronic kidney diseases, clinically labeled as dwarfism, movement artifact, or metallic artifact.
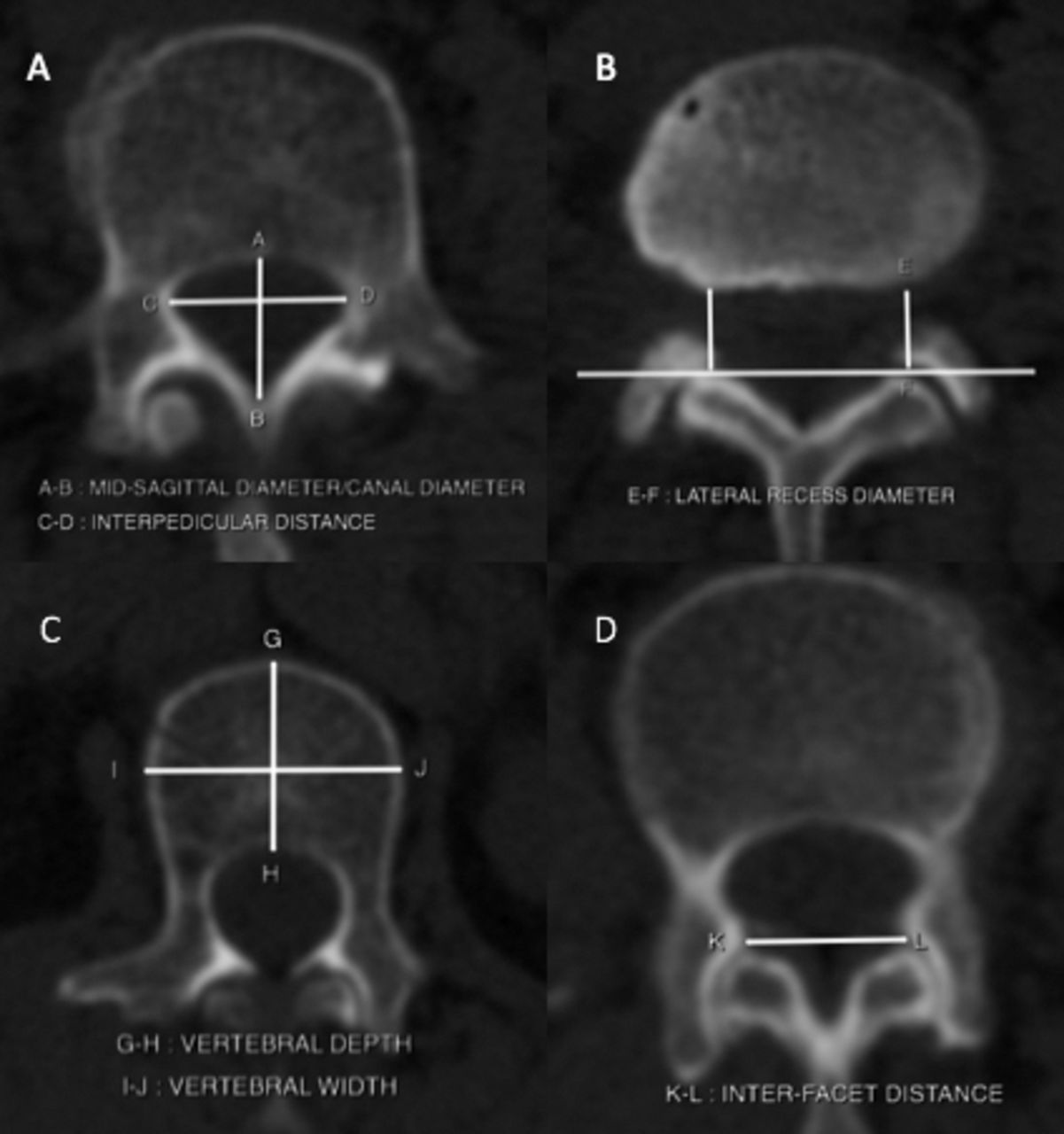
A CT scan was performed using 64-slice and 128-slice multi-detector CT. Unenhanced CT was performed from the level of diaphragm to pubic symphysis with the area to be covered (field of view) from D12 vertebra to S1 vertebra. Sections 3-mm thick with reconstruction up to 1 mm were analyzed. The images were reconstructed in true axial, coronal, and sagittal planes. The scans were reformatted with bone windows in axial, sagittal, and coronal planes. Measurement was done as shown in Figure 1.

A: Spinal canal diameter/midsagittal diameter—(A–B) Distance between posterior border of the vertebrae to the lamina at the midline. Spinal canal width (interpedicular distance) (C–D) Maximum distance between pedicle. B: Lateral recess diameter—(E–F) The distance between the posterior aspect of the vertebral body and anteromedial point of facet joints. C: Vertebral depth—(G–H) Distance between anterior and posterior end of vertebral body in the plane of the upper and lower end plate respectively. Vertebral width—(I–J) Distance between the lateral border of the vertebral body in the plane of the upper and lower end plate respectively. D: Interfacet distance—(K–L) Distance between the anteromedial points of the facet joint.
Data were processed and analyzed with SPSS, version 17 (SPSS Inc, Chicago, IL), with P value of .05 set to be significant.
An unpaired t test was used to compare the different dimensions of the lumbar spine of Indian patients with those of other populations, and an independent t test was used to compare male and female populations.
RESULTS
In our study, we measured different parameters of each vertebra from D12 to S1. For simplicity, we divided these parameters broadly into 2 groups:
Vertebral dimensions include upper and lower vertebral width, upper and lower vertebral depth, and intervertebral disc height.
Canal dimensions includes spinal canal AP diameter, lateral recess diameter, intervertebral foramen diameter, and interfacet distance.
We measured the different dimensions of vertebrae and compared between men and women by applying an independent t test. We also compared our study with other studies.
Canal Diameters
The diameters of the spinal canal were found to change both transversely and anteroposteriorly from D12 to S1. The AP diameters of the spinal canal gradually decreased from D12 to L4, followed by an increase at L5 and then a decrease from L5 to S1 both in men and women; thus, it was observed that the shape of the spinal canal was changing cranio-caudally from circular to oval. The maximum spinal canal depth (SCD) was noted at the D12 level (in men, SCD = 16.19 mm; in women, SCD =16.33 mm) and minimum spinal canal depth was noted at the S1 level (in men, SCD = 11.00 mm; in women, SCD = 11.19 mm). There was not much difference in SCDs between the vertebrae of men and women (P > .05), but values of the AP diameter of the spinal cord were greater in women than in men (Table 2).
Canal dimensions (mean ± SD).
The right and left lateral recess diameter (LRD) gradually decreased from D12 to S1 in both men and women, as depicted in Table 2. The maximum LRD was noted at D12 (in men, right LRD = 11.45 mm, left LRD = 11.60 mm; in women, right LRD = 9.46 mm, left LRD = 9.67 mm). The minimum LRD was noted at S1 (in men, right LRD = 7.50 mm, left LRD = 7.61 mm; in women, right LRD = 7.45 mm, left LRD = 5.80 mm). The LRD was significantly more in men from the D12 to L5 vertebrae (P < .05). There was a significant difference between right and left diameters at all levels (P < .05).
The right and left intervertebral foramen diameter (IVFD) constantly decreased from D12 to S1 in both men and women, as depicted in Table 2. The maximum IVFD was noted at D12 (in men, right IVFD = 10.62 mm, left IVFD = 10.50 mm; in women, right IVFD = 10.43 mm, left IVFD = 10.46 mm). The minimum IVFD was noted at S1 (in men, right IVFD = 5.77 mm, left IVFD = 5.57 mm; in women, right IVFD = 5.80 mm, left IVFD = 5.75 mm). There was no significant difference between men and women at all levels. A significant difference between right and left was seen only at the S1 level (P < .05).
Interfacet distance (IFD) increased gradually from D12 to S1 in both men and women. The minimum IFD was noted at D12 (in men, IFD = 15.12 mm; in women, IFD = 14.33 mm).The maximum IFD was noted at S1 (in men, IFD = 27.91 mm; in women, IFD = 26.89 mm). The IFD was significantly (P < .05) larger in men from the D12 to L5 vertebrae (Table 2).
Dimensions of Vertebral Body
Significant differences were noted between men and women in most of the dimensions of lumbar vertebral bodies.
Upper vertebral width (UVW) progressively increased from D12 to S1 in both men and women, as depicted in Table 3. The minimum UVW was noted at D12 (in men, UVW = 36.99 mm; in women, UVW = 34.62 mm). The maximum UVW was noted at S1 (in men, UVW = 49.08 mm; in women, UVW = 46.17 mm). The UVW was significantly larger in men at all levels (P< .05).
Vertebral dimensions (Mean ± SD).
Lower vertebral width (LVW) gradually increased from D12 to L5, followed by a decrease at the S1 level in both men and women. The minimum LVW was noted at S1 (in men, LVW = 30.78 mm; in women, LVW = 29.67 mm).The maximum LVW was noted at L5 (in men, LVW = 46.93 mm; in women, LVW = 45.91 mm. The LVW was significantly larger in men at all levels (P < .05; Table 3).
Upper vertebral depth (UVD) progressively increased from D12 to L5, then it decreased at S1 in both men and women. The minimum UVD was noted at D12 (in men, UVD = 27.09 mm; in women, UVD = 25.10 mm). The maximum UVD was noted at L5 (in men, UVD = 32.41 mm; in women, UVD = 30.94 mm). The UVD was significantly (P < .05) larger in men at all levels (Table 3).
Lower vertebral depth (LVD) increased from D12 to L4, followed by a decrease from L5 to S1 in men, but in women it progressively increased from D12 to L5, followed by a decrease at S1. The minimum LVD was noted at S1 (in men, LVD = 22.78 mm; in women, LVD = 22.03 mm). The maximum LVD was noted at L4 in men (LVD = 32.15 mm) and in women at the L5 level (LVD = 30.30 mm). The LVD was significantly (P < .05) more in men at all levels (Table 3).
Intervertebral disc height (IVDH) gradually increased from D12 to L4, but decreased progressively from L5 to S1 in both men and women, as depicted in Table 3. The minimum IVDH was noted at S1 (in men, IVDH = 3.55 mm; in women, IVDH = 3.35 mm). The maximum IVDH was noted at L4 (in men, IVDH = 10.60 mm; in women, IVDH = 10.23 mm). The IVDH was significantly larger in men at all levels (P < .05).
DISCUSSION AND COMPARISON WITH OTHER STUDIES
Low backache is the most common complaint requiring radiological investigations in current setup.10 Assessment of lumbar canal size is one of the most essential steps in diagnosing LBA.11 Any pathological changes in the structures that surround the spinal canal and foramina may disturb the alignment of the spinal canal in the lumbar region, resulting in LBA.11 Hence, the morphology of the lumbar vertebrae shows regional curvatures on the sagittal plane that are necessary for absorbing impact and reducing stiffness.10
Lumbar spinal stenosis is a result of a narrowing of the bony spinal canal or intervertebral foramina, resulting in secondary compression of the spinal cord traversing centrally and spinal nerve roots traversing laterally through the intervertebral foramina. Clinically, lumbar spinal stenosis presents as LBA, paresthesia, and bilateral lower limb pain.12,13 The data thus presented in our study provide relevant clinical and anatomical information on lumbar vertebral and canal dimensions in a relatively large sample size.
Population-specific variations in dimensions of body segments exist, thus necessitating continuous data gathering of lumbar dimensions in various population groups. In addition, whereas most studies have been done on a western population using cadaveric samples, no reliable source exists for an Indian population that also uses CT data. Hence, it is necessary to have a large data set to compare with radiographic and osteologic techniques with a view to providing a reference standard for lumbar dimensions within the Indian population group.
Canal Diameters
The AP diameters of the spinal canal gradually decreased from D12 to L4 but marginally increased at L5 and then decreased from L5 to S1 in both men and women; thus, the shape of the spinal canal was changing from circular to oval. The values of the AP diameter of the spinal cord were greater in women than in men. Similar results were observed in the Telangana population by Kumar et al,7 who examined CT-scan–based measurements of the lumbar spine in 61 adult patients (Table 4).
Spinal canal anteroposterior diameter comparison with other studies.
Right and left LRD decreased from D12 to S1 in both men and women. Significant difference was found between men and women in LRD, which was significantly larger in men at the D12 to L5 vertebrae (P < .05). There was significant difference between right and left diameters at all levels (P < .05). A similar pattern was also observed by Alam et al14 in a Pakistani population for both men and women (Table 5).
Lateral recess diameter comparison with other studies.
Right and left IVFD constantly decreased from D12 to S1 in both men and women. The maximum IVFD was noted at D12 and the minimum IVFD was noted at S1. There was no significant difference (P > .05) between men and women at all levels. Significant difference between right and left was seen only at the S1 level (P < .05).
Interfacet distance increased gradually from D12 to S1 in both men and women. The minimum IFD was noted at D12 and the maximum IFD was noted at S1. The IFD was significantly larger in men at all levels (P < .05).
Vertebral Dimensions
Upper vertebral width increased from D12 to S1 in both men and women. Similar results were found by Singh et al15 on a study of 20 cadavers. Alam et al14 studied a Pakistani population and Kang et al16 studied a Korean population using CT morphometry; in both studies, researchers observed similar trends of an increase of UVW cranio-caudally from L1 to L5 (Table 6).
Upper vertebral width comparison with other studies.
Lower vertebral width increased from D12 to L5 but decreased at the S1 level in both men and women. Lower vertebral width was significantly larger in men at all levels (P < .05). A similar study by Singh et al15 on 20 cadavers from a north Indian population noted that LVW increased from L1 to L2 then decreased at L3, followed by an increase from L3 to L5. This pattern was not seen in our study. Alam et al14 conducted a study of measurement of lumbar vertebrae by CT scan on 49 patients from a Pakistani population and noted similar patterns in both men and women, as seen in our study. The values of LVW was greater in men than in women, similar to our study (Table 7).
Lower vertebral width comparison with other studies.
Upper vertebral depth increased from D12 to L5, then it decreased at S1 in both men and women. Upper vertebral depth was significantly larger in men at all levels (P < .05). A similar pattern also was observed by Alam et al14 in a Pakistani population in both men and women. The values of UVD were greater in men than in women at all levels, similar to our study (Table 8).
Upper vertebral depth (anteroposterior diameter) comparison with other studies.
Lower vertebral depth increased from D12 to L4, followed by a decrease from L5 to S1 in men, but in women it progressively increased from D12 to L5, followed by decrease at S1. The minimum LVD was noted at S1 in both men and women, and the maximum LVD was noted in men and in women at L4 and L5, respectively. Lower vertebral depth was significantly larger in men than in women at all levels (P < .05). Similar patterns were observed in a study on a Pakistani population by Alam et al.14
Intervertebral disc height gradually increased from D12 to L4, followed by a progressive decrease from L5 to S1 in both men and women. In both men and women, minimum and maximum IVDH were noted at the S1 and L4 levels, respectively. Intervertebral disc height was significantly larger in men at all levels (P < .05).
CONCLUSIONS
In our study, we measured different parameters (vertebral and canal diameters) of vertebrae from D12 to S1 in an Indian population with the help of CT scans in a relatively large number of patients (N = 302), which was more clinically relevant and accurate in contrast to cadaveric or manually measured data. We compared our study with other studies from the same subcontinent as well as from other parts of world. The present study also provided a comparison between men and women, and we found significant differences in various dimensions of lumbar vertebrae.
The AP diameters of the spinal canal gradually decreased from D12 to L4, followed by an increase at L5, and then decreased from L5 to S1 both in men and women. On comparison, similar trends were noted with other studies, but the values were lower in our research. Vertebral dimensions (vertebral width, vertebral depth) progressively increased from D12 to S1. On comparison, similar trends were observed in other studies.
The dimensions of the lumbar vertebrae and bony canal thus obtained will provide a baseline normative data for evaluation of patients presenting with LBA and lumbar canal stenosis in an Indian population.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- ©International Society for the Advancement of Spine Surgery
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
In this issue




{kind=link}