


ABSTRACT
The treatment of early-onset scoliosis with magnetic growing rods has been established, but the management at the end of the lengthening program is still controversial. The options available are removal of rods and observation, removal of rods and immediate fusion, or replacement/maintenance of rods. We present 2 cases of early-onset scoliosis patients treated with Magec rods, up to skeletal maturity. In the first case of a Lenke 3 scoliosis (14 years and 11 months) with a thoracic curve of 50° and lumbar curve of 40°, we removed the rods and kept the patient under observation. After 5 months, the patient showed curve progression, with a thoracic curve of 61° and a lumbar curve of 57°. Consequently, we performed an instrumented T4 to L4 fusion with a correction of the thoracic curve of 66% and lumbar curve of 60%. In the second case of a Lenke 1 scoliosis (15 years and 10 months) with a thoracic curve of 38°, the rods were removed and the patient was kept under observation. After 10 months, following a curve progression, presenting a thoracic curve of 72°, we performed an instrumented fusion T5 to L2 and right thoracoplasty (6th to 11th ribs) with a 40% curve correction. Observing these 2 cases at the end of the treatment with Magec rods, even in case of a good and satisfying final correction, skeletal maturity, and secondary sexual characteristics, we recommend immediate instrumented spine fusion.
- early-onset scoliosis
- magnetic growing rods
- rods' removal
- spontaneous spine autofusion
- skeletal maturity
- immediate instrumented fusion
INTRODUCTION
Early-onset scoliosis (EOS) is a spinal deformity in children ages 10 years or younger, with idiopathic, neuromuscular, congenital, and syndromic etiology. Untreated EOS patients show a high risk of thoracic insufficiency, impaired cardiopulmonary function, and early mortality rates.1 Additionally, early spinal fusion, before lung maturity, is associated with a significant morbidity due to respiratory complications.2 The development of modern surgical techniques based on guided growth, vertebral compression, or distraction-based implants has intended to avoid these dramatic consequences. EOS treatment with Magec rods has been established, but patient management at the end of the lengthening period, until skeletal maturity, remains controversial. In the literature, the reported options3 are the rods' removal followed by patient observation, rods' removal and immediate instrumented fusion, or rod maintenance/replacement. We present 2 cases of EOS patients treated with Magec rods (NuVasive Specialized Orthopedics Inc, Aliso Viejo, CA) up to skeletal maturity. After the complete lengthening, the authors decided to remove the rods and keep the patient under observation because we observed a good correction of scoliosis, the complete Risser and the appearance of secondary sexual characteristics at the end of treatment with rods. Data for this investigation were collected and analyzed in compliance with the procedures and policies set forth by the Helsinki Declaration, and the parents of 2 patients gave their informed consent to data treatment.
CASE REPORTS
The first patient, a girl who came to our observation at the age of 10 years with a Lenke 3 scoliosis right thoracic 34° and left lumbar 43°, for which we implanted 2 Magec rods (size 5.5-mm standard rod on the right and offset rod on the left, actuator 90 mm) anchored with pedicle screws in T3 to T4 and L3 to L4. After periodic distractions (1 mm every 3 months), we removed the rods at the age of 14 years and 11 months, with a final right thoracic curve of 50° and left lumbar of 40° (Risser 5). Periodic radiographic follow-ups showed both curves' progressions and a shortening of the trunk. Therefore, 5 months after the rods' removal, starting from a right thoracic 61° curve and a left L 57° curve, we performed a final instrumented fusion T4 to L4. Given the good flexibility of the curve, we obtained an excellent clinical and radiographic results, with a final correction of the thoracic curve of 66% and the lumbar curve of 60% (Figure 1).
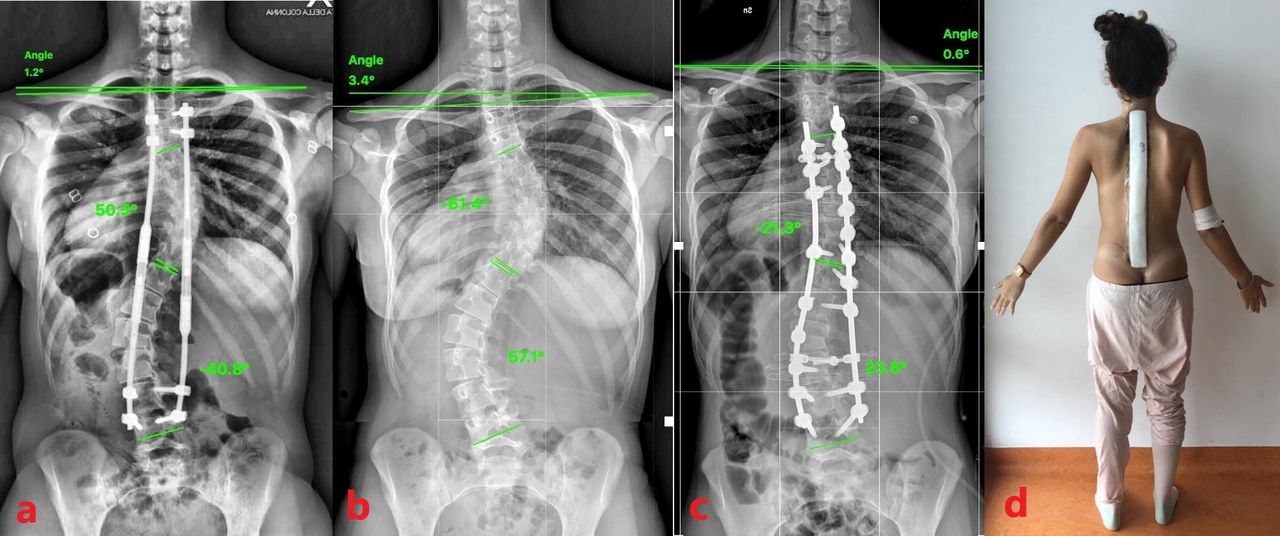
1° case. a) At age 14 years and 11 months, the final distraction of the Magec rods was reached; the radiologic image shows a right thoracic curve of 50° and a left lumbar curve of 40° (Risser 5). b) Five months after removal of Magec rods, the radiologic image shows the curves worsening, with a right thoracic curve of 61° and a left lumbar curve of 57°. c) The radiologic image shows an instrumented fusion T4 to L4 with a right thoracic curve of 21° and left lumbar curve of 23°. d) The clinical image shows the excellent final results.
The second patient is a girl who came to our observation at the age of 10 and a half years, with a Lenke 1 scoliosis right thoracic of 45°. In this case we implanted 2 Magec rods (size 5.5-mm standard rod on the left and offset rod on the right, 90-mm actuator) anchored with hooks in T4 to T5 and pedicle screws in L3 to L4. After periodic distractions, we removed the rods at the age of 15 years and 10 months with a right thoracic curve of 38° (Risser 5). Periodic radiographic controls showed both a progressive and severe progression of the curve, with an evident rib hump and significant shoulder malalignment. Therefore, 10 months after the rods' removal, starting from a right thoracic curve of 72°, we performed a T5 to L2 final instrumented fusion (Figure 2). In this second case, because of the rigidity of the curve, due to a spontaneous fusion in the convexity of the curve, an important rib hump (Figure 3), and to improve the aesthetic result, we decided to associate a right thoracoplasty at the apex of the ribs' deformity (from the 6th to the 11th rib), but resulting in a subsequent pleural effusion. The clinical and radiographic final results were good, with a correction of the right thoracic curve of 40% and well-balanced spine (Figure 2, c and d).
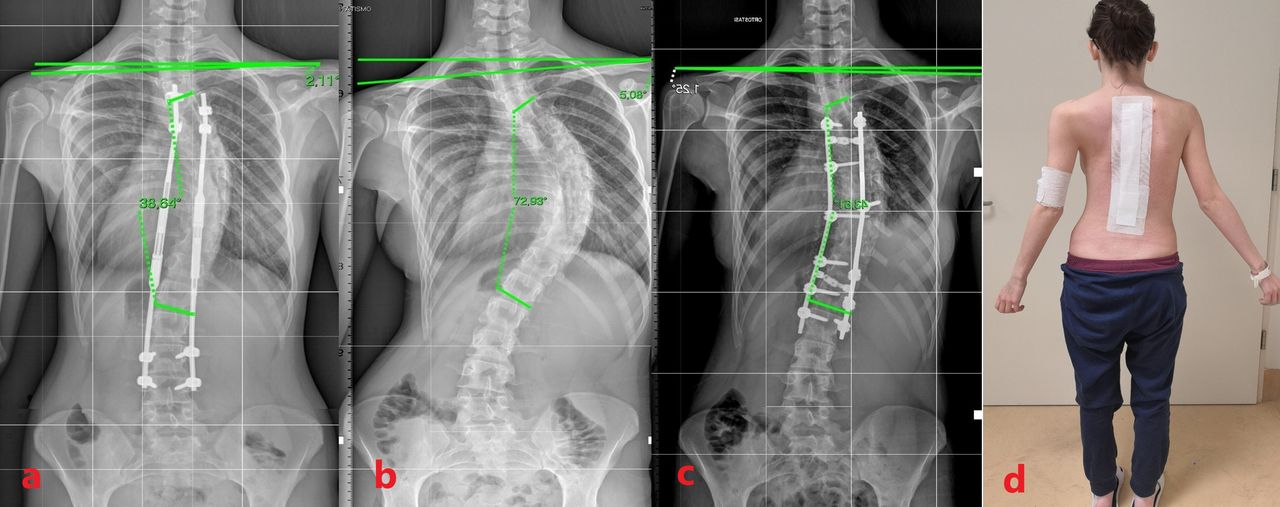
2° case. a) At age 15 years and 10 months, the final distraction of the Magec rods was reached; the radiologic image shows a right thoracic curve of 38° (Risser 5). b) Ten months after removal of the Magec rods, the radiologic image shows the curve's evolution, with a right thoracic curve of 72°. c) The radiologic image shows an instrumented fusion T5 to L2 with a right thoracic curve of 43° and right thoracoplasty (6°–11° ribs). d) The clinical image shows the good final results.

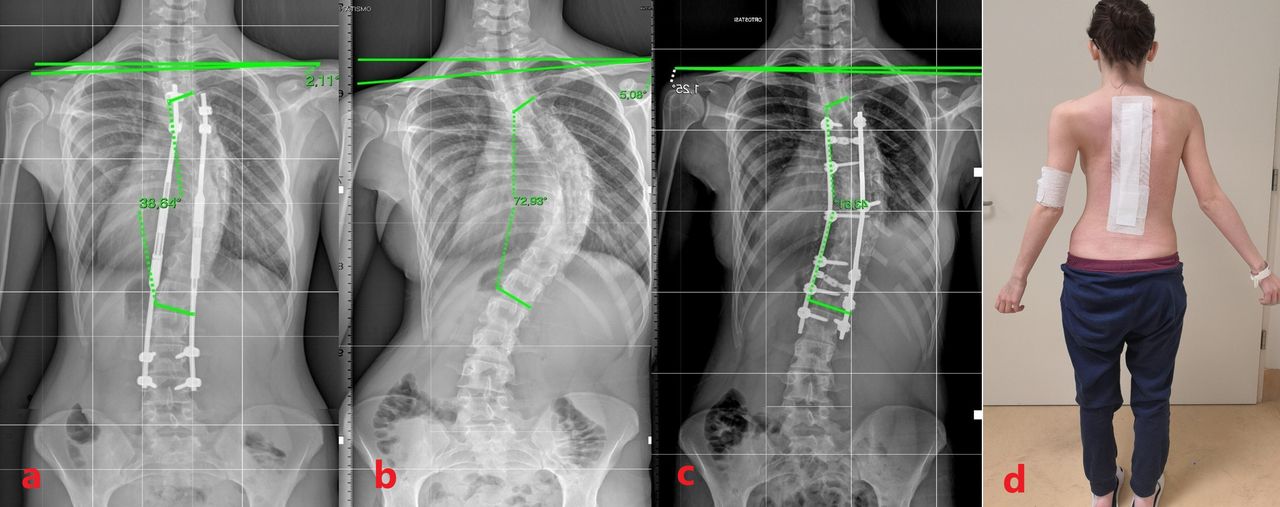
2° case. a) The clinical image, at 10 months after removal of Magec rods, shows the clear worsening, with an unbalanced trunk and shoulders. b) The clinical image, at 10 months after removal of Magec rods, points out a severe ribs hump (Adams test). c) The intraoperative picture, during the final instrumented fusion, shows an arthrodesis (blue arrow) on the convexity side of the thoracic curve, a sign of spontaneous autofusion.
DISCUSSION
Since their introduction, the growing rods have been an effective and safe method to control progressive and severe deformity in a young child, until the trunk reaches an adequate height, while preserving the implicit intention of performing the final fusion. In 2010, Cahill et al4 demonstrated high rates (89%) of spontaneous autofusion in patients with immature spines who were treated with growing rods. Therefore, the authors considered the final fusion, when in the presence of skeletal maturity and good correction, to be unnecessary. The final instrumented fusion, after distraction-based devices, is associated with high complication rates.5,6 In 2017 Kocyigit et al3 mentioned a comparative study in patients treated with growing rods, and they concluded that in patients who achieved skeletal maturity, rod removal without new instrumentation is an unacceptable treatment because it leads to a worsening of the deformity. The results in the 2 presented cases confirm the conclusions of Kocygit et al.3 Despite observing, after the rods' removal, an acceptable and satisfying final correction (≤50°), skeletal maturity (Risser 5), and the appearance of secondary sexual characteristics, we also observed a rapid progression of the deformity. Because of this experience, some observations are needed.
The Risser test may not be entirely reliable for evaluating the potential for further skeletal growth. Minkara et al7 believe that the Sanders classification should be used to guide treatment options in patients with Adolescent Idiopathic Scoliosis because Risser staging results in mistreatment in a total of 1 of 4 patients compared with the Sanders classification.
Spontaneous autofusion after rod removal cannot be a realistic parameter to be taken into consideration for the decision of the subsequent treatment. Jain et al8 outlined several important considerations regarding the quality of the autofusion after growing-rod treatment in EOS: first, it may be incomplete, with some immobile segments and others with some preserved mobility; second, the autofusion mass may be thin; and third, the durability of this autofusion mass is unknown.
The decision to perform spinal fusion at the end of distraction-based treatment is complex and multifactorial, based on patient history and features, family, and surgeon-specific factors.6 In fact, in the first case presented, the choice of final fusion was influenced not only by the progression of the deformity, but mostly by the insistence of the girl and her family members, who did not accept the final aesthetic result. Regarding the second case presented, the choice of final fusion was influenced by the rapid and severe increase in the thoracic curve of about 50%, with an unacceptable aesthetic appearance caused by an important rib hump and trunk imbalance (Figure 3, a and b).
Lastly, the timing of the final instrumented fusion is very important. We observed that the more time that had passed since the rods removal, the more the complex and invasive posterior instrumented resulted, with a consequently less satisfactory final result. In fact, in the second case, 10 months after the rods' removal, the curve had an important thoracic rotation; it was rigid (Figure 3) and required additional thoracoplasty surgical time, with subsequent pleural effusion as a complication.
Because of our limited experience, for those EOS patients treated with distraction devices, when skeletal maturity has been reached, we strongly recommend immediate final instrumented fusion when the growing rods are removed. The “watchful waiting” alternative, leaving the rods in place, could be an option, but currently the risk of complications from long-term observation, such as implant pain or failure, or curve progression, and late infection, still remains unknown.
Footnotes
Disclosures and COI: The authors received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.