


ABSTRACT
Background: The treatment of atlantoaxial instability (AAI) involves stable fixation and fusion with adequate decompression of spinal cord. After the advent of the Goel posterior joint manipulation technique, most of the once irreducible atlantoaxial dislocations (AAD) could be reduced and the need for transoral odontoidectomy became almost nil. Here we tried to iterate the indications of anterior transoral odontoid surgery for AAI in the current scenario.
Methods: A retrospective study compiling the clinical, radiological, and surgical characteristics of 6 cases (5 scenarios). These patients underwent anterior transoral surgery alone or in combination with a posterior approach.
Results: Two patients had a well-formed occipito-cervical fusion mass, with a displaced odontoid and unreduced C1-C2 joint causing cervical myelopathy. A middle-aged woman presented with unreduced AAD following failed C1-C2 joint distraction technique. A displaced dystopic os odontoideum ossicle was found in an adolescent boy, prohibiting the reduction of AAD. A young man had displacement of the fractured odontoid segment with intact transverse alar ligament and C1-C2 joint complex. One patient had a rare scenario of abnormal orientation of the C1-C2 joint. All 6 patients were successfully treated with adequate spinal cord decompression achieved by the anterior transoral route and stabilization by either the anterior approach itself or in combination with posterior surgery. All had significantly better postoperative outcomes except for 1 patient who expired due to poor respiratory reserve.
Conclusion: We tried to emphasize the indications for using transoral anterior odontoid surgery over the posterior approach in the management of AAI. This will prevent the surgical technique of anterior odontoidectomy from becoming an obsolete procedure in the current practice.
INTRODUCTION
Atlantoaxial dislocation (AAD) is a serious condition of the cranio-vertebral junction resulting in spinal cord compression and significant neurological deficits. Several pathologies such as trauma, inflammatory diseases, congenital abnormalities, and idiopathic causes can result in atlantoaxial instability (AAI).1 However, the management strategy for all AAIs remains the same. The treatment is mainly aimed at achieving a stable fixation and fusion with adequate decompression of the spinal cord.2 Traditionally, AADs have been classified as “mobile or reducible” and “immobile or irreducible” subtypes.3 The advent of a posterior joint manipulation technique revolutionized the management strategies for AAD. It was proposed that even irreducible subtypes could be reduced by posterior approach techniques.4 The conventional transoral odontoid surgery described by Scoville et al used to be a standard approach and was used extensively until the recent era, when it was replaced by the Goel/Harms posterior technique.5 Currently, it is being performed mainly as a release procedure for certain specific subtypes of AADs where the posterior approach is not plausible.6 This procedure was rendered obsolete in recent times due to the requirement of a steep learning curve among the performing surgeons, latest technological advancements in surgical approaches, and near-perfect restoration of cranio-vertebral junction physiology in posterior reduction techniques. Because the surgical skills of the transoral approach are dwindling among budding spine surgeons, we tried to emphasize its importance in the current practice by presenting few case scenarios. We have also tried to reiterate the specific indications for using transoral anterior odontoid surgeries in AAI.
MATERIAL AND METHODS
We performed a retrospective review of all the AAI patients operated upon in our tertiary care center from 2010 to 2019. The clinical, radiological, and surgical characteristics of 146 such patients were reviewed, and those who had undergone a stand-alone posterior approach (n = 132/146) were excluded. Patients who had undergone anterior transoral surgery alone or in combination with the posterior approach were included for the current study and their cases were analyzed. Routine transoral surgeries for taking biopsies (n = 4) and tumor excision (n = 4) were excluded. We obtained 6 patients under 5 rare but important scenarios The different clinical scenarios include the following:
1 . Displaced odontoid; well-formed occipito-cervical fusion mass
2 . Failed C1-C2 joint distraction technique
3 . Dystopic os odontoideum prohibiting reduction
4 . Displacement of fractured odontoid; intact transverse alar ligament (TAL) and C1-C2 joint
5 . Abnormal orientation of the C1-C2 joint complex
In this study, each case scenario is presented separately in the “Results” section and discussed at the end.
RESULTS
Scenario 1: Cervical Myelopathy Secondary to Unreduced AAD With a Well-Formed Occipito-Cervical Fusion Mass
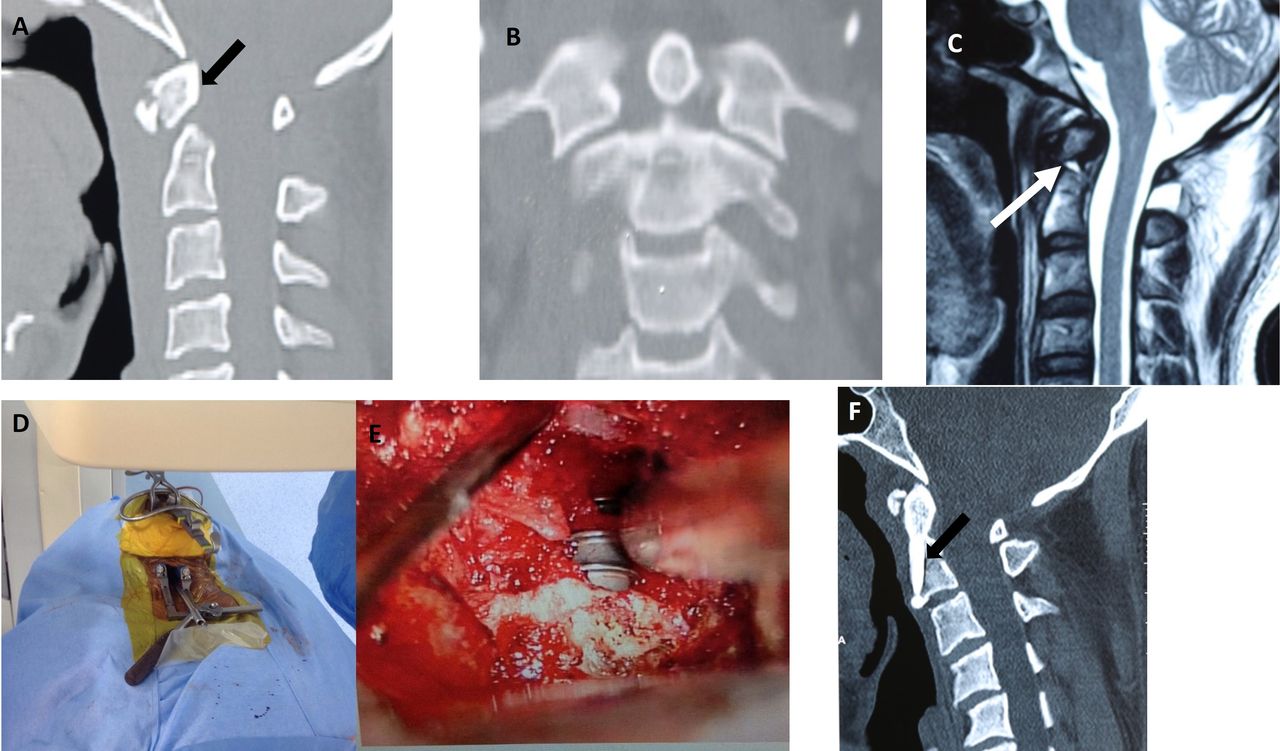
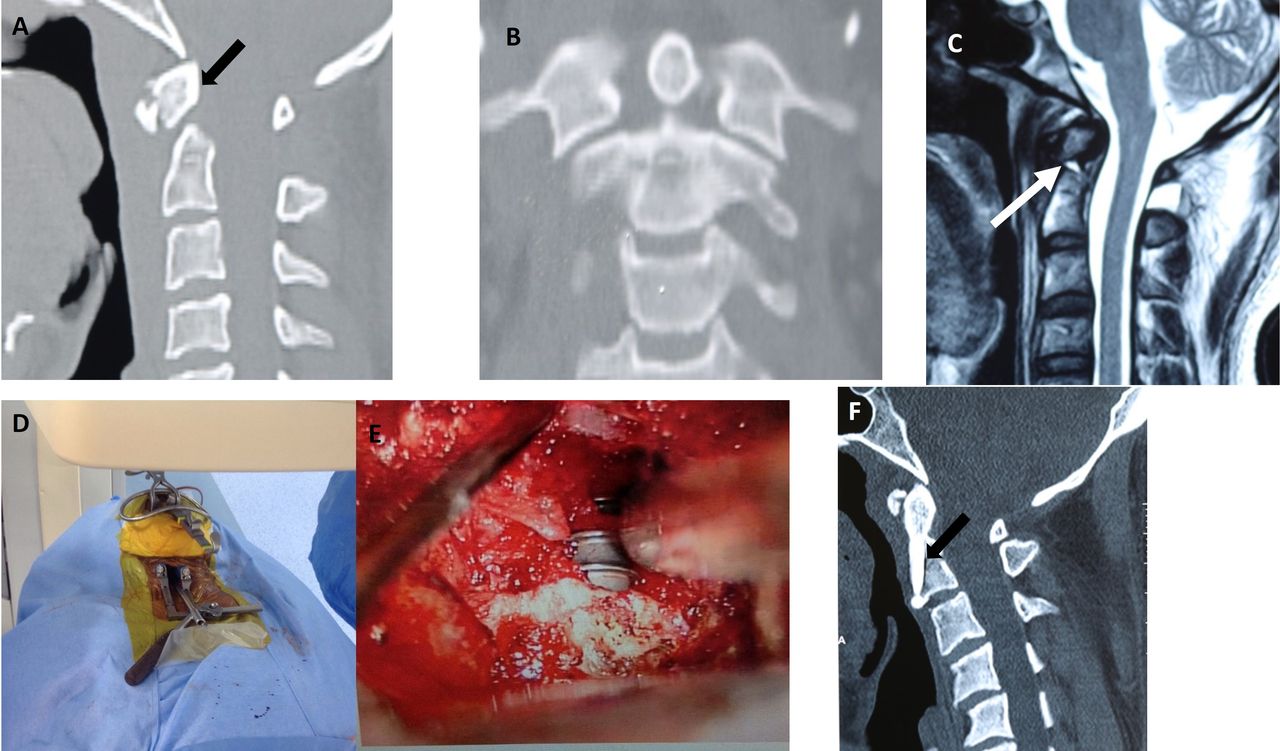
A 67-year-old wheelchair-bound woman presented to us with gait disturbances and progressive upper limb weakness of 5 years duration. Clinically she had features of upper cervical myelopathy and was wheelchair-bound with significant loss of proprioception. Her Japanese Orthopaedic Association (JOA) score was 9/18. She was operated upon elsewhere with occipito-cervical wiring and iliac bone onlay grafting 3 years back with no significant improvement in her symptoms. Computed tomography (CT) scan of the spine showed persistent AAD with an assimilated atlas, well-healed fusion mass extending from occiput to C2 vertebrae, and wires in situ (Figure 1A–1D). MRI showed significant cord compression by the displaced odontoid with myelomalacia at the atlantoaxial level (Figure 1E). Considering a good fusion between occiput and C2 with no movement happening at the C1-C2 joint in flexion or extension and the pathology being direct extradural compression by the odontoid, a plan for transoral odontoidectomy was made (Figure 1F). Postoperatively, she improved significantly with rigorous neurorehabilitation, and by the end of 24 months she was ambulating independently. Her posterior column symptoms and activities of daily living improved exceptionally, and the JOA score improved to 15/18 (Figure 1G).

(A–G) Scenario 1: (A) X-ray of 67-year-old woman with occipito-cervical wiring and bone grafting done outside. (B–D) Preoperative computed tomography of the spine shows well-fused C1-C2 (arrows), making a posterior approach practically impossible. Atlantoaxial dislocation with narrowing of the spinal canal is also observed. (E) T2 MRI sagittal section of cervical spine with high cervical cord compression, myelomalacia, and signal changes. (F) Preoperative image showing decompressed spinal cord after excising odontoid and C1 arch by the transoral approach. (G) Postoperative x-ray shows removal of wires with absent resected odontoid.
A 41-year bed-bound man presented to us with clinical features of cervical myelopathy. His JOA score was 7/18, and he had an occipto-cervical fusion performed 5 years earlier with no clinical improvement. The implant was removed, and MRI showed significant anterior cervical cord compression by the unreduced AAD secondary to the odontoid process. The posterior elements of the spine showed a completely fused mass from occiput to C3 vertebrae. He underwent anterior transoral odontoidectomy for decompression. At the 18-month follow-up, the JOA score was 10/18, indicating significant improvement.
Scenario 2: Cervical Myelopathy Secondary to Unreduced AAD and Failed C1-C2 Joint Distraction Technique
A 38-year-old woman with clinical features suggestive of high cervical myelopathy and a JOA score of 12/18 was operated upon by the Goel technique a year before presenting to us. She came with failed improvement post–C1-C2 fusion surgery. Imaging revealed a spacer between the C1-C2 joint with a fusion mass extending across and over the C1-C2 posterior elements as well as cord compression by the odontoid process secondary to unreduced AAD. She underwent transoral odontoidectomy with substantial improvement in sensory disturbances, and the follow-up JOA score at the end of 12 months was 15/18.
Scenario 3: Dystopic Odontoid Ossicle Lying Between the C1 Arch and Odontoid Process
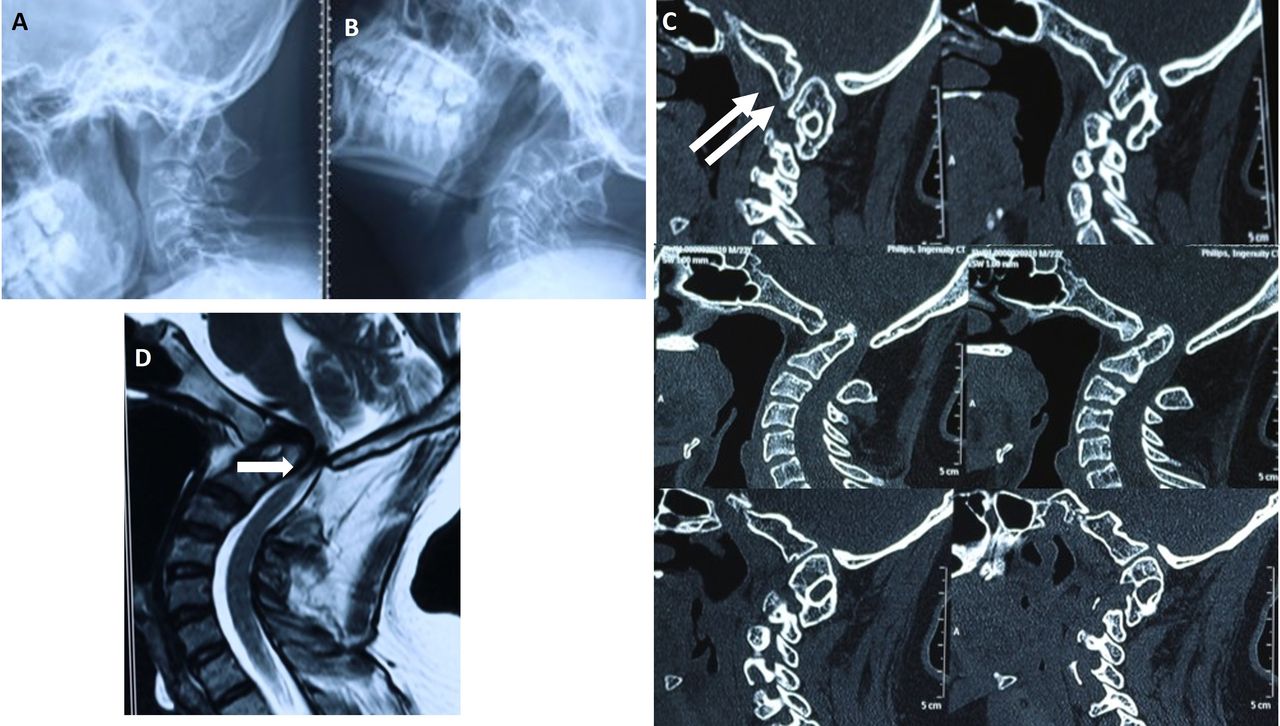
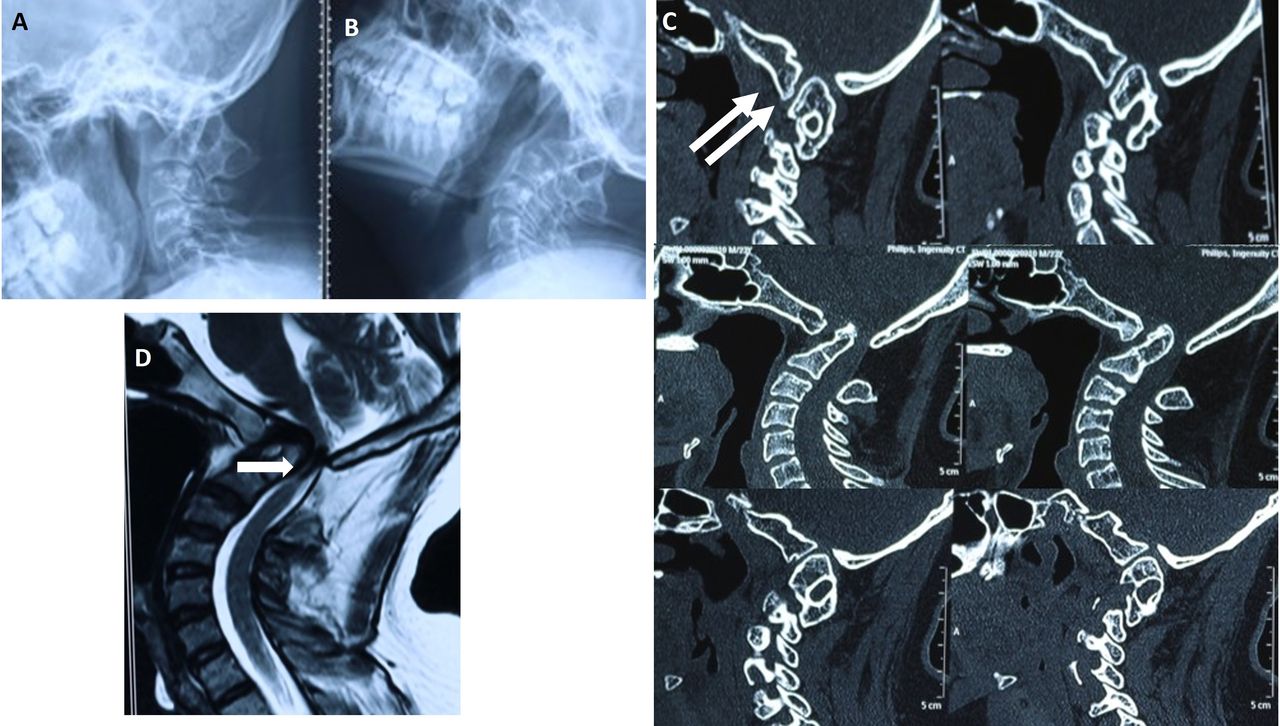
A 14-year-old boy came with a history of trauma to the neck 1 year earlier, with acute onset and progressive weakness of upper and lower limbs. He had cervical myelopathy with a JOA score of 9/18. The CT and MRI of the spine revealed AAD with a dystopic os odontoideum ossicle producing cord compression and myelomalacia. The malunited odontoid ossicle was found between the C1 vertebral arch and the C2 odontoid process, which can prohibit the reduction of AAD even with a posterior joint-manipulation technique (Figure 2). It was decided to do a staged procedure whereby the anterior transoral odontoidectomy was performed in the first stage along with skull traction. The second-stage procedure was stabilization of the spine from occiput to C3 level with wiring, rods, and iliac grafts. The boy was followed up for 2 years and had significant improvement in his JOA score with independence in all activities of daily living (13/18).

(A–E) Scenario 3: (A, B) Flexion and extension x-ray revealing unstable atlantoaxial dislocation secondary to os odontoideum (C) Preoperative computed tomography of the spine shows dystopic os odontoideum ossicle lying between C1 arch and C2 vertebra, making the joint irreducible (arrows). (D) T2 MRI sagittal section of cervical spine with high cervical cord compression. (E) Postoperative x-ray shows occipito-cervical fusion with wires and iliac bone grafting.
Scenario 4: Displacement of the Fractured Odontoid Segment
A 29-year-old man sustained injuries after a road traffic accident and presented to us with severe neck pain and no neurological deficits. He was examined and found to have a type II odontoid fracture with intact TAL, C1-C2 joint complex, and potential AAI. The apical fragment of the odontoid had displaced anteriorly and was hitching against the C1 arch (Figure 3A–3C), which did not descend with preoperative skull traction. We approached the surgery via 2 routes. The first was the classical transoral approach to dislodge the fragment from the C1 arch, and fracture reduction was achieved. A 32 × 4-mm odontoid screw was passed from the base of the odontoid to the apical fragment through a separate approach made at the C5-C6 level on the right side (Figure 3D–3E). He recovered well, and at the 1-year follow-up showed a well-united odontoid without instability and with complete preservation of rotational movements of the neck.
(A–F) Scenario 4: (A, B) Preoperative computed tomography of the spine (sagittal and coronal) demonstrates normal joint C1-C2 joint space, but the odontoid process is hitching against C1, making it irreducible (arrow). (C) T2 MRI of the sagittal section of cervical spine shows a fractured odontoid with mild hemorrhage (arrow) and normal cerebrospinal fluid space and cord. (D, E) eIntra-operative images demonstrating double incision; transoral approach for reduction of the fragment and transcervical approach through C5-C6 for the screw placement. (F) Follow-up computed tomography scan shows well-reduced and united odontoid with screw in situ (arrow).
Scenario 5: Abnormal Orientation of the C1-C2 Joint Complex
A 23-year-old man presented with sudden onset deterioration in walking following a trivial fall and had features suggestive of cervical myelopathy. His JOA score was 7/18 and he had a poor respiratory effort. The CT scan showed an assimilated C1 with abnormally vertical C1-C2 facets, suggesting congenital abnormality (Figure 4C). The tip of the odontoid process was found cranial to the McRae line, and there was an increased atlanto-dental interval, suggesting basilar invagination and AAD. The MRI showed thinning of the cervical cord secondary to compression by the odontoid process against the C1 assimilated arch (Figure 4D). We performed posterior C1-C2 joint manipulation and spacer implantation after careful resection of the joint surfaces to make the orientation horizontal, thereby reducing basilar invagination. This was followed by C1-C2 fixation with a Goel plate. The AAD reduction from the attempted posterior approach was inadequate, and hence the decision of transoral odontoidectomy for direct decompression was taken intraoperatively and executed. The patient was kept intubated postoperatively, and elective tracheostomy was done on day 3 due to poor respiratory effort. Though adequate nursing was given in the intensive care unit, the patient worsened and expired.
(A–D) Scenario 5: (A, B) Flexion and extension x-ray showing unstable atlantoaxial dislocation. (C) Preoperative computed tomography of the spine shows vertical alignment of C1-C2 joint space (arrows), assimilated C1, and basilar invagination of the bone. (D) T2 MRI of the sagittal section of cervical spine pinching the brain stem and high cervical cord (arrow).
DISCUSSION
The primary goal of surgery in any type of AAD is decompression of the cord and stabilization with good fusion of the vertebral elements.2,7 Decompression can be achieved indirectly by reducing and simultaneously fusing the C1-C2 joint, thereby pushing the odontoid process away and preventing compression of the cord.8,9 The vintage method is by direct decompression through an anterior odontoidectomy, often followed by occiput-C2 fusion.10 The transoral approach was first described by Kanavel to remove a bullet entrapped between the skull base and C1. However, it was successively implemented by Scoville and Sherman in 1951 for resection of the odontoid process in basilar impression.5 Fang and Ong used it in 1962 for the management of 6 patients with traumatic C1-C2 instability and tuberculosis of the upper cervical spine.11 The advantages of this approach include direct addressal of the compressing element and less manipulation of the spinal cord. The limitations include but are not limited to wound dehiscence and frequent infections, velopharyngeal insufficiency, poor nutritional outcomes postsurgery. After Goel's introduction of posterior reduction techniques, this approach gradually faded away due to the frequent incidence of these complications.
The first 3 cases had a common scenario: undergoing posterior fusion surgery in a different hospital and presenting to us on a later date with progressive illness or failed improvement. All had unreduced AADs and, as a result, the odontoid process was compressing the cord. These patients had completely fused posterior elements; hence, the posterior approach might result in complications such as dural injury, spinal cord damage, and vertebral artery tear due to a completely altered posterior anatomy. Moreover, one of the goals of surgery is bound to fail because there is a need to remove a well-formed fusion mass. So, a direct decompression with transoral odontoidectomy was the preferred method.
All AADs are reducible, provided the C1-C2 joint can be opened up and manipulated.1,12 In scenario 3, an offending os odontoideum ossicle was stuck between the arch of C1 and C2, making reduction of the joint impossible. A complete posterior approach in this condition may not completely reduce the AAD and a sufficient decompression cannot be achieved. Hence, a staged procedure was performed with satisfying results.
Irreducible odontoid fractures with gross displacement is a contraindication for odontoid screw osteosynthesis and an indication for C1-C2 fusion.13,14 Anterior odontoid screw osteosynthesis is possible even in irreducible odontoid fractures with a preserved TAL and a C1-C2 joint complex, in which the fragment can be reduced by open surgical method via transoral approach. The advantage of osteosynthesis is to maintain the rotation of neck, especially in a young active person as in scenario 4. In the last scenario, an intraoperative decision of anterior odontoidectomy was made owing to the failed reduction of AAD. The vertical orientation of the C1-C2 joint complex prevents the atlas from reducing over the axis in the translational plane. In such situations, re-creation of the C1-C2 joint by osteotomization will help in reduction but may fail significantly when joints are completely vertically aligned, limiting the osteotomy. In such cases the decision of anterior transoral odontoidectomy for decompression can be taken intraoperatively based on the degree of reduction.
Goel et al12 postulated that with the C1-C2 joint manipulation technique, all AAD initially considered to be irreducible would become reducible, and the transoral odontoidectomy gradually faded away. However, the literature and most spine surgeons still believe that the anterior approach is not an obsolete procedure. Xu et al15 proposed a new clinical classification system for reducibility in AAD based on preoperative traction and transoral reducibility. They postulated that all AADs can be divided into reducible, irreducible, and fixed subtypes. They had 2 patients with fixed AAD in their case series who were treated by transoral atlas and odontoid excision along with “transoral atlanto axial reduction plate” fixation.15 Subin et al1 achieved reduction of the fixed AAD subtypes through transoral surgery by removing the callus, scar, and granulation tissue between the joint surfaces with excision of cartilage and eventual fusion without posterior fixation by traction alone.
Goel et al12 reported on the irreducible AADs caused by traumatic and congenital etiologies but intervened in all the irreducible subtypes through the posterior approach with intraoperative traction and joint manipulation. They also placed a spacer into the C1-C2 joint with a lateral pillar plate and screw fixation that helped in reduction of AADs. In our series, 3 patients had irreducible AADs secondary to iatrogenic posterior fusion; in such cases, the posterior approach is not only difficult but also dangerous owing to high chances of vascular and dural injuries. When fusion has already been achieved and removing the fused mass would not be an ideal situation, odontoidectomy is the method of choice for decompression of spinal cord with fewer complications.
Odontoid fractures with more than a 6-mm displacement require surgery for solid bone fusion, and the chances of nonunion are high if not dealt with appropriately. The fracture has to be reduced to anatomical position for fusion, and this is usually by preoperative traction. Irreducible fractures are relative contraindications for anterior odontoid screw fixation. These cases require posterior C1-C2 fusion for better results, considering the impending risk of AAI.16 Several methods of reduction maneuvers in irreducible odontoid fractures are described in the literature. The type of maneuver depends on the nature of the fracture, direction of displaced fragment, and chances of closed peroral manipulation of the fragment.17–19 Similar to this, our patient with irreducible and anteriorly displaced odontoid fracture had a preoperative traction up to 10 kg and it failed. We did not increase the weight owing to potential neurological damage. Intraoperatively, peroral closed manipulation of fragment also failed because the fragment was hitching against the C1 arch. Hence, peroral open reduction of the fragment was performed with good reduction.
In the last scenario, the posterior approach failed in reducing the odontoid fragment owing to the limitation in conversion of a vertically oriented facet to a horizontally orientated one. Elbadrawi et al11 performed a posterior procedure first, followed by anterior odontoid surgery, in their patients (9/20) to stabilize the atlantoaxial joint. The etiologies involved in their study were 3 cases of odontoid nonunion, 3 cases of infection, 2 cases of neoplasm, and 1 case of os odontoideum.11
The major setback in the anterior approach is working under depth with complex anatomical structures surrounding the odontoid and complications such as wound infections, wound dehiscence, and cerebrospinal fluid leak, which has been reported in earlier literature.19 In our study, these complications were not encountered due to adequate and meticulous preoperative care and wound closure. However, we had 1 patient with poor respiratory reserve who underwent postoperative tracheostomy, required ventilator support, and finally expired. Requirement for tracheostomy following a transoral approach is high at about 10.8%, and 3.4% in a transnasal approach (less tracheal edema, allowing early extubation). The percentage of patients developing mortality after 30 days is 2.9%, dysphagia is 3.8%, and velopharyngeal insufficiency is 3.3%. These complications of transoral odontoidectomy can be avoided by the transnasal approach,20 but we preferred the transoral route in all, because we gently retracted the uvula with a rubber catheter rather than splitting it up and none developed these complications.
Apart from taking biopsies and tumor excision, the transoral approach for AAIs is rarely done these days. Our series enlists the indications for using the transoral approach even in current scenarios, and we strongly defend it from being forgotten by the new generation of spine surgeons. The confidence of spine surgeons increases when they understand the complex anatomy of the atlantoaxial joint and experience these complex surgeries that also add to their surgical armamentarium. We also recommend the aforementioned conditions as indications for transoral anterior odontoid surgeries in atlantoaxial pathologies.
Footnotes
Disclosures and COI: The authors have received no funding for this study and report no conflicts of interest.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2020 ISASS.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.