


Abstract
Background Successful implementation of endoscopic spinal surgery programs hinges on reliable performance and case cost similar to traditional decompression surgeries of the lumbar spine.
Materials and Methods To improve the statistical power of studying the durability of endoscopes with routine lumbar endoscopy, the authors performed a retrospective survey study among endoscopic spine surgeons by email and chat groups on social media networks WhatsApp and WeChat. Descriptive and correlative statistics were done on the surgeon’s responses recorded in multiple-choice questions. Surgeons were asked about their clinical experience with spinal endoscopy, training background, the types of lumbar endoscopic decompression they perform by approach, their preferred decompression instruments, and their experience with endoscopic equipment failure.
Results A total of 485 surgeons responded, of whom 85 submitted a valid survey recording, rendering a completion rate of 27.1%. These 85 respondents reported a case volume of 12,650 lumbar endoscopies within the past year and, to date, had performed a total of 120,150 spinal endoscopies over their collective career years. The majority of respondents performed endoscopic surgery for herniated disc (65.9%) vs spinal stenosis (34.1%) in a hospital setting, preferentially employing the transforaminal (76.5%), interlaminar (51.8%), and unilateral biportal endoscopic (UBE; 15.3%) approach technique. The most commonly used endoscopic spine systems were Wolf/Riwo Spine (38.8%), Joimax (36.5%), Storz (24.7%), unspecified Chinese brand (22.4%), Maxmore (15.3%), Spinendos (12.9%), Elliquence (10.6%), unspecified Korean brand (7.1%), and asap Endosystems GmbH (2.4%). The most frequent failure mode of the endoscope reported by survey respondents was a blurry image (71.8%), followed by the loss of focus (21.2%), the loss of illumination of the surgical site (18.8%), and the failure of the irrigation/suction system integrated into the endoscope (4.7%). Most respondents thought they had problems with the lens (67.1%), the fiberglass light conductor (23.5%), the prism (16.5%), or the rod system (4.7%). Motorized high-speed power burrs and hand reamers and trephines were the reported favorite decompression tools that were presumably associated with the endoscope’s failure. The majority of respondents (49.5%) performed up to 50 endoscopies before the endoscope had to be either exchanged or repaired. Another 15.3% of respondents reported their endoscope lasted between 101 and 200 cases and only 12.9% reported more than 300 cases. Besides abuse during surgery (25.9%), bad handling by staff was the most common suspected reason (45.9%), followed by the wrong sterilization technique (21.2%). Some 23.5% of respondents noted that the endoscope failed during their surgery. In that case, 66.3% asked for a replacement endoscope, and 36.1% completed the surgery with the broken endoscope. However, 10.8% stopped and another 6% of respondents woke the patient up and rescheduled the surgery to complete the decompression at another time.
Conclusions Spinal endoscopes used during routine lumbar decompression surgeries for herniated disc and spinal stenosis have an estimated life cycle between 50 and 100 surgeries. Abusive use by surgeons, mishandling by staff, and deviation for prescribed cleaning and sterilization protocols may substantially shorten the life cycle. Contingency protocols should be in place to readily replace a broken spinal endoscope during surgery. More comprehensive implementation of endoscopic spine surgery techniques will hinge on technology advancements to make these hightech surgical instruments more resistant to the stress of daily use and abuse of expanded clinical indications’ for surgery. The regulatory burden on endoscope makers is likely to increase, calling for increased reimbursement for facilities to cover the added expense for capital equipment purchase, disposables, and the endoscopic spine surgery program’s maintenance.
Level of Evidence 3.
Clinical Relevance End user surgeon survey study.
INTRODUCTION
Many more spine surgeons graduating from postgraduate training programs in orthopedic spine or neurosurgery incorporate spinal endoscopy into their developing practice.1–3 In part, this is because of patient demand, their personal interest, the appeal of innovation in spine care in general, and last but not least, a reflection of an attempt to deliver more targeted and individualized spine care at a lower cost to patients who are looking for less burdensome treatments for common painful conditions of the lumbar spine that are also less disruptive to their lives.4 Early return to work, recovery, and healing times are significant concerns to patients and their employers,5–8 as corroborated by a recent analysis.6 With endoscopy of the spine likely being here to stay,9 the increase in case volumes leads to a better understanding of this modern technology’s preferred clinical application scenarios10 and its associated clinical outcomes, as well as a better understanding of its shortcomings.1,11 Sophisticated complex optical systems inherent to most modern endoscopes are manufactured by renowned vendors whose success in the marketplace depends on availability, quality, durability, and prompt support in the field should something go wrong with the endoscopic instrumentation.12
The perioperative performance parameters of any endoscopic spinal surgery program depend on many moving parts, including well-trained and trustworthy staff with dependable knowledge of the cleaning and sterile processing procedures while employing careful handling of these sensitive optical instruments through a well-established and uninterrupted chain of custody. Moreover, appropriate intraoperative applications of the endoscopes by surgeons, who may not always understand the characteristics of a rigid rod-lens system design of modern spinal endoscopes and their performance limits as they attempt to expand clinical indications of the procedure by trying more complex spinal decompression13 and increasingly fusion14–19 operations, are of utmost importance. Finally, high-quality products, including spinal endoscopes, are the cornerstone of reliability in the clinical outcomes with the endoscopic procedure.
Manufacturers list expected operational cycles in their respective instructions for use materials, which for many vendors range from 150 to 250 cycles when employing their recommended intraoperative applications, cleaning, and sterilization procedures. Since manufacturers cannot predict actual use and abuse characteristics by the end user, real performance cycles may be substantially lower. Anecdotally, many surgeons report much lower operational life cycle numbers. The gap between manufacturer-recommended clinical applications of their endoscopes and surgeon requirements for more complex clinical applications in expanded surgical indication scenarios may be widening. It could negatively impact further implementation and acceptance among surgeons, mainly when higher case numbers expose the shortcomings of the technology and the associated additional expense of capital equipment purchases, disposables, and the ongoing costs of maintaining an endoscopic spine surgery program. This higher per-case cost typically creates more pushback by hospitals and surgery centers, where endoscopic spine surgery still competes with the lower cost of the widely practiced traditional open, miniopen, and other forms of minimally invasive spinal surgery (MIS) procedures. Replacing these traditional spine surgeries with endoscopic techniques is not monolithically dependent on reimbursement. It also depends on the affordability of the technology when rolled out to the majority of patients in the context of their payer base. The key to avoiding these potentially competing agendas between the upsides of innovative technology and higher cost is a reliably performing equipment base.
The purpose of this study was to provide an illustrative analysis of the performance and clinical use characteristic by the surgeon end user of widely used spinal endoscopes to aid in the development of best clinical practice protocols in surgery and sterile processing. Ultimately, the authors were interested in providing the aspiring endoscopic spine surgeon, participating hospitals and surgery centers, and vendors some real-life performance data to facilitate further implementation of spinal endoscopy. Innovative and cost-effective technology improvements are only feasible by illuminating both sides of the user-vendor equation as the surgical indications for the endoscopic surgery are expanding and advances in the clinical program demand better quality products with more reliable and durable endoscopes able to withstand the stresses of increased routine use and abuse in the operating room.
MATERIALS AND METHODS
For the purpose of this investigation, the authors solicited responses to an online survey (www.typeform.com), which was sent to more than 900 prospective respondent surgeons by email and via chat groups in social networks, including WhatsApp and WeChat. Surgeons were asked to answer a variety of demographic, operational, and clinical use questions regarding endoscopes during lumbar endoscopy by choosing responses from several multiple-choice questions. Responding spine surgeons were also provided with a free text box to add any information they thought was relevant. To improve survey completion rate and minimize the impact of geographic bias, the survey questions were written by the team of authors. The survey ran from September 9, 2020, to October 8, 2020. The authors were blinded as to the identity of the responding surgeon at all times. Upon completion of the survey, the responses were downloaded in an Excel file format and imported into IBM SPSS (version 27) statistical software package for further data analysis. Descriptive statistic measures were used to count responses and calculate the mean, range, and standard deviation as well as percentages. X 2 statistics was used to determine the strength of association between factors. Missing responses were included for accurate percentage calculation and are listed at the top of each data table. Wherever applicable, a P value of 0.05 or less was considered statistically significant, and a confidence interval of 95% was employed for all statistical tests.
RESULTS
A total of 485 spine surgeons accessed the online survey on the typeform.com website. Eighty-five submitted a valid survey recording. Thus the completion rate was 27.1%. The demographics of the responding surgeons are shown in Figures 1 and 2. The majority of respondents were residing in Brazil (34.1%), South Korea (18.8%), and China (14.1%). The remaining respondents, in descending order, were from India (12.9%), Thailand (3.5%), Colombia (2.4%), Ukraine (2.4%), the United States (2.4%), and other countries (9.4%).
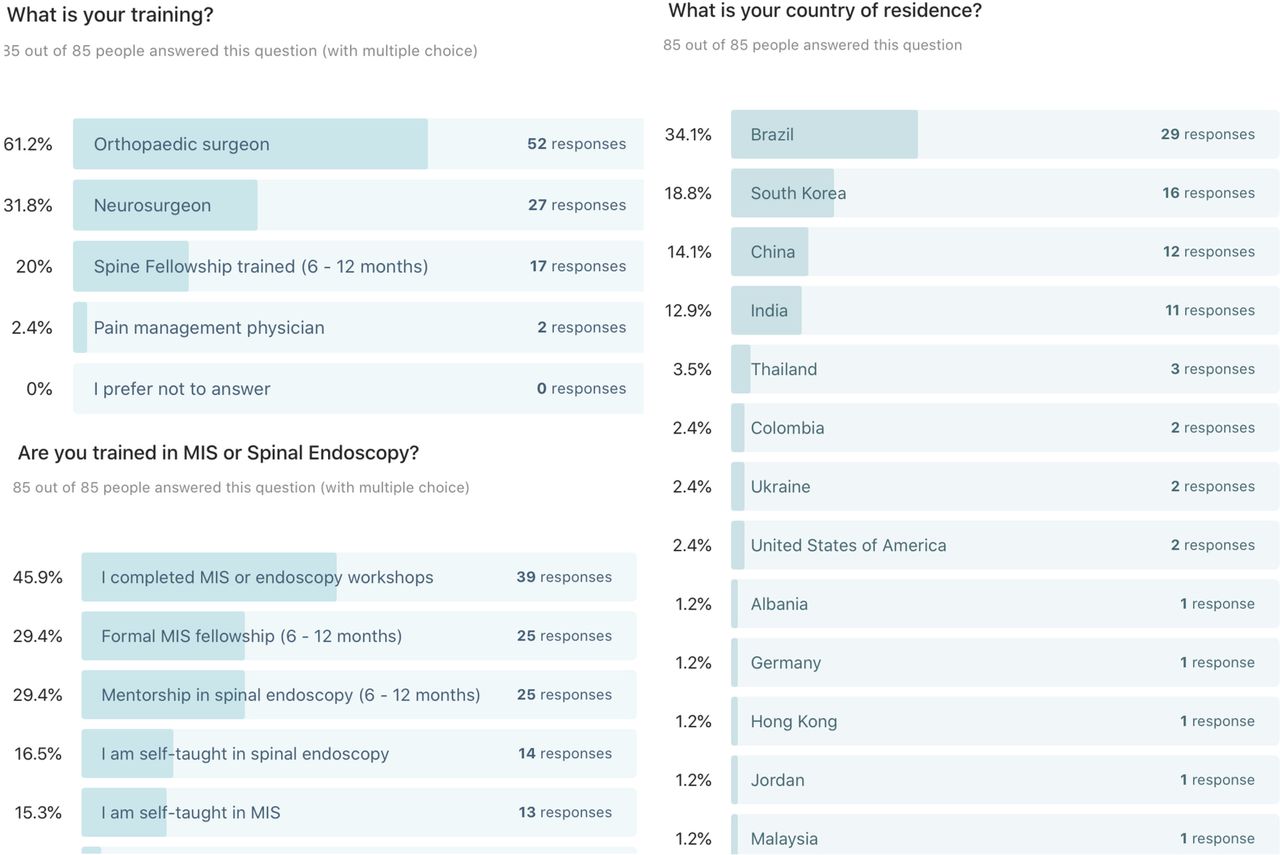
The percentage breakdown of responses to survey questions on endoscope durability with multiple possible answers on training background and country of residence given by the 85 participating spine surgeons is shown. The majority of respondents were orthopedic surgeons (61.2%) who received their spinal endoscopy training in short workshops (45.9%) or formal 6–12 months mentorship programs (29.4%). The minority (29.4%) had formal 6–12 months of postgraduate fellowship training in minimally invasive surgery (MIS). Multiple responses to the MIS/Endoscopy training question were allowed.
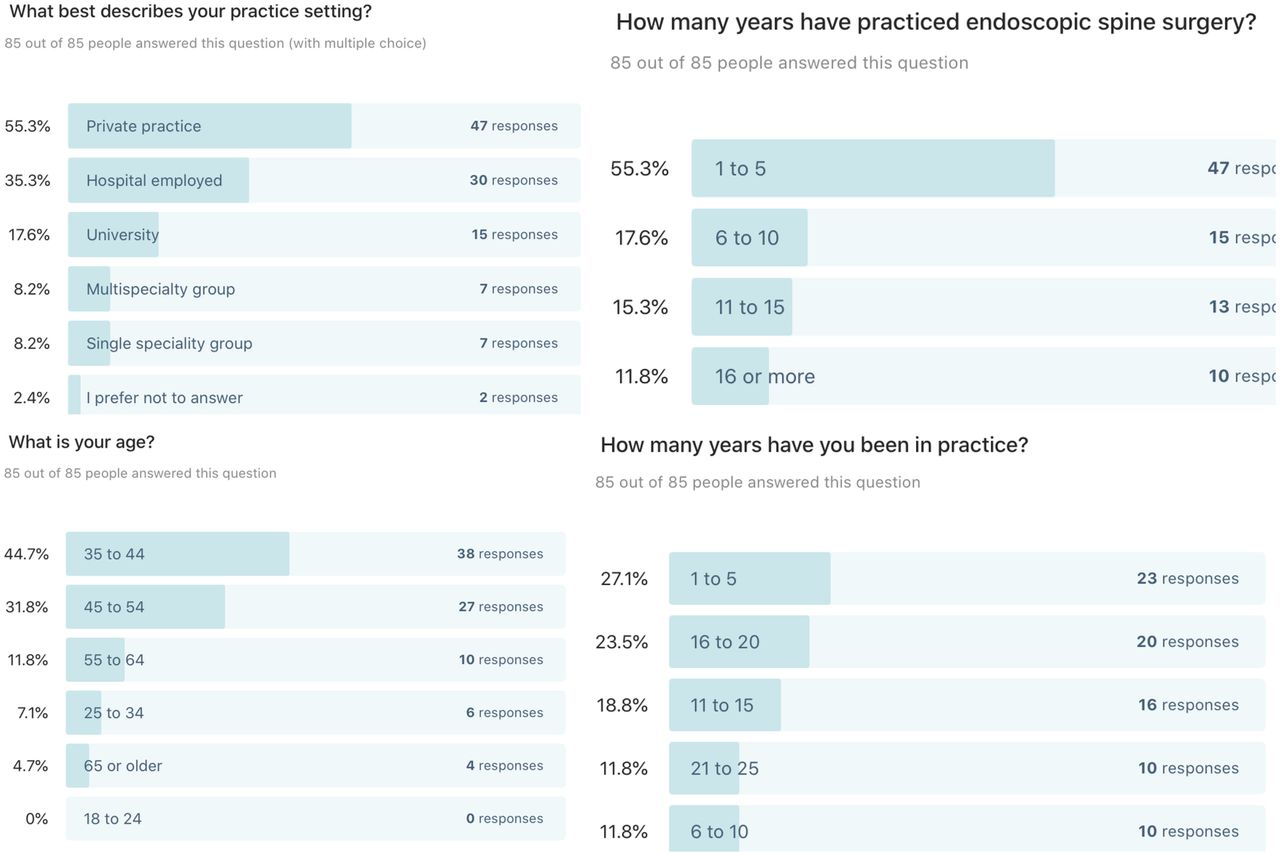
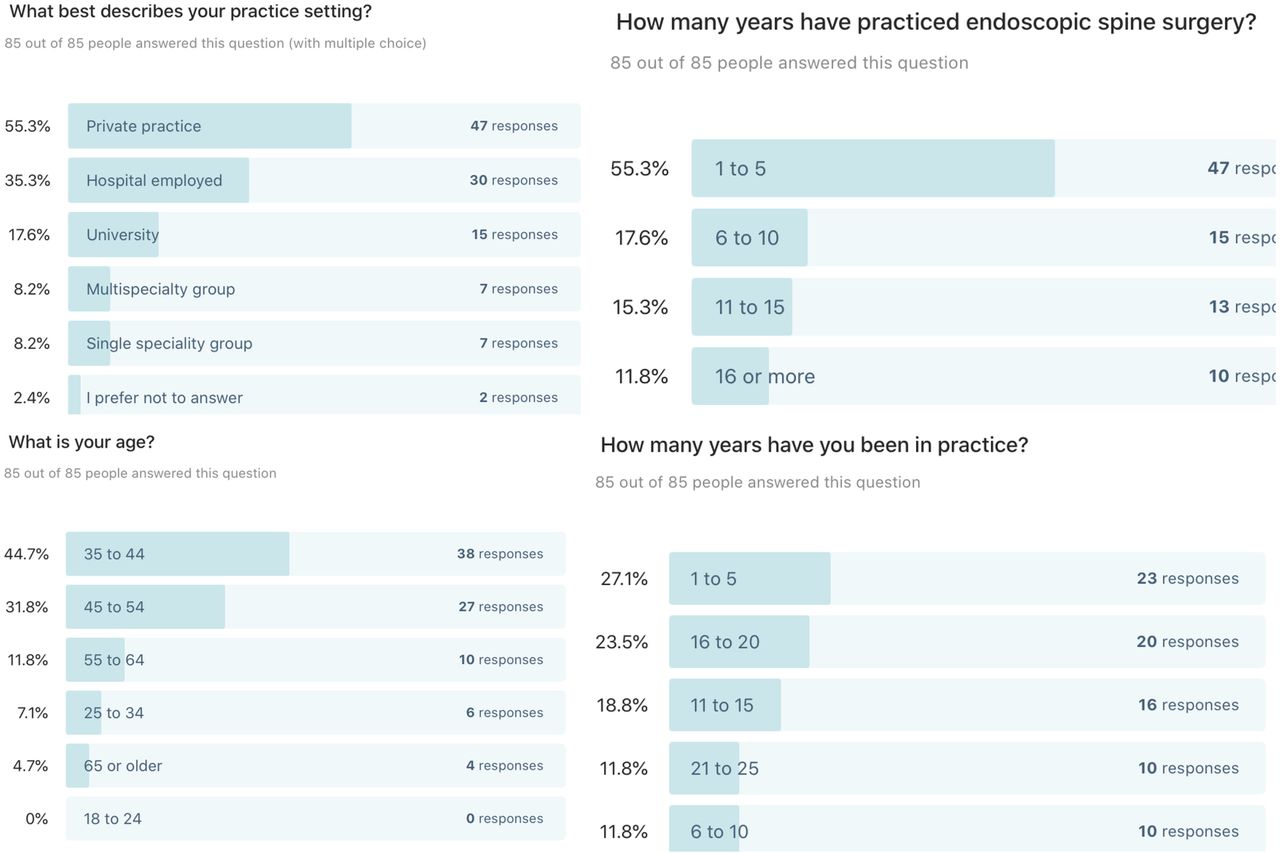
The percentage breakdown of responses to survey questions on endoscope durability with multiple possible answers on practice, age, years of practice, and years of performing endoscopic spine surgery given by the 85 participating spine surgeons is shown. The majority of respondents were in private practice (55.3%) and aged between 35 and 54 years (76.5%). The minority (27.1%) were in practice for 5 years or less. However, most respondents (55.3%) had 5 years or less of clinical experience with the spinal endoscopy procedure.
Of the 85 respondents, 31.8% indicated that they were neurosurgeons, 61.2% designated that they were orthopedic surgeons, and 2 respondents were pain management physicians (2.4%). The survey captured only male surgeons. The majority of respondents were between 35 and 44 years of age (44.7%) and 45 and 54 years of age (31.8%). Regarding additional training, 45.9% of respondents indicated that they completed a dedicated MIS or endoscopy workshop and used it as their primary spinal endoscopy training resource (Figure 2). Another 29.4% completed a formal 6 to 12 months MIS spine fellowship, while 29.4% of respondents had been able to find a mentor as a training resource. Fourteen of the 85 responding spine surgeons (16.5%) were self-taught in endoscopic spine surgery, and another 15.3% were self-taught in MIS spine surgery.
When asked about their practice setting, 55.3% of respondents indicated that they were in private practice. Another 17.4% worked in a university setting, and 35.3% were hospital employed. Regarding work experience, 27.1% of respondents indicated they had been in practice for 1 to 5 years. Another 23.5% of respondents indicated 16 to 20 years of postgraduate clinical experience. As an approximate measure of proficiency in endoscopic spine surgeons, the authors found that more than half (55.3%) of respondents only had been performing endoscopic spinal surgery for 1 to 5 years, followed by smaller groups of spine surgeons who indicated that their experience ranged from 16 to 20 years (23.5%), 11 to 15 years (18.8%), and 21 to 25 years (11.8%). Only the remaining 22.6% of respondents had professional experience with spinal endoscopy more than 10 years, and only 10.8% (10/85) of 16 years. Therefore, 45.7% of respondents had significant experience (over 6 years) in endoscopic spine surgery. Most respondents worked in an organization with 1 to 5 additional spine surgeons (Figure 3).
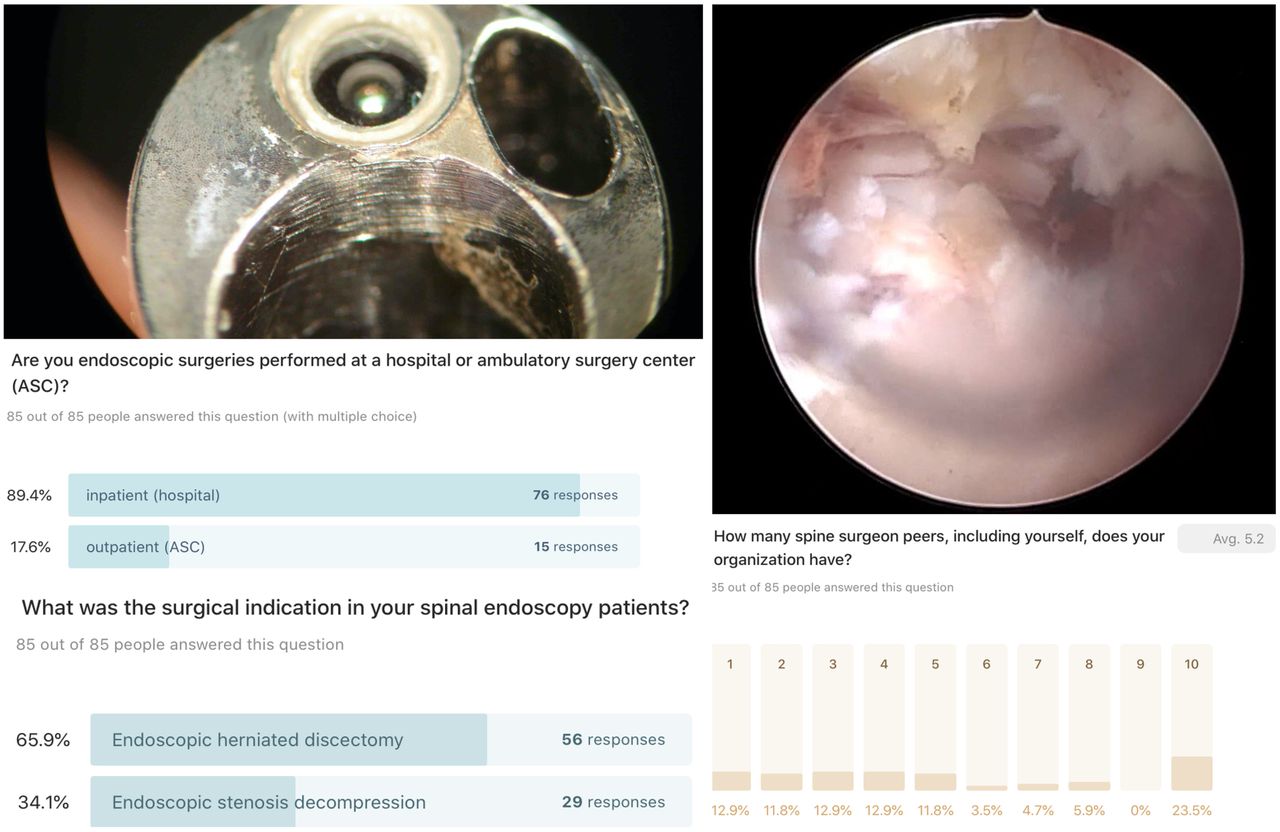
Damage to the endoscope’s lens and working channel with mechanical burrs or drills (left top panel) resulting in blurry vision (top right panel) was a common intraoperative failure mode reported by many participating survey surgeons, who performed 89.4% of lumbar endoscopic decompression surgeries in a hospital. The surgical indication was herniated disc in 65.9% and spinal stenosis in the remaining 34.1% of operations in which respondents employed endoscopic decompression techniques. Only 23.5% of respondents worked in an organization with 10 or more spine surgeons. Most respondents (62.3%) were in smaller practice settings, with 5 or fewer peer spine surgeons. Multiple responses to these questions were allowed.
Endoscopic spine surgeons reported a case volume of 12,650 lumbar endoscopies within the last year. Over their collective career years, they performed a total of 120 150 spinal endoscopies to date. Most respondents (89.5%) performed their surgeries in a hospital setting (Figure 3). Only 17.6% performed their surgeries in an outpatient ambulatory surgery center (ASC). The majority of respondents performed endoscopic surgery for herniated disc (65.9%) vs spinal stenosis (34.1%). About a quarter (25.9%) of respondents were significantly concerned with their endoscopic spine system’s ability to withstand the abuse during the contemplated endoscopic operation (Figure 3, top two panels). The most commonly employed endoscopic approach was posterolateral (50.6%), followed by interlaminar (31.8%) and unilateral biportal (UBE; 12.9%). The same group of respondents admitted to concomitant use of the various endoscopy techniques: transforaminal (76.5%), interlaminar (51.8%), and UBE (15.3%). In decreasing order, the most commonly used endoscopic spine systems were Wolf/Riwo Spine (38.8%), Joimax (36.5%), Storz (24.7%), unspecified Chinese brand (22.4%), Maxmore (15.3%), Spinendos (12.9%), Elliquence (10.6%), anonymous Korean brand (7.1%), and asap Endosystems GmbH (2.4%) (Figure 4). An illustrative case of the consequence of a spinal endoscope’s intraoperative failure used during a spinal stenosis decompression is shown in Figure 5.

Only 25.9% of respondents were somewhat or very concerned with the possibility of the spinal endoscope breaking during surgery and considered alternate decompression procedures. Failure of spinal endoscopes was reported to be more likely during posterolateral (50.6%) as opposed to interlaminar (31.8%) or unilateral biportal endoscopic (UBE) (12.9%) surgery. The majority (76.5%) of respondents preferred transforaminal over interlaminar (51.8%), or UBE (15.3%). The vendor breakdown in decreasing order revealed respondents preferably used equipment made by Wolf/Riwo Spine™ (38.8%), Joimax™ (36.5%), Storz™ (24.7%), an unspecified Chinese brand (22.4%), Maxmore™/ InnoView GmbH (15.3%), Spinendos™ (12.9%), Elliquence™ (10.6%), an unspecified Korean brand (7.1%), asap endoscopic products GmbH (2.4%), and other unidentified vendors (2.4%). Multiple responses to these questions were allowed.

Shown are the axial (top left panel) and sagittal (top right panel) T2-weighted magnetic resonance imaging scans of a case of a 45-year-old woman who underwent transforaminal decompression for L4/5 spinal stenosis with a herniated disc. During the transforaminal decompression, the lens failed (bottom left panel), resulting in blurry vision (bottom right panel). An unidentified surgeon sent in this case example via the online survey tool exhibiting the broken endoscope (bottom left panel) and the resulting deterioration of endoscopic visualization of painful spinal pathology during a transforaminal decompression procedure.
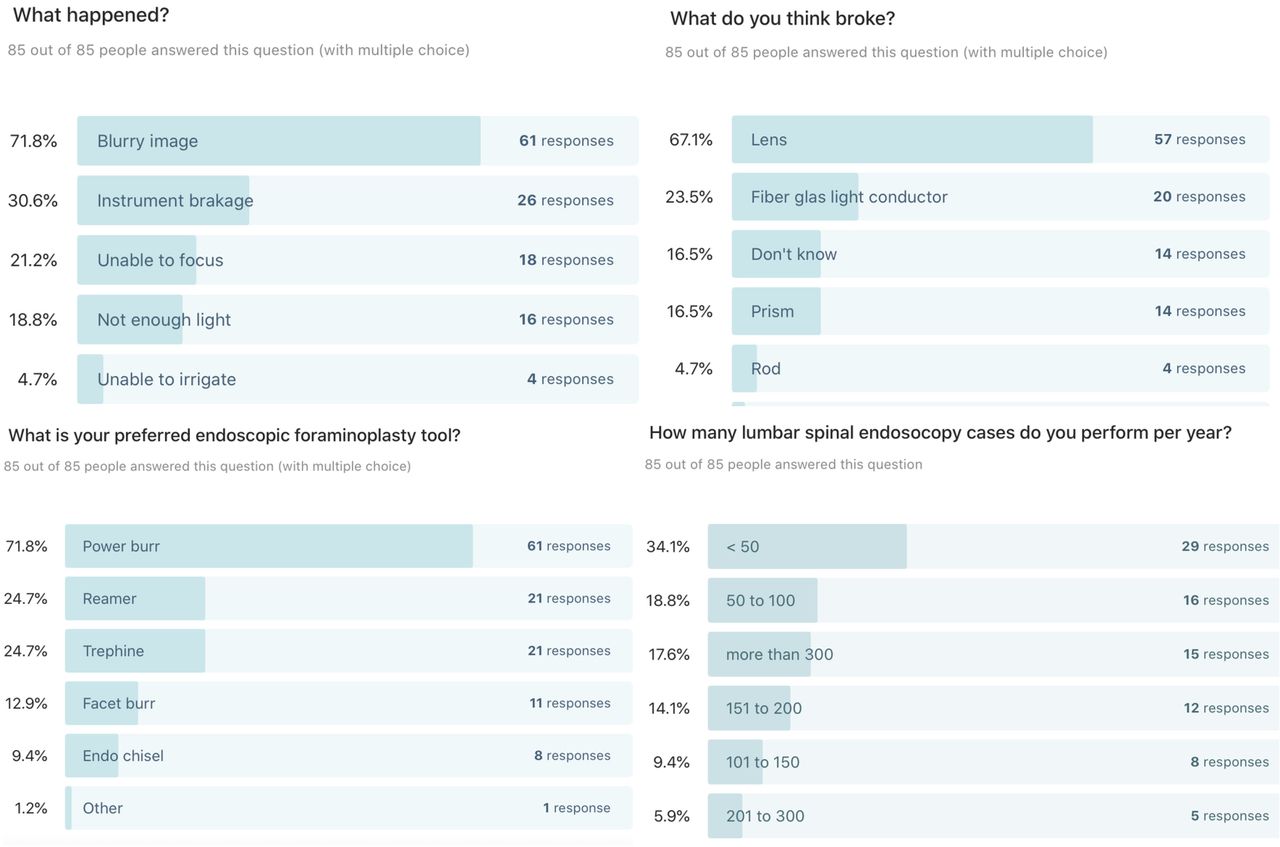
The most frequent failure mode of the endoscope was a blurry image (71.8%), followed by the loss of focus (21.2%), the loss of illumination of the surgical site (18.8%), and the failure of the irrigation/suction system integrated into the endoscope (4.7%). Concomitant instrument breakage was reported by 30.6% of respondents. In decreasing order, most surgeons thought they had problems with the lens (67.1%), the fiberglass light conductor (23.5%), the prism (16.5%), or the rod system (4.7%). However, 16.5% of respondents could not determine what went wrong with their endoscope during surgery (Figure 6). Their respective annual endoscopic caseload is also summarized in Figure 6, with 52.9% of respondents reportedly performing 100 surgeries or fewer per year. Motorized high-speed power burrs and hand reamers and trephines were the reported favorite decompression tools that were presumably associated with the endoscope’s failure, as described below.

Respondents indicated that the most commonly encountered problems with a spinal endoscope that failed during lumbar endoscopic decompression in decreasing order were blurry vision (71.8%), lack of optical focus (21.2%), and dim illumination (18.8%). Powered high-speed burrs were reported as the favorite decompression tools introduced through the endoscope’s inner working channel to accomplish decompression of the symptomatic neural elements (71.8% of respondents). Lens (67.1%) and light conductor (23.5%) failure were reported as the most commonly encountered problems. Multiple responses to these questions were allowed. More than half (52.9%) of respondents performed 100 or fewer cases per year concerning case volume. High-volume surgeons performed 150 or more endoscopic spine surgeries per year (37.6%).
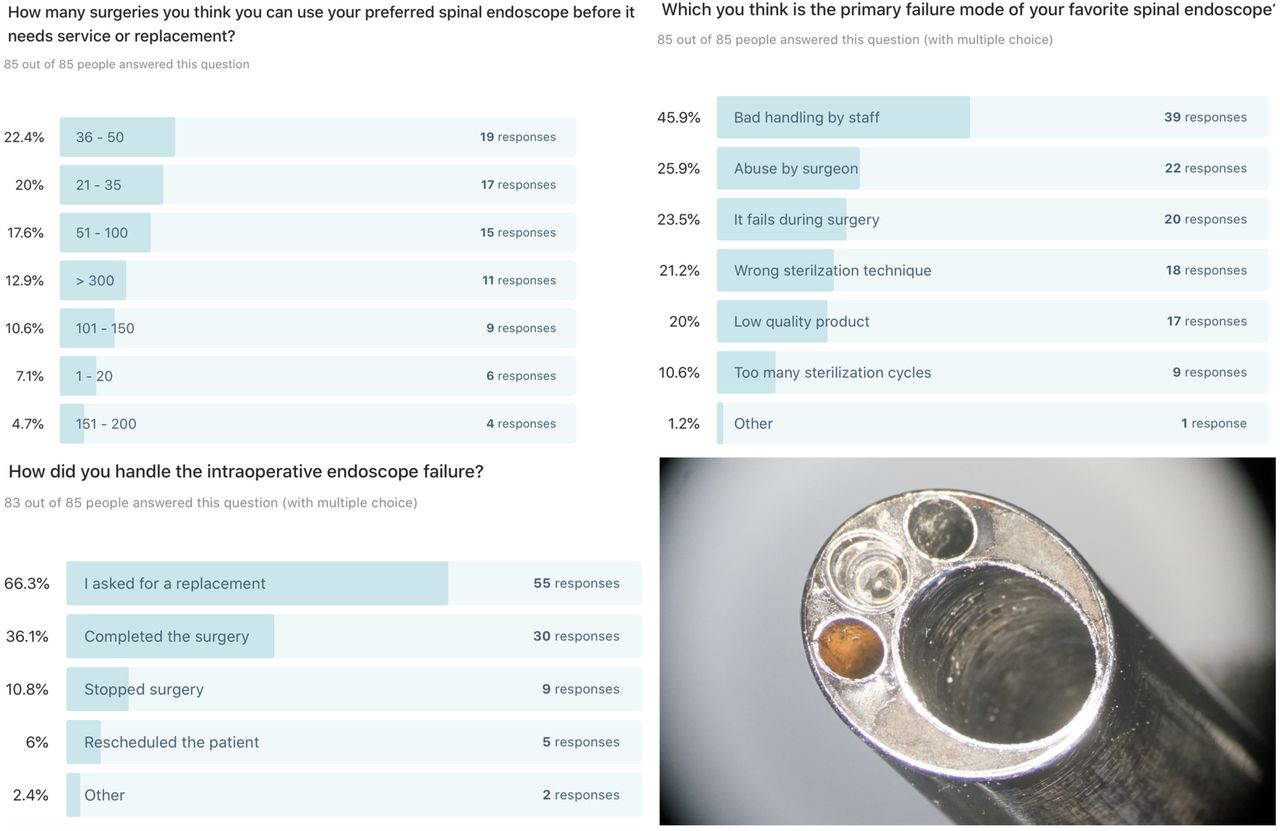
As far as the perceived durability of their preferred brand of spinal endoscopes, 49.5% of respondents reported that they were able to perform up to 50 endoscopies before the endoscope had to be either exchanged or repaired (Figure 7). Only 12.9% of resondents reported a possible caseload of over 300 endoscopic surgeries. Another 15.3% of repondents reported their endoscope lasted between 101 and 200 cases. However, 7.1% said that it endured fewer than 20 surgeries suggesting a significant variation in product quality and usage-related abuse by the surgeon and the staff at their respective surgical facilities. Surgeons suspected bad handling by staff was the most common reason (45.9%) why their favorite endoscope underperformed and failed earlier than its projected life cycle. Abuse by the surgeon (25.9%) or the wrong sterilization technique (21.2%) was reported as another possible explanation for early failure. Remarkably, 20% of respondents thought they had a low-quality product in their hands. Even more remarkable, 23.5% of respondents noted that the endoscope failed during their surgery. In that case, 66.3% asked for a replacement endoscope, and 36.1% completed the surgery with the broken endoscope. However, 10.8% stopped, and another 6% of respondents woke the patient up and rescheduled the surgery to complete the decompression at another time. Some examples of endoscope failures are illustrated in Figures 8 and 9.
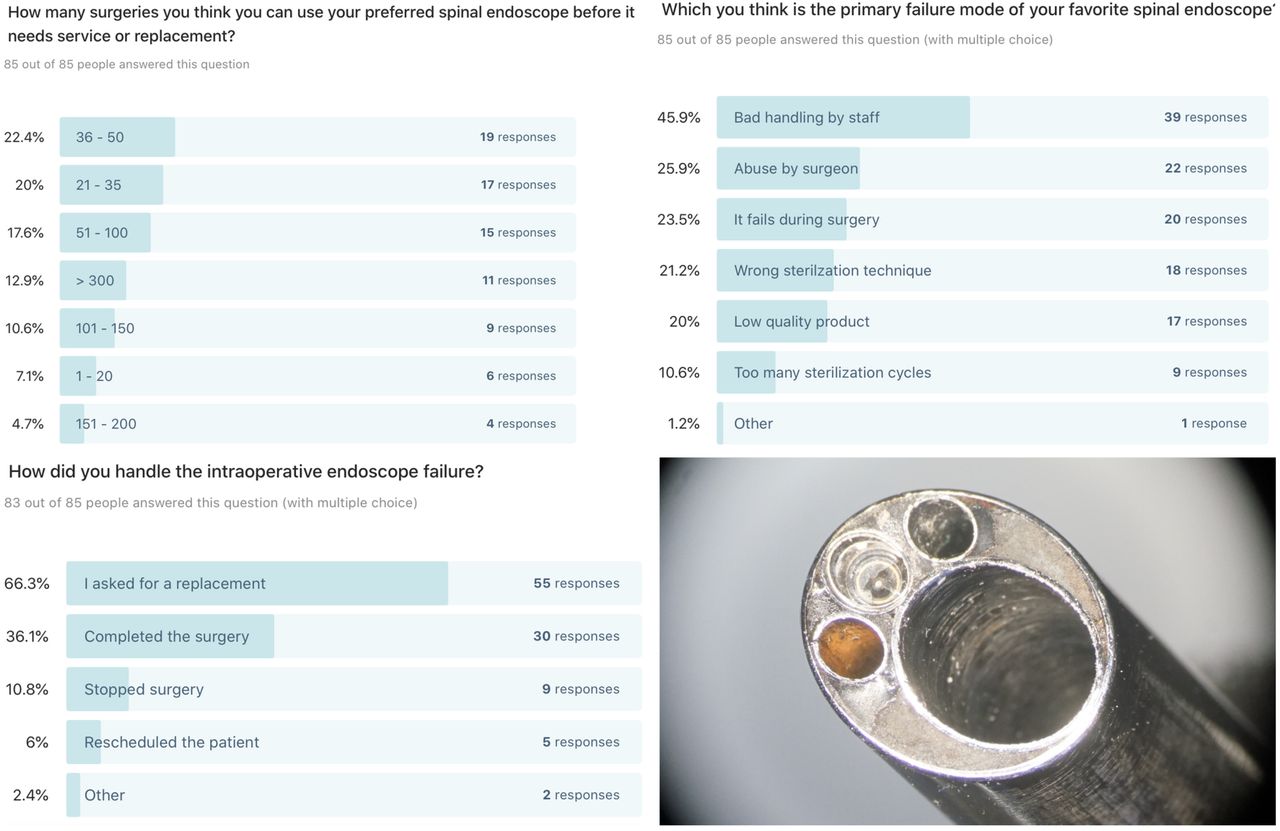
To the authors' surprise, only 28.4% of respondents reported that their preferred spinal endoscope ordinarily lasts for 100 or more lumbar decompression surgeries before it has to be replaced. Typically, instructions for use provided by manufacturers suggests that their endoscope should withstand 150 to 200 operation and sterilization cycles. Actual usage numbers reported by rrespondents were operational life cycles of 21 to 36 surgeries (20%), 36 to 50 surgeries (22.4%), or less than 20 surgeries (7.1%), suggesting a significant variation in product quality and usage-related abuse by the surgeon and the staff at their respective surgical facilities. Surgeons suspected bad handling by staff was the most common reason (45.9%) why their favorite endoscope underperformed and failed earlier than its projected life cycle. Abuse by the surgeon (25.9%) or the wrong sterilization technique (21.2%) was reported as another possible explanation for early failure. Remarkably, 20% of respondents thought they had a low-quality product in their hands. Even more remarkable, 23.5% of respondents noted that the endoscope failed during their surgery, highlighting the need for backup equipment and contingency plans. The bottomright panel shows a microscopic view of a spinal endoscope whose manufacturer advertised superior quality related to the lens’s gold welding. Nevertheless, the lens detached from the endoscope had to be retrieved intraoperatively from the patient with a backup endoscope from a different manufacturer.

Illustrative examples of microscopic views provided by several vendors to responding survey surgeons who solicited estimates for repair on returns. Common usage-related problems include a scratched ocular (A), scratched working channel with tears (B), cracked lens (C), scratched and deformed outer tube (D), a cracked lens with a blurry view (E), and dented and torn inner working channel with perforations (F). In the latter example, the holes allow irrigation fluid to enter the tube housing the optical system.
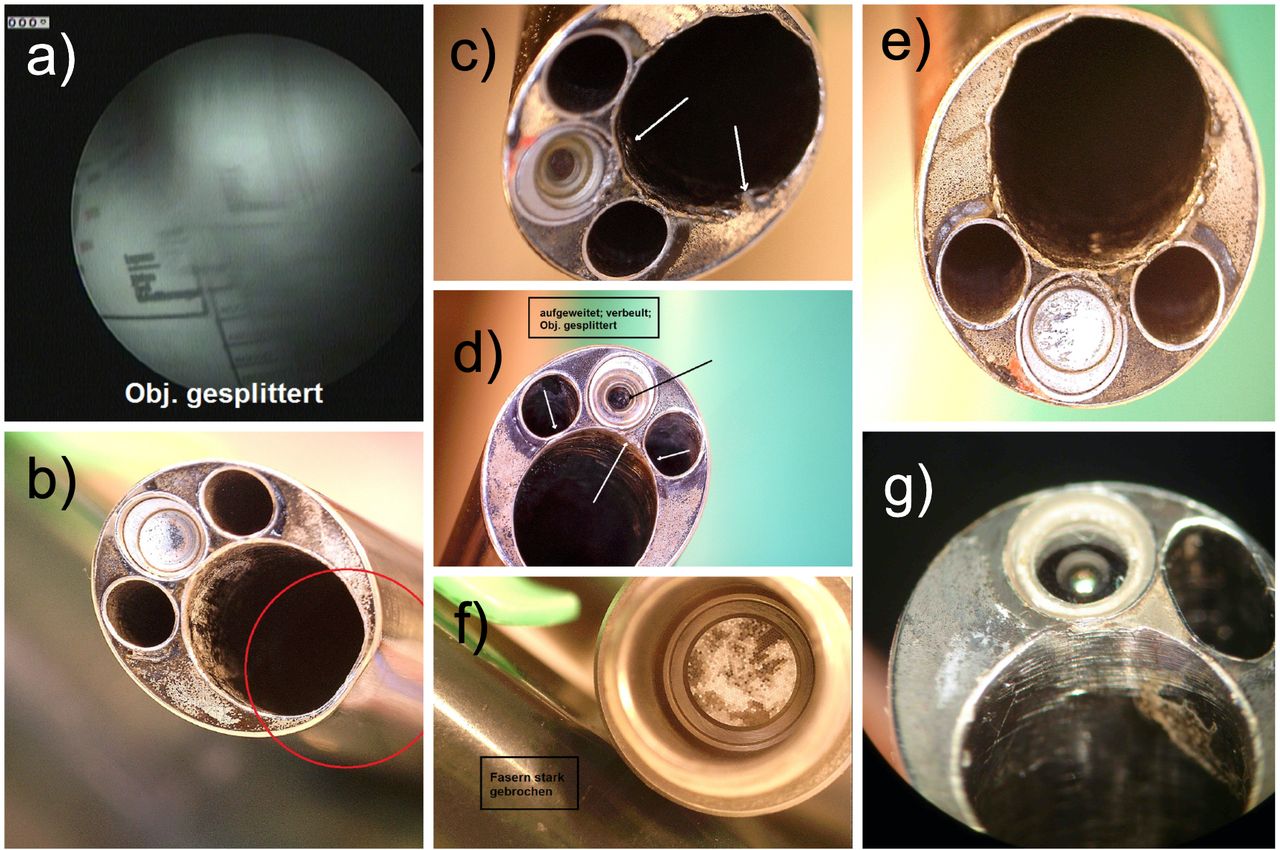
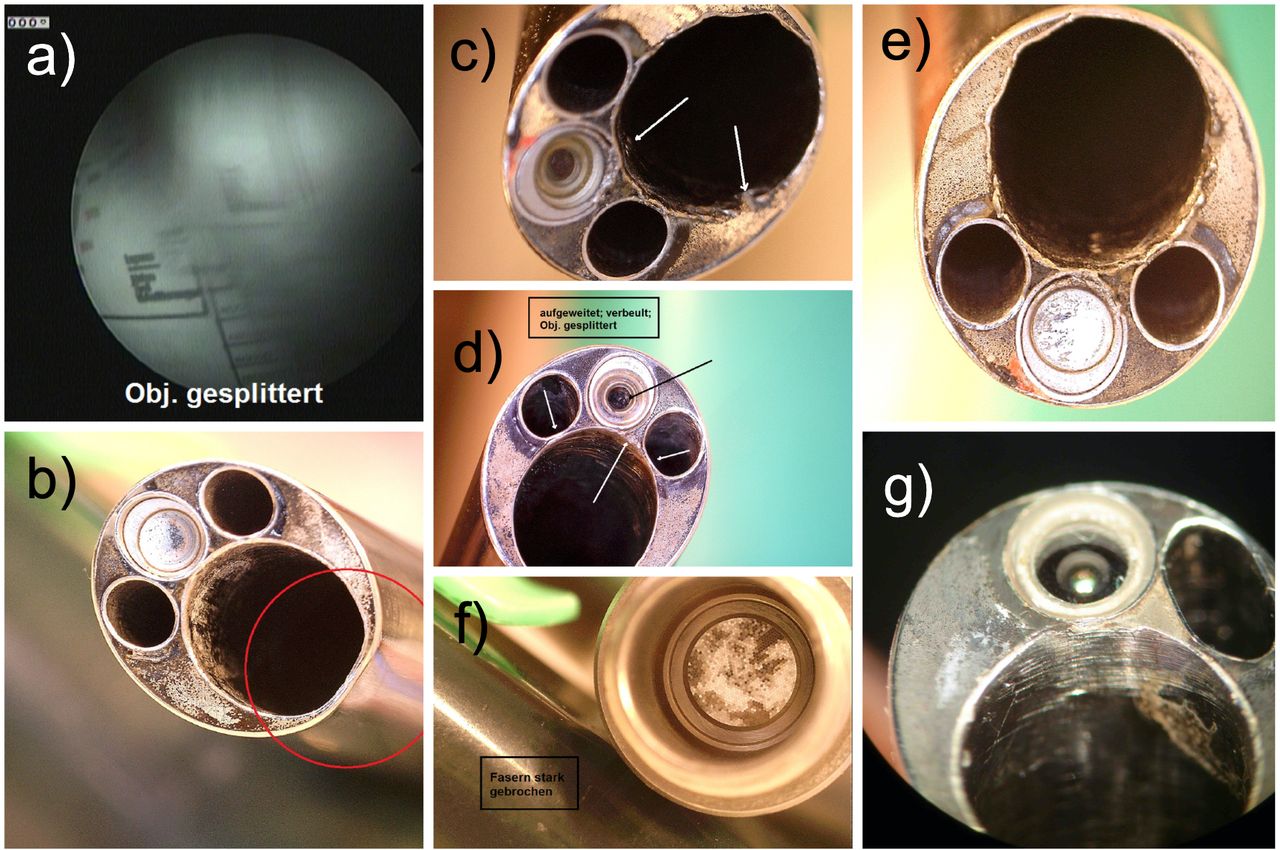
Additional illustrative examples of microscopic views provided by several vendors to responding survey surgeons who solicited estimates for repair on returns because of blurry or distorted vision (A). Other usage-related problems were dented outer tube (B), damage to the lens and working tube from inappropriate use of side-firing laser (C), a cracked lens with deformed working-, irrigation- and suction channels from the vibration of a high-speed power burr damaging epoxy sealing the working channel tube (D), deformation of the working tube from forceful use of hand reamers and chisels (E), a cracked lens from hammering (F), and destroyed distal working tube from high-speed power burr retracted into the working channel while still running (G).
Regardless of brand and usage, the mean number of endoscopic evaluations calculated from the point ranges surgeons reported that could be performedwith any given endoscope before it had to be replaced was 113 (SD 94.2). There was no statistically significant difference in the caseload between vendors under routine clinical use. Some slight variations in reported life cycles became apparent when calculating endoscopes’ percentages by a vendor with life cycles up to 100 and above 100 cases (Table). None of the subcategories, including “abuse by the surgeon,” “bad handling by staff,” or “low-quality product,” rose to a level of statistical significance. Therefore, the numbers breakdown is not presented herein. The crosstabulation between endoscope life cycles and the type of decompression tool employed by the surgeon (power burr, trephine, reamer, or endo-chisel) also did not show any statistically significant association, suggesting that not one single decompression technique is associated with higher failure rates of spinal endoscopes but that cumulative damage is more likely to be responsible for the ultimate failure event that every spinal endoscope will invariably reach.
Lifecycles of lumbar endoscopes by vendor under routine use for discectomy and stenosis surgery.
DISCUSSION
This retrospective study on a total of 120,150 lumbar endoscopies done by 85 surgeons in various private or academic, single- or multispecialty practice settings in 16 countries determined the estimated average life cycle of a spinal endoscope used in routine lumbar decompression surgeries for herniated disc or stenosis of the spinal canal is between 50 and 100 cases–less than half the number most manufacturers suggest in their instructions for use that the end user should reasonably expect if their product is used and processed according to their recommended guidelines for use, cleaning, and sterile processing. How can this stark difference be explained? The answer may perhaps be rather obvious. The regulatory process mandated by the respective agencies governing the mandatory self-certification marks required on many types of products to enter the Common (EU) European market (CE Mark), the United States market requiring approval by the Food and Drug Administration (FDA), or the China CCC Certification, China Customs, or India BIS Certification just to name a few, dictate the testing conditions. The life cycle numbers listed in endoscope manufacturers instructions for use are based on a benchtop in vitro testing scenarios which do not account for the human factor. Both surgeon use and improper handling by staff may contribute to lower actual life cycle usage numbers. Why is this important? It is simple. The added cost per case of introducing the endoscopic equipment has to be taken into account when implementation of an endoscopic spine surgery program is being considered at a hospital or an ASC. This notion was of particular importance to spine surgeons from China, where spinal endoscopy rather than an operating microscope was introduced in many hospitals because of the latter’s higher capital purchase cost. The authors’ observations put things in a very different light, though, considering that the average spinal endoscope lasts only 100 cycles. At an average capital purchase price of $10 000 for a spinal endoscope in China, the added case cost for purchasing and maintaining a spinal endoscopy program would be $100.
While clinical benefits have been demonstrated with the lumbar endoscopic decompression procedure in numerous peer-reviewed articles,11,20–41 high implementation and maintenance cost remains of concern to most healthcare institutions as the downstream cost savings may not be realizable within the same organization. Spinal endoscopy is, in fact, competing to replace traditional open and other forms of MIS, which are being performed without the need for additional large upfront capital- and disposable equipment purchases. The pressure for cost savings in already overstretched healthcare systems is high in most countries, and new technology implementation is often weighted against its cost vs benefit. Many hurdles entirely unrelated to patients’ clinical benefits may exist and impede the transition to these more modern innovative endoscopic spinal surgery protocols. Similarly, the pressure on endoscopic equipment manufacturers and associated vendors, who struggle with the higher burden of new regulatory rules, is insurmountably high, thus getting in the way of implementing innovative business models with sustainable revenue cycles.
Recently, the CE Mark regulation has changed from the Europe Standard EN 60950–1 to EN 62368–1 under which all audio/video (A/V) and information, communication technology (ICT) equipment sold in Europe will have to comply with the new EN 62368–1 hazard-based standard by December of 2020. This also applies to all existing equipment currently CE marked under EN 60950–1. In 2017, the European Parliament passed legislation to transition the EU’s medical device directive (MDD) to the more rigorous medical device regulation (MDR). This move was prompted by the MDD’s notifying body’s lack of oversight of a French breast implant manufacturer who had substituted high-quality medical silicone gel with low-quality industrial silicone in its breast implants, causing several casualties. Lawsuits for different varieties of negligence were also settled. The MDD was revised and reissued as the MDR and significantly expanded the accountability for future legal damages to virtually all economic operators (eg, authorized representatives, importers, distributors, etc). These increased reporting requirements and accountability criteria have increased the scrutiny on risk assessment documentation, technical files, and quality-control processes raising production costs disproportionally higher for manufacturers of spinal endoscopes, who face the same cost of MDR implementation but operate in a small niche market plagued by inconsistent demand. This higher regulatory burden will likely stifle rapid technological innovation needed to advance clinical protocols as the cost for change is too high. The higher regulatory burden in Europe and North America could skew the playing field in other markets where lower-cost products may have an advantage. Complaints from manufacturers as of this article’s writing have halted complete MDR implementation in Europe, and the stakeholders continue to debate the way forward. Ultimately, this ongoing dynamic may play out in operating rooms worldwide considering most spinal endoscope manufacturers, including OEM makers, reside in Europe.
As with any new technology, formalized postgraduate training lags. This postgraduate training gap was also reflected in the responses given by participating surgeons regarding the endoscopic specialty training. While 29.4% completed a formal 6 to 12 months MIS spine fellowship, 45.9% of surgeons indicated that they received their spinal endoscopy training in a short weekend workshop. Another 29.4% had been able to find a mentor as a training resource. Nevertheless, a significant portion of responding spine surgeons (16.5%) were self-taught, which highlights the fact that many of the younger surgeons–44.7% of respondents were between the ages 35 and 44 years–have to figure out by themselves how to implement a spinal endoscopy surgery program and develop contingency plans for intraoperative failure of the spinal endoscopy system.
One of the most convincing findings of this study relates to the rising surgical case volume done with endoscopic minimally invasive techniques. Some 12,650 of the 120,150 captured by this team of authors were done within the past year. While the authors had no way of determining a trend, it was apparent that the case volume by younger surgeons coming online is substantially increasing, considering 10.5% of the entire case volume was done just within the past year (as of the date of terminating the survey). Transforaminal endoscopic decompression surgery was the favorite among spine surgeons, with 76.5% indicating that they employ it routinely. The interlaminar approach was employed by surgeons at a lower rate, with surgeons reporting that they used it in 51.8% of their cases. UBE was of low relevance in this study. Over half (55.3%) of the surgeons participating in this survey were less experienced with 5 or fewer years of clinical experience with the spinal endoscopy procedure. Although we could not establish a statistically proven correlation with the type of surgical approach, surgeon skill level, annual case numbers, use of motorized power instruments, bad handling by staff, and vendor, all of these factors likely play into the cumulative damage of spinal endoscopes that eventually fail. While the burden to improve resistance to frequent sterilization cycles is clearly on the manufacturing side, some surgeon-related failure modes stand out; for example, the endoscope tip is a regular site of damage to the lens, the fiberglass light carrier, the seal between all components. Retracting power burrs while still running against the lens will invariably destroy it. The uncontrolled use of side-firing lasers may have a similar effect. Some manufacturers have attempted to make the lens components more robust by gold welding it in place, but as shown in one case example (Figure 7), it may still fail. Nearly a quarter (23.5%) of responding spine surgeons had a spinal endoscope that failed during surgery. Some 66.3% had a replacement endoscope available and another 36.1% of surgeons were able to complete the surgery with the broken endoscope. However, 10.8% stopped and another 6% of surgeons woke the patient up and rescheduled the surgery to complete the decompression at another time, thus, highlighting the need for contingency plans for such endoscopic equipment failures illustrated in Figures 8 and 9.
Ultimately, this article is a plea to endoscopic spine surgeons and the makers of this hightech equipment alike to work collaboratively on practical solutions to the everyday problems reported herein. Hopefully, that will entail continued technology improvements. However, it also calls for improved training of surgeons and their staff on handling and processing, establishing well-controlled custody chains of the instrumentation while controlling implementation cost, and not inflating the case cost for lumbar decompression procedures. The reimbursement structure in the United States is currently in a reverse relationship to implementation cost. Spinal endoscopy costs more and reimburses less. Since 2016, there has been a current procedural terminology (CPT) code addition (62380) that provides a billing code for endoscopic decompression of the spinal cord or nerve roots at the lumbar level. However, the relative value units (RVU) proposed by the Centers for Medicare Services (CMS) in 2016 based on the intensity and an identical intraservice time was 9.09 with a final conversion factor in 2017 of $35.89 per RVU. The American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) recommended a work RVU of less than the 10.47 number based on a crosswalk to CPT code 47562 (Laparoscopy, surgical; cholecystectomy) since CMS at the time stipulated that CPT codes 62380 and 47562 are similar in intensity but that the work involved in furnishing CPT code 62380 was overestimated. The malpractice, facility expenses, and total facility RVU numbers were undiscoverable for 62,380 at the time of this article’s writing. In comparison, CMS recommended in 2018 a work RVU of 13.18, facility expense RVU of 10.95, malpractice RVU of 4.06, and total facility RVU of 28.19 for CPT code 63030 (laminotomy). For laminectomy (CPT code 63046), the respective 2018 RVU numbers were work RVU of 17.25, facility expense RVU of 12.90, malpractice RVU of 5.43, and total facility RVU of 35.58.42 This glance at the US reimbursement landscape highlights the importance of good stewardship with any endoscopic spine surgery program if it is to be rolled out across the board and not just to a few patients who can afford it.
Our retrospective survey study was plagued by the same bias limitations as any other retrospective and survey study. Our response rate of 27.1% is on par with previously reported online surveys. The average response rates for an in-person survey have been reported at 57%, mail survey at 50%, email survey at 30%, online survey at 29%, telephone survey at 18%, and in-app survey of 13%, rendering the overall average survey response rate of 33%.43–47 Responses were blinded, and the authors had no information about the identity of the responding spine surgeons limiting the impact of intuition and hindsight bias among the investigators.48 The effect of nonresponse bias due to the low response rate may improve survey accuracy and was of no concern to this team of authors since low response rates in the 20% range have been related to more accurate measurements than surveys with 60% to 70% response because the missing data are not random.49 Additional limitations may have arisen from geographic bias. The digital communication used in this survey study could have obliterated existing geographic diversity and various cultural perspectives of responding to spine surgeons. The authors assumed a negligible impact of geographic bias factors because statistical testing did not affect geographic or cultural factors in the collected data. Instead, the authors were cautious not to generalize this retrospective survey’s findings in the context of their preconceived notions of endoscopic instrumentation failure to counter the homogenizing effect of the digital data acquisition across multiple geographical and cultural boundaries. Hindsight and recall bias by the responding surgeons may have been the most relevant limitations of this study since the information presented herein was not based on a patient registry but was based on the surgeon’s ability to recall the specific details surrounding the intraoperative failure of the endoscope and resist the influence of clinical outcome knowledge, which are anchored in reconstructive memory (hindsight bias).48 The authors recognized that their personal experience with endoscope failure during routine lumbar endoscopy might have been different and acknowledged the genuinely alternative insights from other surgeons.
CONCLUSIONS
There are a few solid take-home points from this retrospective survey study among busy endoscopic spine surgeons. Spinal endoscopes used during routine lumbar decompression surgeries for herniated disc and spinal stenosis have an estimated life cycle between 50 and 100 surgeries. Abusive use by surgeons, mishandling by staff, and deviation from prescribed cleaning and sterilization protocols may substantially shorten the life cycle. Failure of the lens and fiberoptic light carrier are standard failure modes resulting in blurry vision or insufficient illumination and may catch the inexperienced endoscopic spine surgeon off guard. Contingency protocols should be in place to readily replace a broken spinal endoscope during surgery. More comprehensive implementation of endoscopic spine surgery techniques will hinge on technology advancements to make these hightech surgical instruments more resistant to the stress of daily use and abuse of expanded clinical indications’ surgery and to keep the cost per case on par with traditional open decompression surgeries. The regulatory burden on endoscope makers is likely to increase, calling for increased reimbursement for facilities to cover the added expense for capital equipment purchase, disposables, and the endoscopic spine surgery program’s maintenance.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Jorge Felipe Ramírez León is shareholder & President of Board of Directors Ortomac, Colombia, consultant Elliquence, USA. Anthoney Yeung designed and trademarked his inside-out YESS™ technique and receives royalties from the sale of his inventions; his indirect conflicts of interest (eg, honoraria, consultancies to sponsoring organizations) are donated to IITS.org, a 501 c 3 organization). The remaining authors have no relevant conflicts of interest or financial disclosures.
Center for Advanced Spine Care of Southern Arizona andSurgical Institute of Tucson, Tucson, AZ 85712, USA
Disclaimer This manuscript is not meant for or intended to endorse any products or push any other agenda other than the associated clinical outcomes with endoscopic spine surgery. The motive for compiling this clinically relevant information is by no means created and/or correlated to directly enrich anyone due to its publication. This publication was intended to substantiate contemporary endoscopic spinal surgery concepts to facilitate technology advancements.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2021 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.