


Abstract
Study Design A design-agnostic standardized effect meta-analysis of 48 randomized, prospective, and retrospective studies on clinical outcomes with spinal endoscopic and interspinous process spacer (IPS) surgery.
Objective The study aimed to provide reference set of Oswestry Disability Index (ODI) and visual analog scale (VAS) effect size data for back and leg pain following endoscopic and IPS decompression for lumbar herniated disc, foraminal, or lateral recess spinal stenosis.
Background Mechanical low back pain following endoscopic transforaminal decompression may be more reliably reduced by simultaneous posterior column stabilization with IPS.
Methods A systematic search of the PubMed, EMBASE, Web of Science, and the Cochrane Central Register of Controlled Trials from 1 January 2000 to 2 April 2020, identified 880 eligible endoscopy and 362 IPS studies varying in design and metrics. The authors compared calculated standardized effect sizes (Cohen’s d) for extracted ODI, VAS-back, and VAS-leg data.
Results The pooled standardized effect size combining the ODI, VAS-back, and VAS-leg data for the total sample of 19862 data sets from the 30 endoscopy and 18 IPS was 0.877 (95% CI = 0.857–0.898). When stratified by surgery, the combined effect sizes were 0.877 (95% CI = 0.849–0.905) for endoscopic decompression and 0.863 (95% CI = 0.796–0.930; P = 0.056) for IPS implantation. The ODI effect sizes calculated on 6462 samples with directly visualized endoscopic decompression were 0.917 (95% CI = 0.891–0.943) versus 0.798 (95% CI = 0.713–0.883; P < 0.001) with indirect IPS decompression (P < 0.001). The VAS-back effect sizes calculated on 3672 samples were 0.661 (95% CI = 0.585–0.738) for endoscopy and 0.784 (95% CI: 0.644–0.923; P = 0.187) for IPS. The VAS-leg effect sizes calculated on 7890 samples were 0.885 (95% CI = 0.852–0.917) for endoscopic decompression and 0.851 (95% CI = 0.767–0.935; P = 0.427).
Conclusion Lumbar IPS implantation produces larger reduction in low back pain than spinal endoscopy. On the basis of this meta-analysis, the combination of lumbar transforaminal endoscopy with simultaneous IPS has merits and should be formally investigated in higher grade clinical studies.
Clinical Relevance Meta-analysis on the added clinical benefit of combining lumbar endoscopic decompression with an interspinous process spacer.
Level of Evidence 2.
INTRODUCTION
Considering stabilization after endoscopic decompression of a severely degenerated lumbar spinal motion segment has been suggested to improve clinical outcomes with this still relatively new outpatient spine surgery.1–3 Spinal endoscopy is now increasingly performed for claudication symptoms in the elderly due to herniated disc and spinal stenosis.2,4–10 Degenerative disc disease is often associated with progressive loss of intervertebral height from vertical collapse, initially causing predominantly foraminal and lateral recess stenosis.11–15 In its end stage, degenerative disc disease is known to result in loss of its internal structural integrity, which is often corroborated by the presence of a vacuum phenomenon on radiographic studies.15,16 The structural equivalents of such radiographic vacuum discs were recently described as intradiscal fissuring, cavitation, and delamination from the end plate often found during routine inside-out endoscopic direct visualization of the lumbar disc space in over two-thirds of affected patients.17 Over time, additional instability-related problems may ensue due to altered facet joint biomechanics, eventually leading to its hypertrophy and hypertrophy of the ligamentum flavum compounding the stenosis problem.3,18,19 Overgrowth of the ligamentum flavum has been stipulated to be a direct result of anterolateral instability,20 thereby contributing to the late development of central stenosis in addition to foraminal or lateral recess stenosis often seen in the early stages of the disease.
Technological advancements in video endoscopic equipment and instruments afford the contemporary endoscopic spine surgeon the ability to tackle more complex problems, including those seen in patients with severe spinal stenosis. In experienced hands, good long-term outcomes can be achieved with both the inside-out21 and the outside-in1 transforaminal endoscopic decompression. Complication rates,22 readmission rates,23 reoperation rates, and conversion rates to open fusion surgery are substantially lower with the transforaminal endoscopic decompression surgery—particularly when expertly executed.24 While the overall 5-year durability of the transforaminal endoscopic decompression was demonstrated to be excellent without the need for open salvage decompression fusion surgery,1,21,25 the additional use of follow-up radiofrequency ablation and endoscopic foraminal decompression procedures may be deemed appropriate in up to one-third of lumbar endoscopy patients to manage contralateral or adjacent segment symptomatic stenosis and mechanical low back pain to maintain the treatment effect of the endoscopic index procedure.1,21,24 Effectively, the end result is a staged management approach that we have advocated previously for the treatment of common lumbar pain generators that may affect patients’ walking endurance differently depending on the functional context at the time when the spine care is delivered.26 Mechanical back pain after endoscopic decompression, particularly in those patients where a hollow vacuum disc is found requiring additional medical, interventional, and surgical treatments, is not uncommon,27–30 which is why we entertained the further use of spinal stabilization in conjunction with the lumbar endoscopic spinal surgery.
While both anterior31,32 and posterior33 column stabilization can be considered and are technically feasible to be performed endoscopically, the posterior column stabilization with interspinous process spacers (IPS) appears more attractive because of the (a) ease of minimally invasive implantation34–37 and (b) vast extent body of outcome literature on the clinical application of several implant systems in the treatment of claudication symptoms in patients with spinal stenosis, thereby catering to the individual surgeon’s preference.38–44 Furthermore, nearly all IPS systems are approved by the Food and Drug Administration (FDA) for standalone use obviating the need for posterior supplemental fixation,45–55 which would, if necessary, complicate the scope of the endoscopic surgery, raise costs,51,56,57 and take away from the attractiveness of the outpatient nature of the endoscopic surgery—a factor that could deter patients specifically seeking out endoscopic spine surgeons who do not subscribe to the routine use of pedicle screws. In contrast, there is currently only one interbody fusion system approved by the FDA for standalone anterior column stabilization.31,58 Many other static and expandable interbody fusion systems suitable for the minimally invasive stabilizing anterior column reconstruction are available.58–65 Still, they are not FDA approved to be used without supplemental use of posterior pedicle screw instrumentation.
The motivation for the conjunctional use of IPS with the endoscopic spinal decompression procedure stems from the desire to improve clinical outcomes with both methods and their associated durability. It is well known that the endoscopic lumbar decompression may rid patients of sciatica-type low back and leg pain as well as significantly improve endurance-limiting claudication symptoms but leave them with mechanical back pain that can be severe at times.3,66,67 IPS are well known to produce good relief from these types of symptoms comparable to the various forms of open and minimally invasive lumbar decompression surgeries in the short term and midterm68–72 while being associated with higher long-term reoperation rates than their surgical counterparts involving a formal decompression of the symptomatic compressed neural elements.36,44,73–76
In this meta-analysis, comparing numerical clinical outcomes with the directly visualized endoscopic and the nonvisualized indirect IPS decompression, the authors were interested in examining the associated effect sizes (ES) of commonly employed patient-reported outcome measures: the Oswestry Disability Index (ODI)77–79 and the visual analog scales (VAS) for back and leg pain.80 Many published meta-analyses attempted to demonstrate clinical superiority of the endoscopic spinal surgery outcomes when compared to traditional translaminar microsurgical decompression techniques by selecting a few high quality studies, especially randomized controlled trials,81 while excluding the findings from noncontrolled studies that are highly prevalent in the spinal surgery literature. Restricting meta-analyses by type of design or, for that matter, metrics of outcomes limits integration of clinically comparable data that might provide a comprehensive view on treatments and associated outcomes across settings.
To the authors’ best knowledge, a meta-analysis comparison of results between lumbar endoscopic spinal decompression and IPS implantation that is agnostic to and thus supersedes study design and standardizes observed effects has not been reported. Instead of performing a narrowly focused meta-analysis based on a few randomized prospective, nonrandomized or single-group prospective studies, or well-controlled cross-sectional retrospective studies, we were interested in a broad investigation of the ES associated with reported clinical outcome improvements with lumbar endoscopic spinal and IPS surgery by extracting and analyzing the ODI and VAS means, SD, and the number of patients in each study. We performed additional subcategory, modifier, and wave analyses to cross-tabulate extracted ES by the length of follow-up, patients’ age, the indication for surgery, the publication year, and the type of study design employed by the authors of the original studies. Ultimately, the authors intended to create a reference table of ES with the IPS and endoscopic spinal surgery to employ it in the comparative evaluation of the clinical merits of combing these 2 procedures.
MATERIALS AND METHODS
Search Strategy and Study Selection
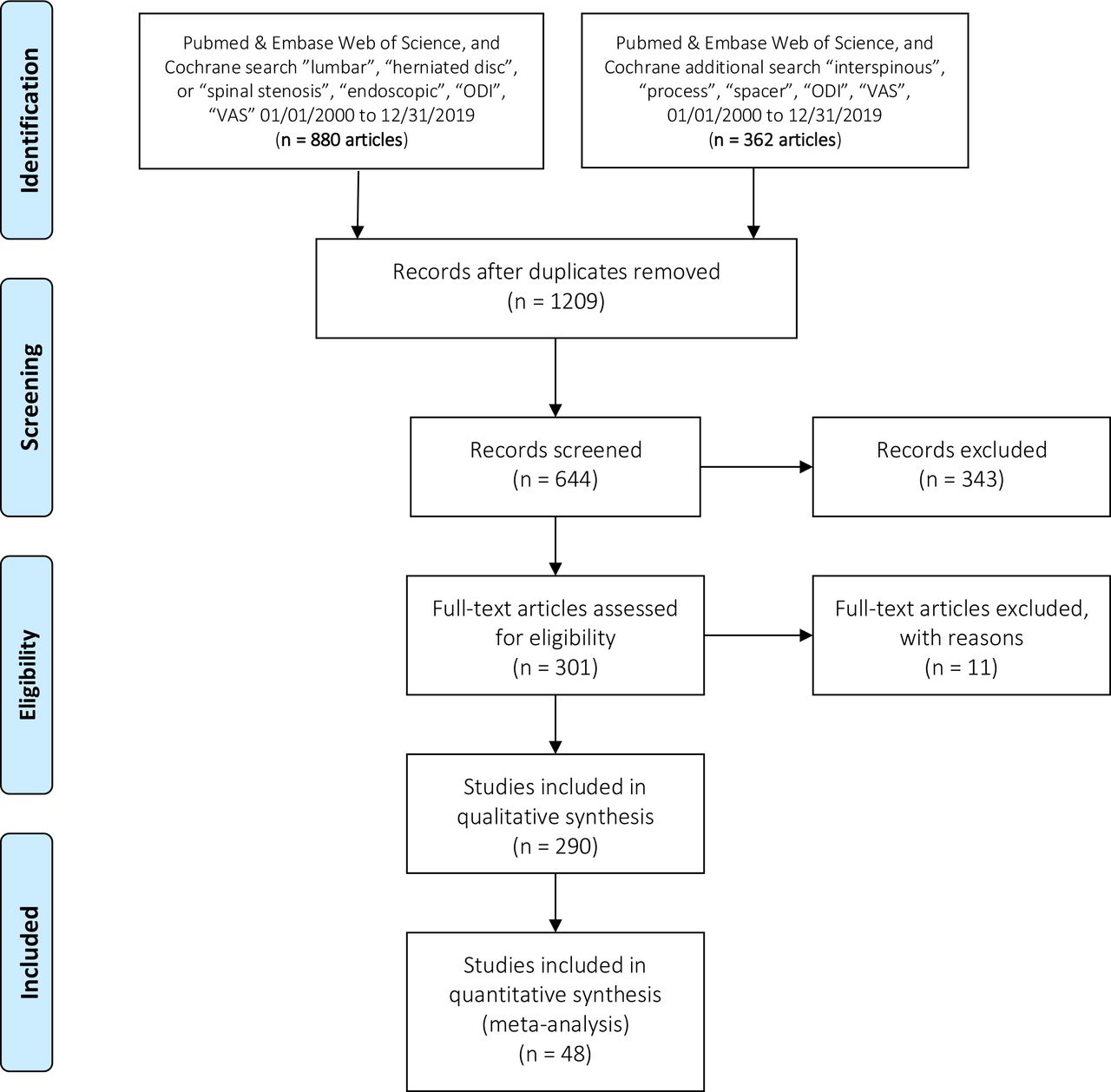
The authors were interested in analyzing the ES data reported for commonly used numerical clinical outcome instruments including the ODI,77–79 and VAS80 for back and leg pain with lumbar endoscopic decompression and the IPS procedures. Therefore, we performed a meta-analysis of clinical studies on IPS and endoscopic decompression for lumbar herniated disc and spinal stenosis, reported here in alignment with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.82–89 For this purpose, 3 authors (KUL, MYW, and ATY) searched the English-language literature on PubMed, Embase, Web of Science, and the Cochrane Database from 1 January 2000 to 31 December 2019 using “lumbar” and “herniated disc” or “spinal stenosis’’ and “endoscopic” and ‘‘ODI” and “VAS,” or “interspinous” and “process” and “spacer” as keywords. They compared their searches to finalize the set of studies to be reviewed for possible inclusion. Discrepancies were resolved by consensus (Figure 1).
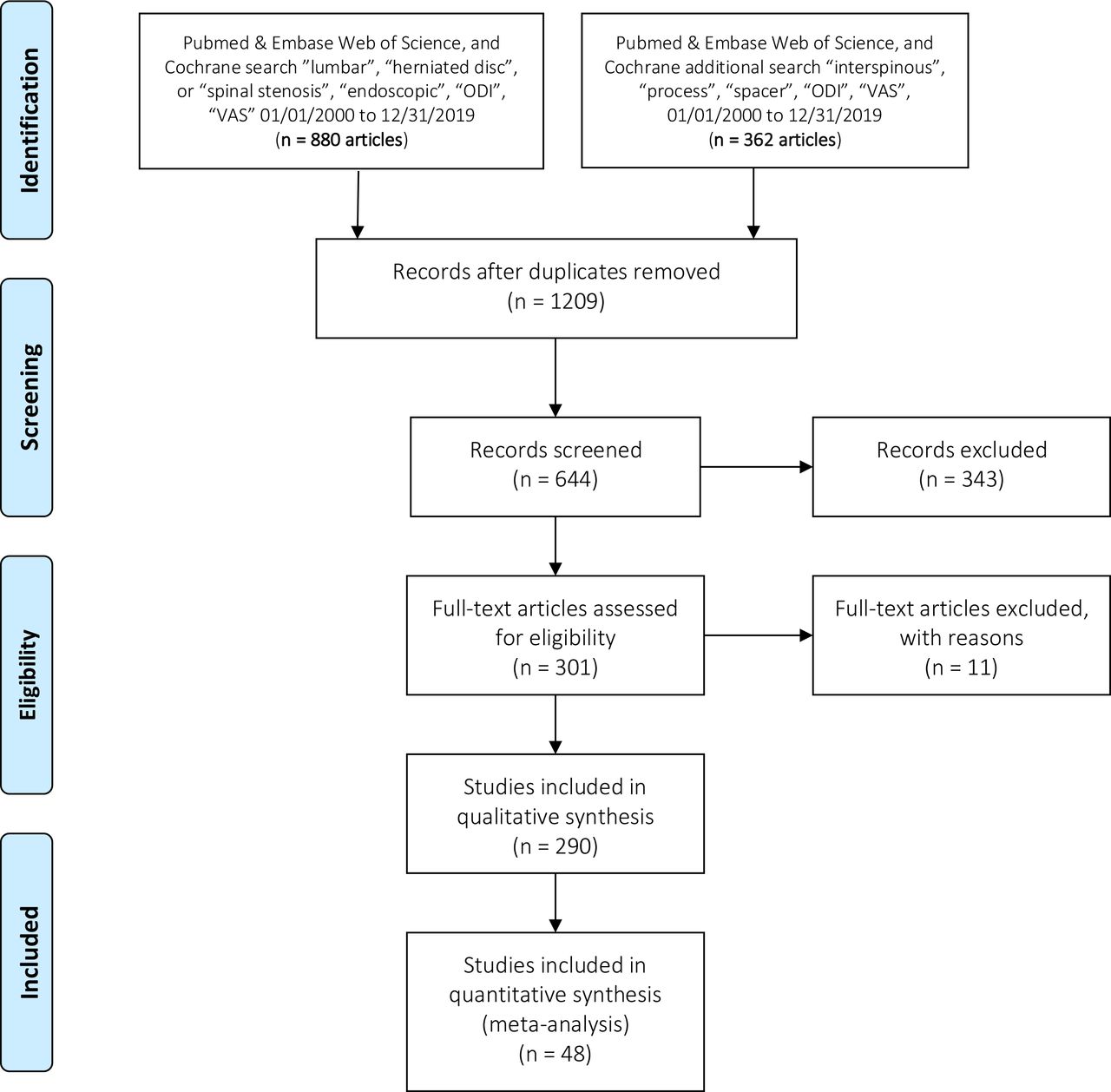
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of selected endoscopy and interspinous process spacer studies. ODI, Oswestry Disability Index; VAS, visual analog scale.
Inclusion/Exclusion Criteria and Data Extraction
To be retained in the meta-analysis, studies needed to employ cross-sectional retrospective, prospective single treatment group, or randomized prospective multitreatment arm study designs comparing endoscopic with other minimally invasive spinal surgery techniques (MISST) including tubular retractor, and others. Studies needed to report IPS and endoscopic spinal surgery outcomes on patients suffering from symptoms related to lumbar herniated disc and foraminal or lateral recess stenosis utilizing the ODI, and the respective VAS scales for back and leg pain. IPS studies using the Zürich claudication score90–93 were excluded since it is not a common outcome measurement tool in endoscopic spinal surgery studies. Only studies that reported the mean, the SD, and the sample size preoperatively and postoperatively for the ODI, VAS-back, and VAS-leg were retained as this was essential information to calculate the effect metrics. Retrieved studies were further stratified by the type of endoscopic MISST access to the neural elements including transforaminal, interlaminar, or combinations, or variations of these techniques. Case reports, review articles, letters to the editor, editorials, short-term reports, and nonclinical studies, such as biomechanical and cadaveric studies, were excluded.
Statistical Analysis
Database
We compiled a database of the included studies by recording the first study author and up to 2 additional coauthors (to differentiate between papers with same and similarly named first author), year of publication, study patients’ mean age, and the preoperative baseline and the postoperative numerical ODI, VAS-back, and VAS-leg scores at final available follow-up. Studies comparing multiple treatments were categorized by comparisons of “endoscopy” or “IPS” implantation vs “microsurgical” or “open” decompression. Additional moderators used in the analysis were study design (retrospective, prospective, and randomized prospective), indication for surgery (herniated disc radiculopathy, stenosis claudication, and discogenic pain), type of MISST (endoscopy, open laminectomy, or tubular microdiscectomy), and IPS implantation.
Standardization of Effects Across Study Designs
Clinical outcome data extracted from the articles included in this meta-analysis were the means and SDs of the VAS-back, the VAS-leg, and the ODI, as well as the sample sizes preoperatively and postoperatively. The ES of postoperative improvements relative to preoperative status was calculated on the basis of the number of enrolled study patients available at last follow-up using Cohen d:
d = (M postop – M preop) / SDpooled (Eq. 1)
where M refers to the respective preoperative and postoperative means and SDpooled to the pooled SD of the preoperative and postoperative scores on the 3 scales of interest.94,95 By convention, d = 0.2 is considered a “small” ES, d = 0.5 represents a “medium” ES, and d = 0.8 a “large” ES. We applied d = 0.2 as the threshold, meaning that if the means of outcomes in endoscopy and IPS did not differ at a minimum by 0.2 SDs, the difference was considered trivial even if statistically significant.
Analysis
The calculated ES, lower limit, upper limit, Higgins I 2 statistic of heterogeneity (I 2), variance (V), SE, number of patients, and significance level (sig) of 95% CI were tabulated for all outcomes combined (ODI, VAS-back, and VAS-leg) and for each outcome separately; this was done across both surgery types and stratified by each surgery. Significance testing for differences between types of surgery was done using random effects analysis of variance of the studentized range statistic Q with separate estimates of T 2 used in the between-group sum-of-squares estimation. These procedures were also applied to subanalyses by study design (retrospective, prospective, and randomized prospective) and surgery indication (herniated nucleus pulposus [HNP]; stenosis claudication). The average reduction of ODI, VAS-back, and VAS-leg was compared to the reported and calculated minimal clinically important difference parameters of 3.0 for the VAS-back and VAS-leg and 15 for ODI.96–101 Statistical significance was set at α of 0.05.
Each of the ODI, VAS-back, and VAS-leg means of each study was weighted in inverse proportion of the respective variances and thus proportional to its precision. Heterogeneity among studies on an outcome of interest was examined by the Cochran Q test with the Higgins I 2statistic quantifying the percentage of variation across studies due to heterogeneity rather than chance. However, as patient-reported outcomes such as the ODI and, especially, the 2 VAS scales are known to be ordinal and inherently anchorless due to interindividual variation in thresholds and valuation, we considered the I 2 as informative but not as cutoffs. To further offset this, all analyses applied a random effects model. Weighted metaregression plots were generated to evaluate associations between standardized ES and the potential moderator variables of patient age (in years) and follow-up (in months). Funnel plots (SE vs ES) were visually assessed for evidence of publication bias and by calculating the one-sided P value for intercept in Egger linear regression analysis and Kendall’s τ. Analyses were performed using Prometa 3, version 3.0 (Internovi, Borne, The Netherlands, 2015). Prometa 3 plotted the ES data in terms of non-standardized differences.
RESULTS
Search Results
The first search yielded 880 publications, and the second search identified another 362 publications. Applying the inclusion/exclusion criteria, 48 publications were subjected to a full-text review resulting in the inclusion of 29 endoscopy5,7,30,102–127 and 19 IPS studies in this meta-analysis (Figure 1).42,46,53,70,128–142
Meta-Analysis Results for Clinical Outcomes
The pooled standardized ES when combining the ODI, VAS-back, and VAS-leg data for the total sample size of 19,862 data sets from the 30 endoscopy studies and 18 interspinous spacer (ISP) studies revealed an overall ES of 0.877 (95% CI = 0.857–0.898). Stratifying by type of surgery, the pooled standardized ES across all outcomes were 0.877 (95% CI = 0.849–0.905; N = 10230) for endoscopic decompression and 0.863 (95% CI = 0.796–0.930; N = 8508) for IPS implantation, with the difference marginally failing statistical significance (P = 0.056).
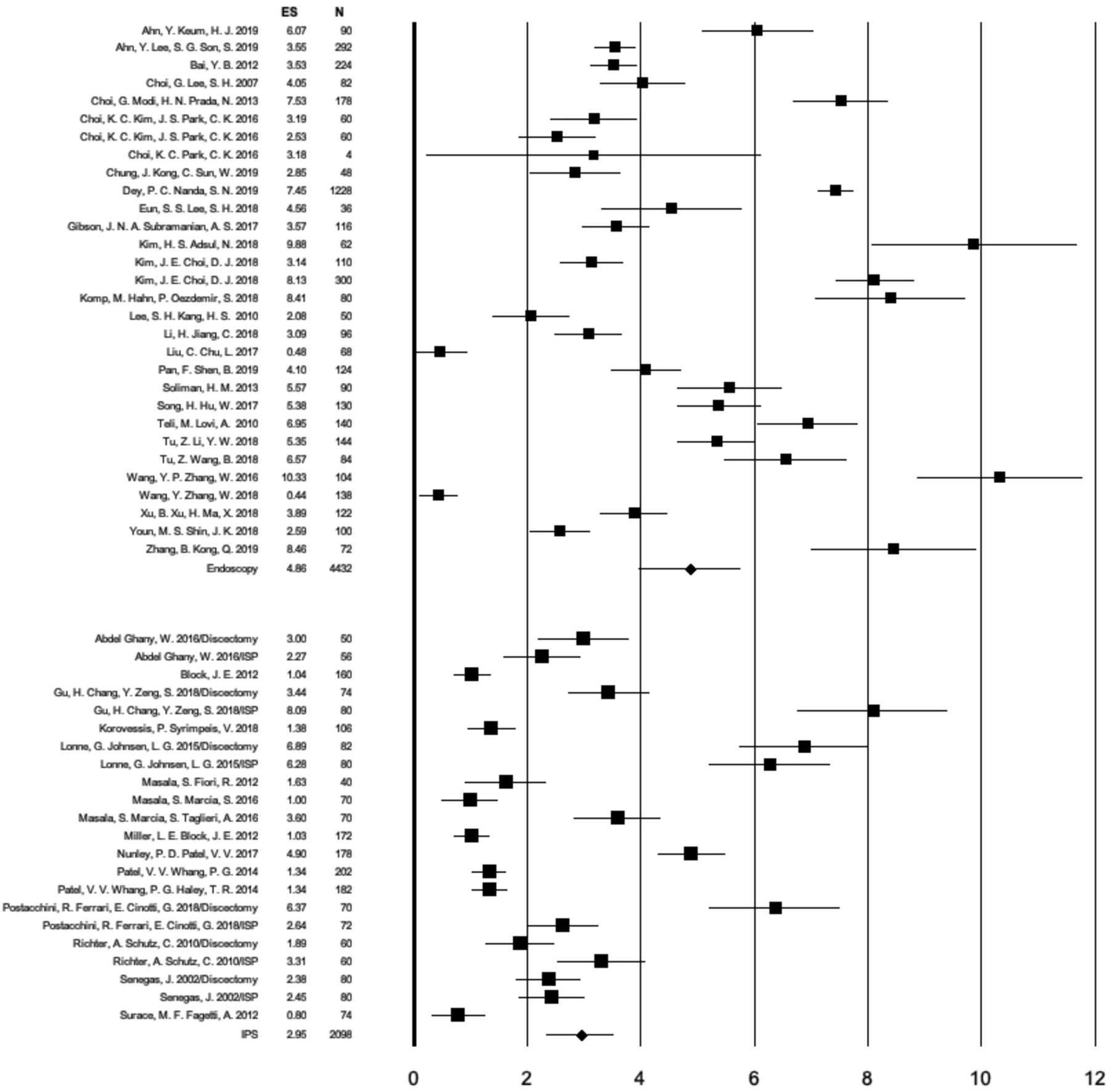
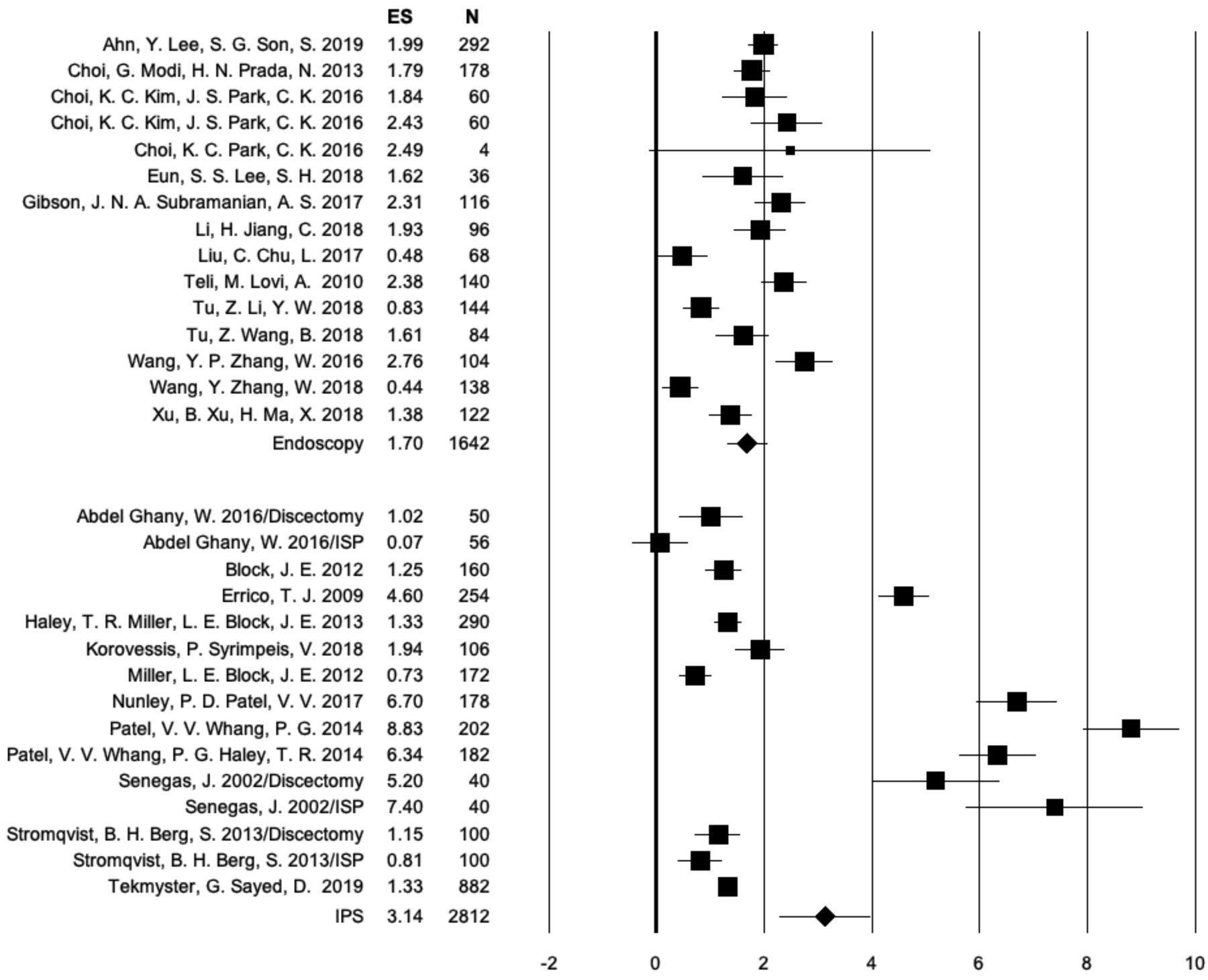
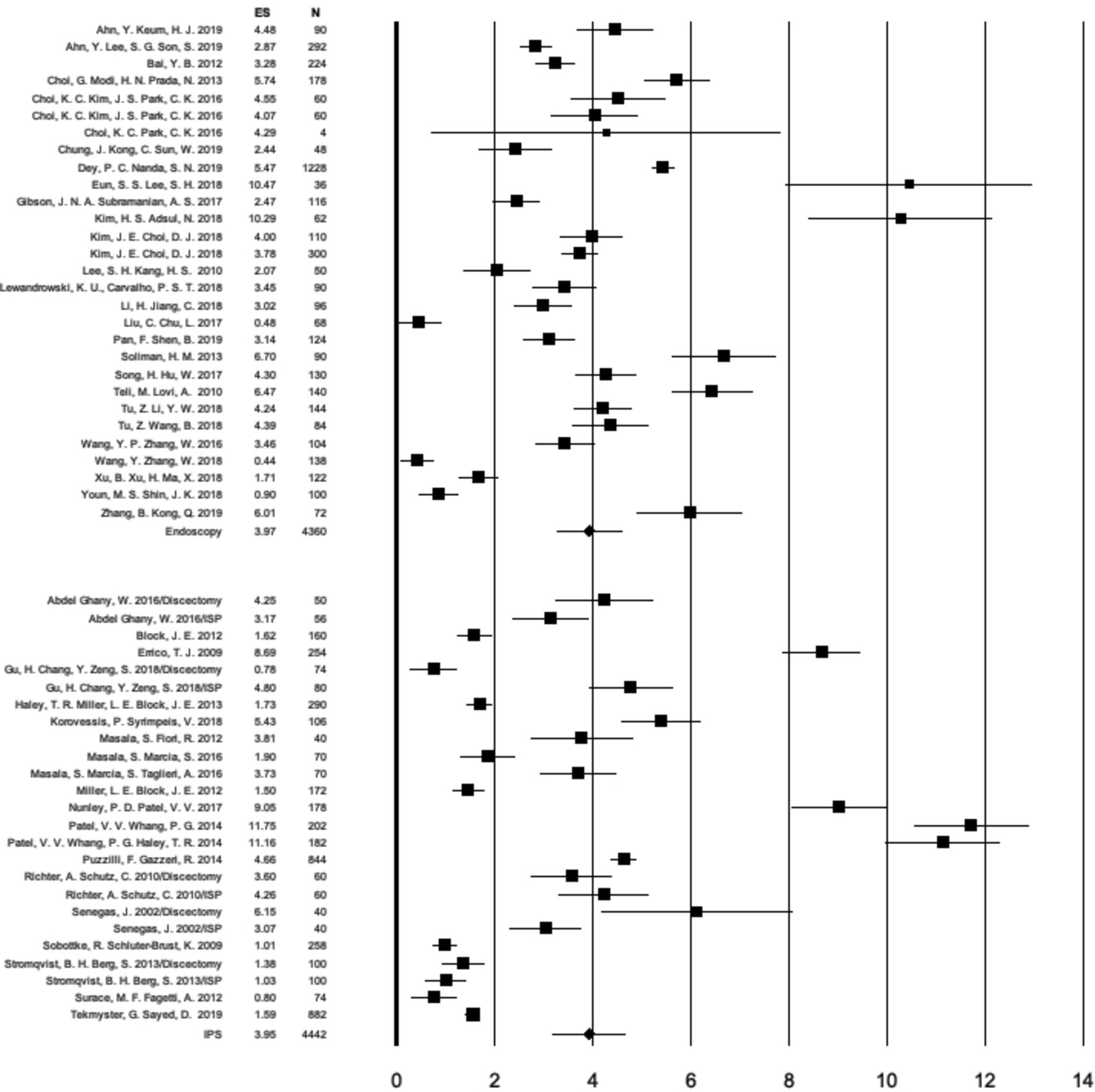
In analyses by specific outcome, the pooled standardized ES for ODI (N = 6462) were 0.916 (95% CI = 0.891–0.943; N = 4364) for lumbar endoscopic decompression and 0.798 (95% CI = 0.713–0.883; N = 2098) for the IPS procedures—a difference that was statistically significant (P = 0.001) (Figure 2; Table 1). The pooled standardized ES for VAS-back (N = 3672) were 0.661 (95% CI = 0.585–0.738; N = 1574) for lumbar endoscopic decompression and 0.784 (95% CI = 0.644–0.923; N = 2098) for the IPS procedures—a difference that was not statistically significant (P = 0.187) (Figure 3; Table 1). The pooled standardized ES for VAS-leg (N = 7890) were 0.885 (95% CI = 0.852–0.917; N = 4292) for lumbar endoscopic decompression and 0.851 (95% CI = 0.767–0.935; N = 3598) for the IPS procedures—a difference that was not statistically significant (P = 0.427) (Figure 4; Table 1).

Forest plot of calculated Oswestry Disability Index (ODI) effect sizes (ES), 95% CI, and the number of patients enrolled in each of the endoscopic spinal surgery and interspinous process spacer (IPS) studies listed in alphabetical order according to the first author’s name. The number of individual study patients is represented by the size of the square. The calculated pooled standardized ES for changes in ODI for the endoscopy studies was 0.917 (95% CI = 0.891–0.943). The corresponding ES for the IPS procedures was 0.798 (95% CI = 0.713–0.883). The analysis of variance Q test of difference showed a statistically higher ODI ES with endoscopy than with the IPS procedure (P = 0.001). Prometa 3 plotted the ES data in terms of non-standardized differences.
List of endoscopy studies included into the meta-analysis with brief summary of study highlights.
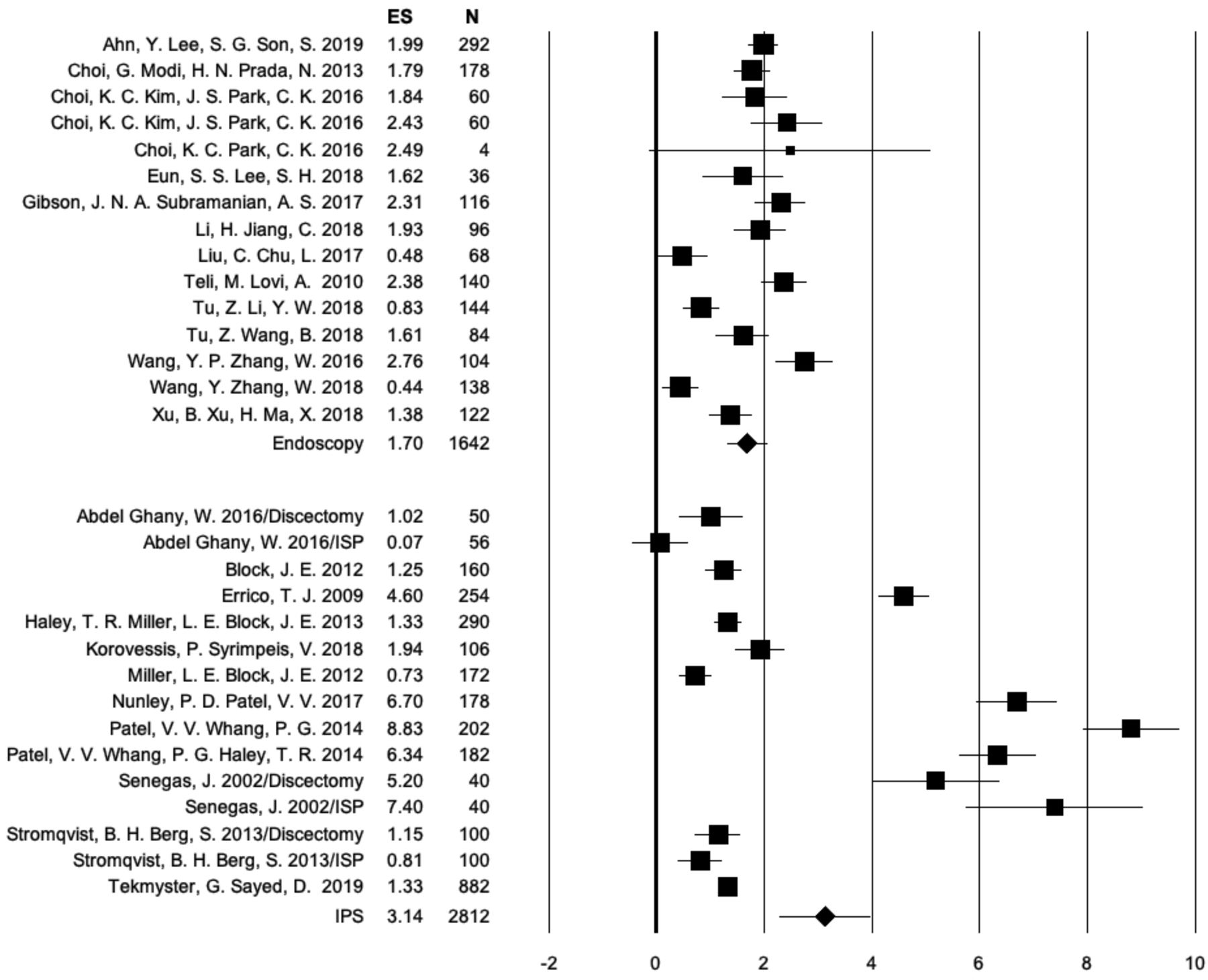
Forest plot of calculated visual analog scale (VAS)-back effect sizes (ES), 95% CI, and the number of patients enrolled in each of the endoscopic spinal surgery and interspinous process spacer (IPS) studies listed in alphabetical order according to the first author’s name. The number of individual study patients is represented by the size of the square. The calculated pooled standardized ES for changes in VAS-back for the endoscopy studies was 0.661 (95% CI = 0.585–0.738). The corresponding ES for the IPS procedures was 0.784 (95% CI = 0.644–0.923). The analysis of variance Q test of difference indicated that this difference in VAS-back ES was not statistically significant (P = 0.187). Prometa 3 plotted the ES data in terms of non-standardized differences.
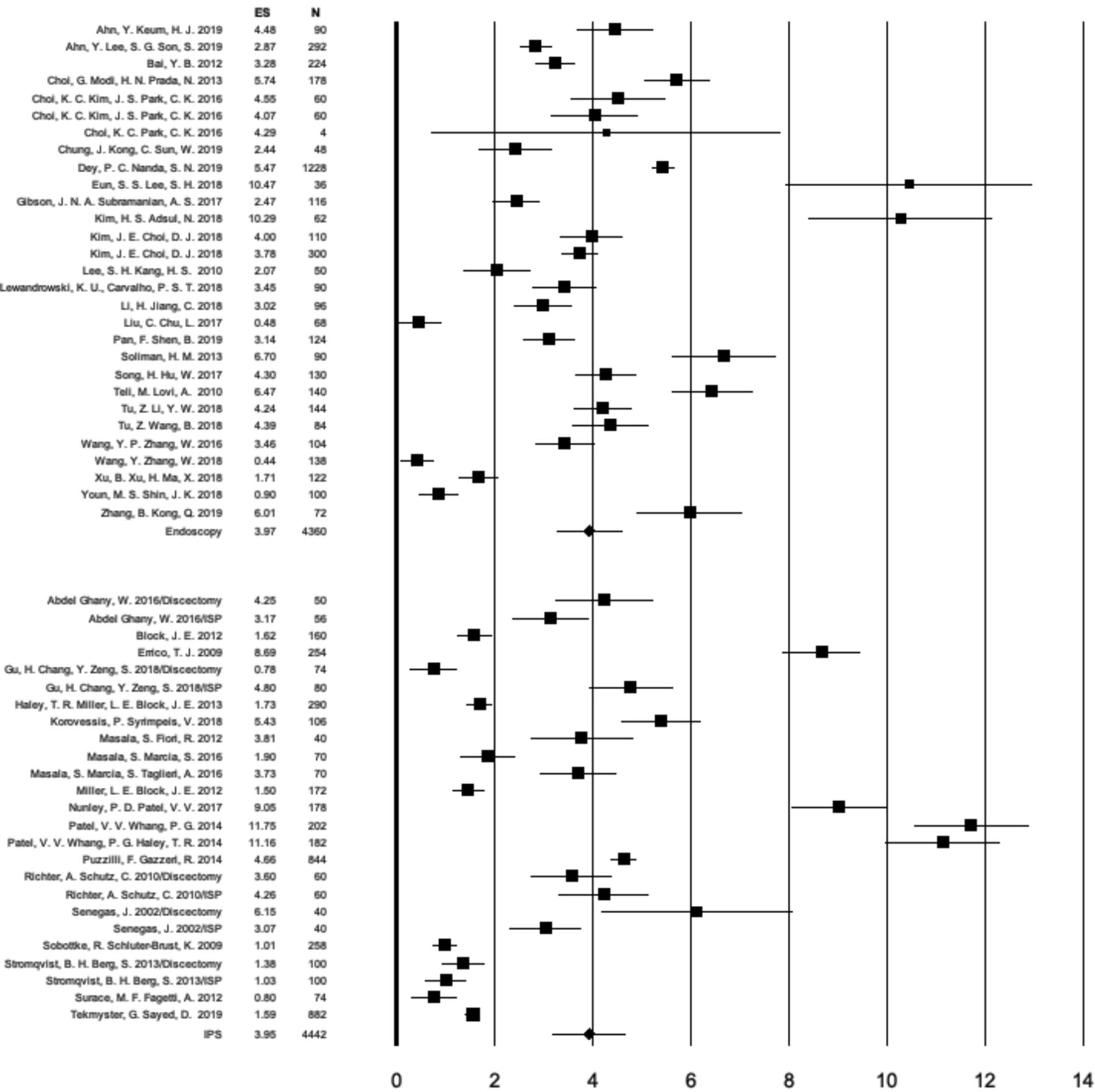
Forest plot of calculated visual analog scale (VAS)-leg effect sizes (ES), 95% CI, and the number of patients enrolled in each of the endoscopic spinal surgery and interspinous process spacer (IPS) studies listed in alphabetical order according to the first author’s name. The number of individual study patients is represented by the size of the square. The calculated pooled standardized ES for changes in VAS-leg for the endoscopy studies was 0.885 (95% CI = 0.852–0.917). The corresponding ES for the IPS procedures was 0.851 (95% CI = 0.767–0.935). The analysis of variance Q test of difference indicated that this difference in VAS-leg ES was not statistically significant (P = 0.427).
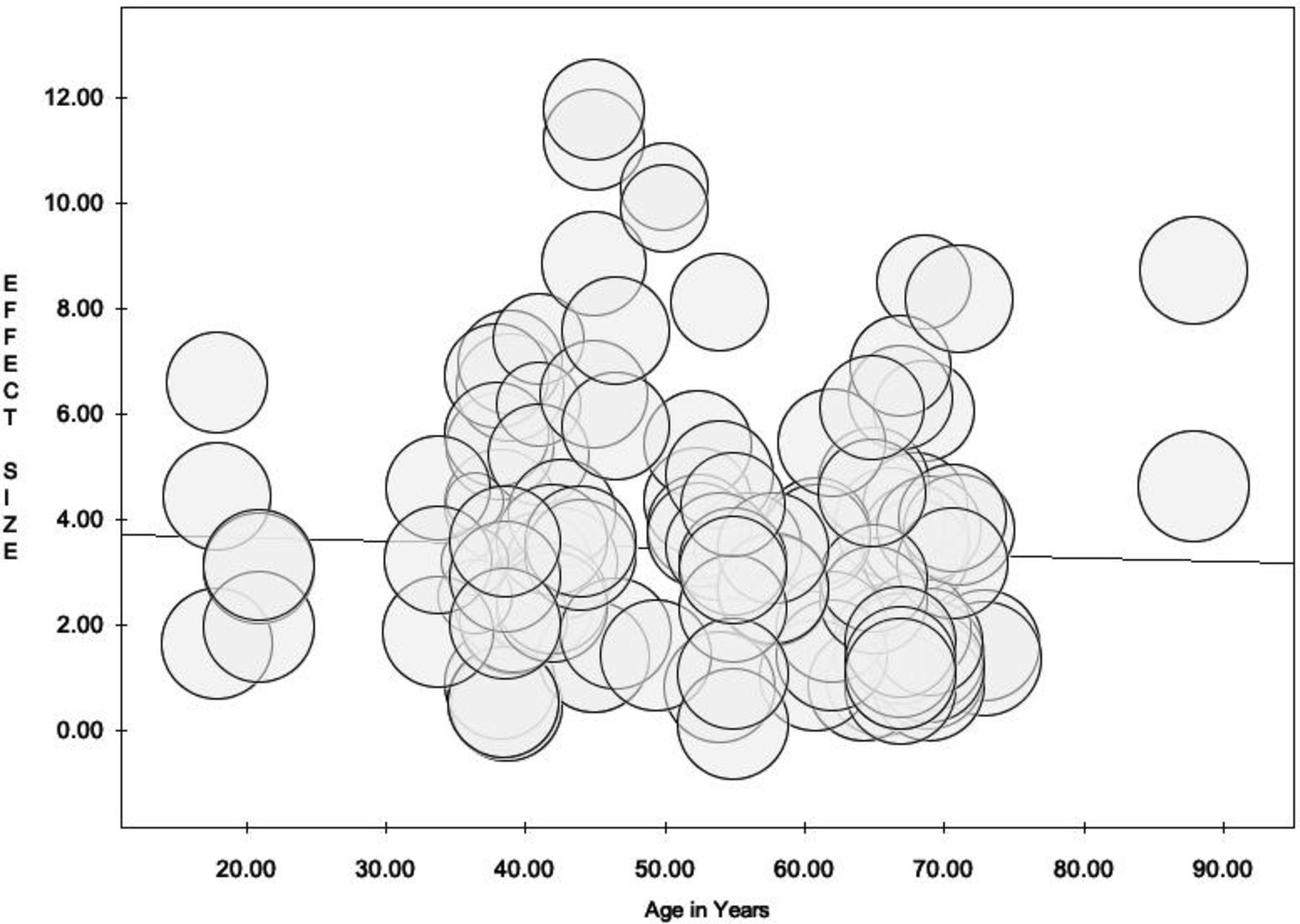
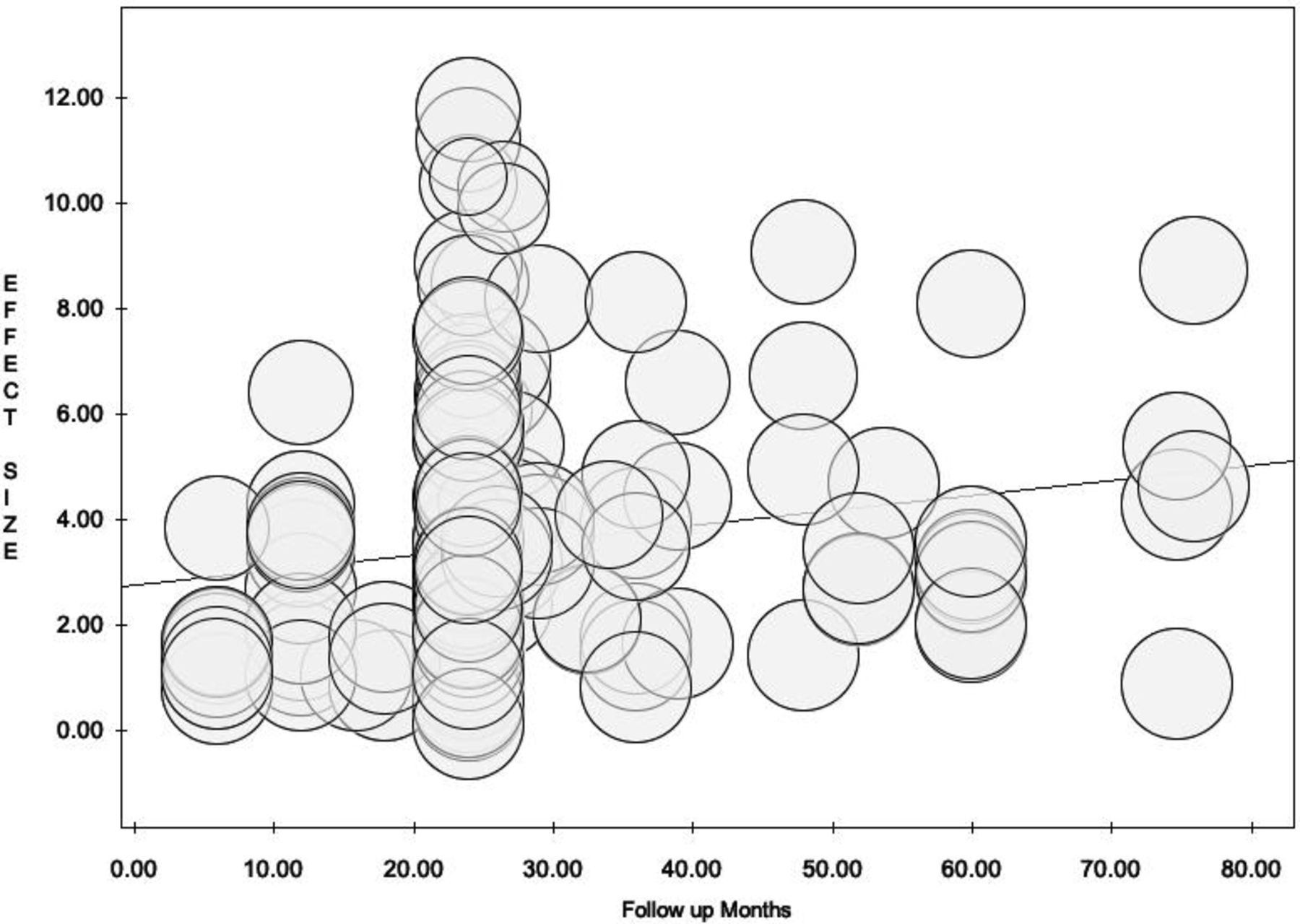
Weighted regression analysis showed no significant (P = 0.289) association between pooled standardized ES and patient age (Figure 5); but did reveal an overall significant association (P = 0.026) between pooled standardized ES and follow-up (in months; Figure 6). Visual inspection of Figure 6 shows a large cluster of studies with follow-up of 24 months and many studies with longer follow-up compared to much fewer studies with follow-up less than 24 months. Further analysis revealed that follow-up of 24 months or more occurred in all of the ISP studies.

Meta-analysis regression plot of effect size vs age in years using random effects model showed no significant correlation (P = 0.289).
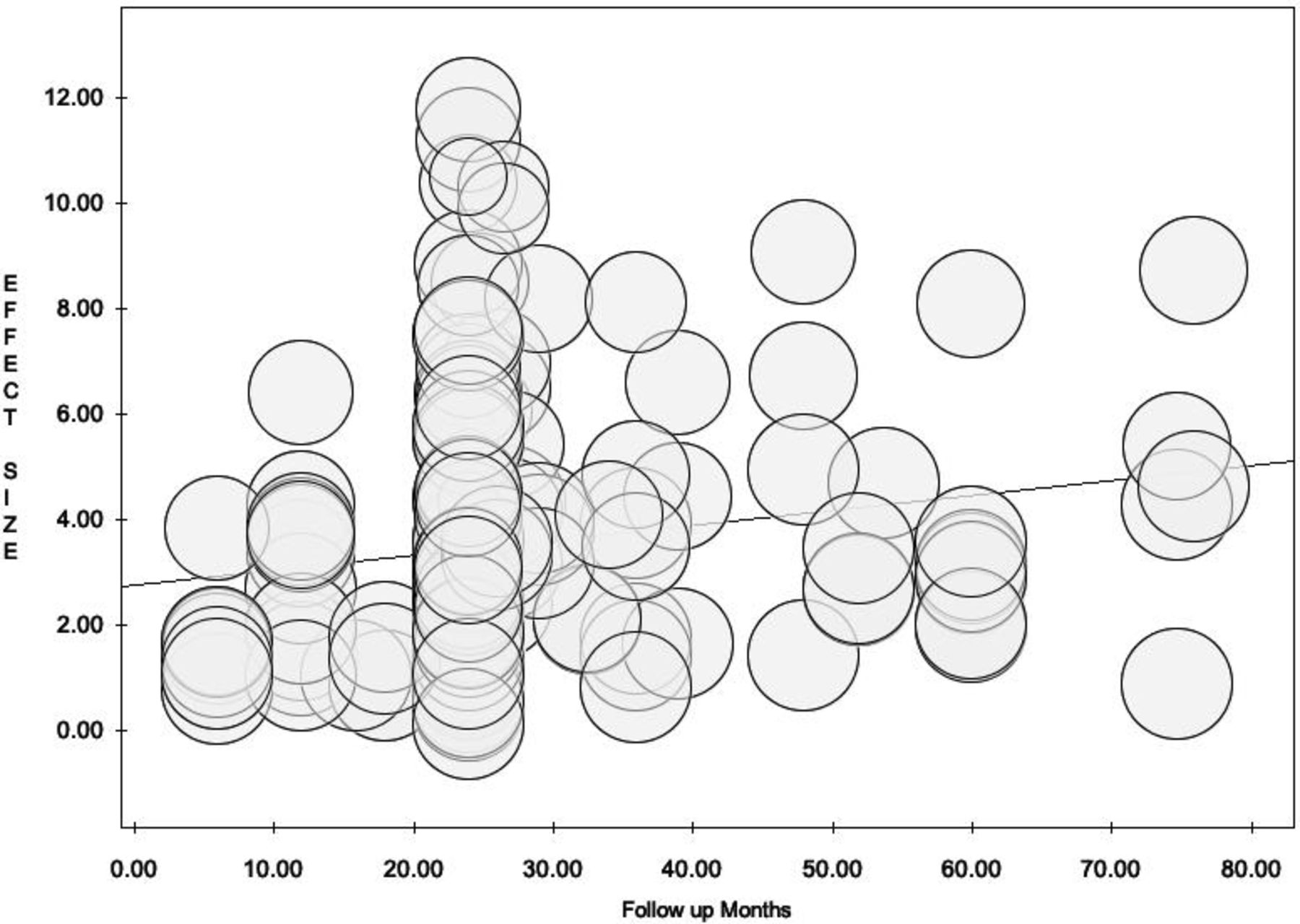
Meta-analysis plot of effect size (ES) vs follow-up in months using random effects model showed a statistically significantly higher proportion of studies (all of the interspinous spacer studies) with either 24 months follow-up or more with higher ES numbers in the longer follow-up studies (P = 0.026).
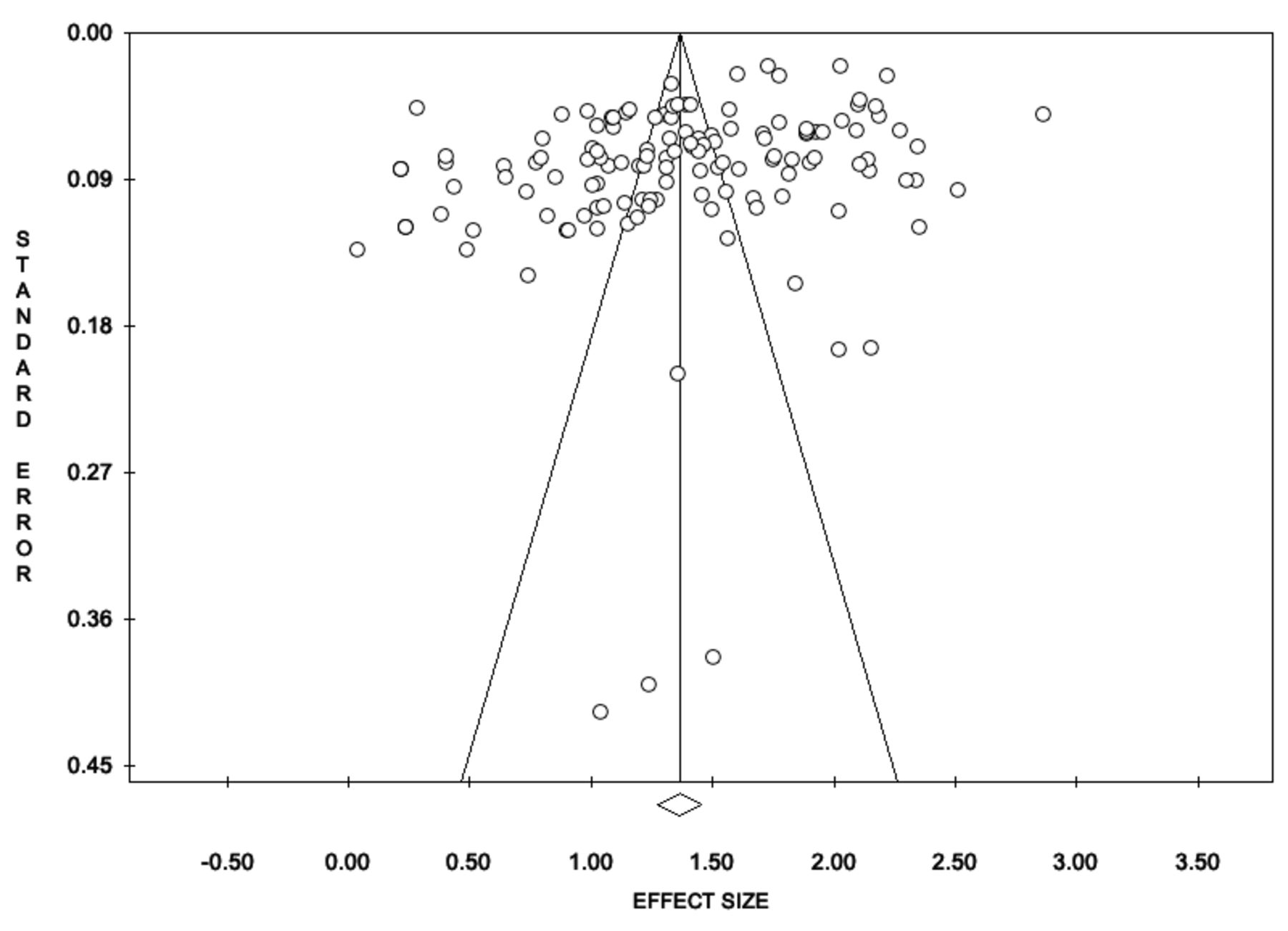
Egger’s regression yielded an intercept of 5.93 (P = 0.001), and Kendall’s τ was −2.17 (P = 0.030) in analyses including all 3 outcome variables. The asymmetric funnel plot with several studies falling outside the expected area of SE vs ES further indicates moderate publication bias (Figure 7).

Funnel plot assessing publication bias (SE vs effect size).
Meta-Analysis by Modifiers
Subanalyses by study design (Table 2) revealed pooled standardized ES for the ODI (N = 6462) of 0.884 (95% CI = 0.846–0.922; N = 3314) for retrospective studies, 0.890 (95% CI = 0.821–0.960; N = 1774) for prospective studies, and 0.843 (95% CI = 0.729–0.957; N = 1374) for randomized prospective studies (differences not significant, P = 0.742). Pooled standardized ES for the VAS-back (N = 4386) were 0.715 (95% CI = 0.587–0.843; N = 2560) for retrospective studies, 0.425 (95% CI = 0.048–0.803; N = 284) for prospective studies, and 0.806 (95% CI = 0.653–0.959; N = 1542) for randomized prospective studies (differences not significant, P = 0.112). Pooled standardized ES for the VAS-leg (N = 7890) were 0.866 (95% CI = 0.819–0.912; N = 4716) for retrospective studies, 0.912 (95% CI = 0.885–0.938; N = 1632) for prospective studies, and 0.860 (95% CI = 0.733–0.987; N = 1542) for randomized prospective studies (differences not significant, P = 0.175).
List of interspinous process spacer studies included into the meta-analysis with brief summary of study highlights.
Subanalyses by surgery indication (Table 3) yielded pooled standardized ES for the ODI (N = 2884) of 0.920 (95% CI = 0.862–0.977; N = 880) for HNP radiculopathy and 0.815 (95% CI = 0.722–0.907; N = 2004) for stenosis claudication (differences not significant, P = 0.076). Pooled standardized ES for the VAS-back (N = 3286) were 0.532 (95% CI = 0.271–0.794; N = 506) for HNP radiculopathy and 0.694 (95% CI = 0.514–0.874; N = 2780) for stenosis claudication (differences not significant, P = 0.307). Pooled standardized ES for the VAS-leg (N = 4464) were 0.868 (95% CI = 0.769–0.966; N = 880) for HNP radiculopathy and 0.830 (95% CI = 0.736–0.874; N = 3584) for stenosis claudication (differences not significant, P = 0.869).
Analysis of effect size, heterogeneity, and ANOVA testing of difference by surgery type.
Analysis of effect size, heterogeneity, and ANOVA testing of difference by study type.
Individual Studies Results and Minimal Clinically Important Difference
Preoperative baseline means (SD) were 59.34 (SD 12.67) for the ODI, 4.90 (SD 1.89) for the VAS-back, and 7.22 for the VAS-leg (SD 1.90). Improvements after endoscopic surgery were an ODI reduction of 46.25 (SD 6.10), VAS-back reduction of 3.29 (SD 0.65), and VAS-leg reduction of 5.77 (SD 0.66).The mean (SD) percent changes of ODI, VAS-back, and VAS-leg ratings at a follow-up of 2 years or longer after endoscopic decompression were 77.94% (SD 10.28%), 67.14% (SD 13.26%), and 79.71% (SD 9.14%), respectively. The mean (SD) percent change of ODI, VAS-back, and VAS-leg at a follow-up of 2 years or longer after ISP implantation was 68.31% (SD 9.39%), 58.12% (SD 11.51%), and 71.21% (SD 11.26%), respectively. The ODI, VAS-back, and VAS-leg reductions producing the ES calculations listed in Tables 1–3 were the equivalent of 3 times reported minimal clinically important differences.84
DISCUSSION
One might ask, what is the point of combining lumbar spinal endoscopy with the placement of an IPS? To those who routinely perform both types of surgeries, the answer is quite obvious. Both procedures have shortcomings that are far outweighed by their advantages but in some cases prompt new interventional and surgical management following the index procedure. In short, spinal endoscopy is attractive to many patients because of the small incisions, low complication rates,22,23 and its outpatient nature. The staged management approach to common lumbar spinal pain generators the authors advocate for143 translates into minor concise surgeries on validated pain generators, while ignoring many other structural problems not contributing to the patient’s pain syndrome in the current context of spine care at the time when the care is delivered. Endoscopy’s downside is persistent mechanical low back pain, which in many patients stems from facet arthropathy or severely degenerated vacuum discs. IPS implants, on the other hand, are attractive because of the simplicity of implantation and the low perioperative burden to spinal stenosis patients who often suffer from poorly controlled medical comorbidities.76 The short-term and midterm track record of IPS to improve claudication symptoms is favorable,41,44,48,53,56,68–70,128,129,144–148 but the reoperation rate is higher than with formal open lumbar decompression surgery.44,48,52,53,55,74,75,128,139,146,148–154 IPS procedures also have been demonstrated to relieve mechanical back pain effectively.71 Hence, combining lumbar spinal endoscopy and IPS procedures may ultimately improve clinical outcomes with these 2 nonfusion technologies—a strategy that fits well within the scope of cost-saving policies of modern healthcare systems. This dynamic was the underlying motivation of this meta-analysis, which accompanies an original study and review article that is published alongside this meta-analysis in this special focus issue of the International Journal of Spine Surgery.
We took a broad approach to extract outcome data from original studies on endoscopic and IPS spinal surgeries to afford the reader the ability to better compare their clinical benefit concerning indication for surgery and burden to the patient in an across-the-board normalized comparison. Highlighting differences in outcomes between directly visualized endoscopic and the indirect IPS decompression by reporting the standardized ES has several advantages, including the ability to test report statistical tests for group comparison. Standardized ES quantify the gradient of difference between the treatment groups rather than confounding this difference with sample size and statistical power.155–157 As eq. 1 above shows, d is calculated by subtracting the mean of one group from the mean of another group and dividing it by the pooled SD. Despite being standardized and simple, the ES is rarely used in the comparison and discussion of clinical outcomes between treatments.155 As we showed here, the d metric can be highly useful as a measure of overlap of treatment benefit between spinal endoscopic and IPS procedures—a form of data interpretation we employed in this study to illustrate the various aspects of clinical benefit between the types of lumbar decompression procedures.
We chose the meta-analysis approach to calculating ES since it overcomes the common problem of not knowing the SD of the population from which the different treatment groups were sampled by estimating it by pooling data from the treatment groups of various studies. The ES derived from preoperative and postoperative disability data (ODI, VAS-back, and VAS-leg) from a total of 48 studies were, in general, large.95 Importantly, they tended to exceed established reference data set of ES with the endoscopic and the IPS procedures by a multiple of about 3, which to the authors’ best knowledge has not been published.
Despite the majority of patients treated with endoscopic or IPS surgery were between the ages of 40 and 70 years, patient age was not found to impact clinical outcomes (Figure 5). Further, and important given the general challenge in surgery for randomized (blinded) clinical trials, neither did the type of study design impact ES—though with one, albeit positive, exception: the ES calculated for the VAS-back underscored the long-term (2 years or more postsurgery) benefit of IPS in relief of back pain (Figure 6), especially in higher quality randomized prospective trials with therefore lower risk of bias. When stratifying by surgical indication as a modifier, ODI and VAS-leg ES for the surgery indication of spinal stenosis-related neurogenic claudication were similar and both were higher than the corresponding ES for VAS-back (Table 4). The overlap in the precision (95% CI) estimates between the VAS-leg ES for the 2 clinical indications studied—stenosis claudication and HNP radiculopathy—was quite large, suggesting that both endoscopic and IPS spinal surgery are effective in relieving symptoms due to either one of these 2 conditions. The calculated VAS-back ES were the higher for the IPS than for endoscopy but not statistically significant because of a large 95% CI overlap. Therefore, the authors’ clinical observation that IPS implantation produces more back pain reduction than endoscopy will need to be formally studied in high quality controlled clinical trials to substantiate this conclusion. Our meta-analysis did not directly compare the clinical 2 outcomes. It instead identified the predominant clinical improvement areas—better improvement of low back pain symptoms with IPS and better radicular pain relief with directly visualized endoscopic decompression. These observations are corroborated by 2 retrospective clinical cohort studies that evaluated clinical outcomes in patients who underwent combined transforaminal endoscopic decompression with simultaneous placement of an IPS.33,158 Another 2-year follow-up study performed by this team of authors on simultaneous minimally invasive IPS placement combined with an endoscopic foraminal decompression reported similar findings.159 At a minimum, our meta-analysis substantiated the rationale for combining the IPS with endoscopy. However, it cannot replace a formal long-term study, which should be carried out as a prospective well-matched cohort study with a robust randomization protocol. Last but not least, implant-related problems may also need to be accounted for as their incidence is currently not known when combining these 2 minimally invasive surgeries both targeting spinal stenosis.
Analysis of effect size, heterogeneity, and ANOVA testing of difference by surgery indication.
As discussed at the outset of this article, we were not interested in pushing endoscopic surgery in favor of IPS. We were only interested in reporting a reference data set of ODI, VAS-back, and VAS-leg ES in the form of reference tables (Tables 3–5) to aid in the ongoing discussion on how to improve the durability of MISST and how to most effectively transition modern spine care to more reliable and less costly procedures by replacing some of the traditional open with endoscopic spinal surgery whose reliability could be improved by performing it in conjunction with a stabilizing procedure, such as an IPS.
We expected to find significant heterogeneity in our meta-analysis. Heterogeneity may be unfavorable in meta-analyses of randomized trials of medical or pharmacotherapeutic interventions as it would suggest significant variability in the outcomes of highly protocolized interventions. In contrast, surgical procedures may follow protocols but its outcomes are also influenced significantly by many factors and class effects (see also below). In addition, disability and pain are subjective and patient outcomes that cannot be objectively scaled because of between-patient variability in appraisal, anchoring, and scaling. Furthermore, while previous meta-analyses were limited to prospective randomized trials,55,73–75,81,160–167 we included nonrandomized prospective studies as well as retrospective analyses. Despite the evidence that well-designed observational studies do not overestimate treatment effects as compared to those obtained in randomized trials,168,169 bias due to differences in the quality of studies and their designs cannot be negated. The use of random effects models in the analyses was intended to manage the observed heterogeneity.
The heterogeneity may also explain the publication bias found in our meta-analysis, a second limitation to be considered. Twenty-eight of the 48 studies included in this meta-analysis were retrospective. Many of these contributed to the spread of study-specific ES data in the 3 forest plots may have tended to cause the funnel plot to be asymmetric with many studies falling outside the funnel. Here too, the use of random effects models aimed to mitigate this bias. Heterogeneity and asymmetry may very well be inherent to surgical studies. Variation in patients’ expectations; the subjectivity and relative lack of anchoring and scaling of disability ratings such as the ODI and the 2 VAS scales; differences in surgeons’ skill level and preferences; variability in organizational process and procedural aspects of the surgery; surgery being carried out either in an outpatient ambulatory surgery center or in a hospital setting; and many other factors may be responsible for the heterogeneity observed in some of the subgroups as evidenced by some of the outliers. The differences found in the ODI, VAS-back, and VAS-leg ES are reflective of real-life clinical scenarios where spine care is delivered under a great variety of patient-related and system-related circumstances. The surgeon skill factor is likely the most relevant confounder in this whole analysis and may be responsible for the wide overlap in successful clinical outcomes regardless of the type of direct or indirect lumbar decompression surgery employed.
CONCLUSIONS
The classic indication for lumbar endoscopy has been lumbar herniation, but it has evolved to include stenosis as an indication. The indication for IPS is also lumbar spinal stenosis. Both spinal endoscopy and IPS address lumbar stenosis, albeit with different approach mechanisms, direct decompression vs indirect decompression. While the authors’ hypothesis is supported by their statistical meta-analysis modeling and corroborated a limited clinical feasibility 2-year follow-up study on 33 patients,159 there is a need for a long-term follow-up comparison of endoscopy with and without IPS, where potential implant-related failures and complications also will have to be taken into account when analyzing the cost-benefit equation. In spite of these limitations and considering that we did not attempt a formal comparison of endoscopy to other MISSTs or traditional open surgical decompression, our meta-analysis supports a clinically important conclusion: the addition of IPS to transforaminal lumbar endoscopic foraminal decompression may improve outcomes by reducing the residual mechanical low back pain that is often observed with this attractive outpatient surgery. The ongoing debate on the merits of endoscopic spine surgery will likely continue; thus, the clinical merits of combining spinal endoscopy with IPS should be further studied. With this meta-analysis, we provided the statistical evidence required to have this debate in an objective manner where one wonders about the continued need for aggressive open surgeries for the indications investigated herein if the reported differences in ES gradients for clinical improvements are marginal.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest related to this work.
Disclosure The authors report no financial disclosures related to this article.
Disclaimer This manuscript is not meant for or intended to endorse any products or push any other agenda other than the associated clinical outcomes with endoscopic spine surgery. The motive for compiling this clinically relevant information is by no means created and/or correlated to directly enrich anyone due to its publication. This publication was intended to substantiate contemporary endoscopic spinal surgery concepts to facilitate technology advancements.The views expressed in this editorial represent those of the authors and no other entity or organization. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.