


Abstract
Background Anterior cervical discectomy and fusion (ACDF) is a common surgery to treat cervical degenerative disc disease. Use of an anterior spacer and plate system (ASPS) results in increased disc height, higher fusion rate, lower subsidence rate, and lower complication rate than a spacer alone.1,2 However, anterior cervical plating is associated with complications, such as dysphagia, plate-screw dislodgment, soft tissue injury, neural injury, and esophageal perforation.3–9 To potentially reduce these drawbacks, integrated spacer and plate (ISP) systems have gained popularity.
Methods From November 2009 to October 2013, a total of 84 consecutive patients who underwent 2-level ACDF using ISP or ASPS were reviewed for clinical and radiographic outcomes. Patient-reported visual analog scale (VAS) and Neck Disability Index (NDI) scores, fusion rates, and hardware failure were determined at 1, 3, 6, 12, and 24 months after surgery.
Results Forty-three patients received ISP and 41 patients received ASPS. There were no significant differences in patient demographics between the 2 groups. Perioperative characteristics were similar, except for operative time. Postoperatively, no significant differences in VAS or NDI scores or fusion status were found. At the proximal surgical level only, there was a trend toward an earlier observed radiographic fusion rate in ASPS vs ISP, but this finding was not statistically significant (P = 0.092). One case of long-term dysphagia was reported in each group. Neither group had implant failures up to 2 years.
Conclusions The ISP system for 2-level ACDF compared to traditional ASPS has comparable clinical and radiographic outcomes up to 2 years postoperatively. There may be a trend toward an earlier observed radiographic fusion in the ASPS group, but there was no difference in long-term dysphagia rate.
Clinical Relavance Integrated spacer and traditional anterior spacer for 2-level ACDF has similar clinical and radiographical outcome.
Level of Evidence 4.
- anterior cervical spine fusion
- traditional anterior spacer and plate
- zero-profile cage
- integrated plate and spacer
- fusion rate
INTRODUCTION
An anterior cervical discectomy and fusion (ACDF) is one of the most common procedures performed by spine surgeons.1 First described by Robinson and Smith in 1955,2 it is used to treat degenerative cervical spine disease via an anterior approach. The surgical goals of ACDF are decompression via discectomy, restoration of intervertebral height and cervical lordosis, and solid arthrodesis. To achieve the restoration and arthrodesis portion, a spacer is used in the intervertebral area where the discectomy is performed. Historically, autograft harvested from a patient’s iliac crest or rib was used as the spacer. However, due to morbidity associated with the actual harvesting, spacers made of polyether ether ketone are now more commonly used instead of harvested autograft to achieve the surgical goals.3–9
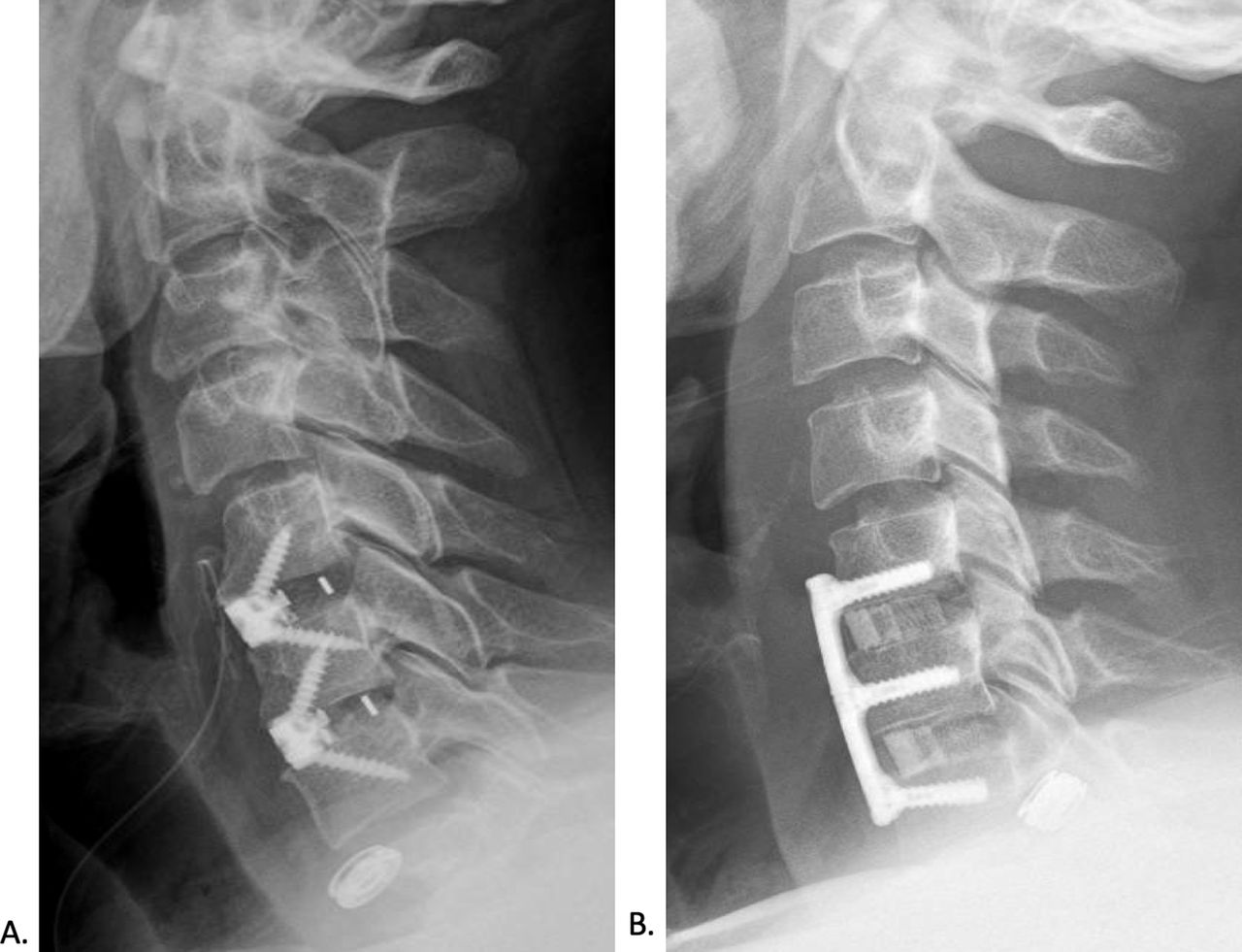
In addition, the use of an anterior plate in addition to the interbody spacer results in increased disc height, a higher fusion rate, a lower subsidence rate, and a lower complication rate when compared to an anterior interbody spacer alone.10,11 Yet, anterior cervical plating (ACP) has been associated with significant morbidity, such as dysphagia, plate-screw dislodgment, soft tissue injury, esophageal perforation, and neural injury.12–18 In an attempt to reduce the drawbacks of the traditional anterior spacer and plate system (ASPS) technique, an integrated spacer and plate (ISP), or zero-profile, system has been developed (Figure).

Lateral radiographs of the cervical spine implanted with (A) integrated spacer and plate and (B) traditional anterior spacer and plate system.
Given the potential to decrease complications associated with ACP and biomechanical studies showing no significant difference in stability between ISP and traditional ASPS,19,20 the ISP systems have recently gained popularity among spine surgeons. Despite their popularity, there are conflicting reports in the literature on the outcome of ISP systems in ACDF procedures, particularly as stratified by number of surgical levels. Thus the objective of this study was to retrospectively review our experience with the clinical and radiographic outcomes of patients after 2-level ACDF with ISP vs ASPS.
METHODS
We reviewed all consecutive patients undergoing a 2-level ACDF for degenerative cervical disc disease between November 2009 and October 2013 at a single institution. The patients were divided into 2 groups, ISP and ASPS, based upon the technique used in their ACDF. All patients older than 18 years, except those who were pregnant or incarcerated, were included. Patients with previous surgery at adjacent levels were also excluded. This study was approved by the university’s Institutional Review Board.
All patients underwent the Smith-Robinson anterior approach for cervical discectomy and fusion in the subaxial spine (C3-C7). The ISP group was implanted with the 2-screw polyether ether ketone cage with integrated plate system (Coalition; Globus Medical, Inc., Audubon, PA, USA) packed with local autograft. The ASPS group was implanted with tricortical allograft interbody spacer with ACP (Cervical Spine Locking Plate, DePuy Synthes Spine, Inc., Raynham, MA, USA).
Preoperative, perioperative, and postoperative clinical and radiographic data were collected. Preoperative data included age at surgery, sex, clinical presentation, medical comorbidities, and surgical levels. Perioperative data included cage size, graft and implant type, estimated blood loss, and operating times. Clinical outcome data included patient-reported visual analog scale (VAS), Neck Disability index (NDI), hoarseness, and dysphagia at 1, 3, 6, 12, and 24 months outpatient follow-up visits. Only completed clinical outcome surveys were included for analysis. Adverse events related to the procedure were documented as well.
Postoperative radiographic data were collected at 3, 6, 12, and 24 months in the form of dynamic radiographs to evaluate fusion status. Fusion status was categorized into solid fusion, stable, or pseudarthrosis. Solid fusion was noted when there was at least 50% of bone growth noted between the 2 vertebrae. A patient was deemed stable if there was no significant bone growth but had less than 2 mm of interspinous motion on dynamic imaging. Lastly, patient was classified as pseudarthrosis if there was 2 mm or more of motion observed between the spinous processes on dynamic films or if less than 50% gross lucency was observed between the fusion masses; if either of these criteria were met, the patient was deemed pseudarthrosis, both criteria were not required.21,22 All imaging studies were reviewed by a board certified neuroradiologist blinded to the study objective.
Statistical Analyses
The 2-sided t test or Wilcoxon rank-sum test as appropriate was used to compare the means or medians of the 2 groups. For each of the outcome variables, VAS and NDI, repeated measure analysis of variance was used to compare the 2 groups. Fisher exact test was used to assess an association between categorical variables. A P value < 0.05 was considered statistically significant. All analyses were performed with SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
A total of 84 patients were identified who underwent de novo 2-level ACDF: 43 patients received ISP and 41 patients received ASPS. In the ISP group, average patient age was 54.8 ± 8.8 years with 21 men and 22 women. In the ASPS group, average age was 58.1 ± 11.5 years with 23 men and 18 women. There was no statistically significant difference in the patient demographics between the 2 groups (Table 1). The mean follow-up time was 14.1 ± 6.2 months and 20.4 ± 10.5 months for the ISP and ASPS group, respectively.
Baseline characteristics of patients by study group.
In regard to operative details, there was no statistically significant difference in surgical levels, cage height, or estimated blood loss (Table 2). The most common surgical levels were C5-C7 followed by C4-C6 in both groups. The only significant difference between the ISP group and ASPS group during the perioperative period was in time of surgery: ISP took on average 199.6 ± 38.6 minutes whereas ASPS took 178.9 ± 34.7 minutes (P = 0.014).
Intraoperative summary by study group.
Clinical outcomes postoperatively also showed no statistical difference in VAS scores, which at different follow-up times ranged from mean of 4.6 to 5.3 for the ISP group and from 3.2 to 6.5 for the ASPS group (P = 0.432). Similarly, there was no difference (P = 0.108) in the postoperative follow-up NDI scores either with ISP group ranging from a mean of 23.5 to 29.3 and ASPS group from 14.0 to 24.3, as seen in Table 3.
Clinical and radiographic outcomes by study group.
Furthermore, there were no significant differences in postoperative time to fusion between the ISP and ASPS groups. At the proximal surgical level, the ASPS group reached observed radiographic fusion at 6.8 ± 5.4 months and the ISP group took longer with a mean of 8.3 ± 5.5 months. While there was a trend toward ISP having longer duration until fusion at the proximal level, this trend did not reach statistical significance (P = 0.092). For observed duration to radiographic fusion at the distal surgical level, again the ISP group had a longer mean time—8.1 ± 5.5 months—than the ASPS group—7.0±6.2 months—but this was also not statistically significant (P = 0.120). Solid radiographic fusion was observed at both levels in 73.7% of the ISP group and in 84.6% of the ASPS group (P = 0.272).
There was a single case of pseudarthrosis in the ASPS group that did not require further surgical intervention, otherwise the remainders of the patients were deemed stable as noted on dynamic films (Table 4). Three patients in the ISP group and 1 in the ASPS had further surgical intervention unrelated to their initial surgery. One case of long-term dysphagia (>3 months) was reported in each group. Neither groups had any report of implant failures or subsidence requiring additional surgery.
Adverse events by study group.
DISCUSSION
In patients with symptomatic cervical degenerative disc disease, ACDF is an effective operative treatment when nonsurgical treatments fail. An attempt to avoid the potential complications of the traditional ACP, systems designed to be zero-profile, such as the ISP system, were developed. The goal of this study was to evaluate the clinical and radiographic outcomes of patients after 2-level ACDF with ISP vs ASPS. Overall, we found the 2 groups were similar in patient demographics and preoperative status. The only statistically significant difference in perioperative measures was a mean surgery time of approximately 20 minutes longer in the ISP group vs the ASPS group. Postoperative outcomes, including VAS scores, NDI scores, fusion rates, hardware failure, and reports of dysphagia, were similar between the 2 groups as well. This suggests that 2-level ACDF with ISP is similar to ASPS.
However, some spine surgeons have cited possible rigidity inferiority of ISP—the segmented construct involving integrated plate spacer with 2 screws of ISP in comparison to the immediate rigidity provided by traditional ACP construct with 6 screws fixated to a continuous plate spanning the 3 vertebral bodies (Figure)—as a serious concern for its use. Clavenna et al23 performed a biomechanical evaluation of multidirectional rigidity of anterior fixation for 2-level and 3-level ISP and traditional ASPS constructs to evaluate this concern. In the 2-level construct at C4-C6, ISP significantly reduced range of motion (ROM) in flexion-extension by 66.5%, lateral bending by 65.4%, and axial rotation by 60.3% compared to an intact spine.23 This stability is statistically similar to that achieved using ASPS constructs.23 In another cadaveric biomechanical study, there was no difference in ASPS and ISP in ROM reduction in axial rotation and lateral bending in 2-level ACDF; but ASPS did have a statistically significant greater reduction in flexion-extension movement over the ISP.24 Furthermore, Paik et al showed that ASPS decreased ROM in all planes more than ISP in both 2-level and 3-level ACDF in a cadaveric biomechanical study.25 Despite the possibility of less reduction in ROM in ISP, our study found there was no difference in radiographic fusion (P = 0.272) nor was there a clinical difference between ISP and ASPS as described by NDI scores (P = 0.108). It is reasonable to presume that should ISP have actually caused less reduction in ROM, these variables (radiographic fusion and NDI scores) would have been affected. However, it is not a direct correlation by any means and therefore, our conclusion should be taken with particular caution.
Additionally, 2 studies have shown decreased adjacent segment disease (ASD) with ISP vs ASPS in ACDF.26,27 Yang et al performed a meta-analysis of multilevel ISP and ASPS ACDF studies with a minimum of 12 months follow-up, which showed that not only was there a statistically significant decrease in incidence of adjacent segment disease with ISP, there was no difference in clinical outcomes between the groups as represented by NDI scores.27 Our study corroborated this finding of similar postoperative clinical outcomes as having several other studies.26–30 This indicates noninferiority of ISP in comparison to ASPS in regard to postoperative clinical outcomes.
Overall, our study revealed no significant difference in fusion rates between ISP and ASPS in 2-level fusions. Similar conclusions were reached by 2 other studies.31,32 However, our study did reveal a trend toward earlier observed radiographic fusion at the proximal level in the ASPS group in comparison to the ISP group. We suspect the possible delay in fusion may be due to slightly more micromotion in the ISP group compared to ASPS group. However, this was clinically insignificant in our patient population as there were no statistical differences in the postoperative VAS scores and the NDI scores between the 2 groups. Similar to our results, Lee et al noted, in a 1-level ACDF study, that the anchored cage (zero-profile) system provided lower motion stabilization and fusion rates (did not comment on statistical significance) compared to an anterior plating system, but no statistically significant difference in clinical outcome.33 However, in several other studies,26–29 fusion rates were equal between the ISP and ASPS groups, which are consistent with our findings.
Wang et al reviewed clinical efficacy of zero-profile anchored spacer vs ACP technique involving 63 consecutive patients with 1-level or 2-level ACDF.34 They noted similar clinical outcomes between the 2 groups but observed that the zero-profile group had significantly decreased surgical time.34 A similar finding in regard to less operative time was found in the meta-analysis of 2-level ISP ACDF surgeries.35 However, in our cohort, the surgery time for ISP was significantly longer (199.6 ± 38.6 minutes) compared to the ASPS group (178.9 ± 34.7 minutes, P = 0.014). We postulate that this is due to technique differences: our ISP technique requires angled screw placement whereas the technique of Wang et al required insertion of anchoring clips without any preparation.34
Similar to the findings of Wang et al of significantly decreased presence of dysphagia in the ISP group,34 Panchal et al performed a study of single-level ISP vs ASPS and demonstrated that in the immediate postoperative period to 6 months postoperatively, the ISP group had a greater improvement in the Voice Handicap Index.36 Interestingly, we observed contrary results with similar dysphagia rates between the 2 groups: one case of long-term dysphagia (>3 months) was reported in both the ISP group and the ASPS group. Lu et al also came to the same conclusion in their meta-analysis on 2-level ISP vs ASPS ACDF,32 as did a recent randomized control trial for 2-level ISP vs ASPS demonstrating no statistically significant difference in dysphagia rate in the short term.37 Scholz et al did show a trend toward ISP having decreased dysphagia rate at 3 months postoperatively, however, this did not reach statistical significance (P = 0.078).37 These conflicting results indicate the need for larger randomized control trials for multilevel ISP constructs.
We acknowledge that there are several limitations to our study inherent to its retrospective nature, including data acquired only by chart review. There is selection bias, even though the groups represent similar cohorts, as the individual attending surgeons did either ISP or ASPS but did not perform both techniques. Another limitation that involved both groups was the lack of complete clinical data on all patients, making correlation to radiographic data difficult. In regard to fusion status, determining by x-ray only has its limitations as well. To address these weaknesses, a large prospective multicenter randomized control study with long-term follow-up is necessary.
CONCLUSION
The ISP system for 2-level ACDF compared to traditional ASPS provides comparable clinical and radiographic outcomes at 2 years, specifically no difference in the long-term-reported dysphagia rate. However, there may possibly be an earlier observed radiographic fusion in the ASPS group.
Acknowledgments
Footnotes
Funding This study was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant #UL1 TR001860.
Disclosures Dr. Panchal reports grants and personal fees from Globus and a patent pending for an anterior cervical plate. Dr. Klineberg reports personal fees from Depuy Synthes. All other authors report no conflicts of interest in regard to this submitted work.
Institutional Review Board This study was approved by the Institutional Review Board of the University of California Davis.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.