


Abstract
Study Design A meta-analysis of 89 randomized prospective, prospective, and retrospective studies on spinal endoscopic surgery outcomes.
Objective The study aimed to provide familiar Oswestry Disability Index (ODI), visual analog scale (VAS) back, and VAS leg effect size (ES) data following endoscopic decompression for sciatica-type back and leg pain due to lumbar herniated disc, foraminal, or lateral recess spinal stenosis.
Background Higher-grade objective clinical outcome ES data are more suitable than lower-grade clinical evidence, including cross-sectional retrospective study outcomes or expert opinion to underpin the ongoing debate on whether or not to replace some of the traditional open and with other forms of minimally invasive spinal decompression surgeries such as the endoscopic technique.
Methods A systematic search of PubMed, Embase, Web of Science, and the Cochrane Central Register of Controlled Trials from 1 January 2000 to 31 December 2019 identified 89 eligible studies on lumbar endoscopic decompression surgery enrolling 23,290 patient samples using the ODI and VAS for back and leg pain used for the ES calculation.
Results There was an overall mean overall reduction of ODI of 46.25 (SD 6.10), VAS back decrease of 3.29 (SD 0.65), and VAS leg reduction of 5.77 (SD 0.66), respectively. Reference tables of familiar ODI, VAS back, and VAS leg show no significant impact of study design, follow-up, or patients’ age on ES observed with these outcome instruments. There was no correlation of ES with long-term follow-up (P = 0.091). Spinal endoscopy produced an overall ODI ES of 0.92 extrapolated from 81 studies totaling 12,710 patient samples. Provided study comparisons to tubular retractor microdiscectomy and open laminectomy showed an ODI ES of 0.9 (2895 patients pooled from 16 studies) and 0.93 (1188 patients pooled from 5 studies). The corresponding VAS leg ES were 0.92 (12,631 endoscopy patients pooled from 81 studies), 0.92 (2348 microdiscectomy patients pooled from 15 studies), and 0.89 (1188 open laminectomy patients pooled from 5 studies).
Conclusion Successful clinical outcomes can be achieved with various lumbar surgeries. ESs with endoscopic spinal surgery are on par with those found with open laminectomy and microsurgical decompression.
Clinical Relevance This article is a meta-analysis on the benefit overlap between lumbar endoscopy, microsurgical decompression, laminectomy, and lumbar decompression fusion.
Level of Evidence 2.
INTRODUCTION
Endoscopic spinal surgery is on the rise, and in some countries has become the standard of care in the treatment of lumbar herniated disc and spinal stenosis in the foramen and lateral recess.1 Within the last 3 years alone, there has been a surge of publications coming out of China,2–54 South Korea,42,55–78 and other Asian countries,79–87 where spinal endoscopy has replaced microsurgical dissection techniques. Many of these articles focus on technological innovations with the procedure. Clinical benefits over traditional translaminar lumbar decompression techniques are often demonstrated in the context of a new instrument or a new technology, which is used to expand the clinical indications for endoscopic spinal surgery. While the transforaminal approach has been the “workhorse” endoscopic technique as pioneered by the senior author of this article some 30 years ago,88–95 alternatives such as the interlaminar,7,9,21,24,41,54,59,96,97 the full-endoscopic, and the uniportal biportal endoscopic (UBE)61,67,98,99 techniques have recently been popularized to promote one method over another. At least on the surface, it may appear to the novice to endoscopic spinal surgery attempting to organize the available clinical information that some authors may be pushing biased agendas by attempting to exploit some perceived procedural advantages and disadvantages to make a case for their preferred spinal surgery technique. One example of this trend is the sheer number of procedural acronyms—YESS (Yeung endoscopic spine system),12,26,90,95,100–104 TESSYS (transforaminal endoscopic spine system),105–110 PELD (percutaneous endoscopic lumbar discectomy),14,19,25,36,54,56,111 SED (selective endoscopic discectomy), BELD (biportal endoscopic lumbar decompression),112 ULBD (unilateral laminotomy with bilateral decompression),113 PBED (percutaneous biportal endoscopic decompression),74 PTED (percutaneous transforaminal endoscopic discectomy),114 UBE (unilateral biportal endoscopy),61,67,98,99 BEIS (intervertebral foramen endoscopy),115 TESSYS (transforaminal endoscopic spine system)-ISEE (Interlaminar endoscopic 270° spinal canal decompression),116 so on—to list the most commonly used terminology. These acronyms are being proposed to improve the relevance of a new version of endoscopic and minimally invasive spine surgery that supposedly improves clinical outcomes. But does it, though, and which of these procedural variations of lumbar spinal stenosis surgery are clinically relevant? The Arbeitsgemeinschaft für Osteosynthesefragen-Spine has proposed an evidence-oriented classification system to meliorate this situation somewhat and to moderate the debate but has not presented any clinical evidence to back it up.117
The authors of this study attempted to grade the clinical evidence on lumbar spine surgeries directed at soft tissue and bony spinal stenosis including modern spinal endoscopy. Many of these studies including control arms consist of traditional translaminar microsurgical and open decompression. Therefore, the authors qualitatively graded and quantitatively analyzed the clinical evidence on the endoscopic literature including that of the respective control groups published thus far by performing a meta-analysis on commonly used numerical spinal surgery outcome instruments: the Oswestry Disability Index (ODI),118–121 and the visual analog scale (VAS)122 for back and leg pain. While many published meta-analyses attempted to demonstrate clinical superiority of the endoscopic spinal surgery outcomes compared to traditional translaminar microsurgical decompression techniques by selecting a few high-quality studies and without reporting the actual effect size (ES) numbers,8,22,34,50,59,123–127 the authors of this article took a different approach to delineate the clinical relevance of procedural variations and technology advances in minimally invasive and endoscopic spinal surgery and the mode of studying them. Instead of performing a narrow focus meta-analysis based on a few prospective or randomized prospective, or well-controlled cross-sectional retrospective studies, this team of authors was interested in a broad investigation of the ESs associated with reported clinical outcome improvements with traditional translaminar and lumbar endoscopic spinal surgery by extracting and analyzing the ODI and VAS means, SDs, and number of patients in each study. Therefore, we performed additional subcategory, modifier, and wave analysis to cross-tabulate ES extractions by the length of follow-up, patients’ age, the indication for surgery, the type of minimally invasive spinal surgery performed, the publication year, and the type of study design employed by the authors of the original studies. Ultimately, the authors intended to create a reference table of ES with the various minimally invasive spinal surgery to employ it in the comparative evaluation and discussion of their clinical merits.
MATERIALS AND METHODS
Search Strategy and Study Selection
The authors were interested in analyzing the ES data reported for commonly used numerical clinical outcome instruments including the ODI,118–121 and the VAS122 for back and leg pain with lumbar endoscopic decompression procedures for soft tissue and bony stenosis. Therefore, we performed a meta-analysis of clinical studies on endoscopic decompression for lumbar herniated disc and spinal stenosis employing preferred reporting items for systematic reviews and meta-analyses guidelines.128–131 For this purpose, the authors searched the English literature on PubMed, Embase, Web of Science, and the Cochrane Database from 1 January 2000 to 31 December 2019 using “lumbar” and “herniated disc” or ‘‘spinal stenosis’’ and ‘‘endoscopic” and ‘‘ODI” and ‘‘VAS” as keywords. Three independent researchers (KUL, JFR, and ATY) contributed their literature searches and also reached consensus with the other coauthors if there were any discrepancies in the interpretation of the selected studies.
Inclusion Criteria and Data Extraction
The literature search was aimed at finding studies which included analysis of endoscopic spinal surgery outcomes reported on patients suffering from symptoms related to lumbar herniated disc, and foraminal or lateral recess stenosis utilizing ODI and VAS for back and leg pain. This literature search included straightforward cross-sectional retrospective, prospective single treatment group, or randomized prospective multitreatment arm study designs comparing endoscopic, with other minimally invasive spinal surgery techniques (MISST) including tubular retractor, and others. Retrieved studies were further stratified by the type of endoscopic MISST access to the neural elements including transforaminal, interlaminar, or combinations, or variations of these techniques. Case reports, review articles, letters to the editor, editorials, short-term reports, and nonclinical studies, such as biomechanical or cadaveric studies were excluded. Each study discovered during the extensive literature search performed by the authors was categorized as retrospective, prospective single treatment group, or randomized prospective multitreatment arm cohort studies. Their respective quality was assessed by the authors via consensus discussions to resolve any discrepancies in study quality assessment by evaluating the risk of bias (ROB) using the ROB assessment tool for controlled nonrandomized observational cohort studies, and the ROB tool for randomized controlled trials.132
Statistical Analysis
The purpose of our meta-analysis was to determine and compare the ES of the clinical improvement of patients treated with the various endoscopic spinal decompression surgery techniques for herniated disc, central, lateral recess, and foraminal stenosis on the basis of the reported numerical clinical outcome instruments. For this purpose, the authors extracted the reported data for ODI, VAS back, and VAS leg at baseline and postoperatively at final follow-up. Only studies which reported the mean, the SD, and the sample size preoperatively and postoperatively were included in this meta-analysis for the ES calculation using random ES models. The authors considered other ways of calculating the ES from reported t values or significance levels less accurate with the potential of underestimating the ES and did not employ them.
Clinical outcome data extracted from the articles included in this meta-analysis were means and SD of the VAS back, the VAS leg, and the ODI. The ES of postoperative improvements was calculated on the basis of the number of enrolled study patients available at last follow-up using Cohen d analysis. We used Prometa3 version 3.0 for the meta-analysis by creating a meta-analysis database of the included studies by recording the first study author and up to 2 additional coauthors, the year of publication, the study patients’ mean age, and of the preoperative baseline and the postoperative value of the 3 numerical outcome variables at final available follow-up. Studies comparing multiple treatments were categorized by comparisons of “endoscopy” vs “microsurgical” decompression, laminectomy, and variations of these procedures with and without fusion. Additional moderators used in the analysis were the study design (retrospective, prospective, and randomized prospective), the indication for surgery (herniated disc radiculopathy, stenosis claudication, and discogenic pain), the type of MISST (endoscopy, open laminectomy, and tubular microdiscectomy), and, if employed, the type of endoscopic (transforaminal outside-in, transforaminal inside-out, interlaminar, combined outside-in and interlaminar, or biportal UBE endoscopy). The calculated ESs, lower limit (LL), upper limit (UL), the Higgins I 2 statistic of heterogeneity (I 2), variance (V), SE, number of patients, and the significance level (sig) of 95% CI were tabulated separately for ODI, VAS back, and VAS leg. The underlying average reduction of ODI, VAS back, and VAS leg was compared to the reported and calculated minimal clinically important difference (MCID) data—3.0 for VAS leg and VAS back and 15 for ODI.83,133–137 Furthermore, the extracted mean ODI, VAS back, and VAS leg from each individual study were weighted by the inverse of the variance for each outcome instrument. The data heterogeneity was examined by Cochran Q test and the Higgins I 2 statistic with an I 2 threshold of greater than 50% being considered as sufficient. Funnel plots (SE vs ES) were visually assessed for evidence of publication bias and by calculating the P value (1-sided) for Egger intercept using the Prometa3 software, version 3.0 (Internovi, 2015). IBM SPSS statistics version 26.0 was used for area-plot analysis of ES vs SE to graphically display the extent of the overlap in postoperative surgical decompression benefit.
RESULTS
Initial Search Results
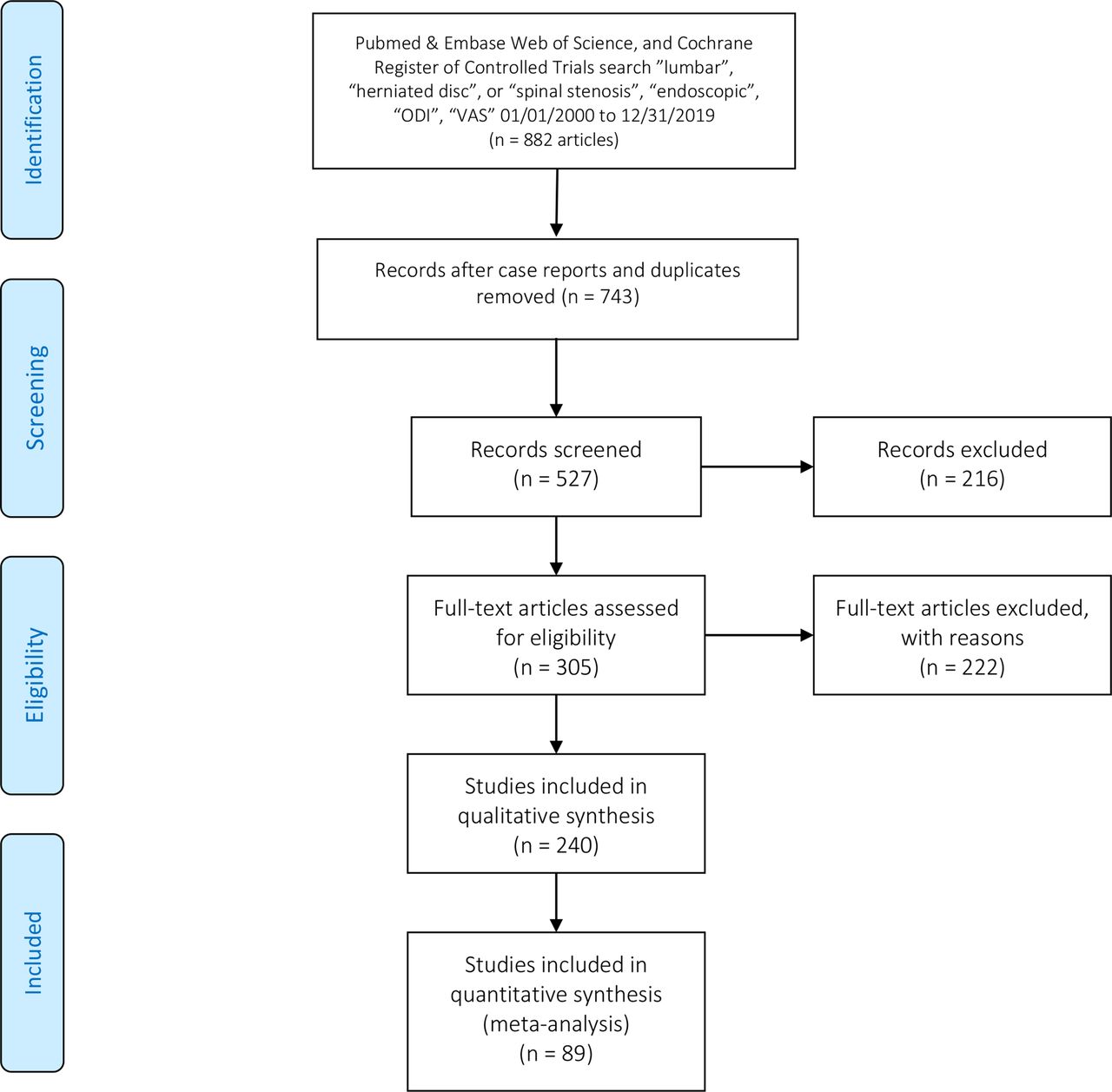
The initial screening literature search using the keywords “lumbar” and “herniated disc” or ‘‘spinal stenosis’’ and ‘‘endoscopic*” and ‘‘ODI” and ‘‘VAS” as subject headings identified 882 studies in PubMed, Embase, Web of Science, and the Cochrane Central Register of Controlled Trials. Among these 882 studies, duplicates, case reports, review articles, letters, technical notes, or patents as well as studies not reporting the average mean, SD of ODI and VAS scores, and number of patients or length of follow-up were excluded. The remaining 89 eligible studies were subjected to a full-text review. In attempt to compare short-term and long-term ES, study analysis was further stratified into short-term—53 studies with less than 2-year follow-up (Table 1)1,4,5,7,9,11,13,18–20,23–28,36,38,40,42,43,45,51,56,66,68,74,78,111–114,116,138–156—and long-term follow-up (36 studies) with a minimum of 2 years or longer follow-up (Table 2).10,30,33,41,46,49,52,53,55,60,67,71,75,76,97,157–175 The details of the preferred reporting items for systematic reviews and meta-analyses study selection process are summarized in Figure 1.

Preferred reporting items for systematic reviews and meta-analyses flow chart of selected lumbar spinal stenosis studies found in PubMed, Embase, Web of Science, and in the Cochrane Central Register of Controlled Trials using the keywords “lumbar” and “herniated disc” or ‘‘spinal stenosis’’ and ‘‘endoscopic” and ‘‘ODI” and ‘‘VAS” as subject headings analyzed to compare effect sizes of endoscopic to traditional translaminar decompression with and without fusion. ODI, Oswestry Disability Index; VAS, visual analog scale.
List of short-term (<2-year follow-up) lumbar decompression studies included into the effect size meta-analysis comparing endoscopic to other translaminar decompression surgeries with brief summary of study highlights.
List of long-term (>2-year follow-up) lumbar stenosis decompression studies included into the effect size meta-analysis comparing endoscopic to other translaminar decompression surgeries with brief summary of study highlights.
Meta-Analysis Results
The ODI, VAS back, and VAS leg data obtained from the collective analysis of the 23,290 samples extracted from 89 articles with 112 study entries considering multiple treatment arms revealed an overall ES of 0.9 using a random effects model with an LL of 0.89 and UL of 0.91 and I 2 98.49. The weighted regression analysis for age vs overall ES showed no significant correlation between these 2 variables (P = 0.539). The weighted regression analysis for follow-up vs overall ES showed a significant correlation between these 2 variables (P = 0.014). The majority of the 89 studies only provided short postoperative follow-up times: under 12 months in 17 study entries, 1 year in 27 study entries, under 24 months in 23 study entries. Long-term follow-up was reported by 36 articles of which, 18 study entries had follow-up of 2 years, 17 study entries had follow-up data between 2 and 4 years, and another 10 study entries over 60 months with the longest 2 follow-up study entries running for 74.8 and 76.2 months. However, there was no statistically significant difference in ES on analysis of variance (ANOVA) Q testing between short-term and long-term follow-up studies (P = 0.091). A similar analysis of ES vs publication year using random effects model showed a trend toward increasing ES since 2010 although statistically not significant (P – 0.186) presumably representing clinical treatment improvements due to technology advancements. Publication bias analysis showed overall observed ES as 0.92 (ODI), 0.8 (VAS back), and 0.92 (VAS leg) with a significant improvement (P < 0.0001 for all 3 outcome instruments) on Egger linear regression with an intercept = −0.82 and t = −0.51 for ODI, an intercept = 1.62 and t = 0.74 for VAS back, and an intercept = 0.39 and t = 0.25 for VAS leg. Seventy-two of the 89 studies included in this meta-analysis were retrospective studies. Twelve studies were prospective, and another 5 studies were randomized prospective clinical trials both of which had multiple treatment arms. Twenty-four of the 36 studies included in the meta-analysis with longer than 2-year follow-up were retrospective studies and were estimated to have a high ROB. This was reflected in the asymmetric funnel plot with a significant number of studies falling outside the expected area of SE vs ES plot suggesting that the bias in the underlying studies put the authors’ overall meta-analysis at moderate ROB.
Meta-Analysis by Modifiers
The impact of study design on ES was minimal and statistically not significantly different among retrospective, prospective, and randomized prospective trials (Table 3). The mean ODI analysis on 17,921 patients’ samples showed ES of 0.92 for retrospective, ES of 0.92 for prospective, and ES of 0.91 for randomized prospective trials (P = 0.925). The mean VAS back analysis on 8002 patients’ samples also did not show any statistically significant impact of study design on ES: ES of 0.8 for retrospective, ES of 0.6 for prospective, and ES of 0.81 for randomized prospective trials (P = 0.204). Similarly, the mean VAS leg analysis on 17,295 patients’ samples also did not show any statistically significant impact of study design on ES: ES of 0.91 for retrospective, ES of 0.93 for prospective, and ES of 0.88 for randomized prospective trials (P = 0.575).
Analysis of effect size, heterogeneity, and ANOVA testing of difference by study type.
The indication for surgery was another modifier studied in our meta-analysis (Table 4). Extracted ODI means analysis showed a higher overall ES for endoscopic decompression of spinal stenosis-related claudication symptoms (ES = 0.95; 1638 patients pooled from 14 studies) than for herniated disc (ES = 0.92; 3520 patients pooled from 22 studies) or discogenic back pain (ES = 0.91; 216 patients pooled from 2 studies) at statistically insignificant level (P = 0.094). Moreover, extracted means analysis for VAS back (P = 0.074) and VAS leg (P = 0.74) did not produce any significant difference in overall ES for either of these 3 indications (Table 4). Another question of interest to the authors was the impact of long-term vs short-term follow-up on the overall ES for the 3 clinical outcome instruments measuring benefit from the lumbar endoscopic spine surgery for indications investigated (Table 5). The highest overall ES numbers were calculated at 2-year follow-up for VAS leg (ES = 0.94; P < 0.0001; based on total 17,295 patient samples) and VAS back (ES = 0.9; P < 0.0001; based on total of 8002 patient samples pooled from 55 studies) at a statistically significant level. The overall ES based on the extracted ODI means from a total of 17,543 patients pooled from 108 study entries at 2-year follow-up and longer was ES = 0.92 without statistical significance (P = 0.678; Table 5).
Analysis of effect size, heterogeneity, and ANOVA testing of difference by surgery indication.
Analysis of effect size, heterogeneity, and ANOVA testing of difference by length of follow-up.
Using the type of decompression as a modifier in calculating the overall ES in endoscopic spinal decompression surgeries allowed to compare postoperative improvements in ODI, VAS back, and VAS leg to those achieved with other types of decompression surgeries as they were used in multiarm comparison studies (Table 6). Spinal endoscopy produced an overall ODI ES of 0.92 extrapolated from 81 studies totaling 12,710 patient samples. Tubular retractor microdiscectomy produced smaller ODI ES (ES = 0.9; 2895 patient samples pooled from 16 studies) than open laminectomy (ES = 0.93; 1188 patient samples from 5 studies). The highest ODI ES was observed with endoscopically assisted minimally invasive fusions with percutaneous posterior supplemental pedicle screw instrumentation (ES = 0.95; 166 patient samples pooled from 4 studies; Table 4). Similar, VAS leg ESs were observed with endoscopy (ES = 0.92; 12,631 patient samples pooled from 80 studies) with spinal endoscopy, with small and statistically insignificant (P = 0.592) ES difference to the other MISST procedures listed in Table 6. The VAS back ESs were smaller without any statistically significant difference between spinal endoscopy and the other various MISSTs that were evaluated in the individual multitreatment arm comparison studies (P = 0.4167; 8002 patient samples from 55 studies; Table 6). The postoperative benefit overlap is graphically illustrated in Figure 2. The largest overall ES with the smallest SE was observed with laminectomy, tubular retractor microdiscectomy, and with endoscopically assisted MISST fusion and standalone endoscopic fusion surgery (P = 0.022). There was a wider scatter between SE and ES combinations with spinal endoscopy as a whole likely graphically representing variations in surgeon skill level, indication for surgery, and patient selection criteria (Figure 2).

Meta-analysis regression plot of effect size (ES) vs standard error stratified for the type of decompression surgery using random effects model showed substantial overlap in the plotted relationship between these procedures and, hence, clinical benefit with all lumbar decompression methods some of which were with fusion including endoscopy with statistical significance in spite of the underlying risk of moderate publication bias: endoscopic-assisted minimally invasive surgery fusion - 3 studies, ES = 0.94, endoscopy - 84 studies, ES = 0.9, open laminectomy - 6 studies, ES = 0.89, and tubular microdiscectomy - 21 studies, ES = 0.89, P = 0.022.
Analysis of effect size, heterogeneity, and ANOVA testing of difference by surgery type.
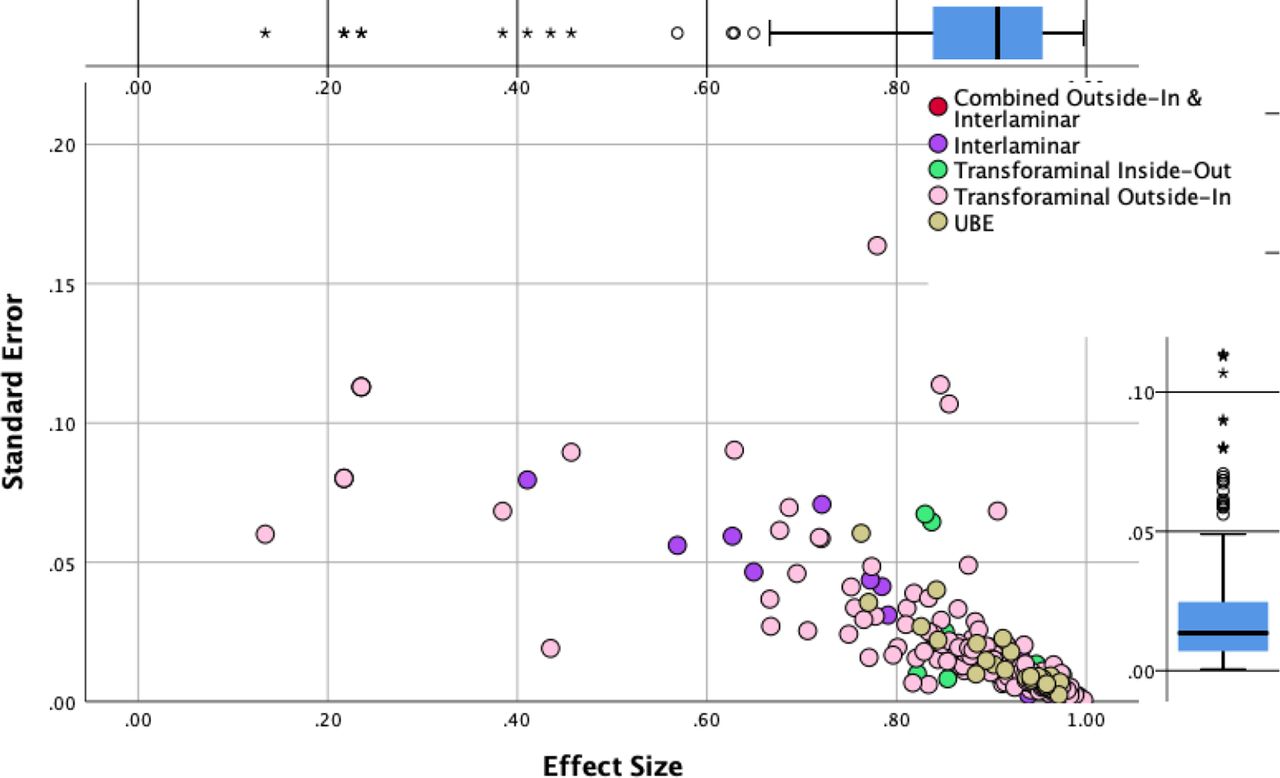
The ES comparison using the type of endoscopy as a modifier in the meta-analysis on 13,184 patient samples pooled from 81 studies showed statistically significant differences (P < 0.0001) between transforaminal outside-in (ODI ES = 0. 9), transforaminal inside-out (ODI ES = 0.9), interlaminar (ODI ES = 0.96), and the combination of the transforaminal outside-in and interlaminar (ODI ES = 0.98), and UBE (ODI ES = 0.93; Table 7). Similar ES differences were calculated for the VAS leg on a total of 13,105 patients pooled from 85 studies at statistical significance level (P < 0.00001) comparing outcomes between transforaminal outside-in (VAS leg ES = 0.91), transforaminal inside-out (VAS leg ES = 0.89), interlaminar (VAS leg ES = 0.93), and the combination of the transforaminal outside-in and interlaminar (VAS leg ES = 0.97), and UBE (VAS leg ES = 0.93; Table 7). Such differences were not statistically significant for the VAS back outcome means obtained on a total of 5134 patients pooled from 37 studies (Table 7). The statistically significant postoperative benefit overlap is graphically illustrated in Figure 3 (P = 0.001). The largest ESs with the smallest SEs were observed with the combined outside-in and interlaminar technique, the transforaminal inside-out, and UBE technique. The widest scatter was seen with the transforaminal outside-in technique.

Meta-analysis area plot of effect size (ES) vs standard error using random effects model showed substantial overlap in the plotted relationship between these 2 variables and, hence, clinical benefit with all endoscopic lumbar decompression methods in spite of the underlying risk of moderate publication bias: transforaminal outside-in with combined interlaminar approach - 1 study, ES = 0.97, uniportal biportal endoscopy (UBE) - 6 studies, ES = 0.92, interlaminar approach - 23 studies, ES = 0.93, transforaminal inside-out approach - 2 studies, ES = 0.89, and transforaminal outside-in approach - 54 studies, ES = 0.89, with statistically significant ES differences between these procedures (P < 0.001).
Analysis of effect size, heterogeneity, and ANOVA testing of difference by type of endoscopy.
Forest Plot Analysis of Long-Term Studies
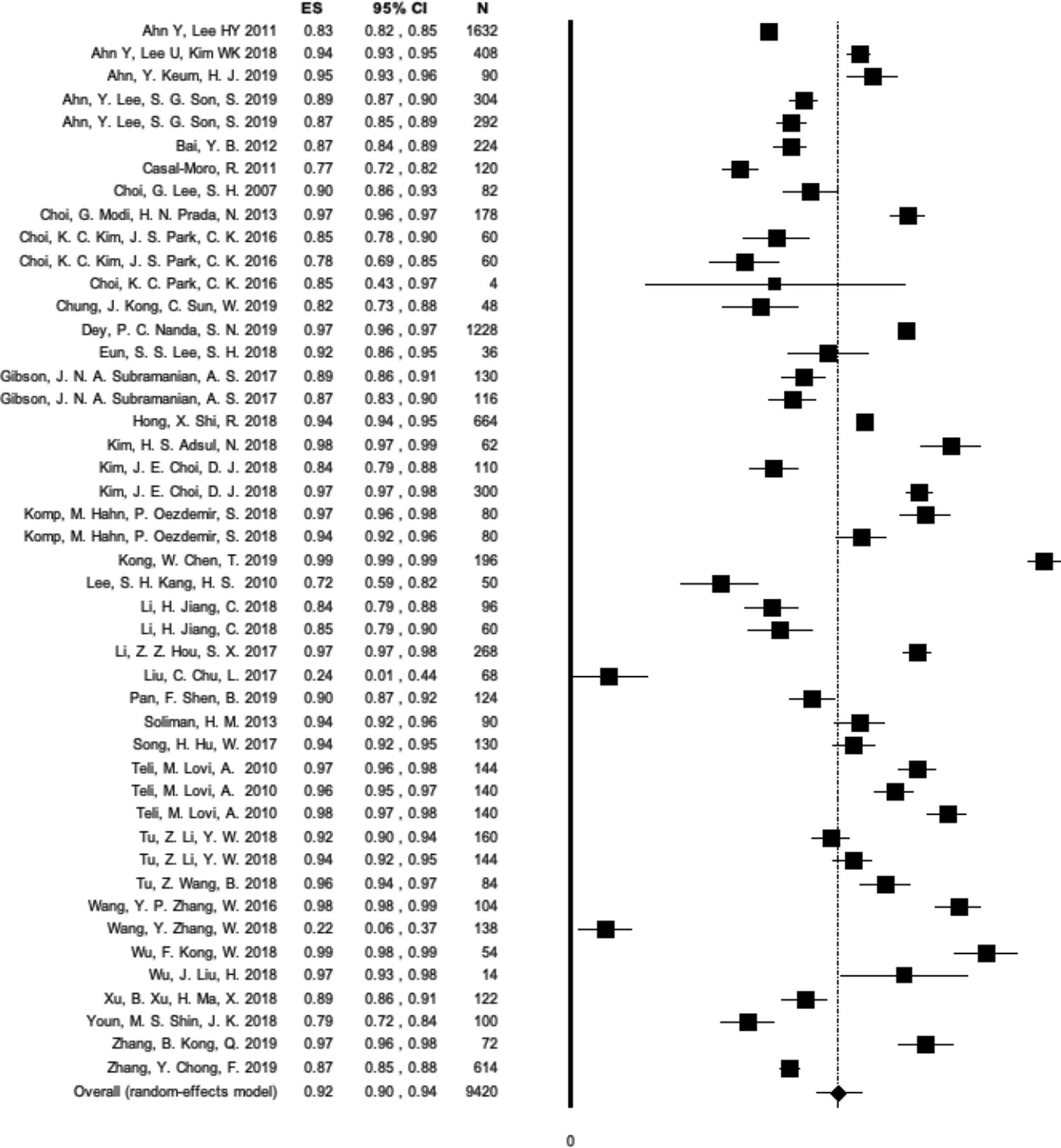
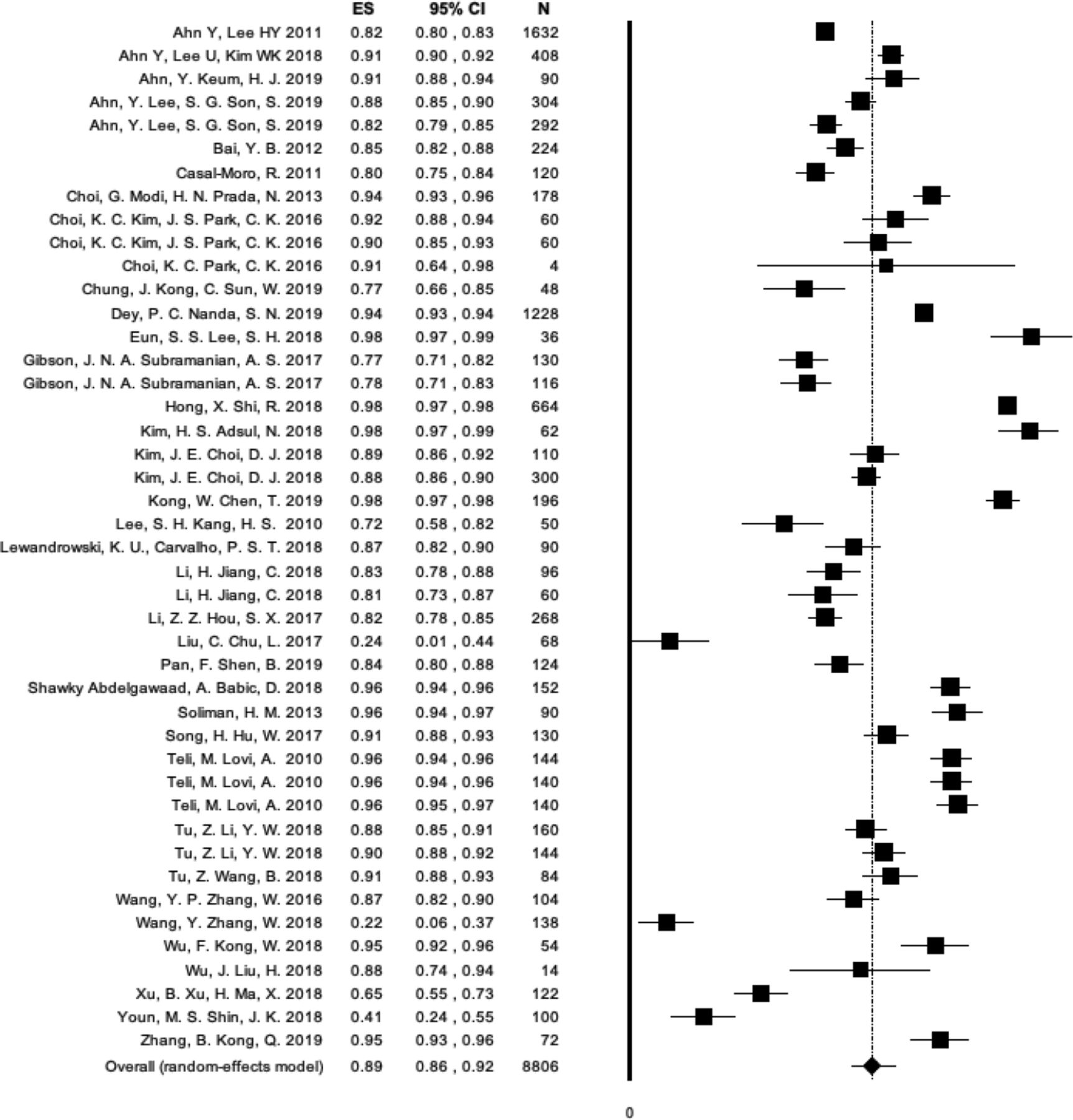
Since the ES analysis suggested a significant difference when studied by follow-up, the authors performed a visual forest plot analysis of the ESs for the extracted means of ODI, VAS back, and VAS leg. There were 46 long-term study entries which reported ODI with a minimum of 2 years or longer. The overall ES for ODI was 0.92 with an LL of 0.9, and a UL of 0.94 calculated from the total of 9420 patient samples (Figure 4). In comparison, there were 26 studies which reported VAS back with a minimum of 2 years or longer follow-up. The overall ES for VAS back was 0.71 with an LL of 0.61, and a UL of 0.81 calculated from the total of 4926 patient samples (Figure 5). Another 44 studies reported VAS leg with a minimum of 2 years or longer follow-up. The overall ES for VAS leg was 0.71 with a lower 95% CI limit of 0.61 and a UL of 0.81 calculated from the total of 4926 patient samples (Figure 6).

Forest plot of effect sizes (ESs), 95% CI, and the number of patients enrolled in each individual endoscopic spinal surgery study (N) calculated for the 46 study groups which reported Oswestry Disability Index with a minimum of 2 y or longer follow-up listed in alphabetical order according to the first author’s name. The number of individual study patients is represented by the size of the symbol. The overall ES was 0.92 with a lower 95% CI limit of 0.9, and an upper limit of 0.94 calculated from the total of 9420 patient samples enrolled in these studies.
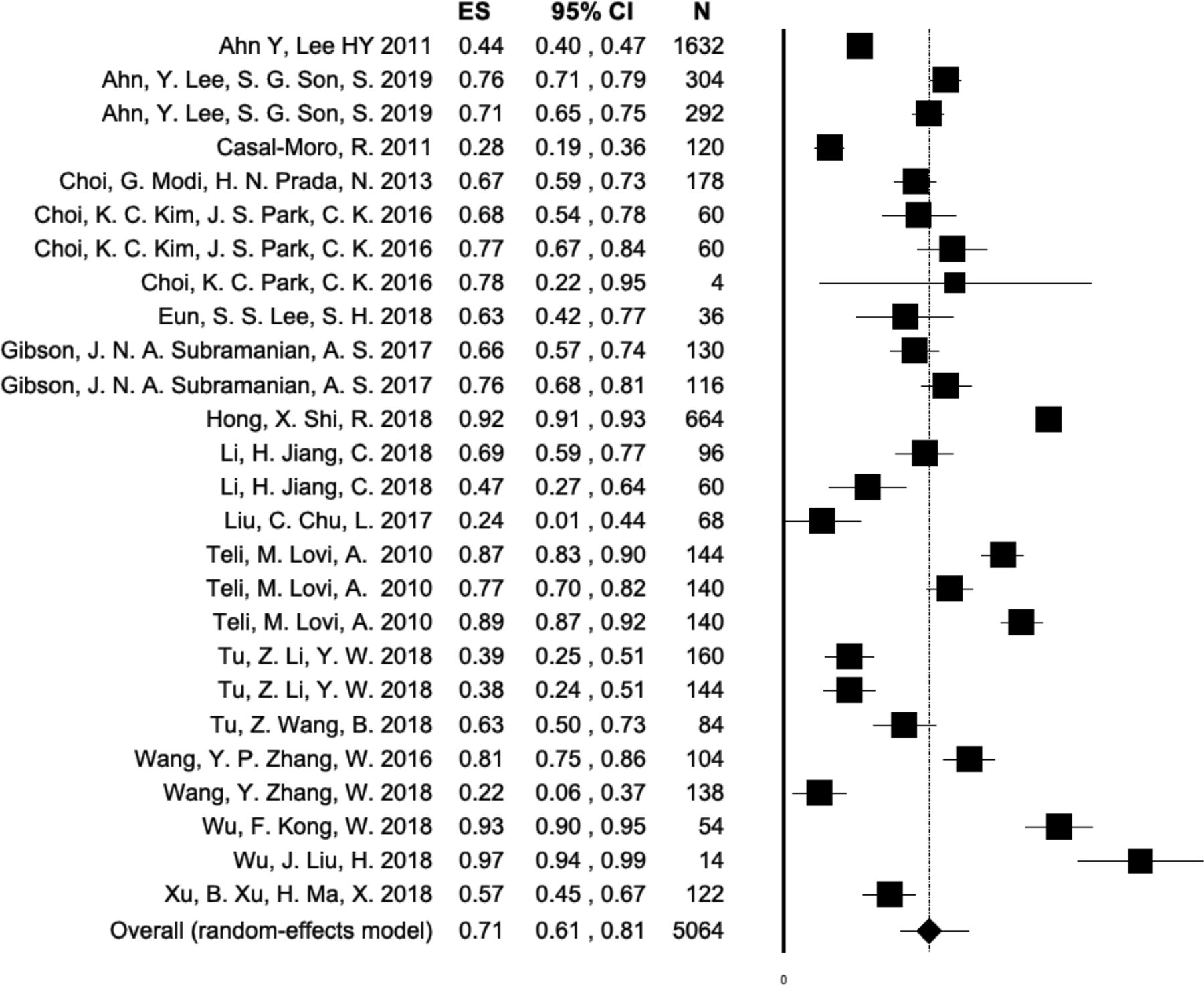
Forest plot of effect sizes (ESs), 95% CI, and the number of patients enrolled in each individual endoscopic spinal surgery study (N) calculated for the 26 study groups which reported visual analog scale back with a minimum of 2 y or longer follow-up listed in alphabetical order according to the first author’s name. The number of individual study patients is represented by the size of the symbol. The overall ES was 0.71 with a lower 95% CI limit of 0.61, and an upper limit of 0.81 calculated from the total of 4926 patient samples enrolled in these studies.
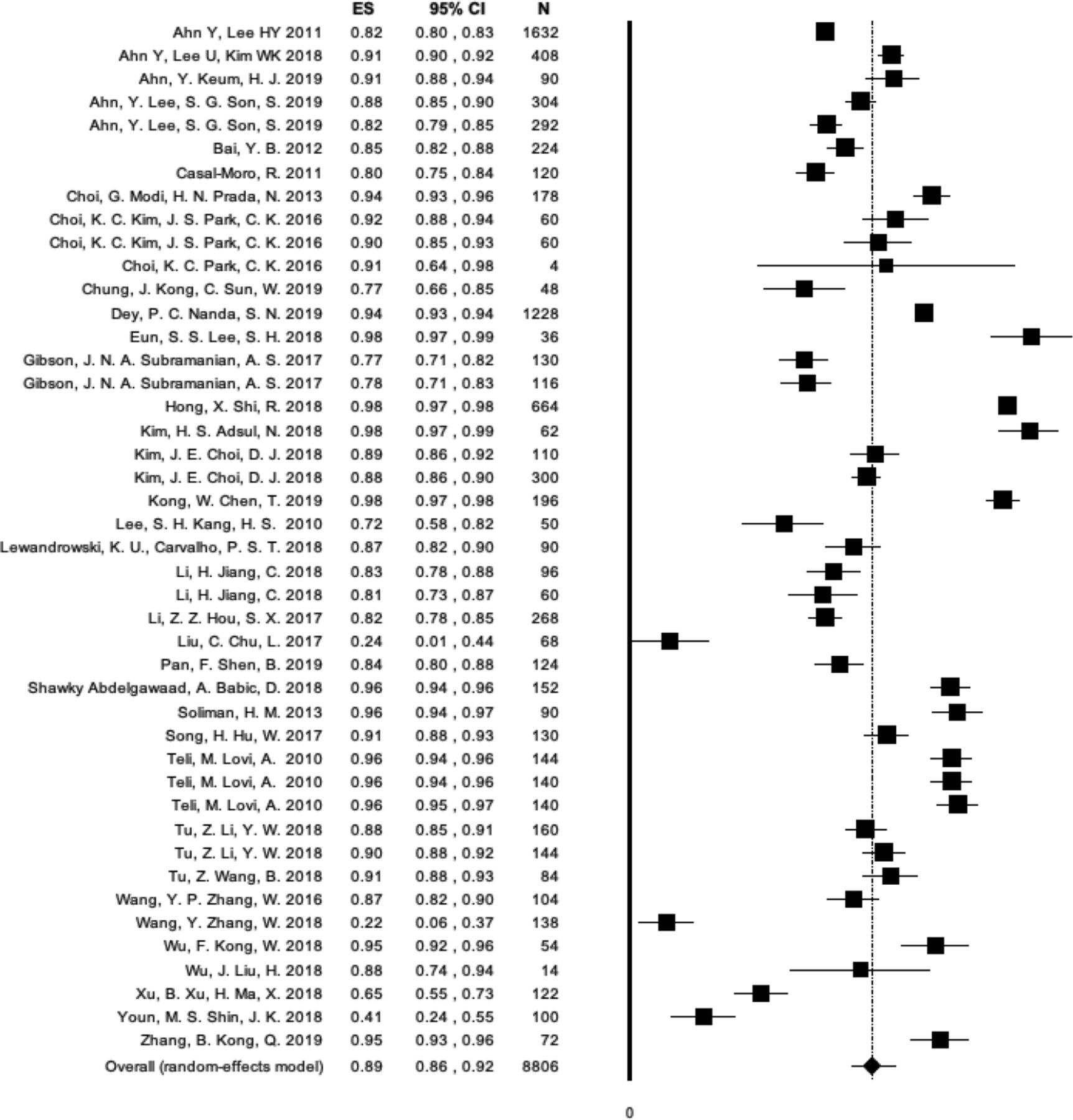
Forest plot of effect sizes (ESs), 95% CI, and the number of patients enrolled in each individual endoscopic spinal surgery study (N) calculated for the 44 study groups which reported visual analog scale leg with a minimum of 2 y or longer follow-up listed in alphabetical order according to the first author’s name. The number of individual study patients is represented by the size of the symbol. The overall ES was 0.89 with a lower 95% CI limit of 0.86, and an upper limit of 0.92 calculated from the total of 8806 patients enrolled in these studies.
Individual Studies Results and MCID
The meta-analysis on the 36 long-term studies showed the following mean preoperative baseline numbers: ODI 59.34 (SD 12.67), VAS back 4.90 (SD 1.89), and VAS leg 7.22 (SD 1.90), respectively. The overall improvements after endoscopic surgery were: ODI reduction of 46.25 (SD 6.10), VAS back reduction of 3.29 (SD 0.65), and VAS leg reduction of 5.77 (SD 0.66), respectively. These ODI reductions are the equivalent of 3 times the MCID for endoscopy.176 The VAS leg reduction was 2 times as high as the reported MCID,176 and the VAS back reduction was on the order of the reported MCID.83,177 The mean percent change of ODI, VAS back, and VAS leg at minimum 2-year follow-up or longer after the endoscopic decompression was 77.94% (SD 10.28%), 67.14% (SD 13.26%), and 79.71% (SD 9.14%), respectively.
DISCUSSION
The authors of this meta-analysis took a broad approach to extract ES data from original studies on the various types of minimally invasive spinal stenosis surgeries to afford the reader the ability to understand their clinical benefit concerning indication for surgery and burden to the patient in an across-the-board normalized comparison. Highlighting differences in outcomes between endoscopic and other forms of minimally invasive (MISST) and traditional open spinal surgery techniques by reporting the ES has several advantages to reporting statistical significance in group comparison tests. The ES calculation emphasizes the size of the difference between the various treatment groups rather than confounding it with sample size.178 Although the ES determination is straightforward—for example, it can be calculated by subtracting the means of the control group from the means of the experimental group and divide it by the SD— ES is rarely used in the discussion of clinical outcomes between various treatments.179 However, it can be highly useful as a measure of overlap between the various lumbar stenosis surgeries. It is a form of data interpretation the authors employed in this study to illustrate the clinical benefit of the various open, minimally invasive, and endoscopic lumbar spinal stenosis surgeries to patients and all other stakeholders involved in the delivery of modern spine care.
We chose the meta-analysis approach to calculating the ESs since it overcomes the common problem of not knowing the SD in the population from which the different treatment groups came from by estimating it through pooling data from the treatment groups of various studies. The authors also expected, based on their collective clinical experience, substantial overlap in terms of clinical benefit of the different endoscopic surgeries. Ultimately, this overlap of clinical benefit was confirmed by the area plots of ES vs SE (Figures 2 and 3). The ES determination was employed by the authors to handle this well-known clinical situation best since this overlap could be conceptualized as the probability analysis by the surgeon to accurately choose the most effective of the various lumbar stenosis surgeries for each patient regardless of whether endoscopic, MISST, or traditional open surgery based on the type of painful pathoanatomy, the clinical context of the patient’s relevant symptoms at the time when the spine care is delivered, and the surgeon’s bias toward a preferred technique based on his or her training, experience, and skill level.180 The impact of skill level was most likely apparent with the transforaminal outside-in technique where the widest spread of ES vs SE was seen (Figure 3). In other words, when attempting to compare clinical outcomes with the various endoscopic and other MISST techniques one is entering a gray zone where many confounding factors impacting clinical outcomes may play out but where identifying the best performing treatment for a certain clinical indication may still be possible at a high probability in spite of substantial overlap in clinical outcomes. While it is obvious that the reported ESs ranging from 0.71 to 0.97 derived from preoperative and postoperative disability data (ODI, VAS back, and VAS leg) extrapolated by the authors from a total of 89 studies were large,181 which represented multiple of the reported MCID,83,177 and without dispute justify the use of the endoscopic and other forms of MISST to treat symptoms related to herniated disc and spinal stenosis in the lateral recess and the foramen, a familiar data set of ESs with these procedures—to the authors’ best knowledge—has not been published. Filling this knowledge gap with the many types of endoscopic spinal surgeries, as exemplified by the long list of acronyms noted in the introduction, was the primary motivation of this team of authors to employ this broad rather than a narrow focus meta-analysis approach.
Employing the inclusion and exclusion criteria stated in the method section, the authors’ meta-analysis was based on studies, most of which were published within the last 3 years, but rarely older than 10 years, thus, likely representing the recent technology advancements facilitating the outcomes of increasing ES—without statistical significance—reported herein. As a result, ESs were calculated based on extracted ODI, VAS back, and VAS leg data extrapolated from a vast number of 23,290 patient samples pooled from 89 studies (Tables 1 and 2). Explicitly, our meta-analysis confirmed that the majority of patients treated with endoscopic and other forms of MISST lumbar stenosis decompressions were between the ages of 30 and 70 years without ES being impacted by that at a statistically significant level by age. Neither did the study design translate into any statistically significant impact on ES (Table 3). In other words, patients’ outcomes are more likely to be impacted by addressing the relevant painful clinical pathology adequately rather than by the way they are studied. Typically, longer follow-up is valued as a prerequisite of meaningful outcome study. However, as illustrated by our meta-analysis, ESs were the largest when extrapolated for VAS back and VAS leg up until a 2-year follow-up in most studies at a statistically significant level (Table 5). Longer follow-up to as much as 6 years and longer did not necessarily translate into larger ESs (P = 0.091); in other words, the natural progression of the disease process may play out with diminishing ESs over time, and perhaps Kaplan Meier durability analyses are more suitable to determine the long-term effects of the contemporary lumbar stenosis surgeries by way of a utilization analysis of additional treatments if any at what point after that.182 Patients with incomplete pain relief and ongoing disability continue to utilize medical services. In the opinion of public health policymakers, the absence of any additional utilization following the lumbar stenosis index surgery is the ultimate proof of superiority by making good on the promise of better value spine care purchasing for the increasing number of aging patients who need it.
When breaking down the ES by a surgical indication as to the modifier, a mixed picture emerged. The ODI ES spinal stenosis-related neurogenic claudication was higher than VAS back and VAS leg at a statistically significant level (Table 4), emphasizing the more functional context of his 10-item outcome tool. The statistical overlap between the VAS leg ESs for the 3 clinical indications studied—stenosis claudication, HNP radiculopathy, and discogenic pain were quite large, suggesting that endoscopic spinal surgery is effective in relieving sciatica-type leg and back pain due to either 1 of these 3 conditions. Using the type of MISST and endoscopic surgery as modifiers was possible, because some of the studies included in this meta-analysis had treatment arms comparing these techniques. There was significant overlap between ESs observed with open laminectomy or tubular retractor microsurgical dissection with similar VAS back, and VAS leg ES data to endoscopy, there were statistically significant differences (P = 0.049) when employing the ODI as an outcome tool with ESs for endoscopy being higher (0.92) than for microsurgical dissection (0.89; Table 6). The open laminectomy (ES = 0.93) and endoscopically assisted interbody spinal fusion followed by percutaneous posterior supplemental pedicle screw fixation (ES = 0.95) had a higher overall ODI ES numbers presumably because of a more comprehensive decompression and perhaps elimination of instability (Table 6). The largest ODI (8198 patients), VAS back (3990 patients), and VAS leg (7954 patients) data set were observed with the transforaminal outside-in approach (Table 7). The highest ODI and VAS leg ESs were found with statistical significance with the interlaminar approach, which was the second most commonly performed endoscopic approach, followed by the UBE uniportal biportal technique (P < 0.0001). Besides the endoscopic lumbar fusion studies included in this meta-analysis, 2 additional noteworthy uniportal endoscopic fusion articles in patients with low-grade scoliosis,183 and patients with symptomatic foraminal stenosis secondary to severe collapsed disc space184 were published within the last year after the cut-off date of this meta-analysis. Based on VAS and ODI outcome reporting, these pivotal studies would not have met the inclusion criteria of our meta-analysis, even if they were published before 31 December 2019, since ES could either not be calculated, or allocated.
As discussed at the outset of this article, the authors were not interested in pushing one endoscopic approach or MISST over another. We were only interested in reporting a familiar set of ODI, VAS back, and VAS leg ESs in the form of reference tables (Table 3 through 7) to aid in the ongoing discussion on how to most effectively transition modern spine care to more reliable and less costly procedures by replacing some of the traditional open with endoscopic and other types of MISST spinal surgery in routine practice. The authors expected the publication bias found in our meta-analysis as one of the main limitations. Seventy-two of the 89 studies included in this meta-analysis were retrospective studies. Twelve studies were prospective, and another 5 studies were randomized prospective clinical trials both of which had multiple treatment arms. Twenty-four of the 36 studies included in the meta-analysis with longer than 2-year follow-up were retrospective. They were estimated to have a high ROB supported by the asymmetric funnel plot, and the spread of ES data in the individual ODI, VAS back, and VAS leg forest plots (Figures 4–6) suggesting that the authors’ meta-analysis was at an overall moderate ROB. To diminish the effect of publication bias the authors employed random ES models for the calculations. While there may be many additional unknown limitations to this type of meta-analysis because of variation in patient’s expectations, surgeons’ skill level, or the organizational process and procedural aspects of the surgery either carried out in an outpatient ambulatory surgery center or in a hospital setting, and many other factors that may be responsible for the heterogeneity observed in some of the subgroups as evidenced by some of the outliers, the difference found in the ODI, VAS back, and VAS leg ESs is reflective of real-life clinical scenarios where spine care is delivered under a great variety of patient- and system-related circumstances. The surgeon skill factor is likely the most relevant confounder in this whole analysis and may be responsible for the wide overlap in successful clinical outcomes regardless of the type of surgery employed. However, statistically significant differences do exist between the type of endoscopic and other types of MISST surgery and should be further investigated to better define and validate preoperative predictors of favorable clinical outcomes with their use. At this juncture, though, the authors accomplished their task of reporting a familiar ODI, VAS back, and VAS leg ES data set (Tables 3–7) for common minimally invasive and endoscopic spinal surgeries, and how they compare to traditional open spinal surgery in the treatment of symptoms related to herniated disc, foraminal, and lateral recess stenosis.
CONCLUSIONS
Despite these limitations, and considering that the authors did not attempt a formal comparison to other MISSTs or traditional open surgical decompression, one argument is to be made from the authors’ meta-analysis: the 3 types of ES data sets with the various endoscopic spinal surgeries are on par with those observed with open laminectomy, microsurgical dissection, and those seen with MISST fusion surgeries which often come with a higher perioperative burden to the patient and are more costly due to the use of implants, higher complication and reoperation rates and unplanned aftercare, longer postoperative recovery and return to work. The surgeon skill level is the most significant confounding factor. The ongoing debate on the merits of endoscopic spine surgery will likely continue. With this meta-analysis, the authors provided the statistical numbers required to have this debate in an objective manner where one wonders about the continued need for aggressive open surgeries for the indications investigated herein if the reported differences in ES numbers for clinical improvements are marginal.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests This manuscript is not meant for or intended to endorse any products or push any other agenda other than the associated clinical outcomes with endoscopic spine surgery. The motive for compiling this clinically relevant information is by no means created and/or correlated to directly enrich anyone due to its publication. This publication was intended to substantiate contemporary endoscopic spinal surgery concepts to facilitate technology advancements. The authors report no conflicts of interest or financial relationships relevant to this work.
Disclosure The authors report no financial disclosures related to this article.
Disclaimer The views expressed in this meta-analysis represent those of the authors and no other entity or organization. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Insights From the ISASS Webinar Series on Current and Emerging Techniques in Endoscopic Spine Surgery | Part 1: Polytomous Rasch Analysis of Surgeon Endorsement of Endoscopic Discectomy/Foraminotomy, Interbody Fusion, and Importance of Patient Feedback During Surgery
- Joint International SILACO, SICCMII, ISASS Symposium as a Model for a Collaborative Framework to Create Literature on Advances in Spine Surgery, Patient Care, and Policy