


Abstract
Background Endoscopic spine surgery is associated with less approach trauma than conventional open translaminar surgery. However, objective evidence to corroborate this empiric observation is scarce. Preservation of the anatomic attachment and sensory function of multifidus muscles have been stipulated to be critical to maintaining the normal function of the lumbar spinal motion segment. The authors were interested in comparing the postoperative approach trauma between traditional open translaminar microsurgical and interlaminar endoscopic discectomy.
Methods The approach trauma to the paraspinal muscles due to interlaminar or open microsurgical discectomy was evaluated on T2-weighted axial magnetic resonance imaging (MRI) images of 39 consecutive patients who underwent lumbar disc surgery. Postoperative MRI images taken at 4 days and within 1 year after surgery were analyzed. Eleven patients underwent conventional open translaminar microdiscectomy surgery. Endoscopic discectomy was performed on 17 patients via the interlaminar and on another 11 patients via the transforaminal approach. The immediate surgical approach trauma was estimated as the defect zone by measuring the normalized relative cross-sectional area (rCSA) of muscle disruption in the surgical corridor 4 days postoperatively. The long-term effect of surgical approach trauma was assessed by measuring the area of the paraspinal muscles that had been replaced by fatty tissue 1 year postoperatively.
Results The rCSA data showed diminished approach trauma with a smaller surgical defect zone in the interlaminar endoscopy group (17.6%) was smaller than in the microsurgical group 4 days postoperatively (41.2%). At 1 year postoperatively, the mean fatty replacement of the paraspinal muscles was 23.6% after microsurgery and 2.1% after the interlaminar endoscopy. Muscle recovery was substantially reduced in the interlaminar endoscopic group, with the muscle zone reducing from 20.3% to 2.1% when analyzed 1 year postoperatively. In the microsurgery group, the muscle damage by atrophy increased from 41.2% to 62.9% at 1 year postoperatively (P < 0.001). Fatty replacement of the multifidus muscle was seen on the ipsilateral and contralateral approach side. There was a negligible change in the muscle zone with the transforaminal approach.
Conclusions Tissue trauma was significantly reduced with endoscopic surgery techniques compared with the traditional translaminar microdiscectomy approach. There was a minor postoperative tissue trauma and hardly any long-term replacement of the multifidus and paraspinal muscles by fatty tissue 1 year postoperatively with the endoscopic technique. The transforaminal approach has the least effect on the paraspinal muscles of the surgical motion segment. Further study is needed to investigate whether these findings translate into decreased postoperative instability or low back pain following endoscopic discectomy surgery.
Clinical Relevance MRI analysis of multifidus atrophy following various lumbar translaminar and transforaminal decompression techniques.
Level of Evidence 3.
INTRODUCTION
Patients often are concerned with the extent of tissue trauma from traditional open lumbar spine surgery. They associate it with higher intraoperative blood loss and more postoperative pain. Nowadays, the public is much more educated about these issues. Many reasons seem plausible, including the easy access to health care-related information on the internet and social media and the aggressive advertising for the latest minimally invasive spinal surgery techniques by physicians and institutions alike. Even professional spine surgeon societies have embraced it by implementing it into their core curriculum and clinical treatment guidelines.
Besides the apparent advantage of eliminating unnecessary surgery by focusing on treating the primary pain generator, the endoscopic approach—whether interlaminar, transforaminal, or full endoscopic—is associated with minimal tissue trauma.1 The collateral damage from surgical exposure may cause denervation of essential stabilizers in the lumbar spinal motion segment, including the multifidus muscles, and contribute to chronic pain syndromes.1–3 We are keenly aware of this postsurgical trauma to the paraspinal muscles. Therefore, we were interested in demonstrating an often underappreciated benefit of the endoscopic staged management approach using minor targeted surgeries by providing visual evidence of reduced postsurgical defect zone and lesser postoperative fatty infiltration suggestive of denervation.4
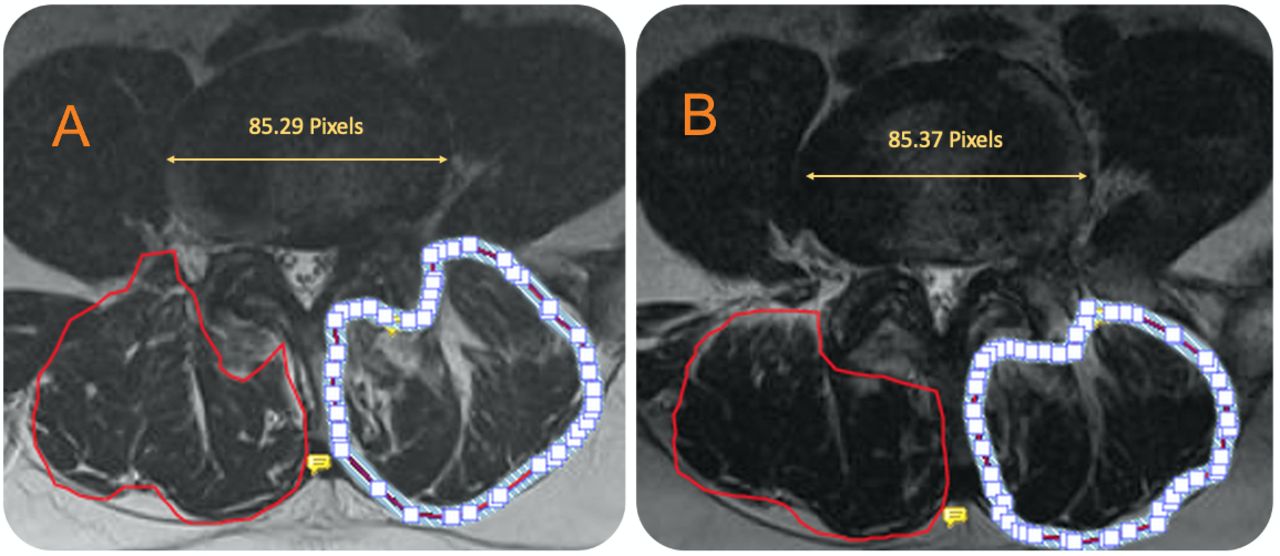
Preservation of the multifidus muscle as one of the most critical dynamic segmental lumbar stabilizers5 has been recognized as one of the essential benefits of minimally invasive spinal surgery techniques application in the lumbar spine.6–12 Loss of its function has been attributed to increased rates of postlaminectomy instability and more low back pain, prompting higher revision surgery rates.13 The multifidus is at particular risk for postoperative dysfunction due to the risk of surgical trauma or traction injury resulting in interruption of its unisegmental innervation.4 The endoscopic approach to the lumbar spine maintains the attachments of the multifidus muscles.14 We serendipitously noticed differences in multifidus atrophy and fatty replacement between microsurgery and endoscopy (Figure 1). We were therefore interested in providing visual evidence for that by analyzing immediate postoperative axial magnetic resonance imaging (MRI) images through the surgical lumbar motion segment following microdiscectomy or endoscopic discectomy via the interlaminar and transforaminal approach by comparing preoperative MRI images with follow-up images taken after surgery and within 1 year postoperatively.

T2-weighted postoperative axial magnetic resonance images (MRIs) are shown to illustrate the extent of postoperative edema and fatty muscle degeneration following a full endoscopic interlaminar directly visualized videoendoscopic discectomy decompression (A, B) vs a traditional translaminar minimally invasive microsurgical decompression employing the operating microscope and a tubular retractor system (C, D). MRIs of study patients with symptomatic herniated disc were obtained at 4 days (A, C) and 1 year postoperatively (B, D). These exemplary postoperative images corroborate this study’s objective cross-sectional area measurements following both procedures by illustrating more edema immediately postoperatively with the standard microsurgical dissection (A vs C) and more atrophy of the paraspinal muscle not just on the approach side but also on the opposite nonsurgical side due to denervation-induced atrophy at 1 year postoperatively (B vs D) when compared with the endoscopic decompression. The observed atrophy and fatty degeneration on the nonsurgical side suggest functional segmental multifidus cross-innervation between both sides.
MATERIALS AND METHODS
Study Patients and Surgical Management
Twenty-eight patients were treated for symptomatic herniated disc either with traditional translaminar microsurgical dissection or with interlaminar endoscopic discectomy in 2010. The patients were age matched with an mean age of 55.3 ± 12.6. Fourteen men and 14 women were enrolled. Surgical treatment for a herniated disc was considered when all nonoperative treatment measures such as supportive care measures, transforaminal epidural steroid injections, and medical management using gabapentin or pregabalin had failed. We have integrated endoscopic discectomy into our practices and employ it as our preferred method of surgical decompression in an outpatient setting. However, occasionally patients underwent traditional translaminar microsurgical dissection, mostly in cases in which surgery was deemed too risky in an ambulatory surgery center due to the patients’ underlying medical comorbidities, such as poorly controlled diabetes, heart or lung disease, or when patients’ health insurance authorization for the endoscopic procedure could not be obtained. Microsurgical dissection was also dictated in some cases when endoscopic equipment was not available in the hospital setting. MRI studies of microsurgical discectomy patients were used as a control group to compare surgical tissue trauma to the paraspinal muscles. The defect zone created by the dissection of the multifidus muscle was of particular interest. The preoperative workup and the inclusion and exclusion criteria for the surgical procedures investigated in this study have been published elsewhere in detail.15–17
The standard translaminar open microsurgical technique through a 22-mm tubular retractor system (Figure 2E) was carried out in 11 patients (27.98%). Seventeen patients (43.58%) underwent interlaminar and 11 patients (28.2%) underwent transforaminal endoscopic discectomy. All microsurgical and interlaminar endoscopic surgeries were done in a similar setup and in a prone position on a lordotic frame and under general anesthesia with concurrent application of local anesthesia as described below. The transforaminal endoscopic surgeries were done under local anesthesia and sedation. The local anesthesia consisting of 0.5% bupivacaine with epinephrine was injected at the determined entry point as well as the entire surgical corridor. The most appropriate skin entry point to approach the surgical level on the symptomatic side for either of the 2 surgical techniques was chosen for surgical techniques with intraoperative use of fluoroscopy in the posteroanterior and lateral plane. Anatomical landmarks, including the midline, the interlaminar window, the intervertebral disc space, and the facet joints, are marked on the patient using intraoperative fluoroscopy. Then, a small 9-mm skin incision is made, and the endoscopic working cannula was inserted to dock at the trailing edge of the surgical lamina medial to the facet joint complex (Figure 2D). In the our minds, the interlaminar approach essentially resembles a miniaturized posterior muscle splitting approach compared with the microsurgical dissection. Hence, we expected diminished tissue trauma with the visualized videoendoscopic direct posterior interlaminar approach compared with the microsurgical open or mini-open technique employing an operating microscope. Since the working area is limited to the interlaminar window, a laminotomy and partial facetectomy were often required. Additional removal of the ligamentum flavum may be necessary to achieve adequate discectomy and decompression of the lateral recess (Figure 2B). The transforaminal endoscopic discectomies were done via the posterolateral approach to Kambin triangle, which we considered for the most part to bypass the paraspinal muscle group.18–23

Clinical example of interlaminar endoscopic approach to the L5-S1 motion segment for a symptomatic herniated disc (A, D). First, the ligamentum flavum is removed (B). Then, the traversing nerve root is retracted with the beveled tip of the tubular working cannula before, and annulotomy is made (C). The alternative posterior translaminar microsurgical dissection and decompression are performed with a tubular retractor system (E). The discectomy is performed following medial facetectomy (F).
In either group, the tubular retractor system or the endoscopic working cannula for the interlaminar approach was inserted over sequential dilators positioning it at the medial aspect of the facet joint at its junction with the lamina. The beveled side of the endoscopic working cannula should be turned toward the ligamentum flavum. The inferior margin of the rostral lamina and, in some cases, the leading margin of the distal lamina can be exposed with rongeurs and a radiofrequency probe. Power instruments, such as burs and Kerrison rongeurs, may be used to remove lamina and remove the inferomedial portion of the facet joint. In the case of endoscopic decompression, specialized miniaturized surgical instruments were used. The bevel of the endoscopic working cannula should be turned to retract the neural structures by retracting either the traversing or exiting nerve (Figure 2C). During the endoscopic discectomy, the hidden zone of Macnab in the axilla between the exiting and traversing nerve was routinely explored in an attempt to complete the decompression while minimizing the extent of medial facet resection to avoid iatrogenic propagation of postoperative instability. The transforaminal discectomy technique has been described extensively in the literature. At the end of the case, the cannula will be turned to visualize the neural structures and control the decompression by a palpation hook. The decompression was deemed complete with either technique once the traversing nerve root was free, and epidural fat floated around the traversing root (Figure 2F).
Cross-Sectional Area Analysis
A 1.5-T MRI system (Signa, GE) was used to obtain axial T2-weighted magnetic resonance images (fast spin-echo method) preoperatively, in the immediate postoperative period (4 days after surgery), and about 1 year (11–13 months) after the operation. Following the method of Chatani, an analysis of grayscale values (0–256) was performed with image-processing software (NIH Image J, Version 1.38i), and the signal intensities of the multifidus muscle were quantified on the axial T2-weighted MRI images.24 There were only patients with single-level and unilateral decompressions, regardless of the surgical method (microsurgical vs endoscopic decompression) used. The signal intensities were measured in the most caudal scan of the decompression site. After careful calibration (to avoid fatty tissue within the muscle), the signal intensities in the cross-sectional area (CSA) of the multifidus muscles of interest were determined in 3 layers (shallow, middle, and deep) to be as extensive as possible. It was outlined while avoiding large fat masses between muscle layers. To control for variations in height, body shape, and weight on the CSA of the multifidus,25 the measurement of signal intensity was performed 3 times in each layer, and the mean value was reported as the signal intensity for each layer. The mean of the signal intensities of the 3 layers was calculated for each side.26 To further minimize measurement errors, the multifidus muscles’ relative signal intensity CSA values were calculated as a ratio to that of the lower margin of the muscles L4 vertebra.27 The mean of the signal intensities was calculated for each side.28 For clarity of data presentation, the endoscopic interlaminar decompression patients were analyzed as the “Endoscopy” group, and the microsurgical discectomy patients were analyzed as the “Microsurgery” group.
Statistical and Outcome Analysis
Primary clinical outcome measures for patients who underwent endoscopic facet cyst resection were the Macnab criteria at final follow-up 2 years postoperatively.29 Statistical tests employed in the outcome analysis of this study included 2-way cross-tabulation statistics to measure any statistically significant association between variables using IBM SPSS Statistics software, Version 25.0. Pearson χ 2, paired t test, and Fisher exact test were employed to assess the strength of association between variables statistically. The mean, range, and SD, and percentages of all nominal variables were calculated. The data from the control side opposite from the decompression site were used as an internal control for paired t test analysis (IBM SPSS Version 27). The difference in the CSA of the multifidus muscle between the approach and nonapproach sides was also analyzed with the paired t test while accepting a statistical significance level of P < 0.05.30 Institutional Review Board approval was obtained for this study (CEIFUS 106-19). Written informed consent was obtained from the patient for publication of this original study and any accompanying images.
RESULTS
The majority of patients reported excellent and good Macnab outcomes (25/28; 39.3%). The remaining patients had poor Macnab outcomes due to incomplete decompression. There were no study patients with significant complications related to approach, surgery, or anesthesia. In the MRI images obtained at 4 days postoperatively (Figure 3), the relative cross-sectional area (rCSA) data showed diminished approach trauma with a substantially smaller mean surgical defect zone in the endoscopy group (17% vs 41%) compared with the microsurgical group. As expected, there was no defect zone with the transforaminal approach (Figure 4). The rCSA for the multifidus replaced by fatty tissue was not substantially different between the interlaminar endoscopy (20%) and microsurgical (22%) group postoperatively. In the axial T2-weighted MRI produced at 1 year postoperatively (Figure 5), the defect zone including scar formations was much more extensive for microsurgical procedures (62%) than for the endoscopy (6%). The fatty replacement of the paraspinal muscles resulted in a mean 23% rCSA decrease after microsurgery and 2% after the endoscopy, respectively. The defect zone was substantially reduced in the interlaminar endoscopic group with good recovery of the paraspinal muscles from preoperatively (20%) to postoperatively (2%). In the microsurgery group, a similar analysis showed an additional increase of the defect zone 41% immediately after surgery to 62% at 1 year postoperatively. All of these differences were statistically significant on paired t testing (P < 0.001). In the transforaminal endoscopic group, there was no significant difference between the observed muscle degeneration.

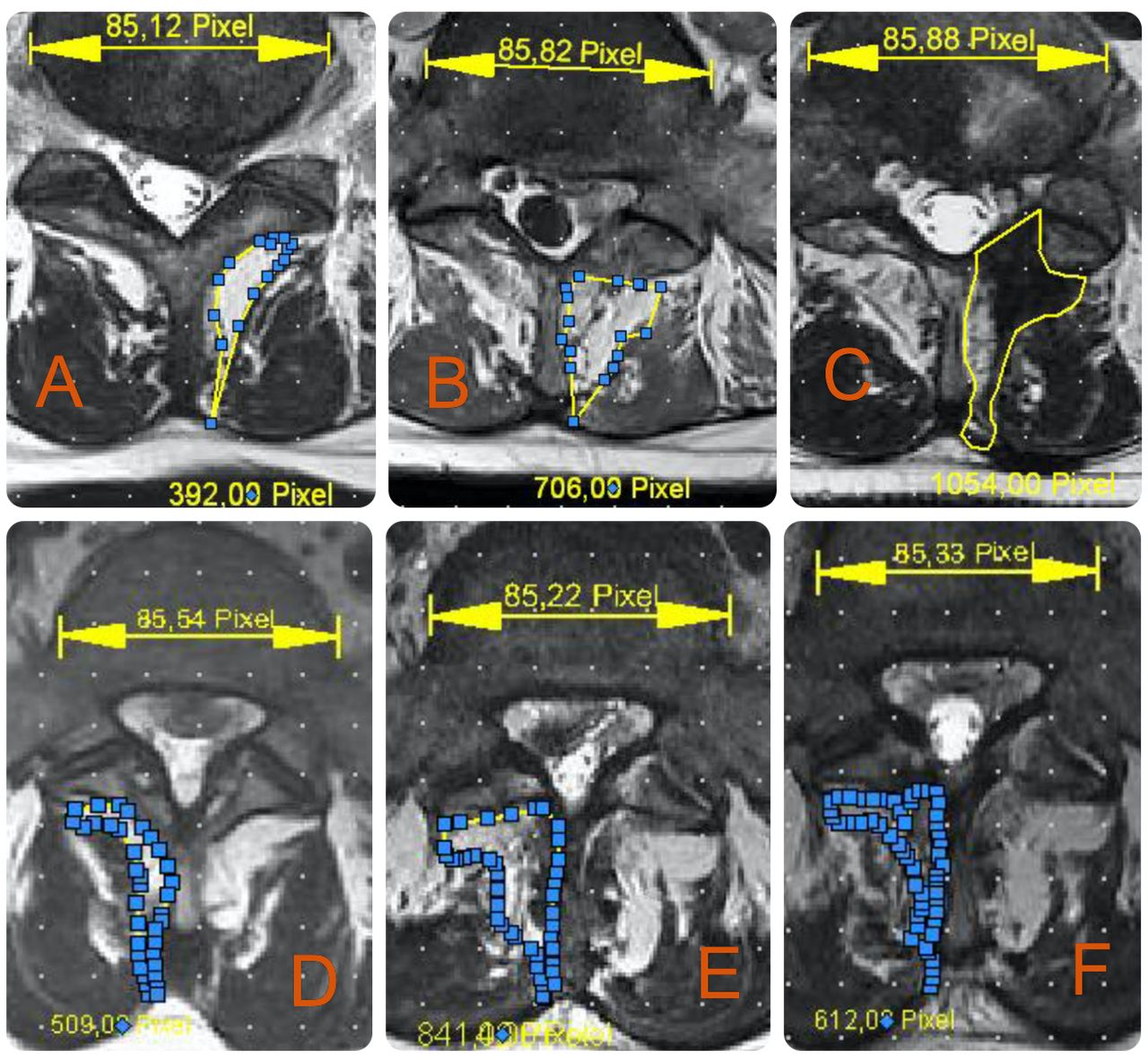
-weighted axial magnetic resonance imaging (MRI) image sequences obtained from patients with symptomatic lumbar disc herniations who underwent either microsurgical discectomy (A-C) or interlaminar endoscopic discectomy decompression (D–F). The MRI panels show the defect zone created by the 2 different surgical techniques. Preoperative measurements (A, D) were compared with measurements done on postoperative MRI images obtained at 4 days (B, E) and 1 year postoperatively (C, F). These area measurements summarized in Table suggested a significantly smaller defect size with the endoscopic vs the microsurgical technique (P < 0.001).
T2-weighted axial magnetic resonance image (MRI) sequences obtained from a 74-year-old patient with symptomatic left L4/5 extraforaminal lumbar disc herniations who underwent transforaminal endoscopic discectomy decompression. The MRI panels show the cross-sectional measurements of the paraspinal muscle zone following the transforaminal discectomy. Preoperative measurements (A) were compared to measurements done on postoperative MRI images obtained within one year from surgery (B). These area measurements summarized in Table 1 suggested no significant atrophy of the paraspinal muscles with the endoscopic transforaminal technique.

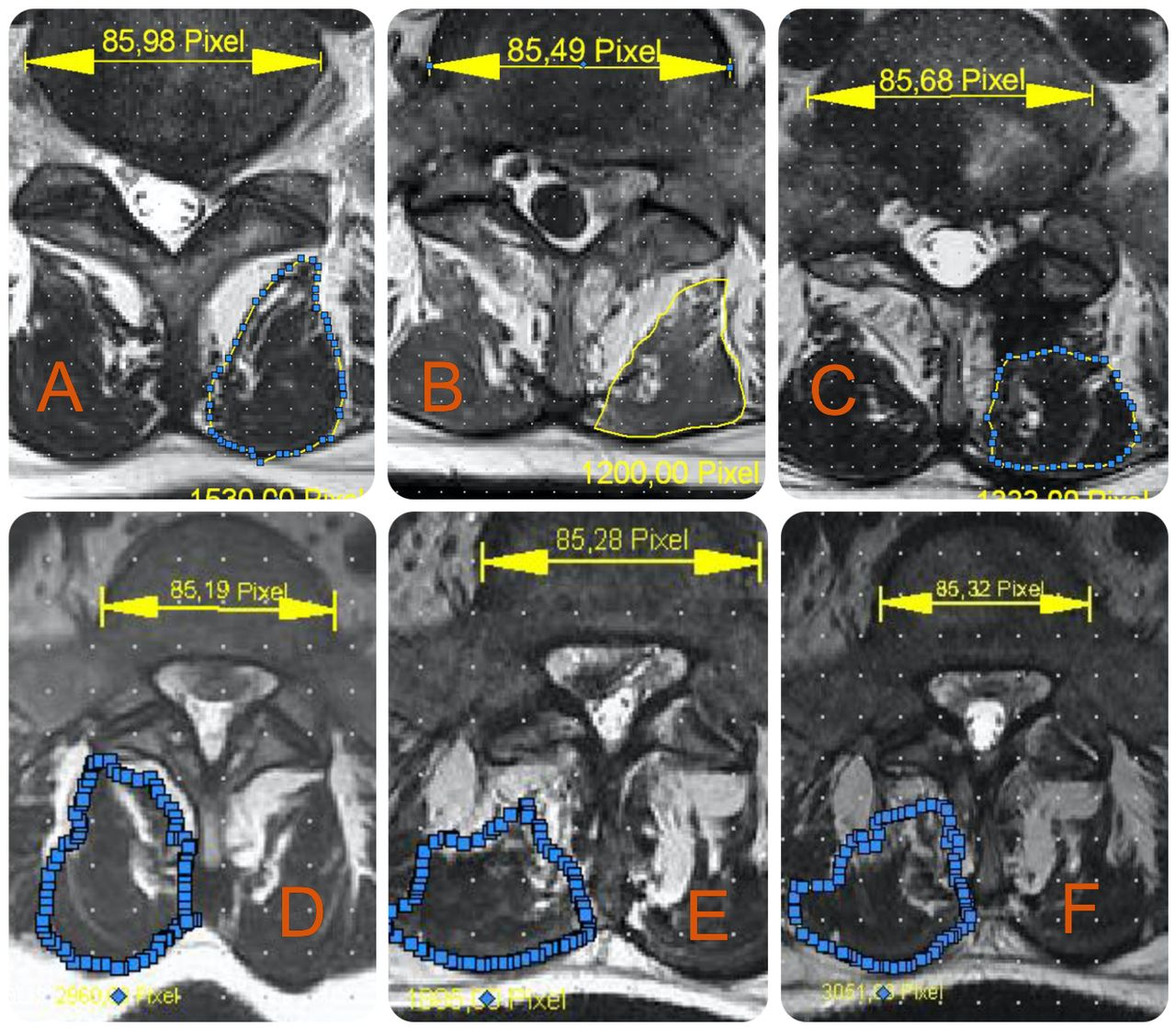
T2-weighted axial magnetic resonance image (MRI) sequences obtained from patients with symptomatic lumbar disc herniations who underwent either microsurgical discectomy (A–C) or interlaminar endoscopic discectomy decompression (D–F). The MRI panels show the cross-sectional measurements of the paraspinal muscle zone following discectomy by the 2 different surgical techniques. Preoperative measurements (A, D) were compared with measurements done on postoperative MRI images obtained at 4 days (B, E) and 1 year postoperatively (C, F). These area measurements summarized in Table suggested significantly less atrophy of the paraspinal muscles with the endoscopic vs the microsurgical technique (P < 0.001). Moreover, there was more paraspinal muscle atrophy with the microsurgical technique not only on the approach side but also opposite from it, implying disruption of cross-innervation between the bilateral paraspinal muscle groups, including the multifidus muscles.
Changes in surgical defect zone and paraspinal muscle zone data obtained at 4 d and 1 y postoperatively for interlaminar endoscopy and microsurgical patients.
DISCUSSION
This study shows that the endoscopic interlaminar procedure diminishes the perioperative trauma due to the surgical approach compared with the dissection necessary for the microsurgical decompression. The transforaminal endoscopic approach hardly had any impact on the paraspinal muscle atrophy. We were not surprised that there was no significant difference in the mean paraspinal muscles rCSA for both minimally invasive techniques (22.6% vs 20.3%) when MRI images were evaluated immediately after surgery.28 However, as expected, the defect zones were rather large with microsurgical dissection (41.2%) than with the interlaminar endoscopic technique (17.6%). Comparing these immediate postoperative CSA measurements on axial T2-weighted MRI images to those obtained on the same patients at approximately 1 year postoperatively revealed stark differences in the muscle atrophy and replacement of the multifidus muscles with fatty tissue typical of degenerative denervation atrophy observed in the paraspinal muscles in patients who underwent extensive exposures during traditional open surgery of the lumbar spine. The size of the defect zone, including scar formations, was more striking for microsurgical procedures (62.9%) than for the endoscopy (6.4%) with statistical significance (P < 0.001). More importantly, the increased paraspinal muscle trauma with microsurgical dissection was illustrated by more considerable rCSA reductions of 23.6% in those microsurgical patients when compared with 2.1% after interlaminar endoscopy (P < 0.001). The advantage of the interlaminar endoscopic approach, which was associated with minor tissue trauma and disruption of the nervous and vascular supply to the multifidus muscle, was further documented by the increase in the multifidus CSA from 2% immediately postoperatively (4 days) to 20% at 1 year after surgery. These observations suggested that the paraspinal muscles recovered from the approach trauma inflicted during endoscopy. In the microsurgical group, the mean defect rCSA increased rather than decreased from 41.2% to 62.9%. These numbers were predominately due to filling the larger microsurgical defect zone with scar tissue as well as the fatty replacement of the paraspinal muscles. Some MRI images also showed reduced CSA of the multifidus muscles opposite the approach side suggesting disruption of redundant cross-innervation from the tissue trauma to the surgical exposure (Figure 2).2 On the other hand, endoscopy patients went on to heal their surgical access corridors with minimal muscle atrophy on the approach side and with none opposite to that.
The motivation for the study stemmed from our occasional postoperative MRI observation of more significant atrophy of the paraspinal muscles—specifically the multifidus muscles—in the microdiscectomy patients than in patients who underwent the interlaminar endoscopic decompression. The transforaminal endoscopic approach affected the paraspinal muscle the least. The patient selection criteria for the various types of minimally invasive decompression surgeries of the lumbar spine typically revolve around the location and extent of the stenotic process, the presence of instability, medical comorbidities, and other demographic factors.31,32 The extent of exposure-related collateral damage to the paraspinal musculature—most notably the multifidus muscle—has found little consideration thus far in the debate of the most appropriate surgical approach and decompression technique to painful stenosis and herniated disc of the lumbar spine. The documentation of the fatty degeneration and atrophy of the multifidus muscle with the microsurgical dissection provided in the present study indicate that unintended devascularization, direct and indirect denervation—the latter by loss of cross-innervation2—may contribute to accelerated degeneration with the development of instability as these dynamic stabilizers may lose their function. This conclusion is further corroborated by our observations and those made by others13,33–37 that such atrophy and fatty degeneration of the multifidus muscles were even routinely seen on the opposite side from a unilateral microsurgical decompression. This understanding of the surgical anatomy of the multifidus muscle provided the theoretical basis for the minimally invasive multifidus split approach to the posterior lumbar spine.7 According to the recorded CSA numbers, the tissue trauma observed in our patients with the endoscopic interlaminar approach was less than with microsurgical dissection. Over the 1-year follow-up period, the defect zone shrunk, and the muscle zone increased, suggesting that the paraspinal musculature recovered and nearly healed to its original status when the miniaturized interlaminar endoscopic approach was employed.
The present study has limitations related to the small number of patients enrolled in each group. We could not perform a comprehensive study of MRI findings following different minimally invasive decompression procedures of the lumbar spine. This study was nearly impractical in Europe and North America, where we reside, considering that most health insurance companies deny coverage for routine postoperative MRI scans. We were only able to enroll a limited number of patients until the need for the MRI studies was questioned and enrollment of additional patients stopped. Ideally, we would have been able to include transforaminal endoscopy patients because one would perhaps expect even less tissue trauma as this extraforaminal approach essentially circumvents the paraspinal musculature nearly in its entirety.17,20,23,38 Moreover, disruption of the multifidus attachments and its respective vascular and nervous supply would also not be expected.35
CONCLUSIONS
The main goal of the the present study was to document the MRI appearance of the microsurgical vs the endoscopic interlaminar decompression technique and to alert spine surgeons on the unintended side-effects of such exposures so they can incorporate these observations in the preoperative decision algorithm they employ when selecting a particular approach and surgical technique in the treatment of their patients suffering from a symptomatic herniated disc and spinal stenosis. Further study of additional confounding risk factors for postoperative muscle atrophy, including the presurgical status of muscle and spinal degeneration, gender, age, previous injury,39 medical comorbidities, surgeon training, and skill level, as well as postsurgical rehabilitation programs,8,39–42 is warranted to further statistically substantiate our observations in a formal comparative study between the commonly employed minimally invasive spinal decompression techniques.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors have no direct (employment, stock ownership, grants, patents), or indirect conflicts of interest (honoraria, consultancies to sponsoring organizations, mutual fund ownership, paid expert testimony). The authors are not currently affiliated with or under any consulting agreement with any vendor that the clinical research data conclusion could directly enrich.
Disclosure The authors report no financial disclosures related to this article.
Disclaimer The views expressed in this article represent those of the authors and no other entity or organization. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This manuscript is not meant for or intended to endorse any products or push any other agenda other than the associated clinical outcomes with the endoscopic versus open microsurgical discectomy surgery. The motive for compiling this clinically relevant information is by no means created and/or correlated to directly enrich anyone due to its publication. This publication was intended to substantiate contemporary endoscopic spinal surgery concepts to facilitate technology advancements.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.