


Abstract
Background Patients may occasionally have persistent or recurrent radicular symptoms after cervical artificial disc replacement (ADR) for cervical spondylotic radiculopathy. We describe our approach using anterior cervical foraminotomy (ACF) to provide symptom relief in such patients without the need to convert to a fusion or remove the ADR implant.
Methods Our operative technique for ACF after cervical ADR begins by starting at the lateral edge of the ADR at the superior end plate of the inferior vertebral body. The ipsilateral uncovertebral joint is drilled with a combination of a high-speed burr and diamond-coated burr to minimize the risk of injury to the vertebral artery. The neuroforamen is entered after drilling through the posterior aspect of the uncinate process. The exiting cervical nerve root should be directly visualized, and a Kerrison rongeur may be used to trace along the nerve root laterally to remove any remaining uncinate osteophyte or process. We queried our internal database for patients with recurrent or new radicular pain following cervical ADR who underwent ACF. Clinical characteristics and outcomes were reported.
Results Five patients with recurrent radicular symptoms after ADR were reviewed. Two ACFs were performed at C5-6, and 2 were performed at C6-7. Four patients developed ipsilateral recurrent radicular symptoms, and only 1 patient developed contralateral new radicular symptoms. Three patients reported complete resolution of their new or recurrent radicular symptoms following ACF, and 2 patients reported only partial resolution. No patients required conversion to a fusion.
Conclusions In patients with recurrent symptoms of cervical spondylotic radiculopathy following ADR, ACF with uncovertebral joint resection can be used to provide direct foraminal decompression without the need for implant removal. This approach also preserves motion at the affected level, preserves cervical spinal stability, and prevents the need for spinal fusion.
Clinical Relevance Patients with persistent or recurrent radicular symptoms after cervical ADR may achieve resolution of symptoms through a modified ACF technique.
Level of Evidence 4.
INTRODUCTION
Over the past decade, cervical artificial disc replacement (ADR) has been successfully adopted for single-level and multilevel cervical disease that is responsible for neck pain, radiculopathy, and/or myelopathy in affected individuals. Numerous studies support ADR having a comparable risk profile with superior clinical outcomes compared to anterior cervical discectomy and fusion (ACDF).1–3 This is presumably due to less hypermobility and subsequent degeneration at the adjacent segment after preserving a functioning motion segment through arthroplasty.4 This is supported by numerous large randomized clinical trials demonstrating significantly lower reoperation rates at the adjacent segment after both single-level5,6 and 2-level ADR.1,7 In addition, ADR has been observed to have a lower reoperation rate at the index level.8 In some cases, however, patients have persistent or recurrent radicular symptoms after ADR originating from the index level of the operation. The current authors have observed this in both the ipsilateral and contralateral side compared to the preoperative symptomatic side. This may be caused either from the development of new foraminal osteophytes causing foraminal stenosis or persistent postoperative foraminal stenosis causing nerve root impingement. In such cases, treatment options have mostly consisted of device explantation and conversion to fusion or posterior cervical foraminotomy, both of which have their disadvantages.8 In the current manuscript, the authors describe an alternative option—anterior cervical foraminotomy (ACF) in the setting of a well-placed arthroplasty implant, without ADR explantation.
Anterior cervical decompression was first described by Robinson and Smith in 1955 and Cloward in 1958 in order to directly decompress spondylotic spurs and disc fragments.9,10 In 1968, Verbiest described an anterolateral cervical approach that required exposure and displacement of the vertebral artery.11 Risk of injury to this artery was probably why this technique was not widely accepted. Anterior cervical foraminotomies and drilling the ipsilateral uncovertebral joint were described in 1996 by Jho to achieve cervical decompression through an anterior approach while preserving a functioning motion segment and avoiding the need to mobilize the vertebral artery.9 In contrast to Verbeist’s approach, Jho technique targeted spondylotic osteophytes directly by drilling the uncinate process.
Performing ACF and widening decompression from an anterior approach are reasonable and logical approaches to prevent conversion to a fusion and avoid its attendant risks, namely pseudarthrosis and adjacent segment disease. While posterior foraminotomy as an alternative option, this causes some unavoidable facet joint damage and may not always enable removal of anteriorly based intraforaminal uncovertebral joint osteophytes. We describe our operative technique and offer several cases, as well as a detailed illustrative case, of patients who presented with persistent or recurrent radiculopathy after ADR in whom ACF provided symptom relief without the need to convert to a fusion.
METHODS
Operative Technique
This operation is performed with the patient under general anesthesia induced by means of endotracheal intubation. A standard anterior cervical approach has already been previously described.9,10 We do not use a cervical traction device. Slight extension of the neck is maintained by placing a rolled towel behind the shoulders. We tape both shoulders and gently pull caudally to anchor both ends of the tape to the edges of the operating table only if necessary, such as while operating on the C6-7 level if visualization is otherwise not possible.
Since this is a reoperation procedure, we almost always prefer to use the existing incision for anterior cervical access if the surgical approach is ipsilateral to the radiculopathy. In patients with radiculopathy contralateral to the side of the index surgery, we will request formal vocal cord evaluation by an ear, nose, throat (ENT) surgeon prior to surgery. If there is no subclinical vocal cord paralysis observed by formal ENT evaluation, it is safe and preferred to access the spine ipsilateral to the side of radiculopathy. In these cases where a new incision is needed, we prefer a transverse incision, 2.5 to 4 cm long, along the skin crease for improved cosmesis. The ventral cervical spine is accessed through a combination of sharp and blunt subplatysmal dissection. The carotid artery and sternocleidomastoid muscle are identified early in the exposure and protected in the lateral aspect of the exposure. The omohyoid muscle, trachea, and esophagus are gently retracted medially to expose the prevertebral fascia and anterior cervical spine. It is important to localize the correct level fluoroscopically since scar tissue forms over the implant and distorts normal anatomy. The operating microscope is brought into the surgical field. Extensive elevation of the longus colli muscle on the side of ACF is needed to allow visualization of the uncovertebral joint(s). The longus colli muscles are carefully elevated ipsilateral to the planned ACF using bovie cautery and then displaced laterally in a subperiosteal manner with elevator instruments. This technique should be approached with care because coagulating too far laterally on the colli muscles risks injury to the sympathetic nerve fibers. Additionally, the vertebral artery is vulnerable at the level of the disc space and care should be taken here with the bovie cautery. An anterior cervical discectomy retractor system is used for wide exposure and optimal visualization of the intervertebral disc space.
The lateral edge of the ADR at the superior end plate of the inferior vertebral body is the starting point. Lateral to this point, between the transverse processes of the upper and lower vertebra, is where the ipsilateral uncovertebral joint is found. The uncovertebral joint is sloped cephalad at a 30° against the horizontal plane. Caution should be taken to avoid damaging the implant during exposure and drilling of the uncovertebral joint. The uncovertebral joint is drilled using a standard high-speed burr with an AM8 (Medtronic, Minneapolis, MN) (Figure 1). After drilling approximately two-thirds of the uncovertebral joint, we alternate to a 2-mm diamond-coated burr tip to drill the remaining portion because the vertebral artery lies just lateral to the lateral cortex of the uncinate process and the diamond-coated burr tip is less likely to damage the vertebral artery lumen should the cortical bone be incidentally breached. However, the surgeon must be aware that this burr tip becomes very hot quickly and requires constant irrigation. A thin cortical layer of bone is left attached to the ligamentous tissue covering the medial portion of the vertebral artery.9 Furthermore, we place a Penfield-4 over the vertebral artery for additional protection while drilling the uncovertebral joint. Suspicious transverse foramen morphology on preoperative computed tomography (CT) imaging should prompt advanced imaging with magnetic resonance angiography or CT angiogram to understand the course of the vertebral artery, as well as identify anatomical variations that would place the vertebral artery at risk during drilling of the uncovertebral joint. Upon drilling through the posterior aspect of the uncinate process, the neuroforamen is entered. At this point, a small microsette curette is used to palpate the posterior aspect of the vertebral body, pedicle superior border, and any remaining uncinate process. At this point, the exiting nerve root should be directly visualized and a Kerrison rongeur may be used to trace along the nerve root laterally to remove any remaining uncincate osteophyte or process. Often once the uncinate process is drilled through the cortex at the level of the inferior implant end plate, the entire uncinate process can be carefully removed with a curette, similar to a radical facetectomy in the lumbar spine. During this process, dissection of the connective tissue between the vertebral artery and uncinate process should be done carefully with a blunt instrument such as a Penfield-4.

View of a right-sided cervical foraminotomy showing resection of the uncinate process lateral to the artificial disc implant, decompressing the corresponding nerve root.
Excision of the posterior longitudinal ligament is generally not needed because the ligament was presumably already removed during the original ADR procedure. Meticulous hemostasis is needed, and a surgical drain is not used. The platysma is closed with interrupted 5–0 absorbable sutures in an interrupted fashion, and the dermal layer is closed with interrupted 5–0 absorbable sutures. The skin is approximated with steristripes followed by a 2″ × 2″ gauze and surgical dressing. A final anterior-posterior radiograph should reveal a wide uncinate resection.
RESULTS
Five patients with recurrent radicular symptoms after ADR were reviewed (Table). All of the patients were men, and the mean age was 57 years (range 35–68 years). Two ACFs were performed at C5-6, and 2 were performed at C6-7. Two patients underwent implant of M6 ADRs, 2 had Prestige LPs implanted, and 1 underwent implant with a ProDisc ADR. Four patients underwent ACF on the left side, and one patient underwent ACF on the right side. Four patients presented with left-sided radicular symptoms, and one patient had right-sided symptoms. Three patients had 2-level ADRs, and 1 patient had a 3-level ADR. The mean time to reoperation was 22.3 months for all patients and 6.4 months after the outlier patient who became symptomatic after 86 months was excluded (range 2–86 months). Four patients developed ipsilateral recurrent radicular symptoms, and only one patient developed contralateral new radicular symptoms. Three patients reported complete resolution of their new or recurrent radicular symptoms following ACF, and 2 patients reported partial resolution. Four patients did not require implant removal. One patient with right C5-6, C6-7 ACF for right radicular symptoms had their C5-6 Prestige LP ADR replaced with the same type of implant due to malpositioning. The right C6-7 ACF was performed with implant retention. There were no patients who required conversion to a fusion.
Patient demographics and outcomes of ACF following artificial disc replacement placement.
Case Illustration
Patient 1 is a 35-year-old man who has been a competitive Ju-Jitsu fighter since the age of 5 and recently won the world championship title in his weight class. He complains of a 6-month history of right shoulder and scapular pain with associated right arm weakness when he raises his arm above shoulder level. He denies neck pain, gait instability, or dropping items. His pain is refractory to physical therapy, chiropractic manipulation, and local muscle block injections. Physical examination was significant for atrophy of his right pectoralis and infraspinatus muscles. His right deltoid, biceps, triceps, and wrist extension strength was ⅘, and all other muscle groups were full strength. Sensation was intact to light touch throughout. He did not show evidence of hyperreflexia based on reflex examination, Hoffman sign, or Babinski reflex. Cervical x-ray showed disc collapse of C5-6 and C6-7. There was no instability during flexion-extension radiographs (Figure 2). Magnetic resonance imaging of the cervical spine showed multilevel spinal stenosis from C4-7, with C5-6 being the worst level. C4-5 had severe right and moderate left foraminal stenosis. C5-6 had disc height collapse, severe left and right foraminal stenosis. C6-7 also had disc height collapse and severe right foraminal stenosis (Figure 3). CT scan of the cervical spine showed normal facet joints throughout the cervical spine, a large right foraminal osteophyte at C6-7, and less extensive osteophytes at C5-6 causing foraminal stenosis (Figure 4). The patient wanted an operation that will continue to enable him to compete at a professional level. A C5-6, C6-7 ADR with M6 (Orthofix Medical, Inc, Plano, TX) and right C4-5 ACF without arthroplasty were offered.

Anterior-posterior (A) and lateral (B) cervical x-ray images showing disc collapse of C5-6 and C6-7. There was no abnormal motion during flexion (C) or extension (D) films.
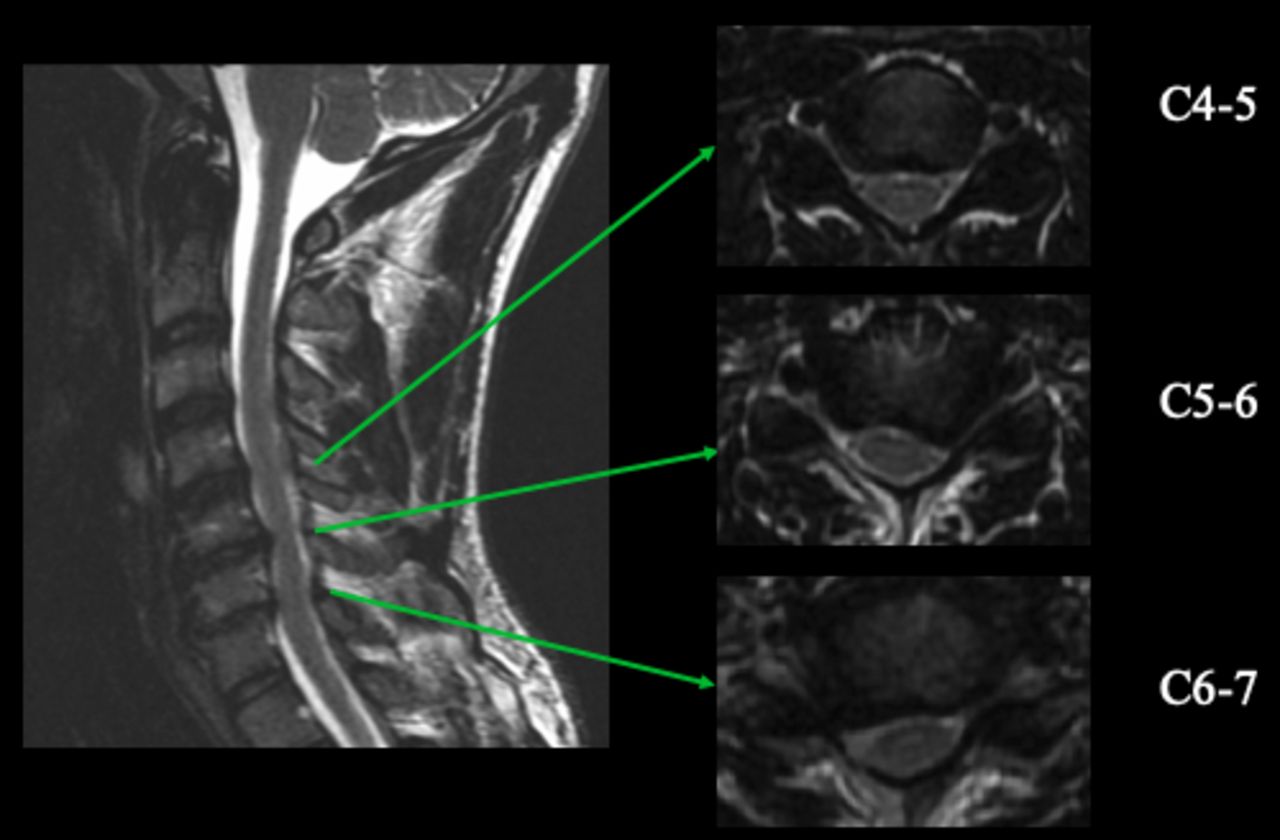
Magnetic resonance images of the cervical spine showed multilevel spinal stenosis from C4-7, with C5-6 being the worst level. C4-5 had severe right and moderate left foraminal stenosis. C5-6 had disc height collapse with severe left and right foraminal stenosis. C6-7 also had disc height collapse and severe right foraminal stenosis.

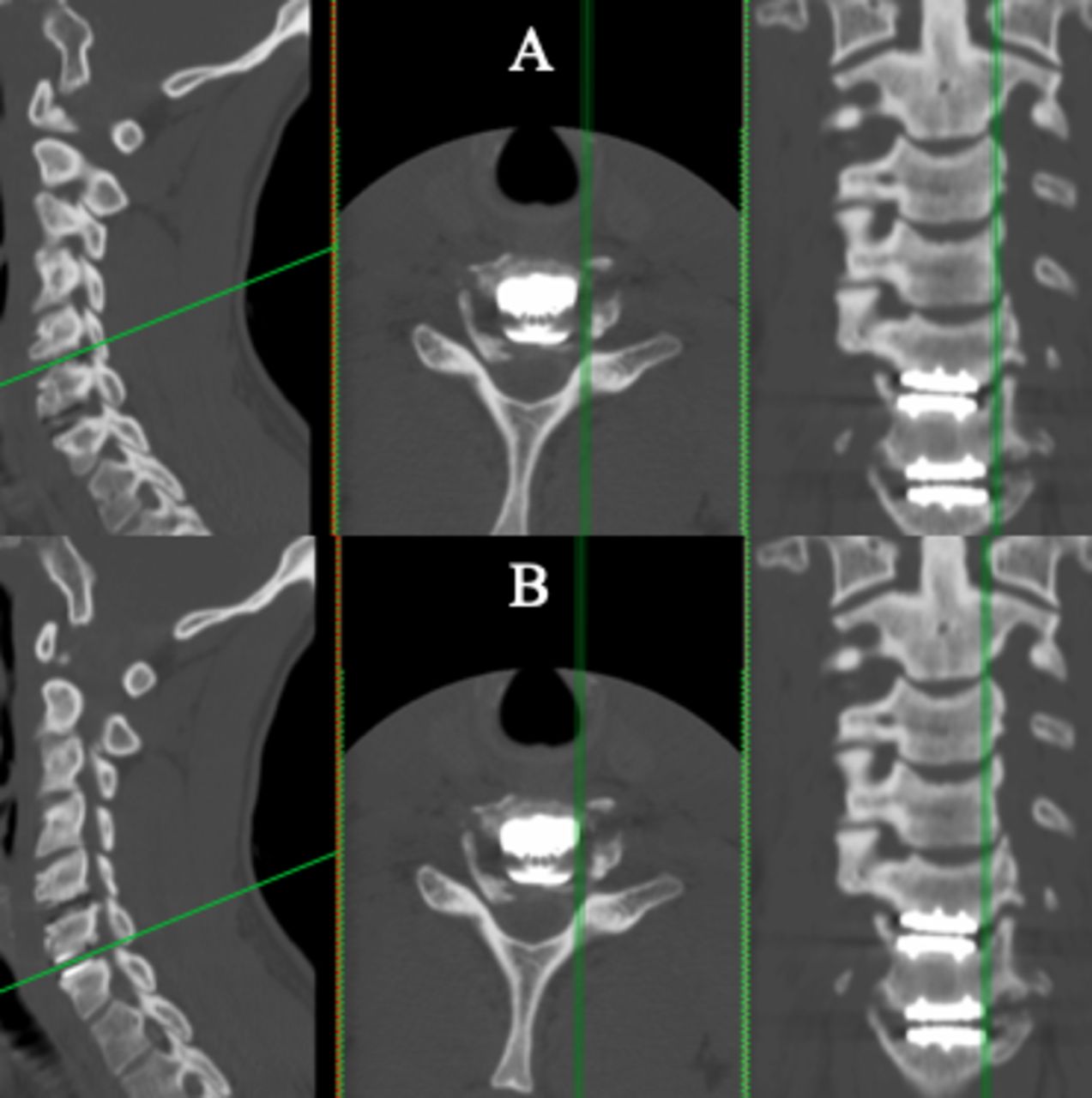
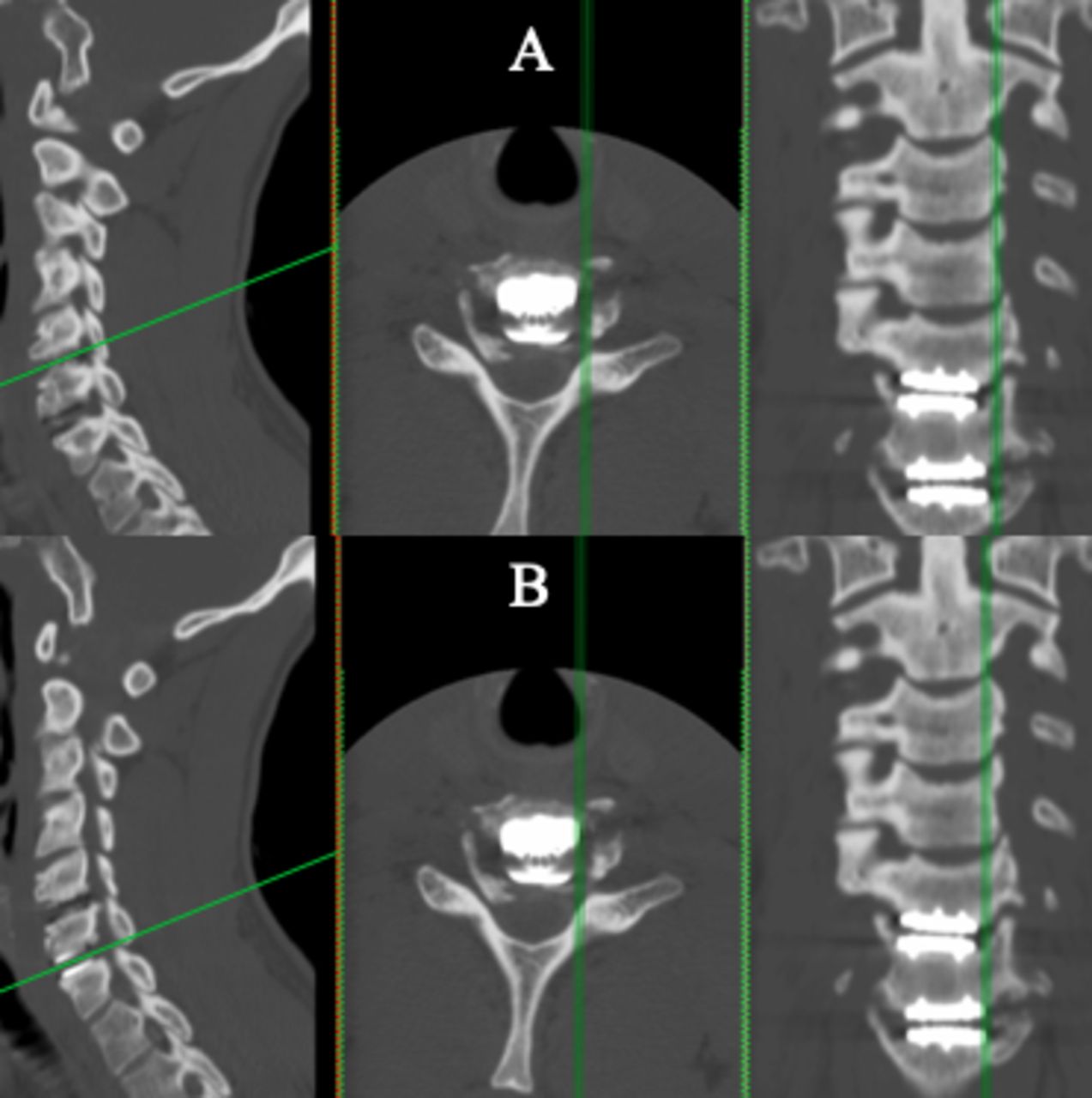
Computed tomographic images of the cervical spine showed normal facet joints throughout the cervical spine, a large right foraminal osteophyte at C6-7 (A), and less extensive osteophytes at C5-6 causing right-sided foraminal stenosis (B).
The C6-7 level was addressed first at the time of surgery. A high-speed burr was used to drill off a significant portion of the posterior uncinate processes bilaterally, and the posterior longitudinal ligament was released to perform wide foraminotomies bilaterally to the point that the nerve root takeoff was visualized exiting on both sides. A size 6 mm tall × 16 mm deep implant was used (Figure 5). The same steps were carried out at the C5-6 level (Figure 3). After both implants were inserted, a right-sided anterior C4-5 foraminotomy was performed adjacent to the native disc without complications. Two weeks after surgery, his presenting symptoms had resolved but he complained of a similar pattern of pain and weakness on the left arm. The deltoid strength was 4+/5, and the left biceps, triceps, and wrist extension strength was ⅘. At 6 weeks following the operation, his symptoms persisted despite physical therapy. CT myelogram of the cervical spine was performed at 12 weeks postoperatively that showed persistent left far-lateral intraforaminal osteophytes at C5-6 and C6-7 (Figure 6). Seven months after the original procedure, a C5-6 and C6-7 ACF was offered with a left-sided neck incision, after ENT vocal cord evaluation. The aforementioned surgical technique was performed to drill the uncovertebral joints and uncinate processes, first at the left C6-7 level followed by the C5-6 level (Figure 7). Four weeks after his reoperation, he reports resolution of his left-sided shoulder pain and improved strength in his left arm. At final follow-up visit 4 months postoperative, he reports complete resolution of bilateral upper extremity symptoms and that he is back to training in Jiu-jitsu.

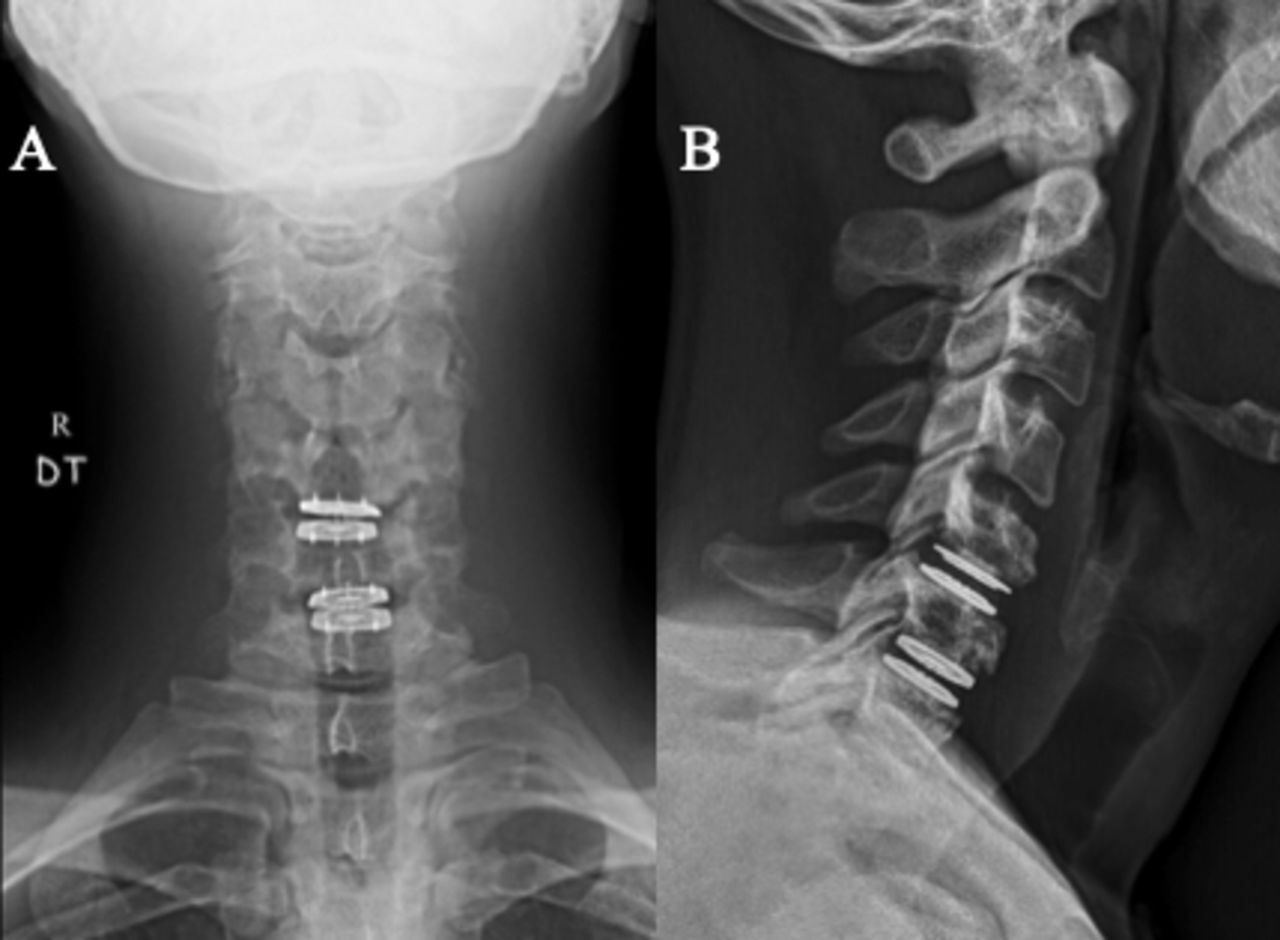
Postoperative anterior-posterior (A) and lateral (B) cervical x-ray images showing appropriate placement of artificial disc replacements at C5-6 and C6-7 and right anterior cervical foraminotomy at C4-5 without hardware.
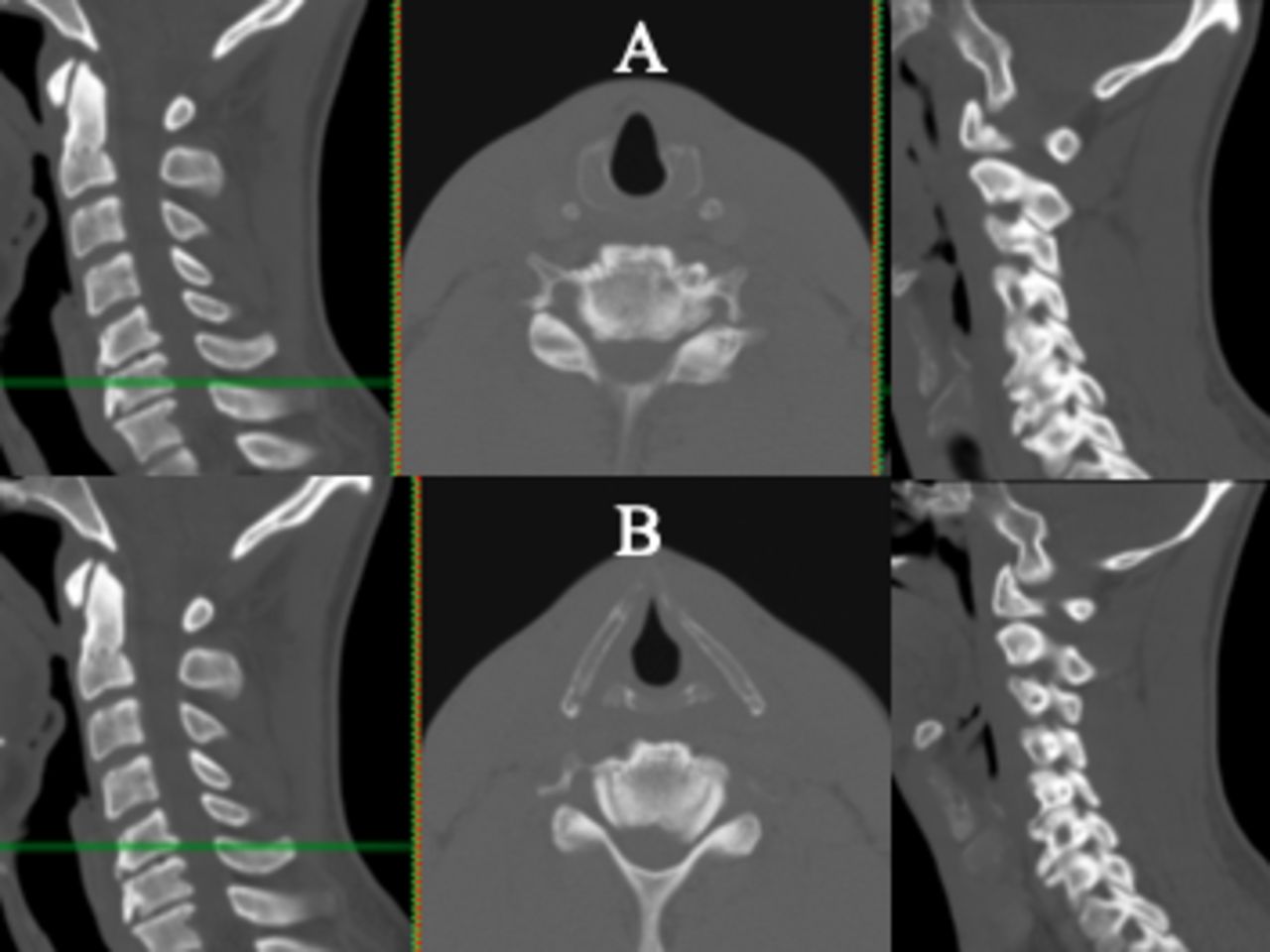
Computed tomography myelogram of the cervical spine at 12 weeks postoperatively that showed left foraminal osteophytes at C5-6 (A) and C6-7 (B).

Anterior-posterior cervical x-ray image after left anterior cervical foraminotomy was performed for new left-sided radicular symptoms at C5-6 and C6-7, demonstrating wide uncinate process resection.
DISCUSSION
Summary of Case
Our illustrative case describes a young patient with resolution of his ipsilateral radicular pain and development of new contralateral radicular symptoms in a similar dermatomal and myotomal distribution following a 2-level ADR. This case highlights a clinical situation that ensues when surgeons fail to perform an aggressive enough uncinate resection during initial decompression and ADR placement. Leaving too much uncinate process behind during ADR placement may be problematic because uncovertebral osteophytes may form or persistent unresected osteophytes may become symptomatic given the restored mobility of the motion segment. In this particular case, the new radicular symptoms developed on the patient’s contralateral side, but the remaining 4 patients in our series had persistent ipsilateral radicular symptoms with correlative foraminal stenosis. Performing select ACFs in our patients achieved symptom relief without the need to remove the ADR implant or convert to a fusion and preserve functional motion segments.
Long-Term Outcomes Following Anterior Foraminotomy
Although the ACF technique has been described several years ago, it does not have the same popularity among spine surgeons compared to anterior cervical discectomy and fusion and posterior foraminotomies for cervical radicular symptoms.12,13 Until recently, there have not been studies reporting long-term outcomes of ACF for 1-level or 2-level cervical radiculopathy. Park et al provide encouraging clinical outcomes for 44 patients who underwent ACF and report a mean follow-up of 8.8 years.12 In this study, 39 (89%) patients achieved an excellent or good outcome at final follow-up. There were no index level reoperations; however, 2 additional operations for symptomatic adjacent segment degeneration were reported (4.5%). Radiographically, adjacent segment degeneration was noted in 6% and 11% at the cranial and caudal segments, respectively. Two interesting findings from Park et al were the high prevalence of postoperative complaint of shoulder pain and same level degeneration. Seven (16%) patients sought primary care for postoperative shoulder pain following ACF (6 had pain on the ipsilateral side of radiculopathy and 1 on the contralateral side). Furthermore, acceleration of disc space narrowing was apparent in all operated levels. Restriction of range of motion was seen in 40% of cases, and spontaneous fusion was seen in 10% of cases. The fear of premature disc degeneration and vertebral artery injury is probably the biggest factor hindering more widespread adoption of this technique.
Cervical Instability, With or Without Partial Uncovertebral Joint Resection, for Spondylotic Radiculopathy
The major biomechanical function provided by the uncovertebral joints is the regulation of extension and lateral bending motion, followed by torsion of the cervical spinal vertebra.14,15 Some biomechanical studies suggest the possibility of spinal instability after unilateral uncovertebrectomy during anterior foraminotomy.14,16 A Japanese biomechanical study of sequential resection of cervical uncovertebral joints in human cadaveric spines showed that unilateral foraminotomy caused a 30% decrease in stiffness of the functional spinal unit during extension.14 However, early clinical outcomes do not show evidence of postoperative cervical spinal instability following ACF for cervical spondylotic radiculopathy.17,18 A recent Russian study by Klimov et al (2021) reports clinical and radiological outcomes of single-level ACF in patients with degenerative cervical radiculopathy.19 In this study, 36 patients were followed for a mean of 33.3 months and a battery of radiological parameters, including cervical sagittal vertical axis, spinocranial angle, neck tilt, T1 slope, and C7 slope, was evaluated to assess sagittal balance. All patients retained stability of the cervical spine based on White and Panjabi’s criteria (3.5 mm of translation, 11° of kyphosis), and sagittal balance parameters did not change significantly. No study has yet investigated the effects of uncovertebral joint resection on spinal stability after ADR placement. In our series of 5 patients undergoing ACF with uncovertebral joint resection following ADR, we report no case of postoperative instability at the latest follow-up visit as measured by dynamic flexion and extension views. Furthermore, it is the routine practice of some of the current authors to perform a significant uncinate resection at the time of ADR insertion without observed clinical instability. However, we do utilize ADR implants with more constraint, such ProDisc (Centinel Spine, West Chester, PA), M6 (Spinal Kinetics LLC, Sunnyvale, CA), and Prestige LP (Medtronic, Minneapolis, MN) as opposed to less constrained implants such as the Mobi-C (Zimmer Biomet, Warsaw, IN).
Analysis of Reoperations After ADR
Patients with new or recurrent radicular symptoms following ADR may be surgically managed by implant repositioning, implant removal, and subsequent fusion, or ACF with uncovertebral joint resection. A recent study by Zigler et al from Texas Back Institute analyzed the overall reoperation rate for a large consecutive series of 535 cervical ADR patients with ProDisc-C implants who were at least 2 years postoperative from their index surgery.20 Reoperations occurred in 30 patients for an overall reoperation rate of 5.6%. Among the various causes for reoperation, 3 led to ADR removal with anterior discectomy and fusion (due to device migration, subsidence, and spondylosis), 1 required ADR repositioning, and 21 for adjacent segment degeneration. One reoperation for ADR repositioning due to onset of new radicular symptoms (laterality was not mentioned) was taken back to surgery on postoperative day 6. There were no reoperations for device failure or vertebral body fractures. Even in cases with appropriate ADR indications and confirmation of proper implant placement, patients may present with complaints of postoperative, recurrent radicular symptoms. In these cases, the radicular etiology may be related to technical issues of insufficient uncovertebral joint decompression or development of bony osteophytic spurs causing nerve root compression. In either case, ACF with uncovertebral joint resection is a reasonable approach that provides direct decompression without destabilizing the cervical spine and preserving the functioning motion segment.
CONCLUSION
In patients with recurrent symptoms of cervical spondylotic radiculopathy following ADR, ACF with uncovertebral joint resection can be used to provide direct foraminal decompression without the need for implant removal. This approach also preserves motion at the affected level, preserves cervical spinal stability, and prevents the need for spinal fusion or removal of the ADR implant.
Footnotes
Funding The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests Eli Baron (Eli.Baron@cshs.org): Royalties from Elsevier, McGraw Hill on 2 textbooks. Carl Lauryssen (clauryssen@gmail.com): Sea Spine (consultant and royalties), CTL (consultant and royalties), BK Spine (royalties). Jason M. Cuellar (Jason.Cuellar@cshs.org): Centinel Spine (consultant).
Disclosure The authors report no financial disclosures related to this article.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.